
Abstract
Background:
In September 2012, a series of methanol poisonings occurred in the Czech Republic as a result of an influx of illicit alcohol into (predominantly) cheap alcoholic beverages on the retail market. The public authorities decided to prevent public health risks by prohibiting sales of liquors that contained more than 20% alcohol (> 20% liquor). The “partial” prohibition lasted for almost two weeks, but the poisonings still continued. This article assesses the impact of the methanol poisoning risks and the (partial) prohibition on alcohol drinking patterns, and describes the understanding of risks and their mitigation in vulnerable groups.
Methods:
The rapid assessment and response method (RAR) was used during the (partial) alcohol prohibition. Semi-structured interviews were conducted with respondents recruited for the study in alcohol-intake settings (e.g., bars and restaurants, street alcohol outlets) in six regions. In total, 107 alcohol users were interviewed, mostly with risky drinking patterns (69% scored ≥ 1 on the CAGE scale), and 53 alcohol retailers/staff members serving alcohol.
Results:
About one third of the alcohol users in the study (35%) drank > 20% liquors during the prohibition; a higher score on the CAGE scale was associated with a lower probability of drinking > 20% liquors during the period of the prohibition, probably because of the perception of being at high risk of poisoning. There was some increase in drinking liquors with an alcohol content less than 20%. Those who continued drinking > 20% liquors typically did so in the belief that some sources of these were safe.
Conclusions:
Public policies aimed at reducing the risk of methanol poisonings in emergency situations should adopt broader measures than those focusing on market control. These measures include increased access to brief interventions, addressing the strategies that alcohol consumers adopt to prevent risk, and, in general, helping consumers make informed choices to prevent further fatalities.
Keywords
In many countries, the regulation of alcohol markets has not been able to prevent the risks of methanol poisoning that occur mainly as a result of unrecorded alcohol production (Rehm, Kanteres, & Lachenmeier, 2010). Outbreaks of methanol poisoning have been documented in several countries, and often lead to fatalities resulting from metabolic acidity, respiratory arrest, hypotension, cerebral enema, and coma. In Norway, where methanol poisonings occurred between 2002 and 2004, nine of the 51 hospitalised patients died (Hovda, Hundreri, Tafjord, Rudberg, & Jacobsen, 2005), and so did 25 of the 111 individuals hospitalised for methanol poisoning in Estonia in 2001 (Paasma, Hovda, Tikkeberi, & Jacobsen, 2007), and four out of the 50 methanol-poisoned patients in Iran between 2000 and 2009 (Massoumi et al., 2012). In the USA, 2254 methanol poisoning cases were recorded between 1993 and 1998, and one in every 183 cases led to death (Davis, Hudson, Benson, Easom, & Coleman, 2002). In Edirne, Turkey, in 2005, almost 3% of all forensic autopsies were methanol-related (Azmak, 2006). Major consequences of non-fatal methanol poisoning include impaired vision, neurological impairments, or brain damage, mostly irreversible (Paasma, Hovda, & Jacobsen, 2009). A recent study has also shown cognitive impairments among methanol poisoning survivors (Bezdicek et al., 2017).
Several treatment approaches towards methanol poisonings have been described, among them fomepizole antidoting (Hovda et al., 2005; Zakharov, Navratil, & Pelclova, 2014), the administration of bicarbonate and ethanol, haemodialysis, and mechanical ventilation (AACT, 2002; Paasma et al., 2007). While the standards of methanol poisoning treatment are well developed (AACT, 2002), insights into informal social control and prevention activities around methanol poisonings among alcohol users are clearly lacking in the literature. These could help to guide activities that would prevent methanol poisonings in a crisis period – such as the outbreak of methanol poisonings in the Czech Republic in 2012.
Between 6 September and 14 September 2012, 19 fatalities resulting from methanol poisonings occurred in the Czech Republic. This was due to the intake of unrecorded alcohol containing methanol that had been put into bottles bearing the labels of established brands of > 20% liquor; the bottles were distributed through the conventional retail chain. As there is no licensing system for alcohol sales in the Czech Republic, and no form of state monopoly in place, it turned out to be impossible in the short run to effectively track and recall from the market all products that could be tainted with methanol. The authorities responded by prohibiting the sales of any liquors containing more than 20% alcohol (> 20% liquors), effective between 14 September and 27 September 2012. Criminal investigations conducted in the meantime suggested that > 20% liquors produced after 31 December 2011 were deemed safe, and the sale of such beverages recommenced after 27 September. However, seven more fatalities took place during the period of the (“partial”) prohibition, and an additional 19 occurred in the six months following the prohibition. In all, 81 individuals were hospitalised with acute methanol intoxication and survived, of whom 20 suffered visual impairment; further consequences are being monitored in a longitudinal research study (Zakharov, Pelclova, Diblik, et al., 2015; Zakharov, Pelclova, et al., 2014).
The “partial” prohibition, i.e., a prohibition of > 20% liquors, was a notable event in the Czech Republic, which over the long term has recorded high levels of alcohol consumption (Belackova & Stefunkova, 2016; Vondráčková & Št'astná, 2012; Zakharov, Pelclova, et al., 2014). The latest data show that 13 litres of alcohol per capita are consumed yearly in the Czech Republic, of which 26% are consumed in the form of liquor (WHO, 2014). In 2012, 4.8% of the Czech population (7.2% of men, 2.4% of women) were assessed as problematic drinkers who are probably addicted; about 7% in total were harmful or risky drinkers (Mravčík et al., 2014). On the topic of alcohol consumption and policy in the Czech Republic throughout its recent history, a sociologist who authored a renowned book carrying a similar title to that of this article stated that “the inexpensive and omnipresent beer has been a part of the social contract between the government and the society” (Bútora, 1995, p. 40). Up until now, the levels of alcohol taxation in the Czech Republic remain among the lowest globally (WHO, 2004), and there are no restrictions on the hours or locations of the premises that sell alcoholic beverages (WHO, 2014). With the high level of alcohol consumption and potential dependency, and with a rather “liberal alcohol policy”, it was unclear how effective the market controls would be and how alcohol users would respond to the sudden risk of poisoning from one of their beverages of choice and to its prohibition.
Reducing harms resulting from substance use: Users’ risk-reduction strategies
In an uncertain setting of toxic content being admixed into the drinks people “normally” drink, and when there is a “sudden” prohibition of these drinks, individuals are likely to have diverse responses. While a substantial proportion of alcohol users might respond to the risk of poisoning by abstaining from > 20% liquors, thus controlling their drinking for a period of time, (self-managed) abstinence from their substance of choice might not be a realistic solution for others.
Previous research has shown that reduced drinking of alcohol is a viable solution and a treatment goal for many alcohol-dependent individuals (Amsterdam & van den Brink, 2013), although it may not be viable in the long run (Pendery, Maltzman, & West, 1982). Harm reduction approaches to alcohol consumption that involve controlled drinking can thus help achieve meaningful behavioural changes (Marlatt, Larimer, Baer, & Quigley, 1993), and policies reducing the risks and harms associated with substance use should be made an inherent part of public health strategies (Newcombe, 1992).
Among recreational alcohol users, risk-reduction strategies related to drinking alcohol have included not exceeding a set number of drinks; alternation of alcoholic and non-alcoholic drinks; having a friend who lets one know when one has had enough; stopping drinking at a predetermined time; drinking water while drinking alcohol; putting extra ice in one’s drink; avoiding drinking games and mixing beverages; drinking slowly and avoiding keeping up with others; using a designated driver; going home with a friend; knowing where one’s drink is at all times; and seeking alternative activities that do not include alcohol (Howard, Griffin, Boekeloo, Lake, & Bellows, 2007; Lewis, Rees, & Kilmer, 2010; Sutfin et al., 2009).
When potentially toxic compounds are added to alcoholic beverages, the strategies that reduce the risks of methanol poisonings may, however, be more similar to those of illicit drug users. Individual strategies in this area have included not using drugs when one is alone; not mixing them with alcohol and other depressants; calling the emergency services in the event of an overdose; titrating drugs after a long period of abstinence; or sample-testing drugs before using them (Kerr, Small, Moore, & Wood, 2007).
The toxicity of methanol starts at doses as low as 8 mg, equal to 2% of a standard drink (Paine & Dayan, 2001). Once the methanol concentration achieves this margin, the only effective risk-reduction strategy to prevent methanol poisoning would be to avoid methanol-tainted drinks. Previous research has not looked into the risk-reduction strategies alcohol users employ when exposed to an increased risk of methanol poisoning, and/or the accuracy of the strategies that perceptibly reduce these risks.
This article assesses the impact of the prohibition of alcohol consumption during the period of the outbreak of methanol poisonings in the Czech Republic when > 20% liquors were prohibited for two weeks, and describes the risk-minimisation strategies that alcohol consumers took to prevent methanol poisonings during that period.
Data and methods
This article builds upon the rapid assessment and response (RAR) methodology, a set of tools used to guide an intervention in rapidly changing environments; a combination of qualitative and quantitative methods as well as data triangulation is an inherent part of the methodology (Stimson, Fitch, Rhodes, & Ball, 1999; WHO, 2003). As the RAR methodology had been previously translated into Czech and adopted locally (Miovský, 2007), it was conveniently used by the authors on 25–29 September 2012 in the context of the methanol poisoning crisis and subsequent prohibition in the Czech Republic. Semi-structured interviews were conducted with alcohol consumers and retailers in eight towns located in six different regions (see Table 1). Four of the six regional towns were selected because methanol poisoning cases had occurred there before the RAR started (Central Bohemian Region, Moravian-Silesian Region, Olomouc Region, and Zlin Region); two additional regional towns were chosen because they were prone to the occurrence of risky drinking patterns (the City of Prague because of its concentration of risky behaviours and Usti because of its being a socially disadvantaged region).
Sample composition – number of respondents per region and town.
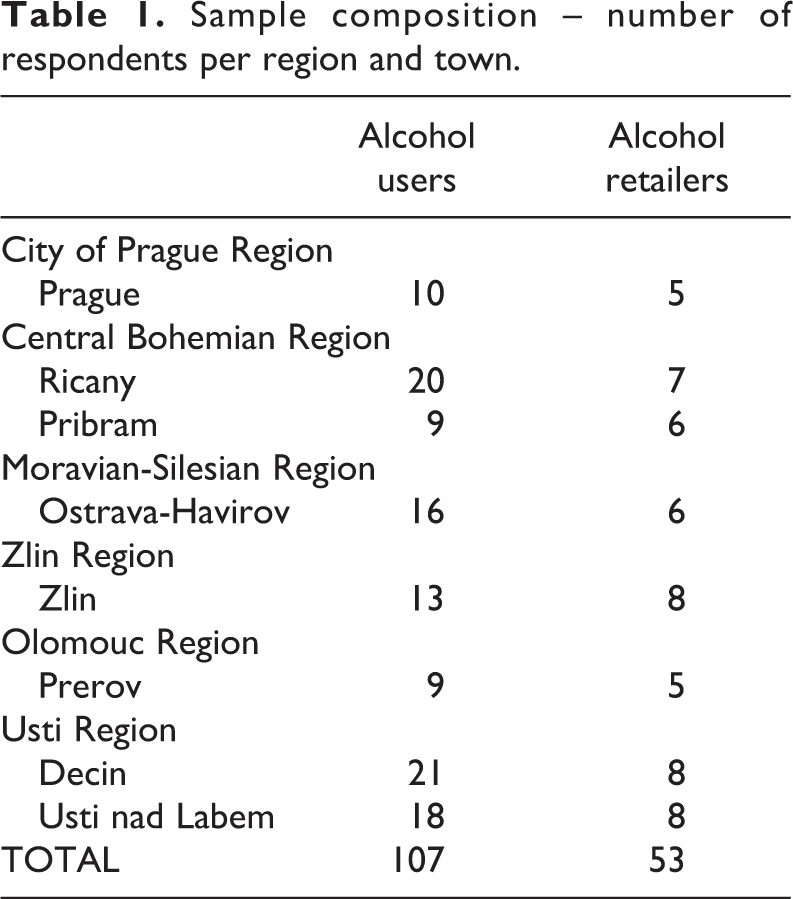
A suitable sample of individuals was recruited in each town in order to reach groups that could be vulnerable to methanol poisonings. In each town, the interviewer located at least four retail stores where alcohol was sold (preferably street retail outlets and small retail venues) and two bars or restaurants, conducting brief semi-structured interviews with the staff (retailer, bartender, etc.) and with alcohol users who were present at the venue. The interviewers were asked to focus when possible on socially marginalised individuals (e.g., homeless individuals) and/or apparent problem drinkers (unless they were intoxicated to such an extent that they could not participate in the interview). The respondents were granted anonymity; no personal data were collected. The interviews were recorded, and the recordings were deleted after transcription. The study was approved by the Ethical Committee of the National Monitoring Centre for Drugs and Drug Addiction.
The semi-structured interviews with alcohol users covered (i) their opinion on the prohibition measures; (ii) their current alcohol consumption patterns and consumption patterns prior to the (“partial”) prohibition; (iii) socio-demographic characteristics; and (iv) the CAGE scale (Bradley, Kivlahan, Bush, McDonell, & Fihn, 2001). The interviews with retailers focused on (i) the current alcohol portfolio available for sale; (ii) their opinion on the prohibition measures; and (iii) the impact of the prohibition on their economic activities.
The quantitative data were processed in Stata IC 11 for the descriptive characteristics of the study sample and for a quantitative assessment of the market situation prior to and during the period of the prohibition. In simple frequency analysis across categories, chi-square statistics were computed as well as z-test for pairwise comparisons within a row; for assessing the characteristics of those who continued drinking > 20% liquors during the period of prohibition, a logit model was used (the most commonly used model to explain a categorical variable with a set of independent predictors), while for the assessment of substitution in drinking patterns between each of the different beverage types before and during the prohibition, pairwise correlation was deployed (Spearman’s rank correlation, which is suitable for ordinal data analysis). As some of the indicated trends were not statistically significant due to low sample size, we used qualitative accounts to complement the description of the changing drinking patterns. The qualitative accounts were inductively coded and aggregated into categories in the NVIVO scientific software (Miovský, 2006; Patton, 2002).
Study population
In total, 107 alcohol users and 53 alcohol retailers were interviewed at 45 different venues (bars and restaurants, street retail outlets, small retail stores, and supermarkets selling alcohol). The average age of the alcohol users in the field assessment was 38 years (min. 16 years, max. 67 years); 76% were male (see Table 2). In comparison with the general population, the target population represented rather more highly educated individuals within the younger age groups (15–24 years, 25–34 years) and individuals with a rather lower level of education in the higher age categories (45–54 years, 55–65 years). Similarly, the younger respondents were more likely to be employed, while the older respondents were more likely to be unemployed. This suggests that the RAR succeeded in reaching two different groups of respondents who frequent nightlife and other alcohol intake venues. A quarter of the respondents were unemployed (26%) and a similar proportion (23%) earned the minimum wage or lower (about 320 EUR monthly); 11% had no source of income.
Socio-demographic characteristics.
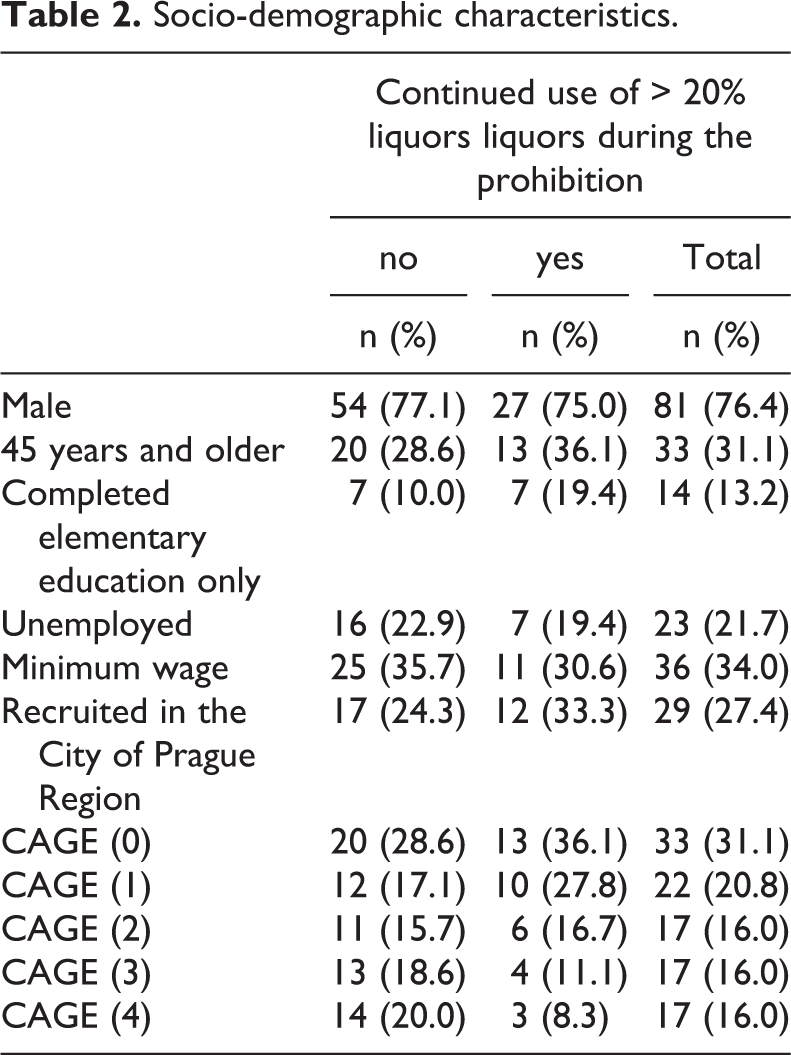
The alcohol users in this study scored rather high on the CAGE assessment: 31% scored 0; 22% scored 1; 16% scored 2; 16% scored 3, and 16% scored 4. In the general population aged 15–64 years in 2012, 83% scored 0 CAGE points (Mravčík et al., 2013). This suggests that the field study reached respondents with rather risky drinking patterns.
Findings
Decrease in consumption of > 20% liquors
The number of those who had abstained from > 20% liquors in the past 30 days increased from 5% before the (“partial”) prohibition to 66% during the prohibition. About one third of the respondents (34%, n = 36) continued drinking > 20% liquors despite the prohibition: 9% continued drinking them daily or almost daily compared to 18% before prohibition; 4% drank such liquors several times per week compared to 17% before prohibition; 12% drank > 20% liquors at least once a week compared to 37% before prohibition. All changes in the frequency of drinking > 20% liquors were statistically significant (see Table 3). Also, a significantly higher proportion of the respondents drank liquors with less than 20% alcohol content at least once a week during prohibition compared to the 30 days that preceded it (9%, a threefold increase). The changes in the frequency of consumption of other beverage types were not statistically significant: on average, the respondents continued drinking them to the same extent as before the (“partial”) prohibition (see Table 3).
Consumption patterns of the field study respondents prior to and during prohibition of > 20% liquors (Septrmber 2012).
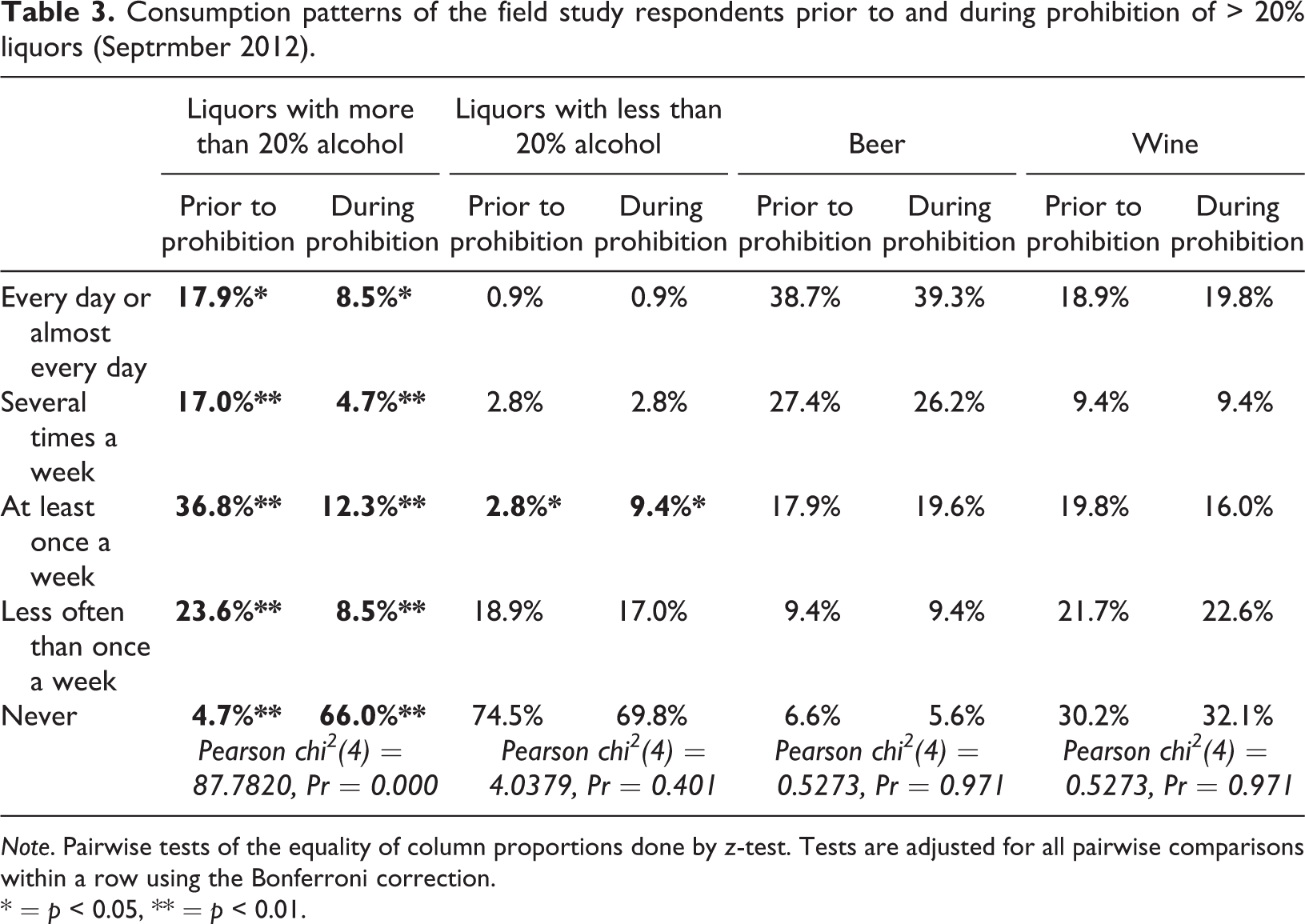
Note. Pairwise tests of the equality of column proportions done by z-test. Tests are adjusted for all pairwise comparisons within a row using the Bonferroni correction.
* = p < 0.05, ** = p < 0.01.
The alcohol consumers in the study were, thanks to widespread media coverage, aware of the risk of methanol poisoning and the related health damage, including a fatal overdose. Nevertheless, almost one third (28%) thought that poisoning “could not happen to them”. Half of the respondents claimed that it “could happen to them, but they did not feel at risk” (50%). Only 17% felt at risk, and 6% claimed that they felt seriously at risk. The perception of “being at risk” increased with the scores on the CAGE scale of risky drinking; while the overall difference in risk perception was not statistically significant, the respondents with the most risky drinking patterns (CAGE score 3–4) seemed to be slightly more likely to perceive themselves as being at the highest risk of methanol poisoning (9% felt very much endangered and 24% felt endangered) (see Table 4).
Individual assessment of the risks of methanol poisoning by the field study respondents.
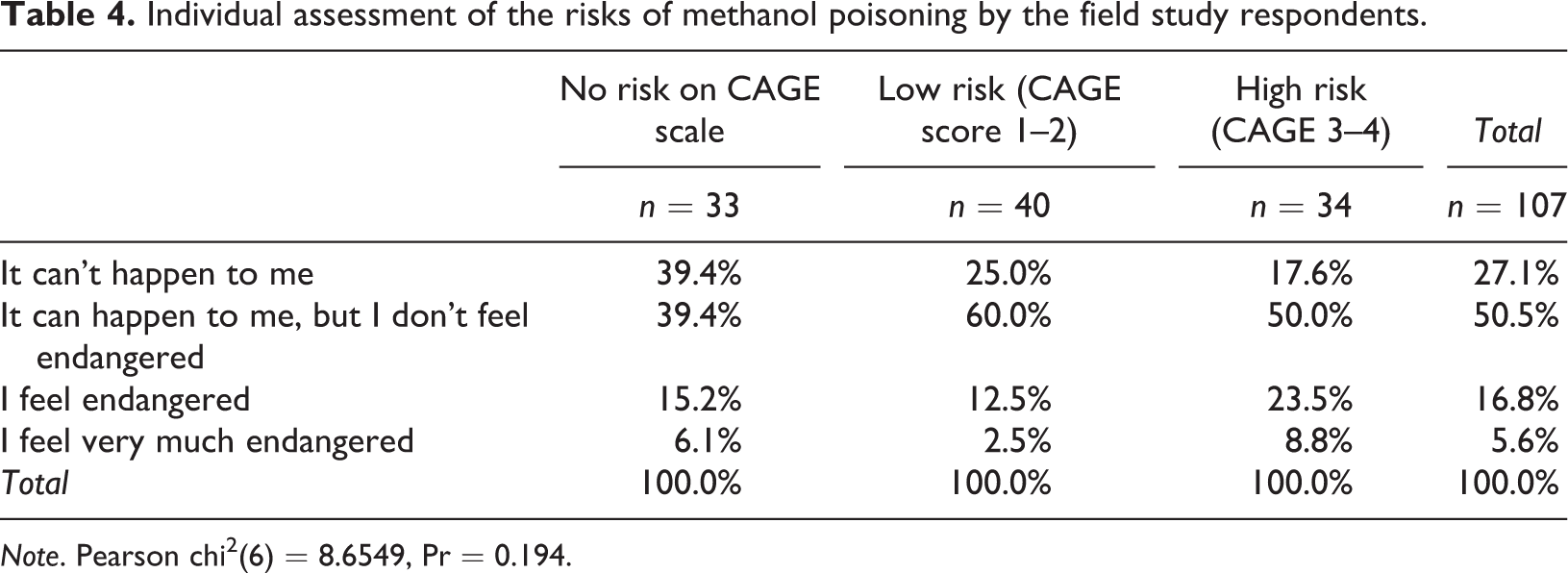
Note. Pearson chi2(6) = 8.6549, Pr = 0.194.
We further examined the characteristics of those who continued drinking > 20% liquors during the (“partial”) prohibition period. None of the likely predictors of continued drinking of > 20% liquors (the respondents’ socio-demographic characteristics and drinking patterns before prohibition) were found to be significant in single-predictor models on the 95% confidence level (unadjusted odds ratios). In a multivariate model though, we found that each additional point on the CAGE score was linked to the respondents being less likely to continue drinking > 20% liquors (AOR = 0.62, p = 0.025) (see Table 5). Thus, the more risky drinkers reduced their consumption of > 20% liquors to a greater extent than did others.
Odds of continued use of > 20% liquors during the prohibition and despite the risks of methanol poisonings (individual respondents’ characteristics).
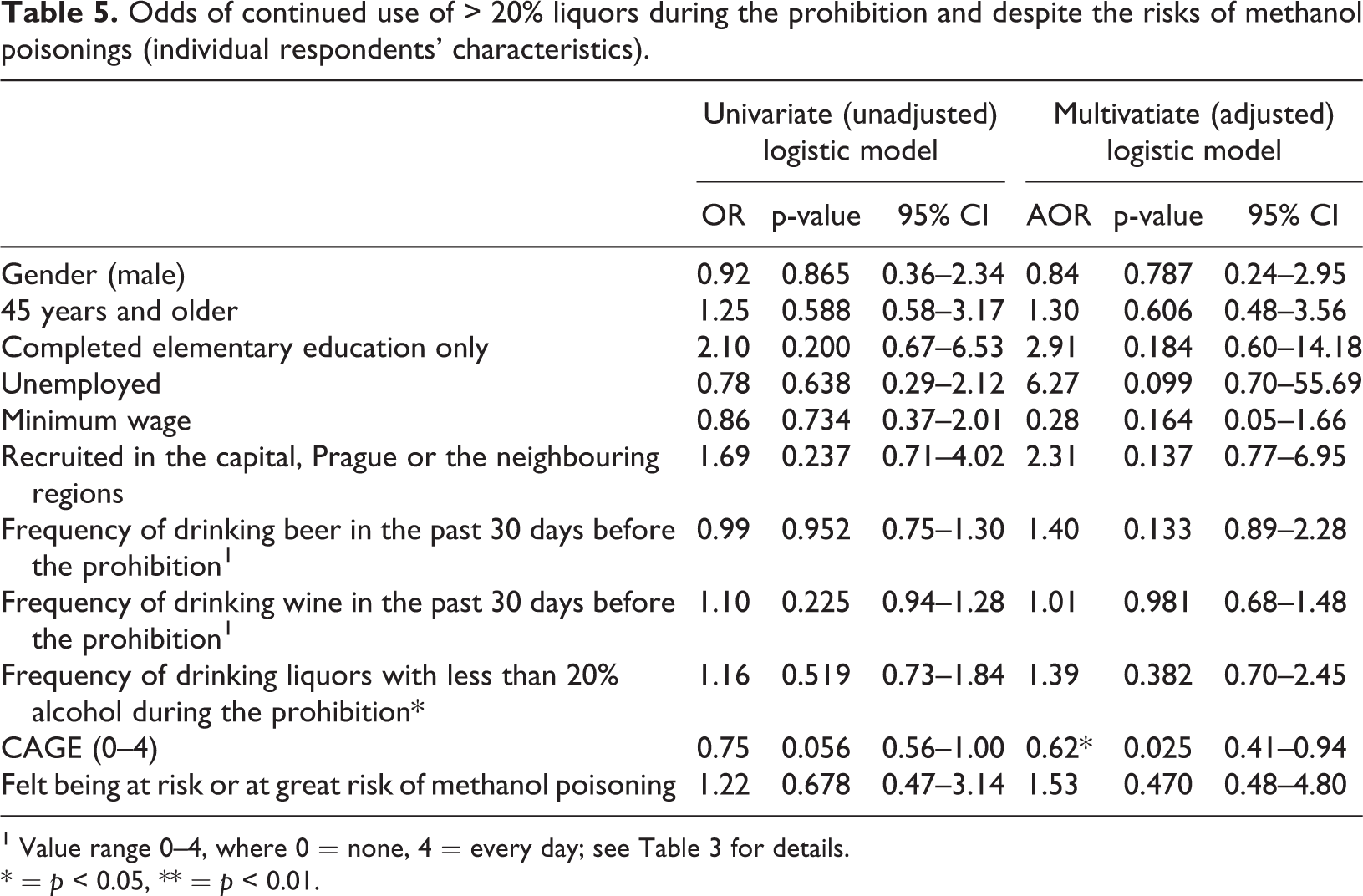
1 Value range 0–4, where 0 = none, 4 = every day; see Table 3 for details.
* = p < 0.05, ** = p < 0.01.
The differential impact the alcohol prohibition had on individuals’ lives and drinking patterns can be demonstrated by the qualitative accounts the respondents provided. Some of them acknowledged the reduction in their intake of > 20% liquors as a positive thing: “It was good; I spent less money on alcohol, my girlfriend was happy to have me home ‘un-drunk’, so fine” (male, 37 years, Usti, CAGE = 2). Others did not mind a temporary cessation of alcohol consumption, but noticed some discomfort in their social groups: “No, I had no problems. I don’t know anyone who would’ve had them. Some people complained that they can’t drink, otherwise nothing” (male, 44 years, Decin, CAGE = 2). For other respondents though, being forced to disrupt their drinking of spirits was perceived rather negatively: Yep, there’s no alcohol, and that’s a problem. What do you think there’s left in life for me? My wife left me, threw me out on the street like some kind of trash, haven’t seen my kids in years, I lost my job and got nothing. Just alcohol. And when there’s none, it sucks. (male, 56 years, Decin, CAGE = 3)
Substitution of beverage type
Abstinence from > 20% liquors did not necessarily lead to an overall reduction in the frequency of drinking. As described above, while there were no notable differences in the frequency of drinking beer and wine before and during the prohibition, the proportion of respondents who drank liquors with an alcohol content less than 20% at least once a week was about three times higher during the period of the prohibition than before it (see Table 6). This documents that, to some limited extent, the respondents may have “substituted” other types of alcoholic beverages for > 20% liquors.
Associations in frequency of beverage consumption between different beverage types before and during the prohibition.
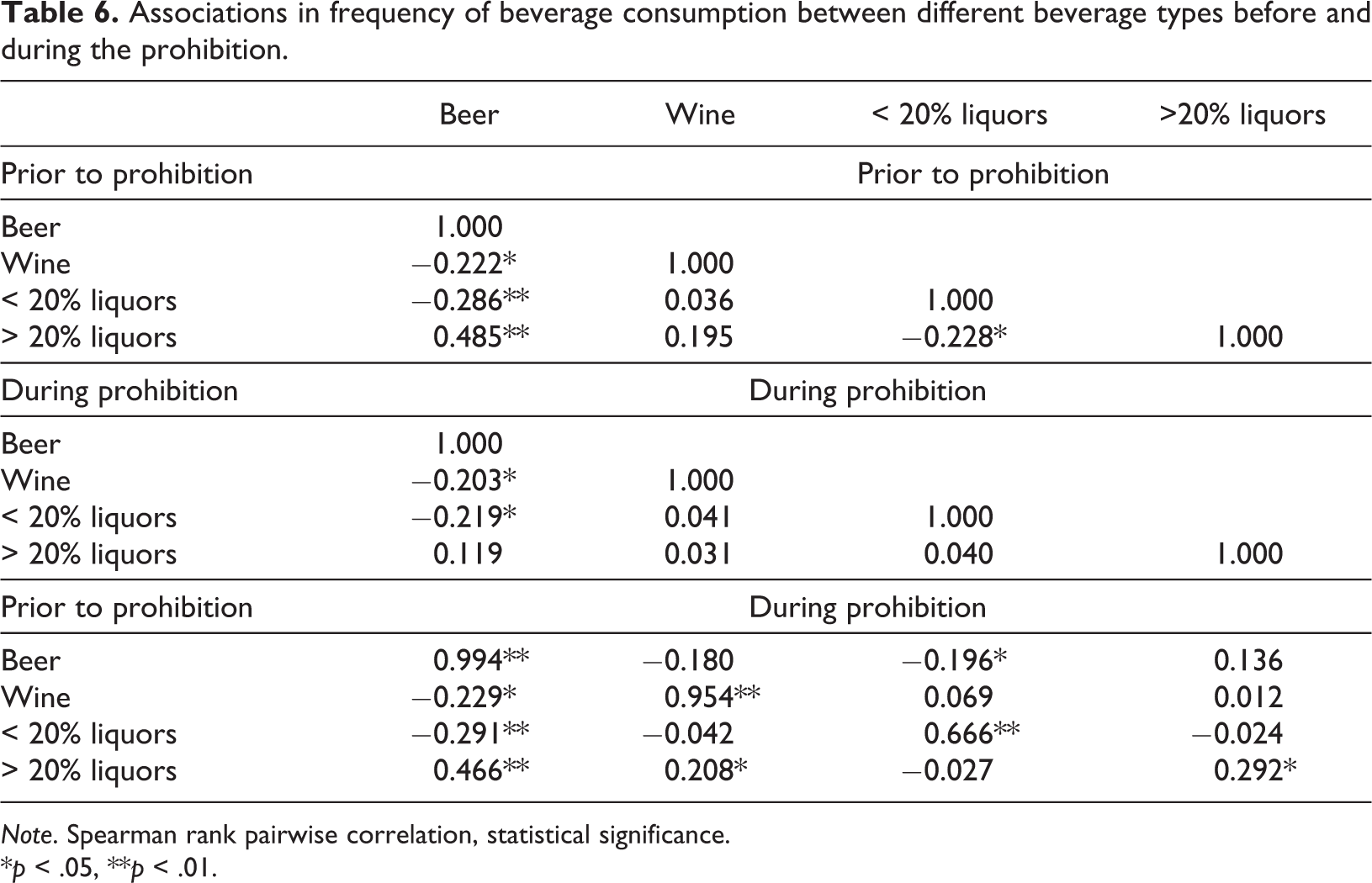
Note. Spearman rank pairwise correlation, statistical significance.
*p < .05, **p < .01.
We further looked into the correlations between drinking patterns for beer, wine, and liquors prior to and during the (“partial”) prohibition. Prior to the prohibition, the frequency of drinking > 20% liquors was significantly and strongly associated with drinking beer (r = 0.49, p < 0.01), and, to a lesser extent, with drinking wine (r = 0.20, p < 0.05). At the same time, there was a weak negative association between the frequency of drinking > 20% liquors and of drinking liquors with an alcohol content less than 20% (r = −0.23, p < 0.01). During the prohibition, the association between the frequency of drinking > 20% liquors was no longer significantly associated with the drinking of any specific beverage type in that period. When looking at the association between pre-prohibition and during prohibition drinking patterns, the frequency of drinking beer and wine was similar in the two periods (between-period r = 0.99 for beer and r = 0.95 for wine, p < 0.01). The association between drinking liquors with less than 20% alcohol content before and during prohibition was, however, lower (r = 0.67, p < 0.01); (potentially) different people drank them with different frequency in each period (see Table 6).
While the data on the frequency of drinking the different beverage types did not provide a clear indication of a substitution effect between > 20% liquors and those with an alcohol content less than 20% (< 20% liquors), the “replacement” was suggested in some of the qualitative accounts the respondents provided: “I still drank the same, it’s just that I drank what was below 20%. And I had to get more of it. At the end of the day, I looked the same as usual” (male, 63 years, Decin, CAGE = 3). Respondents who did not “fancy” these drinks would rather continue drinking beer, either because they did not “miss” > 20% liquors, or because they could not get their hands on any: “When there was nothing to drink, I drank beer. These cherry or apple liquors (with less than 20% alcohol content) are not for me. Maybe I drank a bit more beer” (male, 38 years, Decin, CAGE = 1). Increased consumption of wine occurred too, especially among rather marginalised respondents who were confined to drinking on the street: “So we go in the morning – let’s have rum? Sure, let’s get a shot…But when this started, no one was up for it…so all of us decided it would be better to go wining [drinking wine]” (male, 44 years, Havirov, CAGE = 4). Some of them commented on the negative aspects of this substitution: “When there are no spirits, I drink wine. But I have to drink more of it and it isn’t good for my stomach” (male, 43 years, Usti, CAGE = 3).
Impact of the (“partial”) prohibition on the market and resorting to “safe” sources
The staff at venues serving alcohol (bartenders, shop assistants, and entrepreneurs) reported a significant decrease in their revenues during the prohibition. The median value of the reported reduction in sales was 10% while the mean was 17%, suggesting an unequally distributed impact of the partial prohibition on different venues selling and serving alcohol. The maximum reported decrease in sales was 60%. Overall, when comparing the sales of the different beverage types before and during the prohibition, as reported by the alcohol retailers, there was a slight increase in beer sales, a notable increase in sales of < 20 % liquors and a decrease in sales of wine (all assessed to be statistically insignificant by a t test). On average, the respondents reported that the volume of daily sales of > 20% liquors prior to the prohibition was 2.65 litres a day, and nobody admitted to having sold them during the prohibition. The average volume of wine sold decreased from 6.6 litres a day prior to the prohibition to 3.8 litres a day.
The decrease in wine sales was not mirrored in the frequency of wine drinking, as reported by the study respondents. This may well reflect the fact that many respondents preferred to drink in their homes, where alcohol supplies were “unlimited”. “I had my stocks, and I still have them. I didn’t need to get it somewhere…” (male, 47 years, Ricany, CAGE = 4). However, in some cases, respondents brought their own supplies to the place where they normally went drinking (street retail outlet, pub). “Well, we brought it in. It [drinking] doesn’t taste that good, unless you drink spirits. One day I brought it over, another day Franta did…” (male, 58 years, Usti, CAGE = 1).
Those respondents who continued drinking from these sources had several beliefs about the safety of the > 20% liquors they drank: “I don’t drink these brands of alcohol that were involved. Definitely not those vodkas from street retail outlets” (male, 26 years, Havirov, CAGE = 0). Alternatively, they trusted the premises they drank at: “I don’t drink in questionable venues” (female, 28 years, Decin, CAGE = 1). An important trusted source was spirits from small distilleries: “Lately, I had this home-made plum spirit – that’s through my friend, they don’t dare put in something that would make half the village go blind. They distil it for themselves” (male, 55 years, Ricany, CAGE = 1). The impression that once a bottle had been “proven safe” by somebody else drinking from it, it was safe to drink from was also common: “I knew they had open bottles that I drank from before, so I wasn’t really afraid” (male, 32 years, Decin, CAGE = 3).
Last but not least, there were respondents who used underground sources to obtain > 20% liquors during the prohibition period, sometimes at marked-up prices. “Joe has this acquaintance who works in the alcohol business and has large stocks at home, so we bought a couple of bottles from him” (female, 25 years, Ricany, CAGE = 3). It was not uncommon to obtain > 20% liquors in familiar bars or restaurants either: “I would say something like four out of ten got around the prohibition measures and were breaking them” (male, 41 years, Prerov, CAGE = 0). For some respondents, the solution was to purchase alcohol abroad: “…people went to Slovakia to buy, a lot” (male, 39 years, Zlin, CAGE = 0).
The risk-takers in this study sometimes felt comforted by the fact that drinking ethanol after methanol can reverse the poisoning: “If anything happened, we would reverse it by drinking a plenty of ethanol anyway” (male, 44 years, Havirov, CAGE = 4).
Discussion
About one third of the alcohol users in the study drank spirits with an alcohol content > 20%, even if these were prohibited and there was a risk that the beverage could contain methanol and lead to long-term health consequences or even death. Importantly, a higher score on the CAGE assessment scale was associated with a lower likelihood of continued use of > 20% liquors during the period of the prohibition. This could be linked to the fact that those respondents with a higher CAGE score felt more at risk.
The findings of this study argue in support of previous evidence of how individuals mitigate the risks of their (potentially harmful) substance use (Howard et al., 2007; Lewis et al., 2010; Southwell, 2010; Sutfin et al., 2009). Most people engage in substance use with an understanding that they are managing the interplay between the positive effects of a drug – maximisation of pleasure – and the risks associated with administering or taking a drug – harm reduction (Southwell, 2010). It is a noteworthy finding of this study that the more problematic the drinking patterns among the respondents were according to the CAGE score, the more likely they were to feel at risk and ceased to drink spirits.
On the other hand, it gives cause for concern that those who drank in a less risky manner were not as worried about the possibility of being poisoned by methanol, and rather developed strategies that enabled them to continue their drinking from home and underground sources. Many beliefs the respondents had about the safety of their sources of > 20% liquors were unfounded and resembled the previously described practices of risk neutralisation, scapegoating, self-confidence, and risk comparison (Miller, 2005; Peretti-Watel, 2003), and as such constituted a basis for a continued public health risk.
Another myth voiced by the respondents was that if enough ethanol was consumed at the same time, the potential effects of methanol poisoning would be counter balanced. Although ethanol is an effective antidote to methanol poisoning (Zakharov, Pelclova, Navratil, et al., 2015), it fails to reduce the toxicity of methanol in cases of prolonged exposure (Paine & Dayan, 2001). Rapid assessments of the situation should contribute to the creation of adequate communication strategies which could target and debunk these “myths”.
The greatest limitation of our assessment here was that it was based on the frequency of alcohol intake rather than on the number of standard drinks or other indicators of the (increased) quantity of the alcohol consumed. This was due to the use of rather brief interview tools, which seemed adequate for a rapid field study. Another limitation of the study is the reliability of individual self-reports on drinking; in particular, if the heavy drinkers in this study underestimated their actual drinking during the period of prohibition, this may have biased our findings significantly.
Our findings speak to policy makers, who, when facing an outbreak of methanol poisonings, seek experiences from similar situations. At the same time, the partial prohibition that was adopted by policy makers to prevent methanol poisonings can, for instance, be paralleled with the processes that seek to control the availability of new psychoactive compounds that were demonstrated to be harmful (Council of the European Union, 2005; EMCDDA, 2009). It can be expected that consumers will seek to replace the risky product with its nearest substitutes – some would stay confined to the rank of what they already use, while at other times they would choose the second-best alternative. Also, underground sources will pop up, along with narratives and myths of the “safe” ways to use the substance that they do not want to give up. Ultimately, those who are most at risk as a result of their problematic use patterns are also those who will be the first to seek an alternative in an attempt to stay safe.
Nevertheless, the role of the public authorities should not be limited to controlling options, but should also involve assessing the situation, offering relevant interventions, and adopting adequate campaigning. There is strong evidence in support of brief interventions as an intervention to reduce alcohol consumption (O’Donnell et al., 2014), and it is desirable that this intervention is made broadly accessible (not only) in times of crisis.
While the outcomes of this RAR during the methanol overdose crisis in the Czech Republic in 2012 were presented at several policy meetings that aimed to develop and coordinate a response, the authorities focused their strategies exclusively on controlling the supply chain. As a result, the temporary “partial” prohibition remained the main response. The police, in coordination with the customs and the trade inspectorate, seized over 6000 litres of alcoholic beverages (MOI, 2013), and under the guidance of the Ministry of Health (MOH), almost 15,000 trade inspections were conducted, about half of them preceding the partial prohibition (MOH, 2012a). It could be hypothesised that had a stronger control of the alcohol market already been in place (e.g., a licensing system), the interventions pertaining to market control could have been implemented more efficiently.
Further on, the MOH secured the import of fomepizole to manage the acute poisonings (MOH, 2012b). Also, in December 2012, three months after the outbreak, free-of-charge testing of alcoholic beverages was provided by the regional public health agencies for about three weeks. A methanol content was found in around every eigth bottle that was brought in by the public (IDNES, 2013). Nevertheless, no preventive activities or campaigning were undertaken by the authorities either during the crisis period or after.
According to the Institute of Health Information and Statistics of the Czech Republic, an additional nine methanol poisonings were recorded in 2013 and further seven in 2014; these were on top of the total of 36 methanol fatalities that occurred in 2012. In the preceding years, methanol fatalities ranged between zero and three annually (2001–2011), and there was no significant shift in reported accidental poisonings with ethanol between 2011 (n = 165) and 2012 (n = 167) (Mravčík et al., 2016). We therefore assume that of the 16 fatalities in 2013–2014, about ten were attributable to the 2012 outbreak and, had there been effective strategies in place, these would have been preventable.
Above all, this research documents that a substantial behavioural change over a limited period of time on a (sub-)population level can occur which demonstrates the capacity of individuals to manage their substance use and make responsible choices (Peele, 2016). Our recommendations for public health interventions in this area speak to what has been referred to as a “new definition of health”, according to which individuals can adapt and self-manage in the face of social, psychological, and emotional challenges (Huber et al., 2011; Jambroes et al., 2015). Public health authorities should inform about and facilitate these decisions, more so in period of crisis than ever.
Conclusions
Our findings from the rapid assessment in venues retailing and serving alcohol suggest that the “partial” prohibition of sales of > 20% liquors during a methanol outbreak crisis can reduce their consumption, especially among those with more problematic drinking patterns. Other alcohol consumers will, however, continue drinking risky beverages, and some will shift to the nearest substitutes. Restrictions on availability may not be sufficient to prevent fatalities, especially if there are few controls on the existing alcohol market. Responses to the crises should include adequate interventions such as increased accessibility of specialist services that can assist alcohol consumers with managing their drinking and further interventions that can help them in making informed choices. An understanding of the strategies that alcohol consumers swiftly adopt in order to overcome the crisis is instrumental in this process. Campaigns and messaging which is relevant to these strategies and that can “debunk” the most common myths could prevent risky behaviour and, consequently, serious health damage or fatalities.
Footnotes
Acknowledgment
The authors would like to thank their colleagues who contributed to the data collection, and to the overall rapid implementation of the study, namely Adela Paulik-Lichkova, Jiri Brendza, Lenka Vavrincikova, Jana Bobikova, and Lenka Cablova (in memoriam).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors have declared receipt of funding from the following source: Institutional support from Programme No. PROGRES-Q06/LF.