
Abstract
The resettlement of refugees in rural areas is presenting new challenges for healthcare. This article reports on a community-based participatory research project that explored understandings of health and care across the life course in a refugee-background community in regional south-east Australia. Participants identified key challenges, including lack of access to local services that address their complex needs and problems created by communicating across languages, cultures, and ontologies. Clear opportunities were identified for improving local health services to meet the needs of refugee-background communities. Building on participant recommendations, we argue that appropriate, high-quality healthcare requires the cultivation of dialogue and respect across different understandings of health and care. We suggest that approaches grounded in an ethos of collaboration, power-sharing and dialogue provide a way forward, not just for research, but for embedding practices of cultural safety in rural and regional resettlement.
Refugee-background communities are increasingly resettling in rural and regional areas across the world, including in Australia, North America, and Europe (Schech, 2014; Wilding and Nunn, 2018; Haugen, 2019; Hudson and Sandberg, 2021). In these settings, the complex health care needs of refugee-background populations intersect with the structural disadvantage of rural and regional service provision to exacerbate existing challenges and produce new ones – for both service providers and people with refugee backgrounds (Vasey and Manderson, 2012). While the quality of health care for refugee-background populations in rural and regional Australia is generally perceived to be high, a range of barriers to appropriate, high-quality health care have been identified, including difficulty accessing services, ineffective communication, and divergent understandings of health and care (Smith, Reynish et al., 2019; Sypek et al., 2008). Existing research has tended to focus on early resettlement, and to take the working-age adult as the normative refugee-background subject. Lost in such accounts are the ways in which health and healthcare change across the resettlement period and beyond, the different experiences of people of diverse genders, sexualities, abilities, and linguistic, religious and ethnic backgrounds, and the diversity of needs and experiences across the life course. Moreover, the predominant focus on challenges and deficits in formal healthcare settings risks overlooking the knowledge, capacities, and agency of refugee-background individuals and communities in relation to their own health and care.
This study begins to address these gaps through a community-based participatory research (CBPR) project involving 52 members of the refugee-background Karen community in the regional Australian city of Bendigo – representing young men and women, mothers of young children, and elders and their carers. Using participatory tools including body maps, asset maps, and H-forms (De Jager et al., 2016; Guy and Inglis, 1999; Lightfoot et al., 2016), community members shared their understandings of what good health means, what health challenges they experience, and how well health services meet their needs. The data co-produced through this process supported existing research on the barriers to pursuing good health and appropriate, high-quality healthcare with refugee-background populations in rural and regional settings. At the same time, the dialogic, collaborative approach revealed a range of understandings and practices informed by culture and by experiences of displacement and resettlement. These situated perspectives work alongside institutional and Western biomedical approaches to shape how health is understood, how care is sought, and how both are mediated by factors including life stage, gender, and duration of settlement. The study demonstrates that successful health interventions in resettled refugee-background communities must focus not only on building the health literacy of communities but also, equally, on building the competencies of health services in understanding and integrating diverse forms of health knowledge into their practice (Nimegeer et al., 2011; Shaburdin et al., 2020).
We suggest that embedding a CBPR ethos of dialogue, collaboration, and power-sharing into healthcare practice with refugee-background populations in rural settings could support positive health outcomes by building an ‘ecology of knowledges’ that draws on the multiplicity of health knowledges that exist alongside Western science (Santos, 2014). In the process, it can contribute to tackling structural inequalities relating to both rural and regional, and refugee health. Cultural safety, an approach already widely recognised in Indigenous healthcare in Australia and New Zealand, offers a useful framework. In contrast to approaches that highlight cultural awareness or cultural competency, the concept of cultural safety opens space for consideration of more substantial questions of how to deliver care across cultural difference. This is enabled in part by the recognition that all health knowledge and practice is culturally situated, and care must be provided in recognition of and respect for ontological diversity (DeSouza, 2008; Nunesa and Louvisonb, 2020). We suggest that rural and regional settings – sharing common characteristics of relatively small communities with well-established social and professional networks (Joyce and Liamputtong, 2017) – are uniquely equipped to enact the kind of transformative change that adopting a cultural safety approach would require.
Rural and regional refugee resettlement
Resettlement is one of three durable solutions promoted by the United Nations High Commissioner for Refugees (UNHCR) in response to forced displacement, but is available to less than 1% of the world’s approximately 20 million refugees in any given year (UNHCR, 2020). The Australian Humanitarian Visa program resettles approximately 13,750 people per annum (Department of Home Affairs, 2020a), with approximately 40% resettled in regional and rural Australia (Department of Home Affairs, 2020a). This emphasis on rural and regional humanitarian resettlement reflects a broader pattern in Australia’s migration policy, in which population distribution is addressed alongside humanitarian commitments. While capital city populations continue to grow year on year, regional and rural areas have either been losing population or growing at a much slower rate. This creates problems both for metropolitan and non-metropolitan locales. Overburdened infrastructure and declining housing affordability are significant and growing problems for metropolitan centres, while population loss contributes to economic problems, labour shortages, community disruption and loss of services and infrastructure in regional towns and cities (Hugo and Harris, 2011). In this context, the Australian government has, since the mid-1990s, sought to encourage settlement in regional and rural Australia, including for humanitarian visa and onshore asylum seeker arrivals (Johnston et al., 2009; Major et al., 2013; McDonald-Wilmsen et al., 2009; Schech, 2014). Schemes encourage both primary and secondary regional resettlement, and have included ‘grants for humanitarian community services, needs-based planning and improved settlement information in regional areas’ (Johnston et al., 2009: 193).
Some local communities use resettlement funding schemes and programs to sponsor and attract new arrivals as part of community-led development processes (Boese and Phillips, 2017). It is generally hoped that, once settled outside of the capital cities, people from refugee backgrounds will remain in rural and regional Australia and expand local populations. In some cases, this appears to be successful. There is evidence that people from refugee backgrounds who come from rural areas prefer to settle in rural places (Gilhooly and Lee, 2017; Major et al., 2013). In some cases, refugee-background arrivals fill a specific employment niche that had previously been difficult to fill, allowing expansion of local businesses and industries (e.g. AMES, 2015). For others, it is the promise of a quieter life or more affordable housing that makes regional and rural settlement options attractive, encouraging them to follow family, friends and community groups in order to access better social and cultural opportunities (Mungai, 2014; Wilding and Nunn, 2018). The attitudes, practices and responses of existing community members are important, with an active welcome of new arrivals essential to good settlement outcomes (Haugen, 2019). New arrivals from refugee backgrounds also play a crucial role in the settlement process, though they are often attributed a level of passivity that denies their active role in successful settlement (Cooper et al., 2017; Major et al., 2013).
However, regional resettlement experiences are uneven across Australia, with numerous obstacles inhibiting the growth of refugee-background populations in rural and regional contexts (McDonald et al., 2009). In spite of a gradual increase in heterogeneity of populations outside of the capital cities, rural and regional Australia remains strongly associated with whiteness and racial discrimination, reducing the sense of welcome felt by some new arrivals (Radford, 2016). Furthermore, there is evidence that, more so than their metropolitan counterparts, people from refugee backgrounds in regional areas are excluded from employment, social relations and services (Correa-Velez et al., 2012). While rural communities often respond to new arrivals with a vibrant and active group of volunteers (Haugen, 2019; Sawtell et al., 2016), lack of access to ethnic-specific organisations and services can exacerbate the challenges of settlement, reducing educational opportunities, relevant language support, and access to culturally appropriate services to support health and wellbeing (Fozdar and Hartley, 2013; Major et al., 2013; Mungai, 2014).
Health and healthcare access in resettled refugee-background communities
People with refugee backgrounds form a heterogeneous population and are likely to experience different health issues based on region of origin, experience of displacement and resettlement, ethnic background, and stage in the life course. Complex health needs and poor health are commonly experienced among people with refugee backgrounds due to experiences of poor healthcare prior to and during displacement, exposure to violence and trauma, and resettlement challenges post-migration (Robertshaw et al., 2017; Sypek et al., 2008; Vasey and Manderson, 2012). Common health problems include chronic disease; tropical and communicable diseases; dental disease; micronutrient deficiencies; injuries related to torture and trauma; and chronic pain (Morris et al., 2009; Robertshaw et al., 2017; Sypek et al., 2008). In addition, issues specific to life stage include ‘persistent and pre-existing chronic health conditions’ in older populations (Smith, Hoang et al., 2020: 10); reproductive health and family planning issues for adult women (Morris et al., 2009; Riggs et al., 2017; Sypek et al., 2008); and wellbeing issues relating to resettlement stresses and intergenerational tensions among young people (Joyce and Liamputtong, 2017). Poor mental health is identified as a significant issue across all age groups and is understood to be a result of both pre-migration traumas and post-migration stresses (Morris et al., 2009; Robertshaw et al., 2017; Smith, Reynish et al., 2019).
It is well established that, in both metropolitan and rural and regional contexts, refugee-background communities face a range of practical, structural, cultural, and interpersonal barriers to accessing appropriate, high-quality healthcare, resulting in continuing inequalities (Robertshaw et al., 2017). Practical barriers to effective care include lack of transport, inability to pay out-of-pocket expenses, and the myriad stresses and responsibilities of resettlement. Inadequate understanding of systems and processes, including lack of familiarity with preventative care, can also result in under-utilisation of healthcare services. Structural barriers include appointment availability and wait times, and the short duration of appointments, which can be insufficient given complex health needs and the time required for translation. Non-continuity of care can also impede the building of trust (Morris et al., 2009; Reavy et al., 2012; Riggs et al., 2017; Robertshaw et al., 2017).
Structural disadvantage in healthcare access in rural and regional areas intersects with the issues highlighted above to exacerbate the challenges of accessing appropriate, high-quality healthcare (Joyce and Liamputtong, 2017; Smith, Reynish et al., 2019; Vasey and Manderson, 2012). In rural areas, fewer healthcare providers means that it is more difficult to get appointments, wait times are longer, and people are more likely to sustain out-of-pocket expenses. Additionally, services are likely to have fewer resources for, and experience in, addressing the complex health needs of people with refugee backgrounds, especially in relation to the mental and physical health impacts of trauma (Smith, Hoang et al., 2020; Smith, Reynish et al., 2019; Sypek et al., 2008). Transport can be particularly challenging in rural and regional contexts, both within these locations, where public transport is often limited, as well as relating to travel to major cities to access health services not available locally – a necessity that presents additional financial, practical, and wellbeing challenges (Smith, Reynish et al., 2019; Vasey and Manderson, 2012).
It is also important to acknowledge that understandings of what constitutes appropriate, high-quality care is informed by culture and experience, both for healthcare workers and those seeking care. This means that practitioner and refugee-background patient perspectives on health and care may differ considerably (DeSouza, 2008; Morris et al., 2009; Reavy et al., 2012). The normative whiteness of medical practice and bioethics means that the power to define and evaluate appropriate, effective care resides with institutions and practitioners (Mayes, 2020; Nunesa and Louvisonb, 2020; Smith, Hoang et al., 2020). It is not surprising, then, that language and communication are consistently cited as the most significant barriers to accessing and navigating healthcare for refugee-background populations in resettlement contexts, by both practitioners and people from refugee backgrounds (e.g. Morris et al., 2009; Reavy et al., 2012).
Ineffective communication contributes to patient dissatisfaction and impacts quality of care and health outcomes (Joshi et al., 2013:11). It affects all stages of the process from booking appointments, to communicating needs, receiving appropriate diagnosis and treatment, and following care instructions (Carrico et al., 2017; Morris et al., 2009). Language and communication barriers can additionally result in errors in medical files and patients having their preferences ignored or undermined (Reavy et al., 2012; Riggs et al., 2017). While interpreters are widely used to support communication, challenges frequently arise in relation to availability, medical literacy, and provision of interpreters speaking incorrect languages and dialects (Morris et al., 2009; Robertshaw et al., 2017). In rural and regional locations, language issues can be exacerbated by risks to confidentiality because interpreters and their clients are likely to share membership of small local ethnic communities. In addition, in rural contexts, there is an increased reliance on telephone interpreters, and healthcare professionals are less experienced in working with interpreters (Smith, Hoang et al., 2020; Sypek et al., 2008).
Even where there are high-quality, ethical and accurate interpreting services available, the translation of medical and health information is seldom straightforward. The need to translate across metaphysical or cultural frameworks requires not just translation of medical terminology but translation of cultural conceptualisations of bodies, minds, health and wellbeing (Davidson, 2001; Gavioli and Baraldi, 2011). At issue here is not only access to high-quality healthcare, but also recognition of other knowledges about health and illness (Santos, 2014). The ‘epistemological exclusivism’ (Nunesa and Louvisonb, 2020: 6) of Western medical knowledge, and the primacy of associated service delivery frameworks, serve to marginalise or render invisible these alternative knowledges, demanding that refugee-background service users adapt to dominant practices, regardless of their own understandings and experiences (Kokanovic et al., 2010; Shaburdin et al., 2020). Further, there is a tendency to view cultural attributes and related knowledges as ‘technical problems of practice to be overcome’ (Kokanovic et al., 2010: 521) or, worse, to treat those from minority cultural groups as non-compliant or difficult, thereby absolving healthcare practitioners of responsibility for the lack of provision of appropriate, effective, and culturally safe care (Shaburdin et al., 2020).
Lack of inclusive, culturally informed care is increasingly recognised as a significant issue in healthcare for refugee-background groups (Reavy et al., 2012; Robertshaw et al., 2017; Smith, Reynish et al., 2019), an issue that is further exacerbated by the lack of availability in rural and regional areas of healthcare practitioners with appropriate expertise in trauma-informed care. This is particularly critical in relation to the mental healthcare much needed by people with refugee backgrounds, but too often impeded by divergent cultural understandings and related stigma (Kokanovic et al., 2010; Morris et al., 2009). Low levels of cultural understanding and dialogue and associated low levels of mutual trust can affect the capacity and willingness of refugee-background service users to seek and access care and effective treatment (Carrico et al., 2017; Reavy et al., 2012; Shaburdin et al., 2020; Sypek et al., 2008). In less diverse regions and towns, and those new to resettlement, issues of cultural difference in healthcare settings, and related structural and interpersonal discrimination, can significantly compound health issues and impede care (Shaburdin et al., 2020; Smith, Reynish et al., 2019; Vasey and Manderson, 2012).
Healthy futures for Karen in Bendigo
The Karen are a religiously and linguistically diverse group whose homelands are in the mountainous border zone between Myanmar, Thailand and Laos (MacLachlan, 2012). Following British withdrawal from the region and the establishment of an independent Burma in 1948, a long-running campaign for Karen independence contributed to their persecution by the Burmese government and, ultimately, mass forced displacement into camps across the border in neighbouring Thailand (Lee, 2014). Approximately 100,000 Karen refugees currently live in these camps, including many who were born there and know no other life (Bird, 2019). There are few opportunities to earn an income, and health and education services are poor (Lee, 2014). Since 2005, Karen from these camps have sought sanctuary all over the world, including Australia (Bird, 2019).
Bendigo began resettling a small number of Karen refugees in 2007. Bendigo is a regional city located 150 kilometres north of Melbourne, Australia, on the traditional lands of the Dja Dja Wurrung and Taungarong peoples. It is an important regional commercial and service hub for central Victoria, and is the base for a regional health service administering a catchment area covering approximately a quarter of the state and including a 724-bed hospital (Bendigo Health, 2020). The City of Greater Bendigo has a population of more than 110,000, with 8% born overseas, compared to 26% nationally at the last census, and is less diverse than regional Victoria more generally (ABS, 2020).
Driven by factors including employment opportunities, rural lifestyle, and family reunion, the Karen population in Bendigo is now approximately 2500. Karen is by far the most common language other than English in the City of Greater Bendigo, spoken at home by approximately 0.8% of the population (ABS, 2020). Karen resettlement has paved the way for resettlement of other refugee-background groups, including growing communities from Afghanistan and South Sudan. Bendigo Community Health Services (BCHS) is contracted to deliver the Australian government’s Humanitarian Settlement Program (HSP), which provides support to refugees during the first 6 to 18 months of resettlement, including in relation to housing, health, language, education and employment (Department of Home Affairs, 2020b). Karen settlement in Bendigo has been characterised by mutual goodwill between Karen settlers and long-term locals, and a widely shared desire to collaborate in the production of a positive multicultural future for Bendigo. Challenges remain, however, including in relation to language acquisition, skilled employment, and health outcomes. More generally, entrenched hierarchies of power continue to present barriers to belonging. The Karen are still often regarded as new arrivals, and as beneficiaries of Bendigo’s humanitarianism, rather than as active agents and contributors to the local community; a perception perpetuated by a tendency in the Karen community to publicly present an image of gratitude and deference to the people of Bendigo.
Community-based participatory research
The research reported in this article emerged out of ongoing collaborations between university-based researchers, health services in Bendigo, and the local Karen community, which have, to date, explored resettlement, youth belonging, aged care, and maternal and child health (McKinnon, 2020; Nunn, 2018; Wilding and Nunn, 2016; Wilding, Baldassar et al., 2020). With increasing numbers of Karen people transitioning from the HSP to mainstream services, BCHS were concerned by low levels of help seeking behaviour, alongside continuing health and wellbeing challenges. There was also concern about the capacity of mainstream services to respond effectively and appropriately to Karen service users in light of their cultural difference to the wider Bendigo population and their refugee experiences.
In the context of rural and regional resettlement, refugee-background communities and the local health sector are both relatively small and are engaged in complex relations of interdependency. Given the challenges of divergent understandings of health and care, communication barriers, and power inequalities in mediating service engagement and health outcomes for refugee-background populations, it was critical to utilise a research approach that attended seriously to the knowledge and experiences of the Karen community, in addition to addressing the needs of the health sector. This was achieved through a CBPR approach, in which both BCHS and members of the Karen community contributed to co-producing the research.
Community-based participatory research (CBPR) is an approach to research in which academic researchers and community stakeholders collaborate in designing and implementing research with the aim of applying findings to benefit the community (Bell and Pahl, 2018; Drahota et al., 2016; Jagosh et al., 2015). CBPR is grounded in an ethos of sharing power and resources, and co-learning (Banks et al., 2013; Beckett et al., 2018; Drahota et al., 2016). It utilises community strengths and values community knowledge, and is guided by an ‘explicit commitment to ensuring research leads to, and is informed by, action’ (Banks et al., 2013: 264). CBPR is additionally understood to have instrumental value in ensuring that research and the actions that emerge from it are relevant, appropriate and sustainable (Drahota et al., 2016; Gibbes and Skop, 2020; Jagosh et al., 2015). CBPR is highly appropriate for researching with refugee-background communities as it is a strengths-based approach that honours agency and autonomy, in contrast to common experiences of vulnerability and disempowerment during forced migration and resettlement. Moreover, in a health context, co-producing knowledge with refugee-background community members shifts the focus from service provision and the dominant biomedical model of health and care to attend to affective, cultural, social, and migration-related determinants of health. In doing so, it supports the implementation of culturally and experientially appropriate interventions (Beckett et al., 2018; Culhane-Pera et al., 2010; Gibbes and Skop, 2020).
The success of CBPR is reliant on relations of trust and respect, shared interests, and clear communication, while excessive financial burdens and time commitments, and a lack of shared understanding can undermine the process (Drahota et al., 2016). CBPR aspires to equal partnerships between academic and community co-researchers, however, entrenched power dynamics, relational complexities, and financial and temporal constraints mean that this ideal is rarely fully realised (Banks et al., 2013; Drahota et al., 20016; Gibbes and Skop, 2020). Similarly, the realpolitik of policy and practice often impedes CBPR’s transformative potential (Beckett et al., 2018; Bell and Pahl, 2018).
Methods
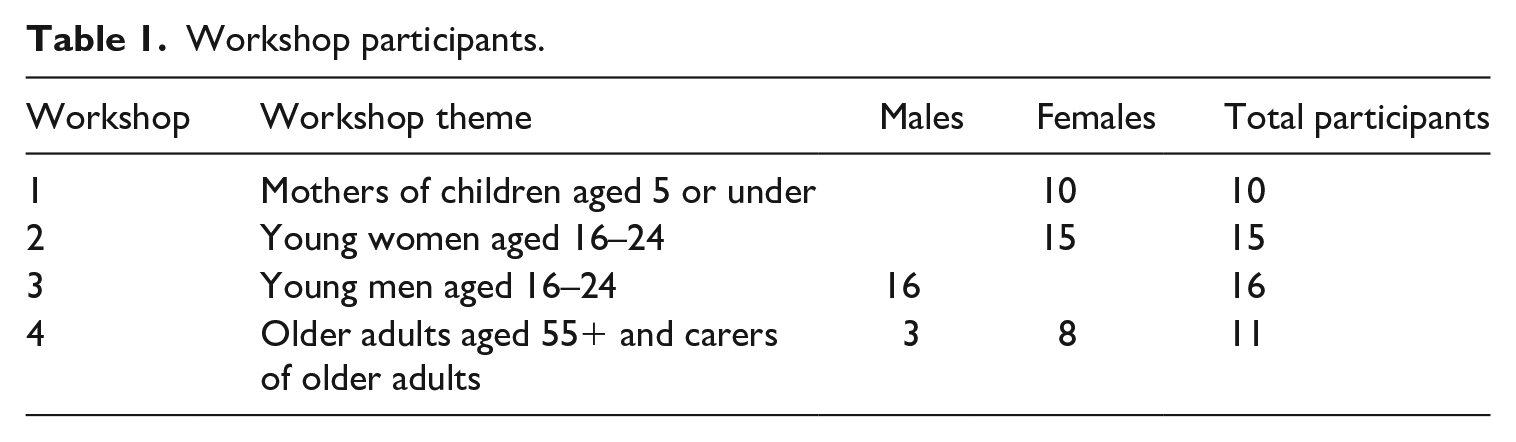
‘Healthy Futures for Karen in Bendigo’ project research was conducted in late 2019, involving 52 members of Bendigo’s Karen community. Attending to the diversity of experiences and perspectives across gender and life stage, separate workshops were conducted with four groups likely to experience distinct health and healthcare challenges: older adults and their carers, mothers of young children, young men, and young women (see Table 1). Participants had resided in Bendigo for between six months and ten years.
Workshop participants.
The project embedded several levels of community participation. BCHS informed the development and implementation of the research and shared in disseminating findings in the Bendigo health sector, while three bilingual members of the Karen community were employed as research assistants, informing the design of the project, recruiting participants, facilitating the workshops, and contributing to analysis and dissemination. In the workshops, data was collaboratively generated using research tools drawn from CBPR and community development approaches that facilitated reflection and dialogue, and focused on the knowledge and capacities of participants. The strengths of this multifaceted CBPR approach included involving those, such as BCHS, with the power to implement change (Beckett et al., 2018), and providing training and career opportunities for Karen research assistants and remunerating them for their work (Bell and Pahl, 2018; Jagosh et al., 2015). Another strength was that the workshops could engage with a wide range of community members, beyond the gatekeepers who often speak on behalf of the community but do not always represent the diversity of their experiences (Gibbes and Skop, 2020). While the participatory workshop approach limited our ability to capture some of the diversity within life-stage and gender cohorts, it was critical for capturing the shared knowledges and practices within and across these groups that have emerged through collective cultural and political histories, and which offer both a critique of and alternatives to existing healthcare practices (Banks et al., 2013; Nunesa and Louvisonb, 2020).
Participants were supported to attend workshops by Karen research assistants. Workshops were conducted on mats laid across the floor in an effort to replicate familiar settings for meeting and discussion in the Karen community, and familiar Karen food was provided by a local community member. In each workshop, participatory tools including body mapping (De Jager et al., 2016), asset mapping (Lightfoot et al., 2016) and H-form diagrams (Guy and Inglis, 1999) were employed with accompanying group discussion (conducted in Po and Sgaw dialects of Karen and/or English depending on individual and group preferences) to address the following questions: (1) What is good health? (2) What are the biggest health challenges facing people in your life-stage/gender cohort? (3) What resources do people draw on to address these challenges? (4) How well are health and wellbeing needs being met by healthcare service providers? And (5) what could be done to improve things? The research tools were selected for their capacity to both capture individual perspectives and experiences and to support collective knowledge production. Workshops were audio and video recorded with participant consent and subsequently translated and transcribed by research assistants and university-based researchers. University-based researchers conducted initial thematic analysis of the data, and then worked with Karen research assistants who confirmed, corrected, and added to findings.
Findings
Perceptions of what is meant by good health were consistent across all of the workshop groups. They were also largely inconsistent with the biomedical model of health in which Australian healthcare professionals are trained. While the biomedical model focuses on the ‘normal’ functioning of the physical body (Clarke et al., 2010), Karen participants emphasised an experience that best translates into English as being ‘happy’, drawing attention to the intersection of multiple factors in health and wellbeing. These included physical attributes, such as the absence of pain, feeling strong and energetic, and looking ‘fresh’, with clear skin and eyes. It also included social factors such as feeling able to participate in the activities of daily life, including communicating with others, enjoying going out with friends, contributing to the community, practising driving or other skills, playing sport, cooking and cleaning (particularly for those in the parent cohort), and attending work and school (for younger participants). In addition, participants drew attention to the emotional aspects of health and wellbeing. Being healthy means feeling the relative absence of worries and pressure, feeling optimistic about the future, maintaining happy thoughts and sharing thoughts and feelings with others in an open way.
The barriers to good health were similarly understood as multidimensional. While physical conditions and illnesses were recognised as factors, they were not the only issues that people considered when evaluating the sources of poor health. Equally important were factors such as lack of access to good food, weather extremes such as heat, cold or rain, and a lack of ‘da hu da por’, a Karen concept that loosely translates as ‘belonging’, ‘unity’, ‘mutual understanding’ and/or ‘connection with a social group’. The most common and serious health concern, emphasised across all workshops, was tha ta cha. While this translates literally as ‘disease of the heart’, and can refer to the physical condition of heart disease, it also refers to a sense of dis-ease in the world and of emotional heartache. Thus, tha ta cha is recognised in people who are experiencing significant pressures, who have been thinking too much about their worries, or who are perceived as less resilient. When a person is experiencing tha ta cha, others are encouraged to be especially gentle, kind and supportive with them in acknowledgement of their vulnerable condition. Tha ta cha – as well as the absence of da hu da por in family or community – was often attributed to resettlement-related issues that were life-stage specific. Older adults and carers, for example, discussed issues of loneliness and social isolation, while younger people experienced pressure to succeed in education and employment, and to support their families. For young men, alcohol and drugs were seen as both a cause of tha ta cha and a way of coping with it. The stresses of family conflict and financial worries emerged across all life stages.
Perceptions of access to local health services reflected culturally and historically situated conceptualisations of health and illness. Access to healthcare in Bendigo was considered a vast improvement on people’s lives in the refugee camps. Mothers, for example, reported much better antenatal and postnatal care in the Australian context. However, many workshop participants also experienced significant social and emotional issues that they felt were not adequately addressed through biomedical care. Particularly for older adults, barriers to communication and an associated poor sense of belonging caused significant concern. This emerged in discussions of not being able to understand referral letters, negotiate telephone booking systems, or locate services in unfamiliar parts of the city or within large buildings. During appointments many participants across all age cohorts were concerned that their symptoms were not well understood by doctors, and that the medicines prescribed were not effective, reflecting a gap between participants’ culturally situated understandings of health and the biomedical system in which they were required to seek treatment.
In all four workshops, it was clear that biomedical service provision was only one part of a complex web of relations and resources that people drew on in the pursuit of good health and effective care. Indeed, across all life stages it was common for Karen people only to seek professional healthcare for severe or persistent symptoms. Other, more commonly accessed resources included over-the-counter treatments such as paracetamol and vitamins, self-care, such as exercising and sleeping well, medications and herbs learned about and/or purchased in Thailand and Burma, and religious practices such as prayer and meditation. Overwhelmingly, however, the most significant resource for advice, assistance and care was community. This included family and friends, religious communities and leaders, multicultural and refugee services, community and ethnic organisations, and education institutions. The wide range of individuals, organisations, and institutions – both Karen and non-Karen – that participants felt comfortable accessing reflects the strong networks of support available to many Karen people in Bendigo. It also suggests a potential strength of rural and regional resettlement locations, where the small-scale, highly networked services, and strong culture of volunteerism and community-mindedness can reduce the risk of isolation. At the same time, these characteristics present potential risks to young people who at times felt highly visible and stigmatised in seeking support – especially for mental health-related issues.
Asked to suggest solutions to improve healthcare services, participants expressed a strong desire for healthcare providers to not only understand what it means to be Karen and from a refugee background, but to be willing to engage in culturally appropriate ways with the healthcare concerns that were being raised (Smith, Reynish et al., 2019). The most common suggestions for achieving this goal included providing longer consultation sessions, better interpreters, culturally significant and welcoming symbols and practices, and/or having Karen-background healthcare providers. Another suggestion was to provide cultural literacy and refugee awareness programs for healthcare providers. Many of the issues raised around access and availability of services echo findings from other studies (e.g. Joshi et al., 2013; Robertshaw et al., 2017; Sypek et al., 2008). What these suggestions cannot address, however, is the need for a deeper appreciation of Karen epistemologies of health that became evident in discussions of terms such as tha ta cha and da hu da por. As highlighted earlier, Western biomedicine has been accused of a tendency towards (at best) ‘epistemological exclusivism’ (Nunesa and Louvisonb, 2020: 6) and (at worst) epistemicide (Santos, 2014) against diverse health and medical knowledges. To create healthcare contexts that meaningfully attend to the health concerns of Karen people and offer more culturally appropriate care, in our view, requires a capacity to traverse ontological difference with the aim of ensuring what has been usefully referred to elsewhere as ‘cultural safety’ (DeSouza, 2008).
A participatory approach to enhancing health: the role of cultural safety
There is growing recognition that diverse ontologies are a feature of care environments (Mol, 2008). This is particularly acute in cross-cultural care settings (Dombroski, 2018; McKinnon et al., 2019). Traversing ontological difference in order to provide appropriate, high-quality care requires an ongoing, two-way process of communication and understanding that transcends linguistic barriers to engage with differing cultural conceptions of health and care (Morris et al., 2009; Reavy et al., 2012). In Bendigo, some healthcare providers, including BCHS, have introduced resources to inform staff about Karen history and culture, and are using translators or providing information sheets written in Karen language. Research conducted with Bendigo Health also reveals that some efforts are being made to support hospital staff to improve cultural competency skills (McKinnon, 2020). However, engaging across ontological differences, and the diverse forms of health knowledge that come with them, remains a challenge.
One framework that provides an approach for working across diverse ontologies is cultural safety (DeSouza, 2008). Developed originally by Maori nurses, and increasingly applied in relation to Aboriginal and Torres Strait Islander communities in Australia, cultural safety is defined by Williams (1999: 214) as: an environment, which is safe for people; where there is no assault, challenge or denial of their identity, of who they are and what they need. It is about shared respect, shared meaning, shared knowledge and experience of learning together with dignity, and truly listening.
Cultural safety goes beyond cultural competence – with its focus on learning aspects of a patient’s culture – to recognise both patients and healthcare workers as bearers of culture and to render visible the normative whiteness of the healthcare system and the unequal power relations that perpetuate it (DeSouza, 2008; Mayes, 2020; Nunesa and Louvisonb, 2020). Cultural safety seeks to confront and address entrenched inequalities through dialogue, collaboration, and reflexive practice (DeSouza, 2008; Reavy et al., 2012).
A cultural safety approach has significant transformative potential for healthcare for refugee-background communities in rural and regional settings, by providing a framework for engaging with the range of challenges outlined above, including divergent understandings of health and care, ineffective communication, lack of trust, and discrimination. Moreover, rather than creating ‘a checklist mentality that essentialises group members’, as cultural competency approaches risk doing (DeSouza, 2008: 129), cultural safety recognises culture as diverse and dynamic, accommodating different orientations to culture within and between refugee-background communities, including across life stages, and throughout the resettlement process (Reavy et al., 2012). It also has the potential to foster reflexive, inclusive care in rural and regional resettlement contexts where there is limited experience and skill in intercultural care (McKinnon, 2020), and where the prevalence of a white rural imaginary that centres Anglo-Australian people and culture often serves to marginalise and exclude those who are non-white and non-Western (Edgeworth, 2015).
The methodology adopted in this research presented an important opportunity to explore strategies for sharing Karen knowledge and promoting cultural safety. Conducted as a partnership between academic researchers, a refugee resettlement and community health service, and participants and co-researchers from the Karen community, the project initiated a process of shared learning and co-production of knowledges of health and care. This process fed into a series of outputs, including a report to summarise findings, a ‘tip sheet’ to communicate key recommendations and key Karen health concepts to local health services, and two short videos in Karen language to summarise project findings and healthcare responses for members of the Karen community (Wilding, Gamage et al., 2020a, 2020b; Wilding, McKinnon et al., 2020). The CBPR approach applied in this project demonstrated the potential for collaborative and dialogic approaches to create a safe space in which an ecology of diverse and divergent healthcare knowledges can be developed and honoured. There are, however, important challenges. Key among these is the responsibility placed on Karen people employed by research organisations or health services, who are critical to the effective and ethical navigation between languages and cultures but who, by virtue of their translational capacities – and their resulting employment – are ambiguously and dynamically positioned between health/research and community perspectives (Banks et al., 2013).
The strength of a cultural safety approach is that it can be applied across all service user cohorts – both refugee and non-refugee background. It does not need to be learned anew for each new wave of settlers. It does, however, require something more significant: the transformation of the ethos and practice of healthcare. Further work is needed with local healthcare service providers to understand how a cultural safety approach might be integrated into practice, and the capacity building and resources that are required to facilitate new dialogic and power-sharing processes. Our findings suggest that to initiate such an approach will require work to disrupt existing power hierarchies and entrenched communicative practices, and allow a more diverse set of health knowledges to be acknowledged and respected. The small-scale and highly networked nature of rural and regional towns may well support the realisation of this transformative potential. This is particularly the case in Bendigo, where the unique positioning of BCHS as both a healthcare and settlement service provider presents the possibility of a whole-of-sector – indeed, whole of city – approach. Despite the challenges of refugee healthcare in rural and regional settings, these resettlement sites have the potential to become leaders in culturally safe healthcare, and through this ethos and practice contribute to reimagining and reconfiguring relations in rural and regional cities and towns.
Footnotes
Acknowledgements
The authors would like to thank all of the Karen community members who contributed to this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the Manchester Metropolitan University – La Trobe University Collaborative Project Grant Scheme, 2019.
Author biographies
![]()
![]()