
Abstract
The aims of this study were to measure changes in the health of social housing tenants and to estimate indicative health effects associated with changes in exposure to indoor air pollutants (IAPs) following a deep energy retrofit (DER). To this end, a pre–post retrofit design was employed to explore the direct and indirect effects of DER over time, including a health questionnaire completed by residents and indoor air quality measurements in homes. Burden of disease estimates (rate per 100,000) for DER homes were estimated by extrapolating IAP measurements collected pre- and post-retrofit in 14 homes. No changes in health outcomes (i.e. respiratory health and health-related quality of life) or healthcare costs as measured by the questionnaire were observed six months post-retrofit. An increase in median IAP concentrations post-retrofit resulted in an overall net negative effect on health outcomes. Our results demonstrate the importance of occupant behaviours such as tobacco smoking and/or under ventilation (due to blocked wall vents) on exposure to PM2.5 and the resulting health outcomes. The mixed method approach employed to evaluate the impact of DER facilitates a more nuanced understanding of DER's effects.
Introduction
In recent years, there has been significant demand for sustainable, energy-efficient housing solutions, driven by the need to address climate change and carbon emission targets. The revised European Energy Performance of Buildings Directive (EPBD) establishes a framework for entirely decarbonising buildings and maximising energy efficiency, while also addressing the health and wellbeing of building users. 1 The EU Renovation Wave, an initiative under the European Green Deal aims to renovate 35 million homes across Europe by 2030, while also addressing energy poverty, which is estimated to impact almost 50 million Europeans.2,3 Energy renovation can significantly alleviate financial burdens on lower-income households and reduce energy waste.4,5 A comparative analysis conducted across 17 European countries suggested that implementing EU common policies on energy poverty awareness, renovations and energy taxation would help energy-poor households overcome energy poverty. 6 Yet, it is crucial to tailor actions based on specific regional-based poverty patterns to develop targeted and impactful strategies for addressing energy poverty and associated health inequalities while adhering to key climate milestones and initiatives. 6
The re-cast EPBD proposes that deep energy retrofits (DERs) be defined as a ‘renovation that transforms building into nearly-zero buildings’. 1 Over the past decade, there has been a notable shift towards DER measures driven by increased targets to achieve energy efficiency. DERs aim to achieve substantial reductions in overall energy consumption through adoption of building fabric insulation upgrades and improved ventilation and heating systems. 7
DERs can improve indoor environmental quality, including thermal comfort (TC) and indoor air quality (IAQ). Improving insulation, upgrading windows and optimising heating, ventilation and air conditioning systems, has been shown to positively impact TC in educational,8,9 occupational 10 and residential buildings. 11 Enhancing TC through DER also plays a pivotal role in promoting occupant health and well-being and therefore potentially lowering healthcare usage and costs. For example, a recent review by Fisk et al. 12 indicates that along with subjective improvements in TC, energy retrofits can also lead to positive effects on general health, mental well-being and respiratory health (excluding asthma), suggesting broad health benefits associated with DERs. Interventions that primarily involve home insulation upgrades have been shown to reduce the risk of chronic respiratory health outcomes, such as chronic obstructive pulmonary disease, asthma and pulmonary hypertension. 13 A retrospective cohort study involving over 200,000 New Zealand homes reported a statistically significant lower relative risk of chronic respiratory disease amongst occupants of homes that received insulation measures compared with a control group. 13 More recently the Irish Government's ‘Warmth and Wellbeing’ pilot study (2016–2020), showed that installing energy efficient measures in the homes of people with chronic respiratory conditions had a positive impact on the general and respiratory health and comfort of participants at least two years post-retrofit. Along with improved TC, participants reported a reduction in visits to healthcare services, higher satisfaction with temperature control in the home and improved ability to meet fuel bills. 14
The link between DER and health is somewhat complex because indoor residential environments contain a complicated array of indoor pollutants. The World Health Organization has highlighted several key indoor pollutants for health, including radon, formaldehyde, particulate matter (PM2.5), nitrogen dioxide (NO2) and microbial pollutants arising from the presence of damp and mould and many more. 15 It is estimated that one in every six homes in the European Economic Area is impacted by dampness, 16 with recent research indicating that pre-birth and/or early childhood exposure to environmental factors such as dampness-related allergens plays an important role in the development of allergic rhinitis, 17 childhood asthma 18 and pneumonia. 19 Exposure to indoor air pollutants (IAPs), like PM2.5, have been linked to adverse health effects, including respiratory, cardiovascular and cerebrovascular issues. 20 Logue et al. 21 estimated the cumulative health impacts from inhalation of IAPs on U.S. residences to be in the order of 400–1100 disability adjusted life years (DALYs) lost annually per 100,000 inhabitants with pollutants such as PM2.5, acrolein and formaldehyde accounting for the vast majority of DALYs. Similarly, Morantes et al. 22 compared the chronic harm caused by IAPs, and identified the most harmful IAPs contributing over 99% of the total median harm of 2200 DALYs/105/year as particulate matter (i.e. PM2.5, PM10), NO2, formaldehyde, radon and ozone.
Hamilton et al. 23 modelled the health impacts of energy efficiency interventions on English homes and concluded that the net positive impact of retrofitting for population health outweighs the potential negative health impacts associated with increased exposure to IAPs, as long as ventilation has been considered as part of the retrofit process. The Irish ‘Warmth and Wellbeing’ pilot study 14 also investigated the likely impacts (using model predictions) of home energy efficient measures on mortality risk due to changes in temperature and exposure to PM2.5, radon and second-hand tobacco smoke. Again, like Hamilton et al., 23 their results also highlighted the importance of good ventilation for ensuring good IAQ. 14 In the presence of purpose provided ventilation the model predicted reduced exposure to indoor-generated pollutants such as PM2.5, and an estimated reduction of almost 6000 cardiopulmonary disease deaths per 100,000 population over 30 years. However, the study called for more empirical data, and future evaluations of energy efficiency renovations to look at and assess ventilation, IAQ, and ambient air quality impacts. 14
Notably, findings from other studies regarding pollutant levels following energy renovation are mixed, with some studies reporting elevated levels12,24–26 and others showing no change or a reductions.12,27 For example, Yang et al. 28 found that differences in pollutant levels, (including radon, formaldehyde and total volatile organic compounds) were dependent on the type of retrofit, with green-certified Minergie buildings showing lower pollutant levels compared to energy-renovated dwellings. Ventilation practices following retrofit also differed significantly, depending on the presence of mechanical ventilation in Minergie homes, versus natural ventilation in energy-renovated dwellings. Previous research11,24,29 on DERs in Irish residential buildings emphasises the critical importance of properly installing and maintaining ventilation systems, alongside the need for adequate information for residents to encourage compliance with desired behaviours around DER measures and their health-associated benefits. These studies noted the significant impact of occupants’ behaviours, such as using open fires, burning candles or smoking, on pollutant levels post-retrofit, particularly PM2.5 aligning with previous findings.30,31 As DERs can create healthier indoor environments and promote occupants’ well-being by optimising ventilation and minimising indoor pollutants, it is recommended to integrate IAQ assessments into DER interventions.
Due to the acceleration of the EU renovation wave and increased focus on indoor environmental exposures and sustainability research, the urgency to understand the health burden of pollutant exposure and how this may be impacted by DER has increased. Ireland is a useful case study to explore this link for several reasons. Ireland has set an ambitious target to retrofit 500,000 residential homes to Building Energy Rating (BER) B2 by 2030. 32 However, retrofitting activity has been relatively slow, averaging 23,000 retrofit projects (the majority which were shallow) per year from 2013 to 2019. 33 More recent figures suggest that while the retrofitting programme is gaining pace, the 2030 BER B2 target may still be missed. 34 Additionally, in 2021 Ireland ranked second to last amongst the EU-28 in efforts to decarbonise heating, largely due to the dispersed density of dwellings reducing the efficiency of retrofitting multiple houses together. 35 Fuel poverty, typically defined as the inability to financially afford an acceptable level of warmth, has been on the rise in Ireland, with 5–15% of households having problems providing a sufficient level of heat in their homes, in the face of rising energy costs. 36 This situation is particularly concerning due to well-reported health associations, including increased risk of cardiovascular and respiratory disorders, alongside adverse effects on mental well-being.37–39 Liddel and Morris’ 40 review importantly observes that multidisciplinary research which expands its focus outside just physical health and clinical outcomes in the context of fuel poverty is essential to efficiently tackle this global issue.
By investigating health outcomes related to changes in key pollutant exposures post-retrofit, alongside analysing subjective health measures and examining health service use and related costs, this research contributes valuable insights into the health impact of DERs. Conducting such multi-disciplinary research in Irish social housing provides much-needed contextual information that can inform the national retrofit programme, which along with reducing greenhouse gas emissions can also potentially alleviate energy poverty and improve occupants’ health and well-being. 41 Therefore, the aims of this study, the Health Impact Assessment of Energy Renovations on Irish Domestic Dwellings (HAVEN) were to measure the changes in the health of occupants in social housing following a DER and to estimate the health burden due to the changes in exposure to IAPs. HAVEN contributes to the knowledge in this area through the holistic evaluation of DER retrofit interventions, paving the way for more informed and health-oriented building retrofit strategies for social housing in Ireland and beyond.
Methodology
Study design
This study employed a mixed-methods, pre–post retrofit design to explore the direct and indirect effects of DER over time. Initially, a pre-retrofit questionnaire was employed to assess general and respiratory health and health service usage to establish baseline levels. Following the retrofit process, a post-retrofit questionnaire re-assessed the same health and health service usage variables. A pre–post data analysis of these measures examined the short-term (six months) effects of DERs. In addition, pre- and post-surveying of IAQ within a small sample of 14 homes was conducted to measure exposure to key pollutants (formaldehyde, radon and PM2.5). 29 The objective IAQ measurements informed the health impact assessment (HIA) component of the study, which estimated health burdens due to the change in exposure to the three IAPs.
Recruitment commenced in August 2020, in collaboration with Local Authorities, Approved Housing Bodies and private retrofit companies. These organisations identified suitable homes and disseminated study recruitment materials to potential participants. Eligibility criteria required participants to be involved in a planned energy retrofit which would achieve a post-retrofit minimum BER of B2 or its cost-optimal equivalent. The primary contact in each home had to be at least 18 years of age. All participants underwent a thorough informed consent process before data collection began. Ethical approval for the study was provided by the University of Galway's Research Ethics Committee (No. 2020.03.009).
Data collection
Health questionnaire.
Participants provided information pertaining to their overall health, respiratory symptoms and medical diagnoses, using a paper-based questionnaire at both the pre- and post-retrofit stage. The health questionnaire (HQ) included questions about conditions such as asthma, eczema, nasal allergies and instances of Covid-19 within the preceding six months. General respiratory symptoms were also examined, including wheezing and phlegm attacks over the same period, with responses recorded as ‘yes’ or ‘no.’ The SF-36 was used to assess health-related quality of life. This instrument yields summary scores for both physical (PCS) and mental (MCS) health components, with higher scores indicating better health functioning. Scores typically ranged from 20 to 60, with a mean score of 50 considered the ‘norm’ within general populations. 42 To assess healthcare utilisation and medication costs, an adapted version of the Clients Services Receipt Inventory was employed. 43 The study employed Irish data on healthcare costs to provide cost estimates of healthcare service use (see Table 1). Data on medication costs was retrieved from the HSE PCRS database. 48 All reported Unit Cost data used 2019 prices using the medical component of the consumer price index. 49
Irish healthcare costing.
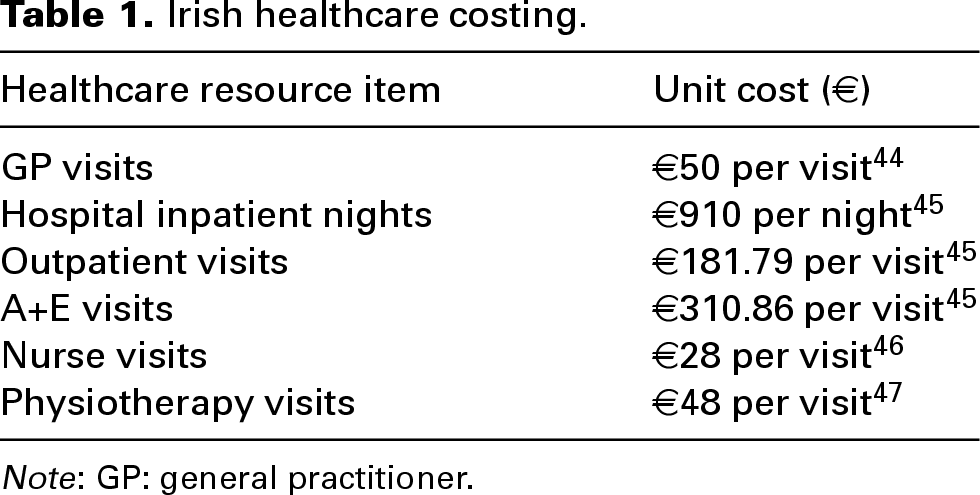
Note: GP: general practitioner.
Health impact assessment.
Estimated health burdens due to the change in exposure to three IAPs (PM2.5, formaldehyde and radon) following a DER were calculated. The HIA methodology involved combining information on the following: (i) measured IAP concentrations (collected in the main bedroom and living area of participant homes pre- and post-retrofit), (ii) the incremental risk to health from exposure to a certain pollutant, (iii) estimated target population, and (iv) background rate of disease (for morbidity or mortality). We used Irish population and background rates of disease data for the year 2019 as this was the most recent year where rates of health outcomes were unaffected by the COVID-19 pandemic. Figure 1 illustrates a schematic of the methodology employed to estimate the health burden. The input data was sourced from various national and international sources.
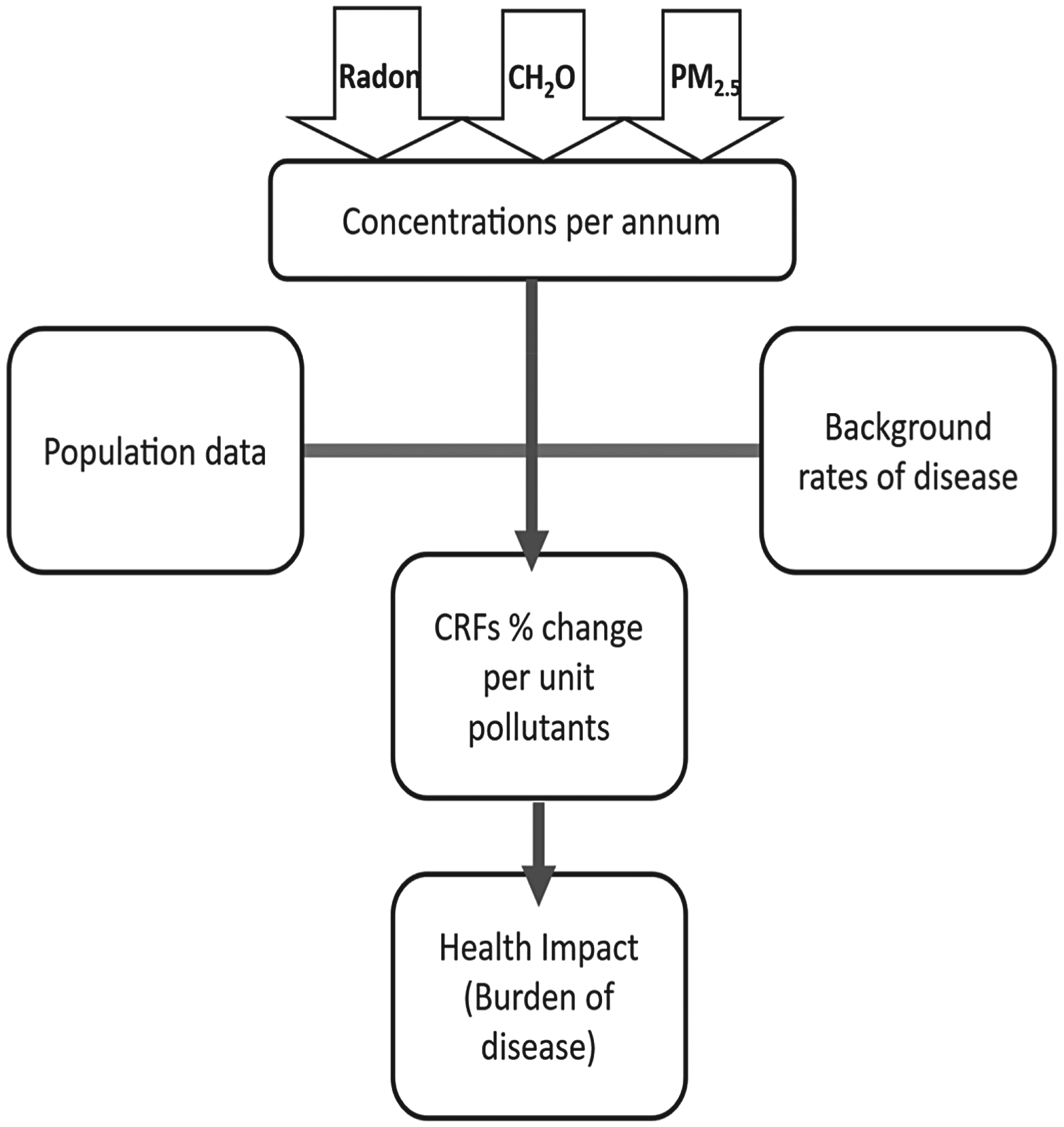
Schematic flow chart of the health burden calculations.
Exposure concentrations were estimated from a limited programme of measurements for PM2.5 and formaldehyde (pre-and post-retrofit) across 14 homes. 30 In addition, post-retrofit radon measurements were available for 18 homes, with pre-retrofit data available for only six of those homes. Estimates of pre-retrofit indoor radon concentrations for the 12 homes where pre-radon data was not collected were extracted using Q-GIS software from the average indoor radon concentrations by electoral division (Ireland's smallest administrative area) as defined by Elio et al. 50 In homes (n = 4) where pre-retrofit exposure concentrations for formaldehyde were unavailable, estimates were made using measured data from previous studies in Irish homes with similar energy profiles.11,24,29 Further details regarding the exposure data from the HAVEN study, used to estimate health burden, including how the exposure data was collected and analysed can be obtained in Coggins et al. 29
For PM2.5, a time-weighted average of the 24-h average concentration was calculated for each home using the expected occupancy times in the measured rooms (i.e. living rooms during daytime between 7 a.m. – 10 p.m., and bedrooms during night-time (10 p.m.–7 a.m.). As the study was examining the impact due to indoor sources only, the PM2.5 concentrations were adjusted to exclude outdoor PM2.5 due to infiltration, assuming an infiltration rate (I/O) of 70% pre-retrofit 51 and 40% post-retrofit. 52 The lower infiltration rate post-retrofit accounted for the increased airtightness and reduced air exchange rate (average of 0.45 h−1) following energy retrofit. For formaldehyde, annual average concentrations were assumed to be equivalent to the 72-h average concentration measurements collected in the homes. Annual radon exposure concentrations were assumed to be equivalent to the concentration measured over a six–nine months period in each home. The concentration measurements were collected over different durations and during different seasons, therefore, we assumed that the measured values are representative of the annual exposure level for each pollutant.
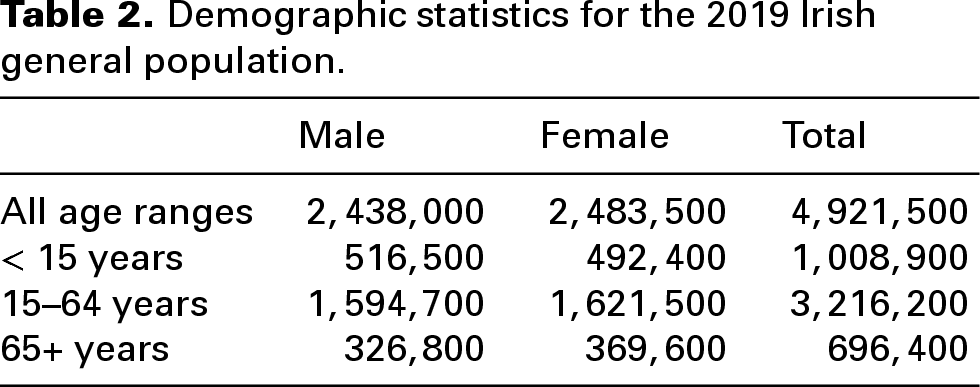
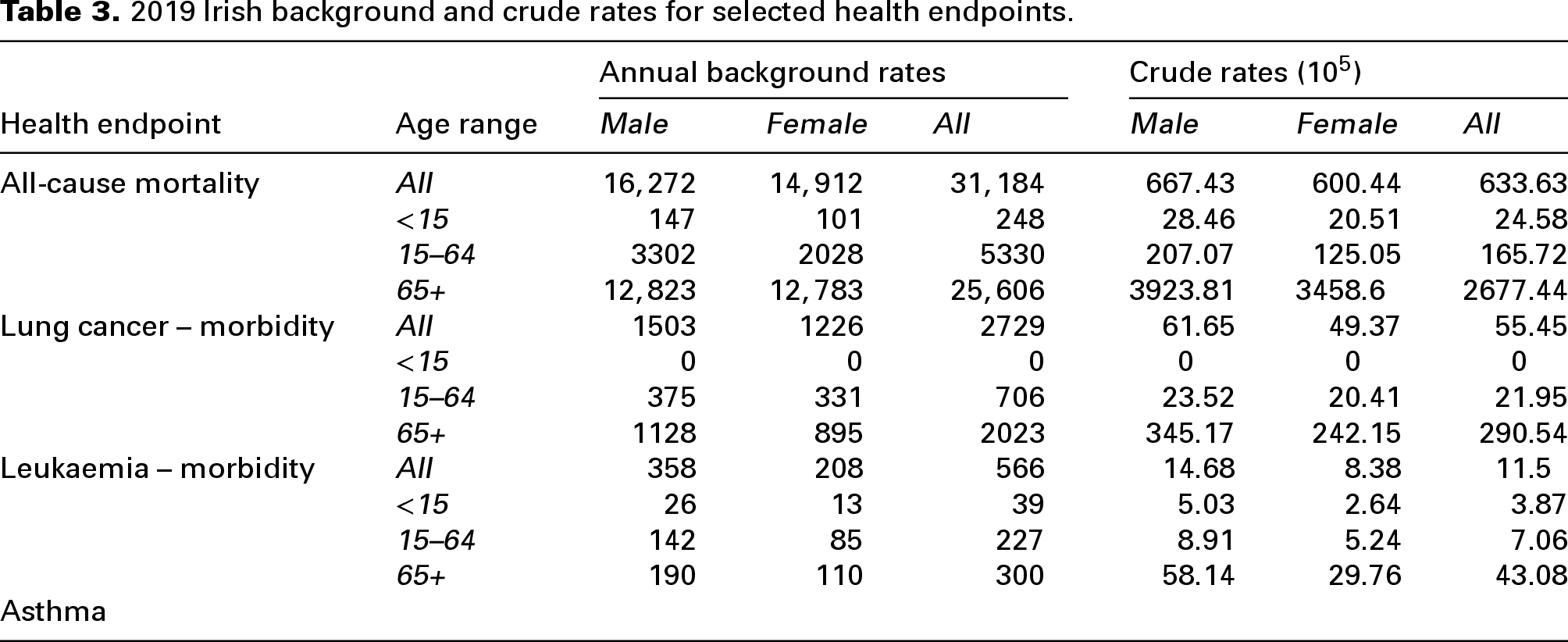
Irish population data and information on background rates of disease (per 100,000 and age groups) (Tables 2 and 3) were obtained from the Central Statistics Office and the National Cancer Registry of Ireland.53,54 As there is no published data on number of asthma cases in Ireland, we used published rates for England from the Institute for Health Metrics and Evaluation. 55
Demographic statistics for the 2019 Irish general population.
2019 Irish background and crude rates for selected health endpoints.
The selected health endpoints for the analysis (Table 4) were chosen based on those commonly reported in epidemiological studies for the selected pollutants. Concentration response functions defining the relation between each pollutant and the subsequent health endpoint were also obtained from epidemiological literature, as presented in Table 4. The estimated change in incidence of disease (morbidity or mortality) due to the incremental increase in a pollutant was calculated using Equation 1
56
:

A summary of the measured pollutants and selected health endpoints used to perform the health burden calculations.
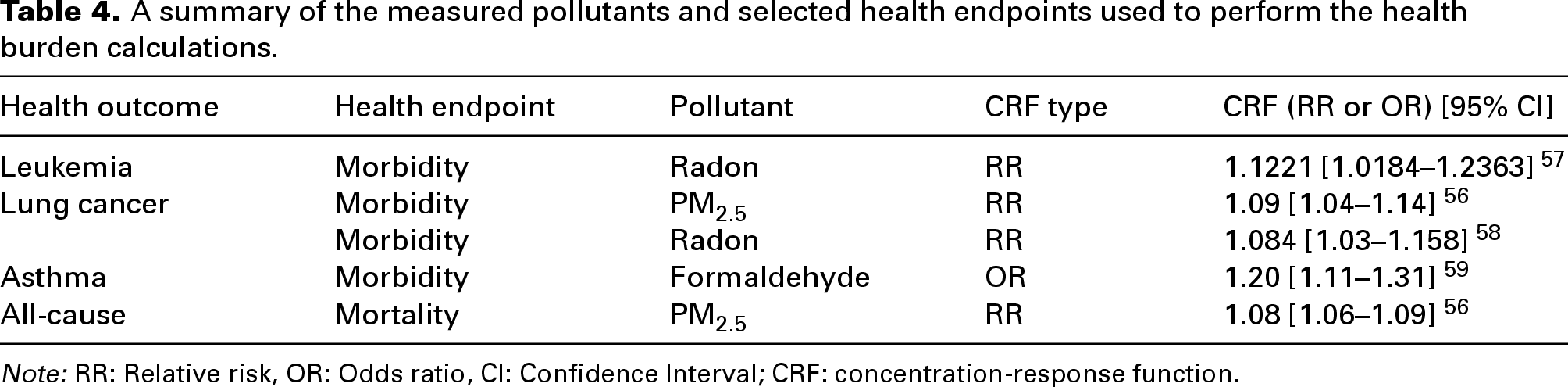
Note: RR: Relative risk, OR: Odds ratio, CI: Confidence Interval; CRF: concentration-response function.
Where ΔCIAP is the measured concentration of the pollutant, ΔCInc is the incremental concentration on which the Relative risk (RR)/Odds Ratio (OR) is based, RR is the relative risk in % of increase in incidence/deaths based per change in increment, OR is the odds of reporting the disease at exposed concentration, N is the total population of Ireland, and Ii is the background rate of disease per 100,000 people.
Data analysis
Health questionnaire.
Descriptive data analysis was conducted on the questionnaire data both pre- and post-retrofit. Frequencies and percentages were calculated for categorical level data and means, and standard deviations were calculated for continuous variables. Changes in health outcomes and health services usage were analysed across timepoints, that is, from pre- to post-retrofit. Pearson Chi-Square tests were conducted to determine changes for categorical variables and the Cochran test was employed to examine differences for dichotomous health variables. The McNemar-Bowker test assessed marginal homogeneity for multivariate health variables. Both the SF-36 and healthcare cost data was analysed using paired t-tests, comparing changes across timepoints. SPSS (Version 26) was used for all quantitative analysis and an alpha level of p < 0.05 was used to define statistical significance.
Results
Demographic profile
Table 5 presents the demographic characteristics of the participants in the pre–post retrofit questionnaire survey, in comparison with the general population in Ireland. The majority of participants were female, with an average age of 53 years at post-retrofit stage and approximately 17% had a third-level qualification, which is lower than the population average (48%). 60 A quarter of participants (25%) were working in semi-skilled/unskilled manual occupations, while almost a third (32%) were in managerial/professional positions, somewhat lower than the national average. In addition, a much lower percentage of respondents reported having a full-time job compared to the national average (i.e. 36% post-retrofit compared to 75% national average). Rates of having private health insurance amongst participants was lower than the national average, with much higher proportions reporting having medical cards (i.e. free public health access based on an income means-test). The majority were renting their homes from local authorities and living in semi-detached residences.
Demographic characteristics of participants, compared to national figures.
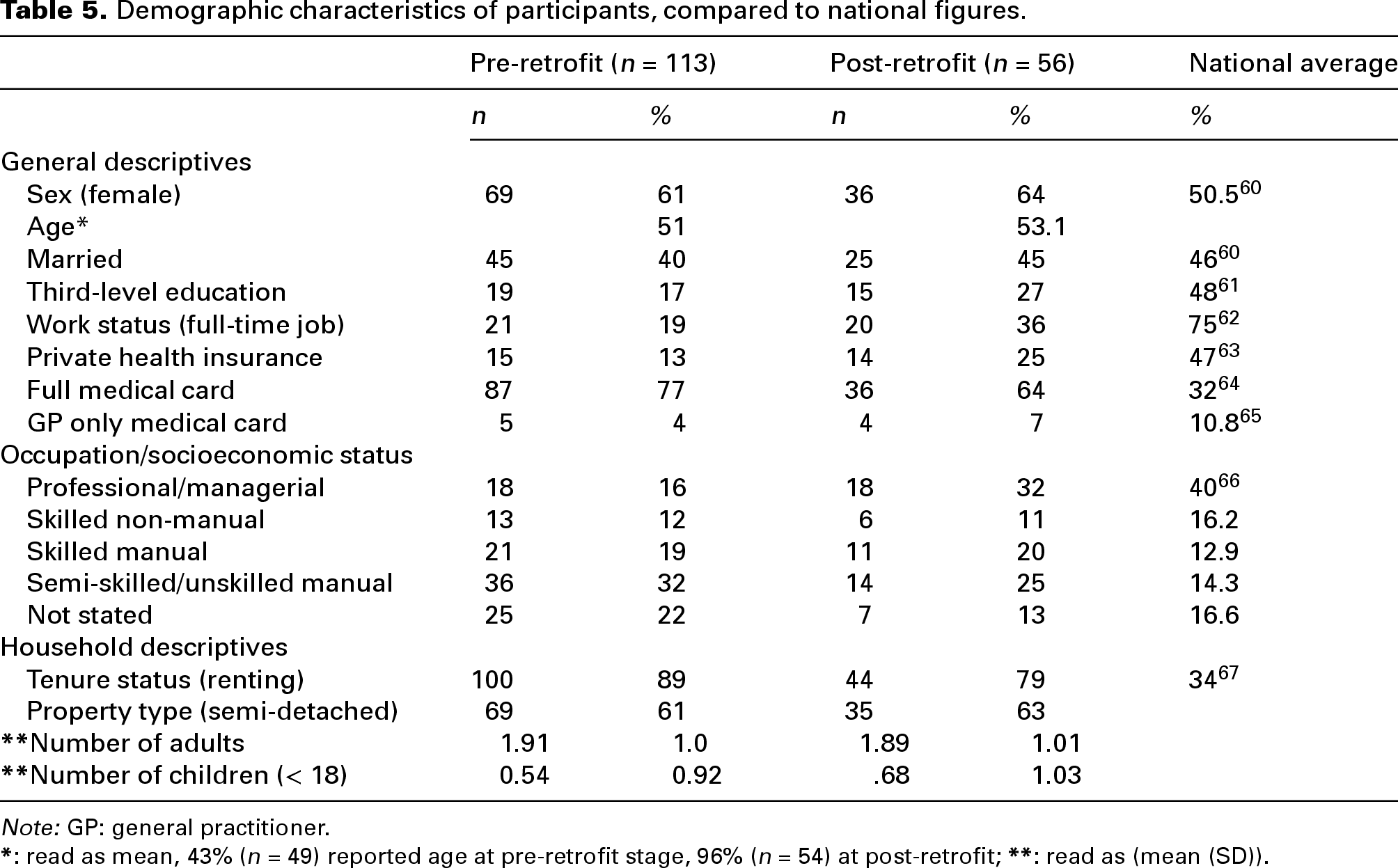
Note: GP: general practitioner.
Health functioning
Table 6 presents the descriptive results for the health data at pre- and post-retrofit stages, showing a high smoking rate and high levels of diagnosed respiratory conditions. Pre–post retrofit changes in health status were only assessed for the 56 homes for which data were available at both time points. Using Cochran's test one significant change in health was observed from pre- to post-retrofit; an increase in COVID-19 diagnoses, with higher instances observed at post-retrofit, χ2 (1) = 6.00, p = 0.014. No significant change in health functioning, as measured through the SF-36, was observed.
Health characteristics of participants at pre- and post-retrofit.
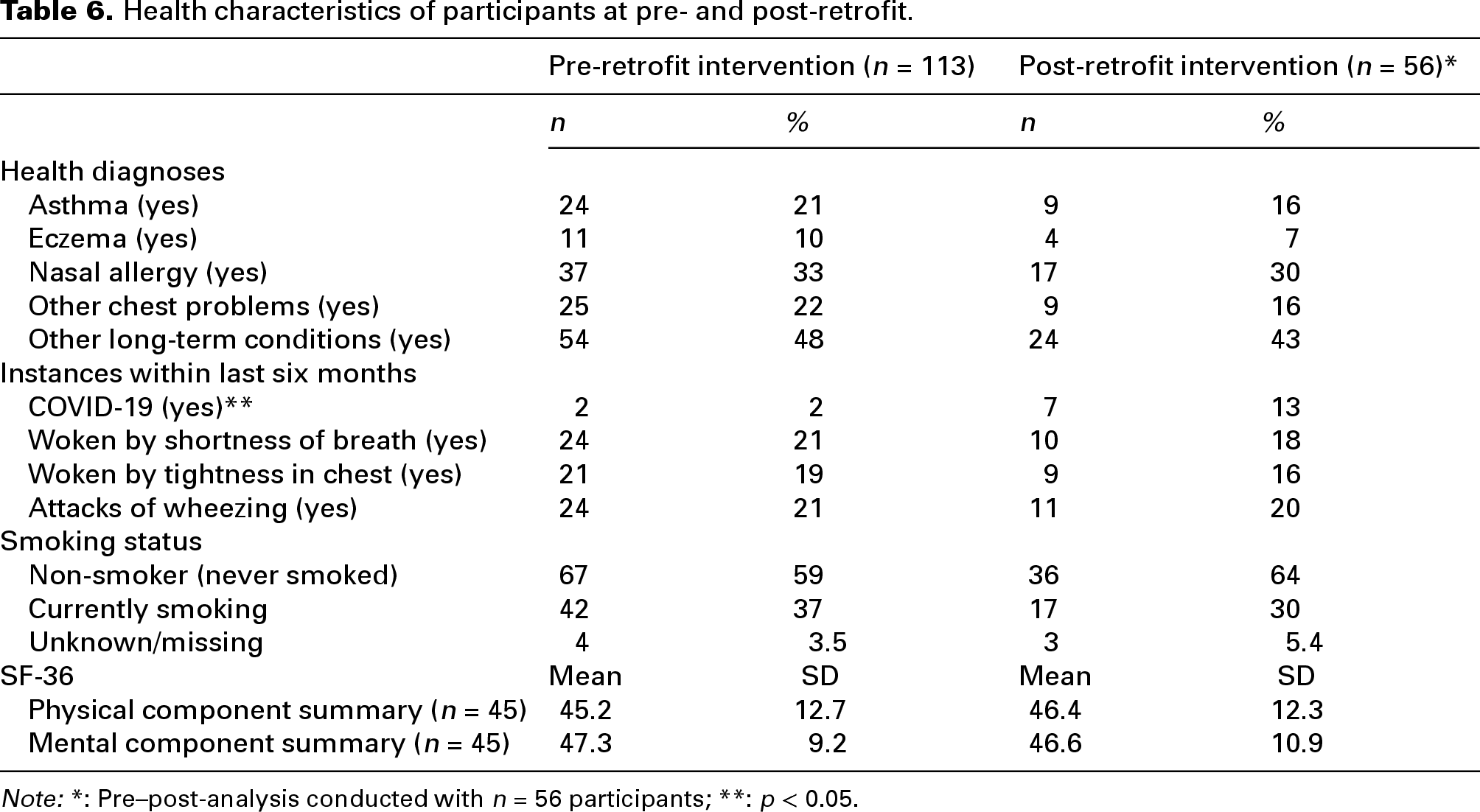
Note: *: Pre–post-analysis conducted with n = 56 participants; **: p < 0.05.
Healthcare utilisation and cost
Table 7 presents the results of the healthcare utilisation by the participants at both pre- and post-retrofit stage. General practitioner (GP) utilisation is slightly higher compared to the national average at both time points. Hospital services have a similar level of usage to the national average.
Healthcare utilisation pre- and post-retrofit.
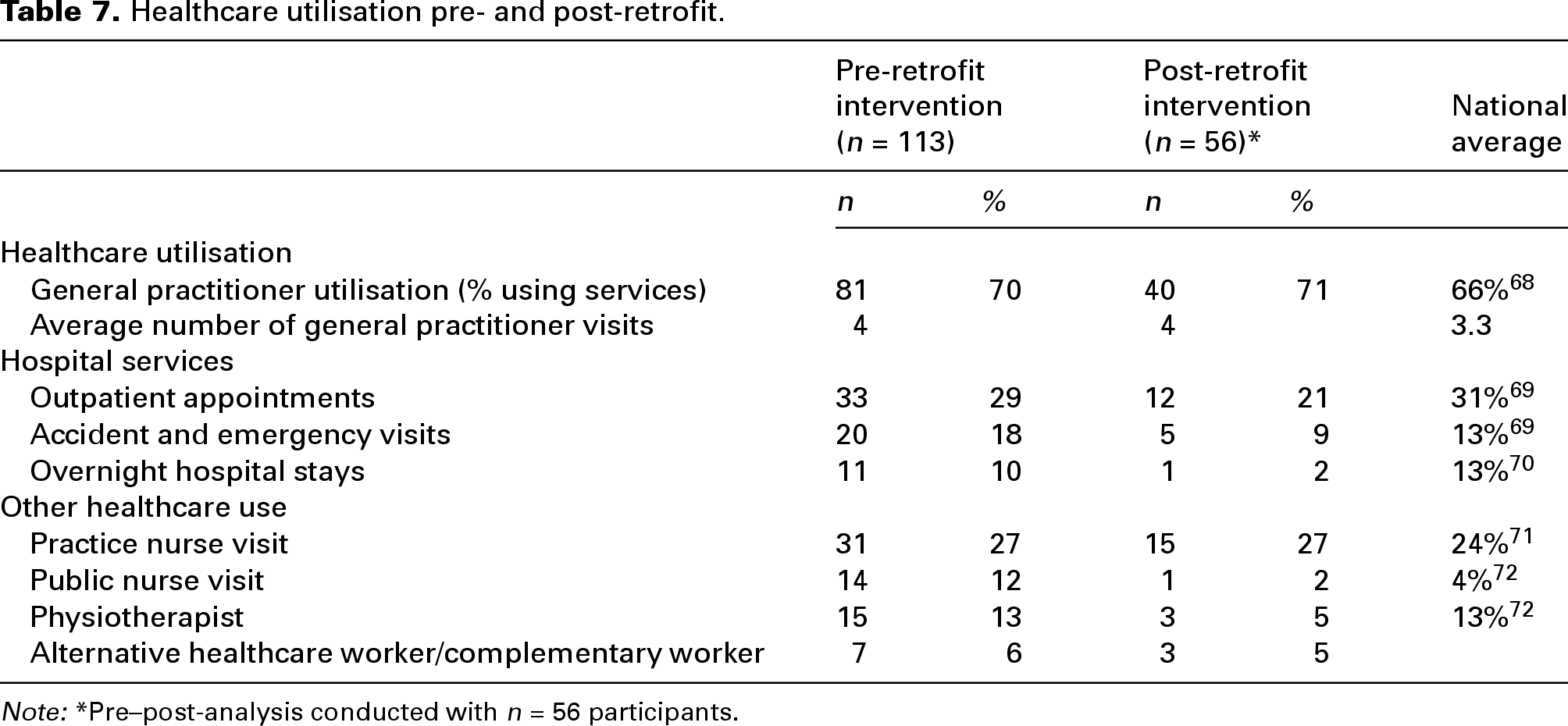
Note: *Pre–post-analysis conducted with n = 56 participants.
We computed healthcare costs using individual level data on the use of the various healthcare services reported in Table 7. We estimated costs based on the number of visits/appointments or number of overnight stays in hospital for respondents multiplied by the average cost of using that service based on the costs presented in Table 1. In total, 78% of respondents (n = 87) in our sample pre-intervention (n = 113) had used at least one healthcare service in the previous 12 months. Table 8 presents the cost data for the pre-retrofit group (n = 113) and then the sample of respondents that completed the survey both pre- and post-retrofit (n = 56).
Estimated healthcare cost data pre- and post-intervention in 2019 prices €.
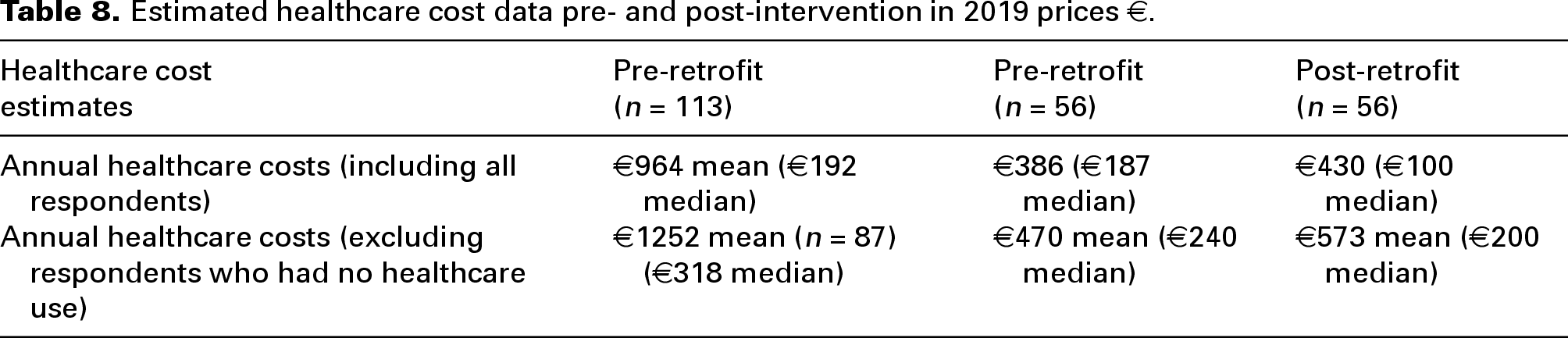
For the (n = 56) sample who completed the survey at both time points, before the retrofit, 46 (82%) participants reported using healthcare services in the previous 12 months. After the retrofit 42 (77%) people reported some form of healthcare use in the previous six months. Results from paired-samples t-tests showed that no significant differences in healthcare costs amongst respondents between pre- and post-retrofit periods (n = 56; p > 0.05).
Medication use
We examined medication use and applied medication cost data to calculate the average cost of medication use of the participants (n = 56 pre- and post-retrofit). Approximately 17% (n = 9) of participants were taking respiratory medication before the retrofit at an average annual cost of € 279. After the retrofit, the average annual cost of medication use was €197 (n = 9).
Health impact assessment
The estimated health impacts associated with the change in exposure to PM2.5, formaldehyde and radon following a DER are presented in Table 9. Health burden estimates are presented for IAP levels in homes pre-retrofit and post-retrofit. Linear mixed effects (LMEs) models were used to examine the impact of different occupants’ behaviours including blocking wall vents and smoking/vaping on indoor pollutant concentrations. 30 Post-retrofit, blocking wall vents was identified as a significant predictor of under ventilation (as evidenced by higher median CO2) in several naturally ventilated homes, and smoking/vaping was identified as a significant predictor of higher PM2.5 concentrations in many of the homes. 30 Therefore, at post-retrofit stage, health burden estimates are presented for all homes, and separately for those naturally ventilated homes which were under ventilated due to the presence of blocked wall vents (formaldehyde) and separately for homes which had known sources of indoor PM2.5 (a resident smoker or vaper) and that were under ventilated due to blocked wall vents.
Health outcome assessment of exposure to selected pollutants for the exposed intervention group.
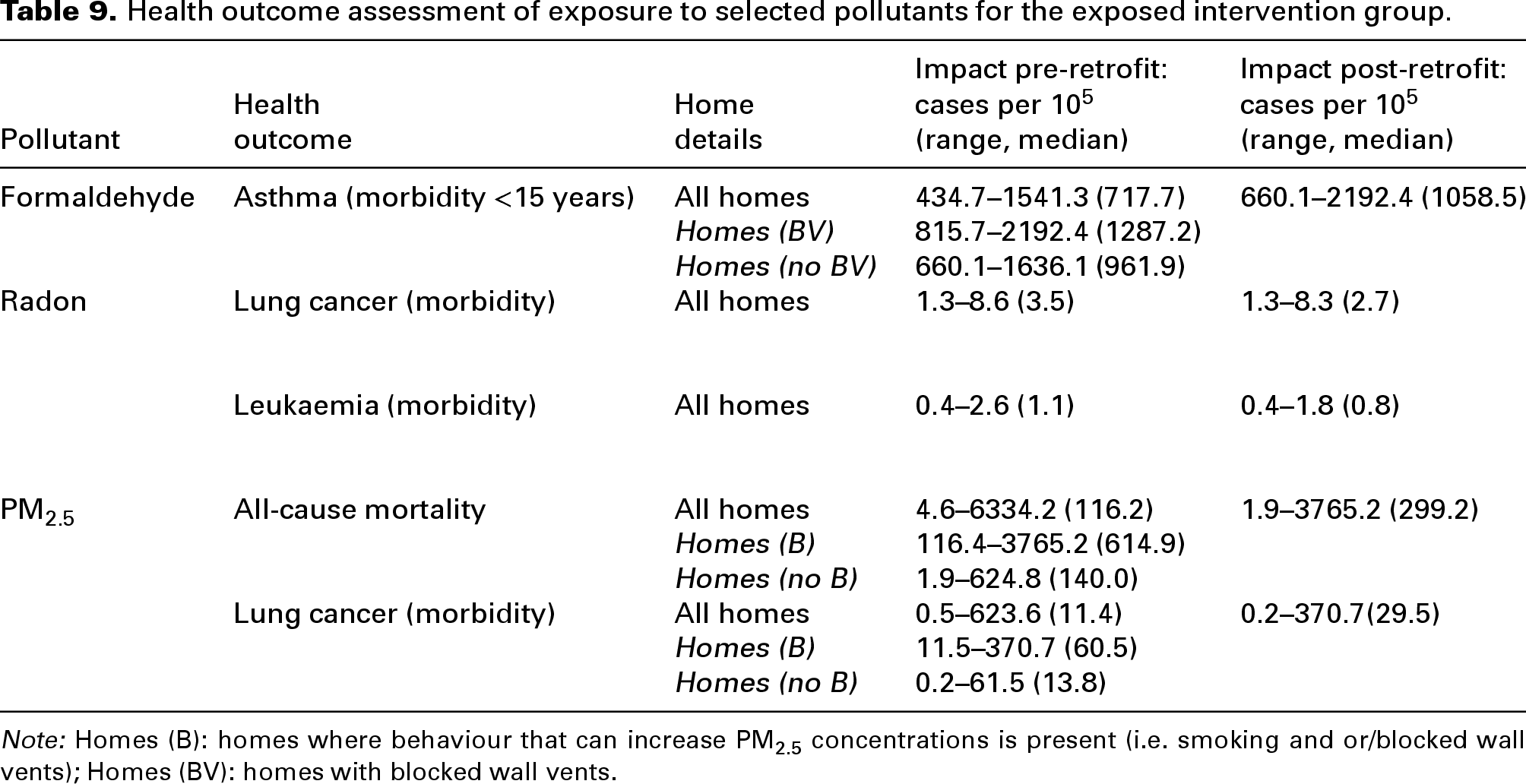
Note: Homes (B): homes where behaviour that can increase PM2.5 concentrations is present (i.e. smoking and or/blocked wall vents); Homes (BV): homes with blocked wall vents.
Our estimates suggest that the greatest health burden is due to an increase in exposure to PM2.5 (all-cause mortality), followed by formaldehyde (asthma morbidity < 15 years) and lung cancer morbidity due to higher PM2.5 exposures. There is no significant difference in the health burdens (lung cancer and leukaemia morbidity) associated with the change in radon exposure following retrofit, compared to pre-retrofit stage. While radon exposure increased post retrofit in half (50%) of the homes included in our study, radon levels were generally low with only five homes > 100 Bq/m3.
Discussion
This study employed a mixed-methods, short-term longitudinal design to assess the impact of DER on health and related healthcare costs. The findings provide valuable insights into the complex interactions between housing improvements and health outcomes, revealing a mixed set of results. While demographic data from the questionnaire survey at both pre- and post-retrofit stages indicates some notable risk factors such as higher smoking prevalence and increased rates of respiratory-related conditions amongst participants in social homes undergoing a planned retrofit, post-retrofit analyses showed no significant improvements in health-related quality of life, as reported through the SF-36 and respiratory functioning pre–post scores, suggesting that the short-term benefits of DERs may be limited or take longer to significantly influence perceived health outcomes. The significant increase in COVID-19 diagnoses post-retrofit in the sample is consistent with the increase in COVID-19 infections in Ireland as a whole in this time period. 73 The lack of change in health functioning observed in this study, differs from that of the recently published Warmth and Well-being study conducted in Ireland, where improvements in health functioning of participants with a pre-existing respiratory condition, living in retrofitted homes was observed. 14 Furthermore, significant decreases in healthcare utilisation were not observed, also differing from the Warmth and Well-being study findings. 14 However, inclusion criteria, sample size and length of follow-up time from pre-to-post retrofit were considerably different between both studies, with the follow-up time of seven months in this study, being much shorter than the two year follow-up time employed by Milner et al., 14 where a longer follow-up time indicated a positive impact on both health and reduction in healthcare use. While our questionnaire findings are inconsistent with those of Milner et al., 14 relatively few studies examining the health impact of retrofitting have been conducted in Ireland, so continued research focus on the impact of retrofitting is warranted. This study examined average healthcare costs pre- and post-retrofit and found no significant difference in costs including medication costs between the two time points (n = 56). However, this may be due to the relatively short follow-up period and the relatively small sample size available to compare costs. This suggests that the healthcare benefits (in terms of reduced use and costs) may take longer to manifest. We also collected the data at various time points to ensure that our estimates were not impacted by seasonality differences pre-and post-retrofit.
The HIA using the objective IAQ measurements showed that for a small number of homes (n = 6) the energy retrofit resulted in positive improvements in health. However, overall, median pollutant concentrations (n = 14) increased after retrofit resulting in a net negative effect on predicted health outcomes. For PM2.5, the median health burden estimate for all-cause mortality, at 615 cases per 100,000, found in under-ventilated homes with elevated PM2.5 levels due to the presence of tobacco smoking is four times higher compared to non-smoking homes with unobstructed wall vents (140 cases per 100,000). Direct comparisons with the findings of Milner et al., 14 who modelled the health impact (change in deaths over 30 years) due to change in exposure to PM2.5 and radon in Irish energy retrofitted domestic dwellings (with no additional ventilation), are challenging as the health outcomes used for PM2.5 differ between the two studies. Milner et al. 14 projected 368 cases per 100,000 population over 30 years for cardiopulmonary and lung cancer deaths, whereas our health burden estimates are much higher, with a median value of 299 cases per 100,000 for annual all-cause mortality. Even if we assume that half of the ‘all-cause mortality’ in this study is due to cardiopulmonary and lung cancer causes based on the findings of Milner et al. 14 (150 cases per 100,000 cases per year) our estimates remain substantially higher. Another key reason for the difference in estimates between the studies is that the modelled PM2.5 concentrations used by Milner et al. 14 (i.e. 9 µg/m3 for under ventilated homes) are substantially lower than the concentrations measured across homes in our study, for example, PM2.5 in Home (B) (smoking/blocked vents) ranged from 23 to 743 µg/m3, with a median of 121 µg/m3. Milner et al. 14 also presented modelled mortality rates (e.g. lung cancer mortality, 214 deaths over 30 years) for increased radon exposure for under-ventilated energy retrofits. 14 As highlighted by Milner et al., 14 these modelled estimates were based on a post-retrofit radon concentration of 45 Bq/m3 estimated using U.K. data which is lower than the median post-retrofit radon concentration of 57 Bq/m3 measured across our n = 18 homes, which were primarily located in medium and low risk radon areas 74 and resulted in an estimated increase of three lung cancer cases per 100,000 per year. Health burden estimates for radon in our study are lower than those reported by Milner et al. 14 despite the slightly higher median concentration, which is primarily due to the use of different relative risks per 100 Bq/m3 in the two studies. Milner et al. 14 used the RR associated with ‘usual’ radon levels (1.16) whereas we have used the RR associated with ‘measured’ radon levels (1.08) as our study was based on radon measurements rather than modelled levels.
Our HIA results demonstrate the critical influence of occupant behaviours, such as smoking and blocking wall vents on exposure to indoor pollutants, and the resulting health burdens following energy retrofits. While our study findings address health risks to adults, other researchers have also reported specific childhood health risks associated with exposure to IAPs and allergens17–19 and have recommended improving ventilation in homes in order to reduce incidence of illness. 17 Our results highlight the urgent need for the National Retrofit Programme to mandate that comprehensive guidance be provided to homeowners and tenants on IAQ and ventilation as part of the retrofit handover. Given the numerous reports of under ventilation in residential buildings75,76 and ventilation performance gaps following energy retrofit25,29,77–79 our conclusion supports others who call for further empirical data,75,80 both IAQ measurements data and ventilation performance data to fully estimate the health impact of indoor air pollution in residential dwellings following energy retrofits.
This study's comprehensive approach, integrating objective IAQ measurements and subjective health assessments, underscores the multifaceted nature of DER's impact. Despite the lack of significant changes in health-related quality of life or healthcare costs, the detailed analysis of pollutant concentrations in conjunction with health and healthcare cost data provides a framework for understanding the broader implications of energy retrofitting. Additionally, a separate analysis examining change in TC 30 (in the homes for which health data is presented in this study) revealed a positive impact of retrofitting on TC, which was also found previously in at least one study, where Heyman et al. 81 reported positive improvements in TC following retrofit, while at the same time, reporting no impact on the health functioning of participants within the homes.
Overall, this study highlights the importance of taking a holistic approach to evaluating the impact of DERs. By linking health, economic and indoor pollutant data, researchers can better explore these interactions through a narrative lens, facilitating a more nuanced understanding of DER's effects. This approach also highlights the potential for such DER evaluations to contribute to public health understanding of the potential long-term consequences, even if short-term benefits are not immediately evident. The approach employed in this study is similar to that undertaken in the Warmth and Well-being study, 14 but adds to our understanding through the inclusion of the HIA analysis using measured pollutant data at pre- and post-retrofit.
Policy and practice implications
Although the findings from this study were mixed, the holistic multi-disciplinary approach employed could be used as a template for future evaluations of the impact of DER, given the multiple interacting outcomes of interest to policymakers. As noted by Armstrong et al., 82 there are benefits to aligning policy objectives not only to single criteria of success such as health impact, but more importantly to address multiple related criteria, including health impact, health inequalities, energy security, greenhouse gas emissions and fuel poverty. Furthermore, recent Irish research highlights the vulnerability of residents living in social housing to negative impacts on health and well-being, finding that lower income families are more likely to live in rented or social housing and experience inadequate housing or poor housing quality, usually reflected by inadequate space, inadequate heating and exposure to damp. 83 Our profile of participants living in social housing, highlights additional health risk factors including a higher smoking rate in comparison with the national average, lower educational attainment, lower rates of working full-time (which might impact on time spent at home) and greater reliance on public healthcare, where targeted interventions such as DER could help reduce health disparities between social housing occupants and the wider population. However, increases in exposure to IAPs post-retrofit resulting from a combination of occupants’ behaviours in more air-tight homes could potentially lead to negative health impacts on this vulnerable group in the long-term. A reported 34% of social housing tenants smoke regularly, which is a significant source of indoor air pollution, therefore it is important that households undergoing DERs understand the consequence of such behaviours on exposure to IAPs, and also the importance of adjusting behaviours after retrofit especially with regard to ventilation. Examples of actions that policy makers could take would be more detailed guidance and handover on use of heat pump technology along with guidance for occupants to avoid blocking of vents. However, as noted by Chiu et al., 84 DER requires a socio-technical perspective and interventions are warranted that support occupants to change habits such as quitting smoking through support from their local medical practice or the provision of more information on the risks to air quality from burning candles within the home. Finally, integrating HIAs as an additional means to evaluate DER initiatives could help identify potential long term health benefits of DERs while including cost data could assess the potential impact on the health service.
Strengths and limitations
The study's strengths include its mixed-methods design, which allowed for a comprehensive analysis of both objective and subjective data, and the integration of health, economic and IAQ factors, providing a holistic understanding of DER's impact. Furthermore, few studies to date have quantified the health impact of DER, therefore, this study adds to the extant literature, with particular relevance for the Irish context. However, several limitations affecting the generalisability of our results should be noted. The COVID-19 pandemic introduced complications in the implementation of the questionnaire survey, resulting in a smaller sample size than anticipated, which while low, is comparable to that of Breysse et al. 85 The attrition rate from the survey from pre- to post-retrofit (50%) further reduced the overall sample size. While 31% of participants were lost from the survey, the other 19% was lost due to delays in the retrofitting programme of works due to COVID-19. Thus, this revised attrition rate of 31% is comparable to that of Milner et al. 14 (30%). Another impact related to COVID-19 and attrition rate seems to be that users with higher health costs as seen in Table 8 did not take part in the survey post-retrofit which it could be speculated was due to health reasons. This highlights a further challenge in assessing changes for those with high healthcare needs through this survey approach during a pandemic indicating that the sample could be biased towards those that remained healthy to return surveys. Additionally, the short-term nature of the study follow-up time limits the ability to observe long-term health impacts including impacts on healthcare costs, which are crucial for a comprehensive assessment of DER's benefits. The health burden estimates were extrapolated from a set of measurements in n = 14 homes, nearly half of which were under-ventilated due to blocked wall vents, which may overestimate the health burden. Over half of the homes that participated in radon monitoring were located in either medium or low risk radon areas. Radon levels in high-risk areas are likely to be much higher, therefore health burden estimates for radon may underestimate the risk. The IAQ data used to perform the health burden estimates spanned different seasons, this was difficult to avoid, as study participants’ preferences and delays associated with delivery of the energy retrofits had to be accommodated. However, the LME models used to analyse the IAQ data 30 included outdoor weather data, accounting for different monitoring periods, this analysis showed that the different monitoring periods had a limited impact on resultant indoor pollutant concentrations compared to occupants’ behaviours. Finally, in the pre–post retrofit health survey analysis, potential confounders such as health status, age and temporal factors were not controlled for due to the smaller sample size. Future studies should account for larger sample sizes and attrition rates to incorporate such confounding factors in their statistical analysis to improve causal inference.
Future research
Given the inconsistency in health-related findings between this study, focusing on all adult occupants and those of Milner et al., 14 who focused solely on occupants with a chronic respiratory conditions, additional Irish studies are warranted to allow us to fully elucidate the complex relationship between retrofitting and health within the framework of Irish policy and implementation of retrofitting programmes. More broadly, future studies should aim to include larger and more diverse populations, in conjunction with longer follow-up times to ensure wider applicability and to more fully to capture the impact of DER on health, healthcare use and costs. Furthermore, refining the holistic approach used in this study could enhance the ability to explore and understand the complex interactions between housing conditions and health. Further research is needed to accurately determine the extent of under-ventilation in energy retrofitted homes; this would enable a more precise evaluation of the disease burden associated with inadequate ventilation to be determined.
Conclusion
In conclusion, while this study provides valuable insights into the short-term impacts of energy retrofitting, further research is needed to fully understand its long-term benefits and to develop effective policies and practices that promote health equity and environmental sustainability. Holistic, multi-disciplinary research approaches are needed to fully elucidate the relationship between DER and health and healthcare impacts.
Footnotes
Acknowledgements
The authors would like to thank the homes who participated in this study and the local authorities, approved housing bodies and private retrofit companies for their support. Thank you also to Edel Killackey and Ciaran Maher for their assistance with the collection of the IAQ data.
Consent to participate
Informed consent was obtained from all study participants, requiring the participants to confirm that they had read and understood the participant information sheet and that they agreed to participate in the study.
Data availability
Data is available upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval for this study was granted by the University of Galway, Research Ethics Committee (Reference No. 2022.03.007, March 2022).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HAVEN study was funded by the Sustainable Energy Authority of Ireland under the SEAI Research, Development and Demonstration Funding Programme 2018 (Grant No. 19/RDD/435).