
Abstract
Aim:
To increase understanding of alcohol-related child maltreatment on the basis of child protection cases in Lithuania. The study is based on a document content analysis of 203 case records of families at social risk. It identifies the prevalence of alcohol-related harm by analysing associations between types of drinkers and child maltreatment. It also maps the distribution of people who typically report this maltreatment. Both qualitative and quantitative analytical approaches are employed.
Results:
Child neglect was the most prevalent type of child maltreatment and was usually reported together with other types of child maltreatment. Child maltreatment was typically mentioned in the context of a caregiver’s heavy drinking. In 85.7% (174) of the cases, the family had at least one problem drinker. More than one problem drinker was detected in as many as a third of all cases. At least one form of child maltreatment was detected in families with a drinking mother in 60% of the cases (χ2 = 4.825, p < 0.05), with a drinking father in 36% of the cases (p > 0.05), and in 15% of the cases (p > 0.05) when there was a drinking partner in the family. The most common source of reporting by the authorities was the police (26.6%), and the most typical non-official source was the child’s relatives (16.3%).
Conclusions:
Alcohol-related child maltreatment needs special attention if issues of child safety in Lithuania are to be disclosed, evaluated, and responded to. Further research on this topic is needed.
There is a rapidly growing body of research within the field of alcohol’s harm to others that stresses the contribution of alcohol overuse to harm experienced by people surrounding the drinker, including children (Callinan et al., 2016; Kaplan, Nayak, Greenfield, & Karriker-Jaffe, 2017; Room et al., 2010; Warpenius & Tigerstedt, 2016). Studies on child welfare outline that parental alcohol overuse is one of the major causes and risks of child neglect and abuse (Esser et al., 2016; Freisthler, Holmes, & Wolf, 2014; Laslett, Dietze, & Room, 2013; Velleman & Templeton, 2016; Wells, 2009; Widom & Hiller-Sturmhofel, 2001). This is known to have negative and long-lasting consequences for the children (Raitasalo, Holmila, Autti-Rämö, Notkola, & Tapanainen, 2015; Rossow, Felix, Keating, & McCambridge, 2016; Rossow, Keating, Felix, & McCambridge, 2016; Velleman & Templeton, 2016).
According to general population surveys internationally, the prevalence of alcohol-related harm to children varies from a low of 4% to a high of 54% (Esser et al., 2016; Kaplan et al., 2017; Laslett, 2014; Laslett et al., 2017). It was found in a RARHA study (joint action on reducing alcohol-related harm) that the highest prevalence of severe harm from a known heavy drinker in Central Eastern and Eastern European countries is in Lithuania. The highest prevalence of persons who lived with a heavy drinker or someone who drank a lot sometimes during the respondent’s childhood was found in the Baltic countries (38.1% among men and 39.7% among women in Estonia, and 38.1% among men and 36.5% among women in Lithuania) (Moskalewicz, Room, & Thom, 2016). Research conducted in Latvia, Macedonia, Moldova, and Lithuania showed the percentages of children who reported at least one type of abuse: 33% of children in Latvia, 42% in Lithuania, 18% in Macedonia, and 43% in Moldova. The children reported the following rates of parental overuse of alcohol: 12% in Latvia, 13% in Lithuania, and 4% in both Macedonia and Moldova. Parental overuse of alcohol was associated with children’s emotional and/or physical abuse in all four countries (Sebre et al., 2004).
Studies of child welfare and harmful parental alcohol use have highlighted heavy alcohol use as a contributor to child maltreatment: internationally the rates varied from 13% to 70% (Laslett, 2014; Rossow, 2000). Families abusing substances tend to have higher rates of maltreatment recurrence (Fuller & Wells, 2003; Laslett, Room, Dietze, & Ferris, 2012) and a greater number of placements and longer stays in out-of-home care (Berger, Slack, Waldfogel, & Bruch, 2010). There is still a gap in understanding the relationship between the type of child maltreatment and drinker category within the family.
The main aim of this study was to increase understanding of alcohol-related child maltreatment in child protection cases. The specific research questions to obtain this aim were: What is the prevalence of alcohol-related problems in child protection cases? What is the distribution of reporting sources – to what extent are the reports filed by the authorities and to what degree do they come from non-official sources, such as the families’ neighbours and relatives? Is there an association between the child maltreatment type and different caregivers as problem drinkers? What is the context of alcohol-related child maltreatment?
Child protection in the Lithuanian system
Lithuania has a population of 2,888,558, with 518,201 children (in 2016). As a former Soviet bloc country, it still has some traits from the old Soviet regime. The current extreme market orientation is not modified by social support institutions and is combined with conservative ideologies about women and family (Kabašinskaitė & Bak, 2006). The liberal approach is growing strong roots in the Lithuanian welfare state system (Aidukaite, Moskvina, & Skucienė, 2016). It is thus not surprising that alcohol consumption and the resulting harms are more prevalent in Lithuania than in other Eastern European countries (Moskalewicz, Room, & Thom, 2016; Shield, Rylett, & Rehm, 2016). A third (29–30%) of all Lithuania’s residents have been found to engage in harmful alcohol use (Kalasauskas, Klumbienė, Veryga, & Petkevičienė, 2012; Tamutienė, 2014).
Lithuania recognises the problem and the risk of child maltreatment posed by the caregiver’s alcohol use. However, the problem is reduced to a specific group, officially defined as families at social risk (FSR). In the legal definition, this concept includes parents with substance abuse problems, lack of social skills, and improper care of their children (Lietuvos Respublikos Seimas, 2006). According to the data of the Information System of Social Support to the Family (2016), Lithuania had 9757 cases of FSR and 19,043 affected children in 2015, and 9676 such families with 18,756 children in 2016. In 2010, 3.66% of all Lithuania’s children were living in families at social risk; the figure had risen to 3.7% in 2014–2016 (Lietuvos Respublikos Valstybės, 2016). Families at social risk are treated as ill and problematic (Žalimienė, 2011), yet support agencies ignore their needs (Žalimienė & Dunajavas, 2015).
Lithuania officially acknowledged child protection from violence by ratifying the UN Convention on the Rights of the Child in 1995. This was reinforced by Civil and Criminal Codes and the Law on Fundamentals of Protection of the Rights of the Child (1996) (Dromantienė & Šalaševičiūtė, 2006), which bans all forms of violence against children, including corporal punishment. As of 14 February 2017, the law also acknowledges various types of child maltreatment (Lietuvos Respublikos Vaiko teisių apsaugos pagrindų įstatymas, 1996, 2017). These documents aim to ensure a safe environment for a child’s development, together with a child’s right to live with parents unless this contradicts the best interests of the child.
The office of Ombudsman for Children’s Rights was established in 2000. The supervision and protection of children’s rights in Lithuania is the responsibility of the municipal Child Rights Protection Service (CRPS). The State Child Rights Protection and Adoption Service coordinates the work of the municipal CRPS, which is in charge of registering families at social risk, investigating situations, conducting interventions and assessments, and, if needed, organising alternative care (Dromantienė & Šalaševičiūtė, 2006).
Muižnieks states, “while Lithuania has a relatively well developed institutional and policy framework for the protection of children’s rights, there is still a considerable gap between the stated policies and their implementation” (2017, p. 21). There is also a tendency of growing violence against children: in 2012, 1261 children most likely suffered from violence; in 2013, 1362 children; in 2014, 1192 children, and in 2015, 1578 children (Ministry of Social Affairs and Labour, 2016). In 2016, the figure had risen to 2474. There are problems in collecting statistics about child maltreatment in Lithuania because of, for example, ignorance of child neglect (as one type of child maltreatment), which is not included in formal reports and statistics (Lietuvos Respublikos Valstybės, 2016).
There are no data about the prevalence of alcohol-related child maltreatment in child protection cases in Lithuania. Child Rights Protection Service specialists have identified problem drinking as one of the fundamental factors behind children being placed in the protection system (Česnuitytė & Okunevičiūtė-Neverauskienė, 2009; Štelemėkas, 2014). The perpetrators of physical and emotional abuse against children are usually household members (Lietuvos Respublikos Valstybės, 2016), and there is an urgent need to understand the child maltreatment types and their relationship to drinker categories in child protection cases.
Research methods
The study was based on document content analysis of the case files of families at social risk (FSR). A case file contains the paper records concerning the family. We employed a content analytic strategy (Miller & Alvarado, 2005) to evaluate demographic, drinking, and other evidence related to formal communications to CRPS. Content analysis was conducted by combining qualitative and quantitative analytical approaches.
Sampling and sample socio-demographic characteristics
The research setting was the municipality of Kaunas, the second largest city of Lithuania, with a population of 297,669 in 2016. In 2015, the FSR register contained 442 families (0.1% of all Kaunas inhabitants) with 620 children (1.2% of all Kaunas children), under the supervision of CRPS of Kaunas Municipality (Lietuvos Respublikos Valstybės, 2016). There is almost no publicly available socio-demographic data about all Lithuanian families with children and FSR. The information about FSR concerns only the number of children and their age in Lithuania as a whole and in each municipality. Stankūniene, Baublytė, and Maslauskaitė (2017) indicated that 27.1% of all children live in single parent families; 23% with single mothers.
The sample size was calculated using the sample size calculator for estimations program (Naing, Winn, & Rusli, 2012), setting the confidence level at 95%, and using the precision level of 0.05. We selected 203 subjects from the FSR register by simple random sampling. Online family files had very limited information about the families (children’s names, dates of birth, parents’ names and ID codes, date and reason of inclusion on/exclusion from the register, and the responsible child protection officer). There was no information about fathers, and it was not evident how many mothers were single, which made representativeness unknown. Thus, being on the register was the only case selection criterion. We decided to analyse the paper-recorded case files in order to increase understanding of alcohol involvement in child protection cases. The Child Rights Protection Services keep the paper-recorded case files (reports about child maltreatment, investigation, case management protocols, etc.) about each family in their office. All 203 paper-record files were obtained from the CRPS.
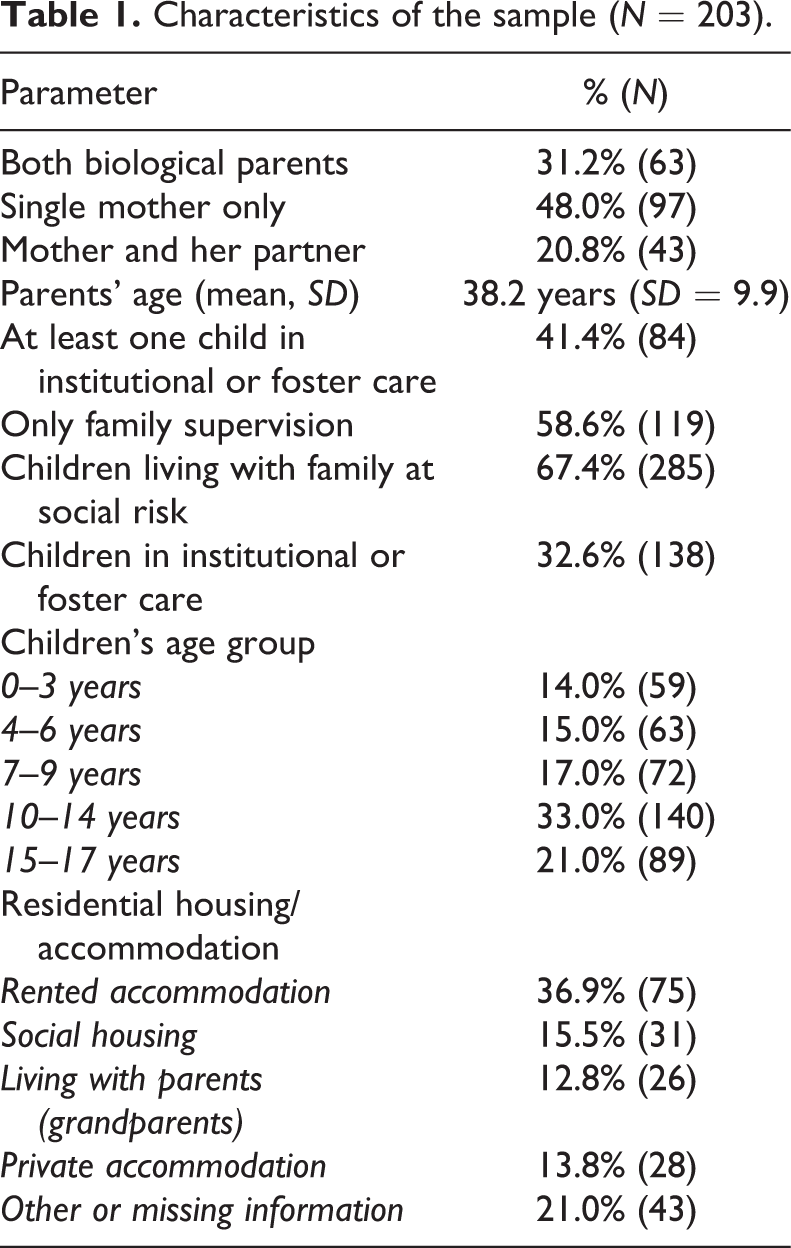
As illustrated in Table 1, the parents’ average age in the selected cases was 38.2 years. The families had 423 children, but only 285 children lived within those families at the time. The children’s age distribution was as follows: of the children living in families at social risk, 14% were 0–3 years old, 15% were 4–6 years old, 17% were aged 7–9 years, 33% aged 10–14 years, and 21% were 15–17 years old. Of the caregivers within a family, 31.2% were both biological parents, 48% were single mothers, while mothers and their partners made up 20.8% of such caregivers. The rest of the children (138) had been removed from home care, and the parental rights were limited. Of the families, 58.6% had supervision and support, and 41.4% had at least one child in out-of-home care. With regard to housing, 36.9% of the families lived in rented accommodation, 15.5% in social housing, 12.8% lived with parents (the child’s grandparents), and 13.8% lived in a private flat or a house.
Characteristics of the sample (N = 203).
Data collecting procedures and ethics
Data collecting was carried out by the author and two research assistants using the paper data collection instrument created by the author. The data were collected between December 2015 and March 2016. The research assistants were provided with one day of training on child welfare procedures, case files, legal reports, and data collection. The researchers signed confidentiality and anonymity contracts with the CRPS, who provided a separate room for analysing and discussing the cases. The researchers reviewed the files and collected data using the data collection forms. Reliability was tested by having all the three researchers review the same three cases. Data were entered into SPSS 24 by the author.
All personal information was removed from the cases to ensure anonymity and confidentiality. The study protocol was approved by Vytautas Magnus University (PR-S-08-01/01).
Categories, variables, coding
The categories and subcategories used as variables for the quantitative content analysis were established during the pilot study of ten case files. The following variables were defined: parents’ age, date of inclusion in the records, reporting sources (police, neighbours, child, other relatives of a child, healthcare institutions, social and educational institutions, anonymous reporters), information on the child’s caregivers (both biological parents, single mothers, mothers and their partners), number and age of children, household status (social, owned, rented), maltreatment (neglect, physical abuse, sexual abuse, emotional abuse, and witnessing violence in the family), informal social support givers, number of penalties for child neglect (court/legal rulings), decision on child care, services for parents, services for child.
The specialists do not fill in any questionnaires or do tests on alcohol use for problem drinkers in the family. The drinkers were identified from the case records filed by the police, neighbours, social workers, or others. A dichotomous variable was used to code problem-drinking mother, father, partner (not biological child’s father), child, and other adult family members (where 0 means no information/non-drinker or N/A, and 1 means that a problem alcohol use/problem drinker was found). The records on frequency of alcohol misuse were not included. Information was also collected and recorded about the treatment of alcohol use disorders, which were measured as dichotomous variables (in the addiction treatment specialists’ written responses to CRPS queries or in the social workers’ reports on work with the family).
Child maltreatment in this study is classified and distinguished into types of neglect, physical abuse, and a child’s being witness to violence. Neglect is a state of omission where, regardless of intention, carers fail to provide health, education, emotional development, nutrition, shelter, or safety for their child (Gilbert et al., 2009). The first time that Lithuanian legislation defined the term “neglect” and specified the maltreatment types was on 14 February 2017 (Lietuvos Respublikos Vaiko teisių apsaugos pagrindų įstatymo, 2017). Before this date only the recommendations from the work with families at social risk had specified that “neglect” referred to not meeting long-term the child’s physical and mental needs, thereby impeding the child’s full-fledged development and functioning. Not meeting the child’s basic needs includes neglect of the child’s nourishment (child is constantly hungry), clothing (child does not have shoes or warm clothes in the winter), and physical safety and health (child does not receive appropriate medical care). It also includes neglect of the child’s socialisation and education, and desertion, abandonment, or banishment from home (Lietuvos Respublikos socialinės apsaugos ir darbo ministrerija, 2003). Child neglect was coded generally on the basis of finding at least one of these neglect types in the file (yes/no). Physical abuse was recorded in those cases when the file had data from the reports about the child’s bruises or scratches or information about the child having been beaten. Sexual abuse was included in the initial plans of analysis, but due to unreliability of data (the files had plenty of contradictory data), it was not included in the quantitative analysis. Witnessing domestic violence (violence in presence of a child) was measured as a dichotomous variable in those cases when the reports from the police and/or social workers were found.
Analyses
The case files for FSR selected by random sampling were analysed, and an SPSS data file (N = 203) was formed. Descriptive statistics, cross-tabulation with χ2, and logistic regression were applied to answer the research questions. The significance level was set at 0.05 for all analyses. Logistic regression for child maltreatment type (physical and witness of violence) as a dependent variable was applied in order to assess the isolated impact of each problem drinker (mother, father, partner). The Hosmer–Lemeshow test was applied in order to test how well the logistic regression models fit. The significance of the fitted models was tested using −2 Log Likelihood and χ2, and Cox and Snell R2 to obtain the proportion of variances explained by the predictors. Odds ratios (OR) with 95% confidence intervals (CI) were calculated. All analyses were conducted using SPSS 24.
Content analyses were used to describe the context of the quantitative data and the context in which the documents functioned.
Results
Reporting to Child Rights Protection Services (CRPS)
Reporting abuse against children is mandatory in Lithuania (Lietuvos Respublikos Seimas, 1996). The legal sanctions for not reporting are previewed only for very serious crimes, but healthcare specialists and psychologists do not report all cases due to confidentiality and lack of identification (Čėsnienė, 2007). Case analyses showed that almost all families were reported as manifesting some type of child maltreatment. Child maltreatment reports come from the authorities (55%) such as the police and social services, and from non-official sources such as the relatives and neighbours (45%) (Table 2). The reporter category varies by maltreatment type and by problem drinker within a family, but statistically significant differences were found only with regard to a child’s being witness to violence (χ2 = 14.19, p = 0.028), and when the mother was a problem drinker (χ2 = 17.45, p = 0.008). The most prevalent official source of reporting was the police (26.6%), while the child’s relatives were the most typical non-official source (16.3%). The least common source to inform the CRPS about experienced maltreatment was children themselves.
Reporters to Child Rights Protection Services by three child maltreatment types and drinker categories (%).
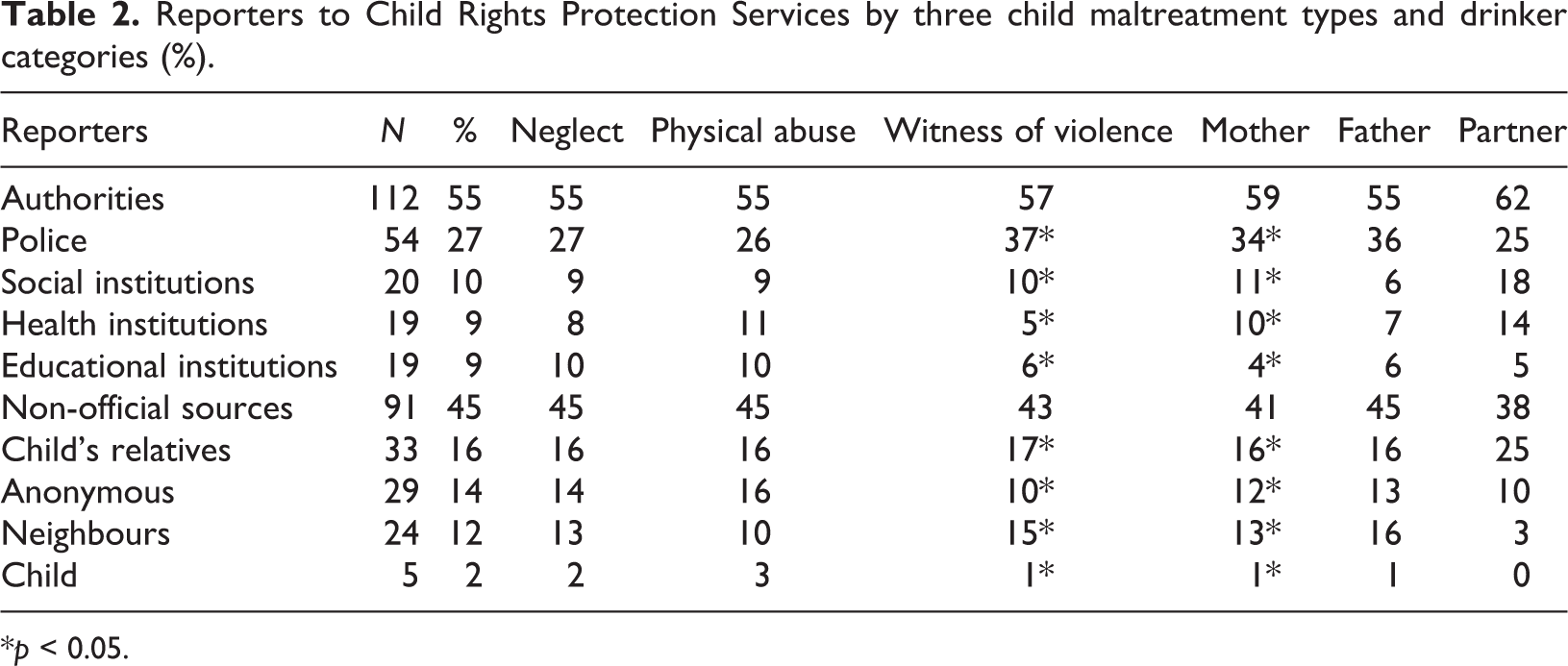
*p < 0.05.
Neighbours most often report long-lasting parental drinking and child neglect. The context of neighbours’ reports was related to mothers’ drinking and concern about children’s basic needs. Case content analysis revealed that problem-drinking parents usually became angry as a result of the report and created false stories about the reporters lying as revenge or for other reasons. It is therefore understandable that many reporters (14%) wanted to remain anonymous to avoid conflict.
Child maltreatment was usually mentioned in the context of a caregiver’s heavy drinking. Typical reporting could be described as follows: The parents drink heavily, do not look after their children, leave children alone at home for a long time, other drinkers often visit the family, children have nothing to eat, they do not attend school. We report that the safety of children is in danger.
As illustrated in Table 2, physical child abuse was most commonly reported by the police, a child’s relatives, and anonymous persons. Reports by healthcare institutions pertaining to child neglect and physical abuse typically related to pregnant mothers who had arrived at the surgery drunk. Healthcare institutions also informed about children’s traumas which had possibly resulted from parental maltreatment or abuse, including long-term physical violence. There were only two cases reported by psychiatric emergency services concerning mothers in a state of alcoholic psychosis. In such cases, the emergency services were requested to take care of the children. These exceptional cases demonstrate that addiction treatment centres focus their activities only on the drinker and do not pay attention to the risk that is being caused to the children. The reports on child maltreatment from paediatricians, family doctors, child psychologists, or psychiatrists were very rare and may indicate a gap of knowledge of how to recognise child maltreatment.
The police (37%) and the children’s relatives (17%) most often reported that a child had witnessed family violence. The most typical police report reads: We had a call from citizen “N” about the noise made by drinking people at address “N”. When we checked the address, we found drinking parents “NN” and another adult “NN”. They were drunk, the blood alcohol content was “N”. Child (children) “N” was found at this address. Due to insecurity the children were placed in “Pastogė” [temporary care institution]. Please make a decision about the future of the child.
Alcohol involvement in child maltreatment
At least one form of child maltreatment was detected in 93.1% (N = 189) of case files on families at social risk. The rest of the cases (6.9%) were mothers under 18 years old considered to be at risk, but there were no data about child maltreatment in their cases. The most common child maltreatment type was neglect (91.1%, N = 185), followed by a child’s witnessing of violence (57.1%, N = 87), and physical violence (40.4%, N = 82).
Alcohol featured heavily in the lives of families at social risk. The case file analysis demonstrated that in 85.7% (N = 174) of FSR at least one family member was a problem drinker. One problem drinker was identified in 47% (N = 95) of these families. More than one person as a problem drinker was detected in 33.5% (N = 68) of FSR. Pearson’s χ2 test results showed that at least one form of child maltreatment was detected in a family at social risk with a drinking mother (60%, χ2 = 4.825, p < 0.05), with a drinking father (36%, p > 0.05), and a drinking partner (15%, p > 0.05). In the category of a drinking mother, there were only five cases with no identified maltreatment. In the categories of a drinking father and a drinking partner, the corresponding numbers of cases were six and three, respectively.
Table 3 presents the cross-tabulation results between problem drinkers in FSR and different child maltreatment types. The results within each drinker category demonstrate very high numbers of child maltreatment. Mothers’ problem drinking statistically significantly contributed to child neglect (χ2 = 4.825, p < 0.01), witness of violence (χ2 = 10.721, p < 0.01), and physical violence (χ2 = 3.481, p < 0.05). The contribution of a problem-drinking biological father was significant to a child’s witnessing violence (χ2 = 5.070, p < 0.05), but not to physical abuse and neglect. In the category of a drinking partner, statistically significant differences were detected in a child’s being witness to violence (χ2 = 20.469, p < 0.001) and subject to physical abuse (χ2 = 10.174, p < 0.001).
Child maltreatment types by problem drinker category (%).
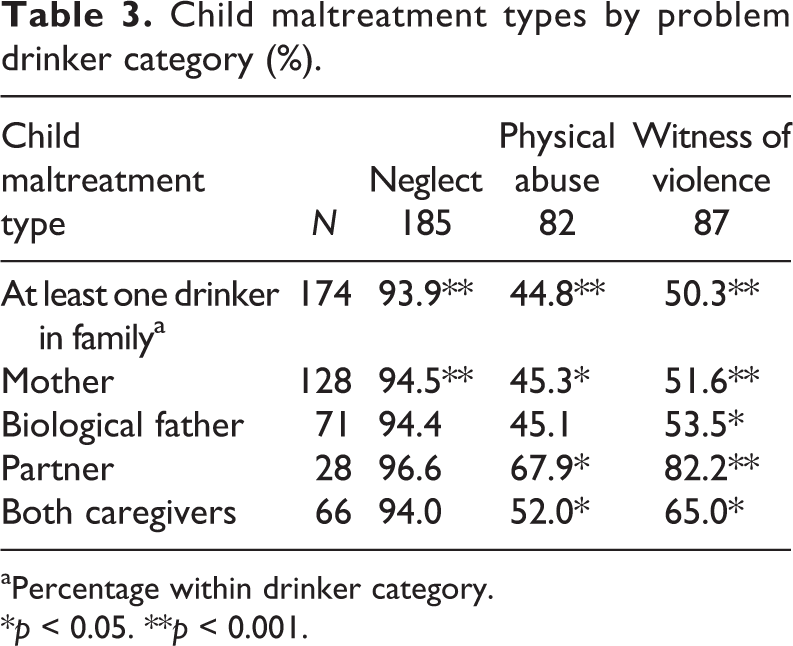
aPercentage within drinker category.
*p < 0.05. **p < 0.001.
Child maltreatment was prevalent in the category of a drinking biological father: neglect (94.4%), physical abuse (45.1%), and a child’s witnessing of violence (53.5%), which was the only to be statistically significant.
There were 42 cases of families living with the mother’s partner; 31 of the partners were identified as problem drinkers. The rates of all three types of child maltreatment were the highest within the drinking partner category in comparison to other drinkers (Table 3), but statistically significant only with regard to the child’s being witness to violence (82.1%) and subject to physical abuse (67.9%).
Logistic regression for child neglect, physical abuse, and witness of violence as a dependent variable was run in order to assess the impact of each drinker: mother, father, and partner. After controlling for other factors in the model, the likelihood of neglect increased by 2.9 times with a drinking mother and the likelihood of the child witnessing violence by 1.8 times (Table 4) when compared with a non-drinking mother. A problem-drinking father increased the likelihood of the child witnessing violence by 1.5 times in comparison with non-problem-drinking father. A problem-drinking partner increased the likelihood of the child experiencing physical abuse by 5.6 times and witnessing violence by 8.1 times (Table 4) in comparison with a non-drinking partner.
Results of logistic regression for child neglect, physical abuse, and witness of violence associated to drinker.
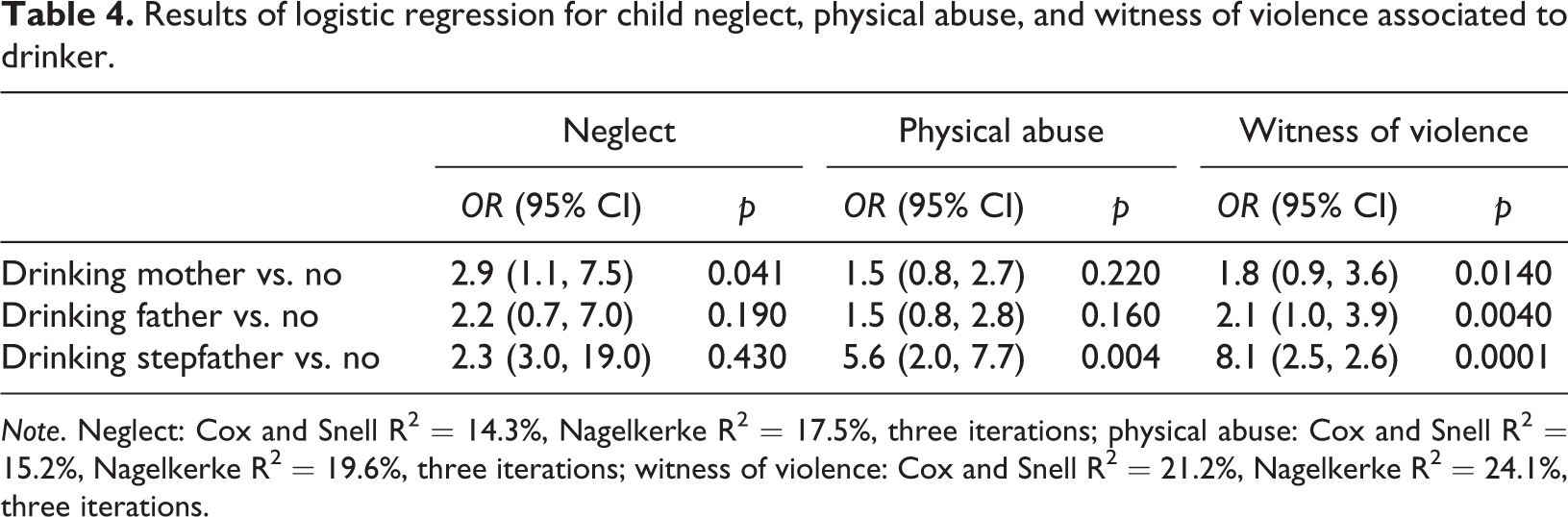
Note. Neglect: Cox and Snell R2 = 14.3%, Nagelkerke R2 = 17.5%, three iterations; physical abuse: Cox and Snell R2 = 15.2%, Nagelkerke R2 = 19.6%, three iterations; witness of violence: Cox and Snell R2 = 21.2%, Nagelkerke R2 = 24.1%, three iterations.
Discussion
Alcohol-related child maltreatment
At least one form of child maltreatment was detected in 93.1% of case files. Alcohol involvement in the cases of child maltreatment was very high. Families at social risk had at least one problem drinker in 85.7% of the cases where at least one type of child maltreatment had occurred. Internationally, alcohol-related child maltreatment prevalence ranges from 13% to as much as 80% of child maltreatment (Forrester, 2000; Forrester & Harwin, 2011; Jones, 2004; Kelley, 2002; Laslett et al., 2013; Rossow, 2000). Prevalence rates are not fully comparable due to different research methods and settings. However, compared to other countries in Europe and globally, the most prevalent alcohol use and related harm have been found in Lithuania (Moskalewicz et al., 2016; Shield et al., 2016).
Reporters
The authorities (55%) and sources other than the authorities (45%) reported child maltreatment to the Child Rights Protection Services in almost equal measure. A similar balance has also been found in the United States, the UK, and Spain (Gilbert et al., 2009). There is, however, a difference in the most common source of reporting: in this study, child maltreatment was most often reported by the police (26.6%), while in the US, the UK, and Spain the most common reporting bodies were educational institutions (16.5%). More study should be carried out to analyse why educational institutions report so little in Lithuania. The police have such a predominant reporting role probably because the law enforcement institution has a duty to inform the CRPS in all family violence cases (Lietuvos Respublikos Seimas, 2011). The State Audit found that this duty was fulfilled only in about one third of cases (Valstybės auditas, 2015), and case file analyses revealed that the police reported to the CRPS about a child being a witness of violence only in 36.8% of cases.
Based on case reviews in California, Jones (2004) showed that Child Protection was more frequently informed by healthcare specialists (21%), law enforcement (20.3%), and schools (18.3%), and by relatives/neighbours only in 12.6% of cases. While in the present study most reports to the CRPS were submitted by the police (27%), an equal share (9–10% each) was submitted by social, healthcare, and education institutions. The impact of relatives/neighbours was higher (28%).
The fact that emergency and intensive care specialists reported only severe physical abuse against children shows that other medical care specialists had difficulties identifying other forms of child maltreatment. This study confirmed that serious injuries were more likely to be reported to child protection (Gilbert et al., 2009). There should be more research analysing why paediatricians, psychiatrists, and psychologists were not among the reporters.
Medical care specialists of adults should be the first to identify alcohol misuse problems of parents and suspect the risk of child neglect, but they did not report anything. However, even though the majority of families at social risk have alcohol consumption problems, addiction treatment specialists do not report to child protection nor do they participate in case management. Addiction treatment and child protection systems are developed under distinct legislative, administrative, and financing structures in Lithuania. Therefore, collaboration between the addiction treatment and the child protection systems should be regulated at the state level, ensuring the organisational, geographical, and financial accessibility of the services. Research in countries where such changes have already been made confirms that such steps have improved parenthood and children’s wellbeing (Dauber, Neighbors, Dasaro, Riordan, & Morgenstern, 2012; Marsh, Smith, & Bruni, 2011; Neger & Prinz, 2015; Osterling & Austin, 2008). These steps towards better child protection should also be taken in Lithuania.
Children themselves reported few cases of maltreatment. This could be related not only to their age, but also to associative stigma (Tamutienė & Laslett, 2017). Other researchers have found that the children of substance-misusing parents have difficulty talking about their situations: they become locked into silence (Barnard & Barlow, 2003; Hill, 2015; Werner & Malterud, 2016a, 2016b). There is a need to analyse why children themselves rarely report on harms from parental drinking.
Child neglect was the most prevalent type of child maltreatment, usually reported together with other types. The fact that the authorities report child neglect when small children are left in public places or when a child has committed a crime, but not related to children’s needs, could be interpreted as a state of “neglect of neglect” (Hobbs & Wynne, 2002). Also, in public reports about child maltreatment, Lithuanian state institutions only include child emotional, physical, and sexual abuse (Ministry of Social Affairs and Labour, 2016; Lietuvos Respublikos Valstybės, 2016). The harm of alcohol to children in early phases is highly tolerated in Lithuania. Neither the authorities nor others – such as relatives and neighbours – pay enough attention to potentially risky situations. Child neglect may thus become chronic and may finally include other types and also very severe forms of maltreatment.
It is evident that the authorities, including the Child Rights Protection Services, need training about all types of maltreatment and its detection. Results from Spain show that detection of child maltreatment improved after training and supporting frontline health and social services professionals (Cerezo & Pons-Salvador, 2004).
Alcohol-related child maltreatment
This study found that child neglect was alarmingly prevalent, more than 90%, if families at social risk had a drinking mother, a drinking biological father, or if the mother had a drinking partner. Very high prevalence rates of child maltreatment were detected within the drinking mother category, with at least one form of maltreatment (96.1%), neglect (94.5%), witness of violence (51.6%), and physical violence (45.3%). The percentage of problem-drinking mothers registered in the CRPS may be a result of social and cultural factors, as child rearing is primarily a mother’s concern in Lithuania. This was reflected in the case files, where single-mother families constituted 48% of the families. Information about the fathers of the children was inadequate, and the involvement of separated fathers in child protection was very low. A similar situation of substance-abusing mothers’ cases was found in London (Forrester & Harwin, 2011). Case file analyses support the insights that caregiver vulnerability and partner violence are often involved in child maltreatment, and that early intervention by the child protection services helps prevent child maltreatment (Wekerle, Wall, Leung, & Trocmé, 2007).
A child’s being witness to violence was the only type of maltreatment with significant covariates for all problem drinkers. Regression analyses showed that the possibility of a child witnessing violence was twice as high when a mother or a biological father was a problem drinker, and eight times higher when the mother’s partner was a problem drinker – all these in comparison with non-problem drinkers. The content analyses disclosed domestic violence against a child’s mother, who was a victim herself and was blamed by the professionals for failure to protect her children. These results confirmed once again the scholarly insights of an overlap between domestic violence and child maltreatment and alcohol being a major risk factor (Jouriles, McDonald, Smith Slep, Heyman, & Garrido, 2008; Stanley, 2011).
Alcohol’s harm to children (and others) should be recognised and properly addressed at micro, mezzo, and macro levels (Warpenius & Tigerstedt, 2016). There is a pressing need to raise awareness of alcohol’s harm to others, especially to children, which affects the whole society, not only a specific group of heavy drinkers. Alcohol involvement in child maltreatment is prevalent and should be prevented before it progresses and manifests in different types of child maltreatment. Tools are needed to assess caregivers’ problem drinking, children’s needs, different types of maltreatment, and inter-agency cooperation. Child welfare and protection workers should be aware of all the risks regarding the type of a problem drinker. If a mother or both carers are problem drinkers, there is a risk of all types of child maltreatment. If a mother lives with a problem-drinking partner, there is an increased risk of child physical abuse. If there is at least one problem drinker in the family, there is a risk that a child will witness family violence.
Research limitations
The first limitation is related to the research setting, which encompasses only the population of families at risk in one city of Lithuania. The results can therefore not be generalised. The second limitation is connected to information found in the case files, which is dependent on the subjectivity of the child rights protection specialists. All specialists possess file records, and the number of documents presented in each case often depends on the subjectivity of the specialist: in some cases the information is detailed, while in others there are only a few pages, and the information is poor.
Although the primary objective of the research was to evaluate emotional and sexual abuse, the data in the cases of sexual and emotional abuse were not used in the analysis because of validity issues of controversial information.
Despite the research limitations, this investigation is a contribution to the initiation of research on alcohol-related child maltreatment in Lithuania.
Footnotes
Acknowledgments
The author is grateful for the valuable comments and suggestions from Ramon Florenzano on earlier version of this article presented in 42nd Annual Alcohol Epidemiology Symposium of the Kettil Bruun Society in Stockholm 30 May–3 June 2016. Big thanks to assistants Juste Martinkeviciute and Mindaugas Vosylius. The Child Rights Protection Service of Kaunas Municipality gave their time and shared their accommodation and the author acknowledges their substantial contribution.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Vytautas Magnus University (PR-S-08-01/01).