
Abstract
Voice problems are common in occupations where there is noise, dust, odours or fumes and microbial contamination. The purpose of this study is to find out the prevalence of hoarseness, its changes over the follow-up and the effect of the remediation on the prevalence. A total of 13 health care buildings were followed, 10 with indoor air problems and 3 as reference buildings. Three buildings were thoroughly remediated, and their effects were analyzed. A health questionnaire was used, before and after the remediation. Blood samples and skin prick tests were performed on all volunteers. Based on findings, 17.0% of the respondents reported hoarseness at least every week. The skin test findings for common environmental allergens, moisture damage microbes and mites were approximately similar in the exposed and reference groups, respectively. Hoarseness had a strong correlation with indoor air problems. Before the remediation, hoarseness and voice problems were more prevalent in the problem buildings. After the remediation, hoarseness was reduced by 50%. In conclusion, this study shows a connection between indoor air exposure and technical damage in buildings. The remediation significantly reduced the prevalence of hoarseness. Mould allergy is rare and does not explain the voice problems.
Introduction
Hoarseness is a common symptom in professions where the voice is used and strained, and in work environment with background noise, such as schools 1 and kindergartens, 2 but also in large hospitals with effective ventilation systems, medication, surgical fumes, etc.3,4 The dryness of the air, dust, man-made mineral fibres and other problems with indoor air are associated with irritation of the respiratory tract. It is widely accepted that moisture and moisture indicative microbes are associated with incident asthma.5–8 Irritative symptoms often precede an asthma diagnosis. That is why the recognition of typical symptoms in problem buildings is important so that remediation can be started in due course before irreversible illnesses, such as diagnosis of asthma.
The mechanisms and risk factors behind hoarseness are partly unknown. Allergies and atopy may trigger voice symptoms, also smoking and other irritant gases, fumes and particles may increase or worsen symptoms.9,10 In dental care, many potentially harmful chemicals are used. In health care work, there is common exposure to pathogenic and other microbes, disinfectants and medical drugs. Sewer gases, the dryness of the air during the heating season, noise and too high temperatures in health care facilities increase the reporting of respiratory irritation.3,4,8
Insufficient ventilation, moisture damage and microbial growth are common in the Finnish housing stock. According to Hellgren and coworkers, 4 15% of hospital buildings are in need of urgent remediation. Health care centres and elderly care facilities have not been investigated systematically. Neither has the health effect of proper remediation been investigated with follow-up studies regarding the personnel.
The treatment of hoarseness consists of voice therapy, voice massage, medication, treatment of respiratory infections, quitting smoking, water pipe or other humidification of the inhaled air and changing the individual’s occupation or work tasks. Follow-up studies on the effects of these interventions are rare.
In clinical praxis, we have observed an increasing trend in voice problems especially amongst women. Although hoarseness is mostly due to benign factors, it has a significant negative impact not only on an individual’s quality of life but also on the national economy; it increases health care visits as well as reduces productivity due to absences. 9 Amongst nursing profession and in medical and dental care, communication with patients and fellow workers is important and a clear and strong voice is an essential tool. Clear verbal communication increases the safety of health care workers. For the sake of occupational safety, prevention, care and rehabilitation, the identification of possible work/workplace-related risk factors is important.
The purpose of this study was to investigate the occurrence of hoarseness amongst medical staff in Finnish primary health care centres and to find out potential risk factors associated with the work and work environment. The second aim was to discover if pathophysiological mechanisms of the hoarseness can be revealed with current immunological and allergological tests. The third aim was to find out if remediation of the buildings influenced the prevalence of hoarseness during a 2-year follow-up with a study population who had continued in their current jobs.
Material and methods
Description of the damaged and reference buildings.
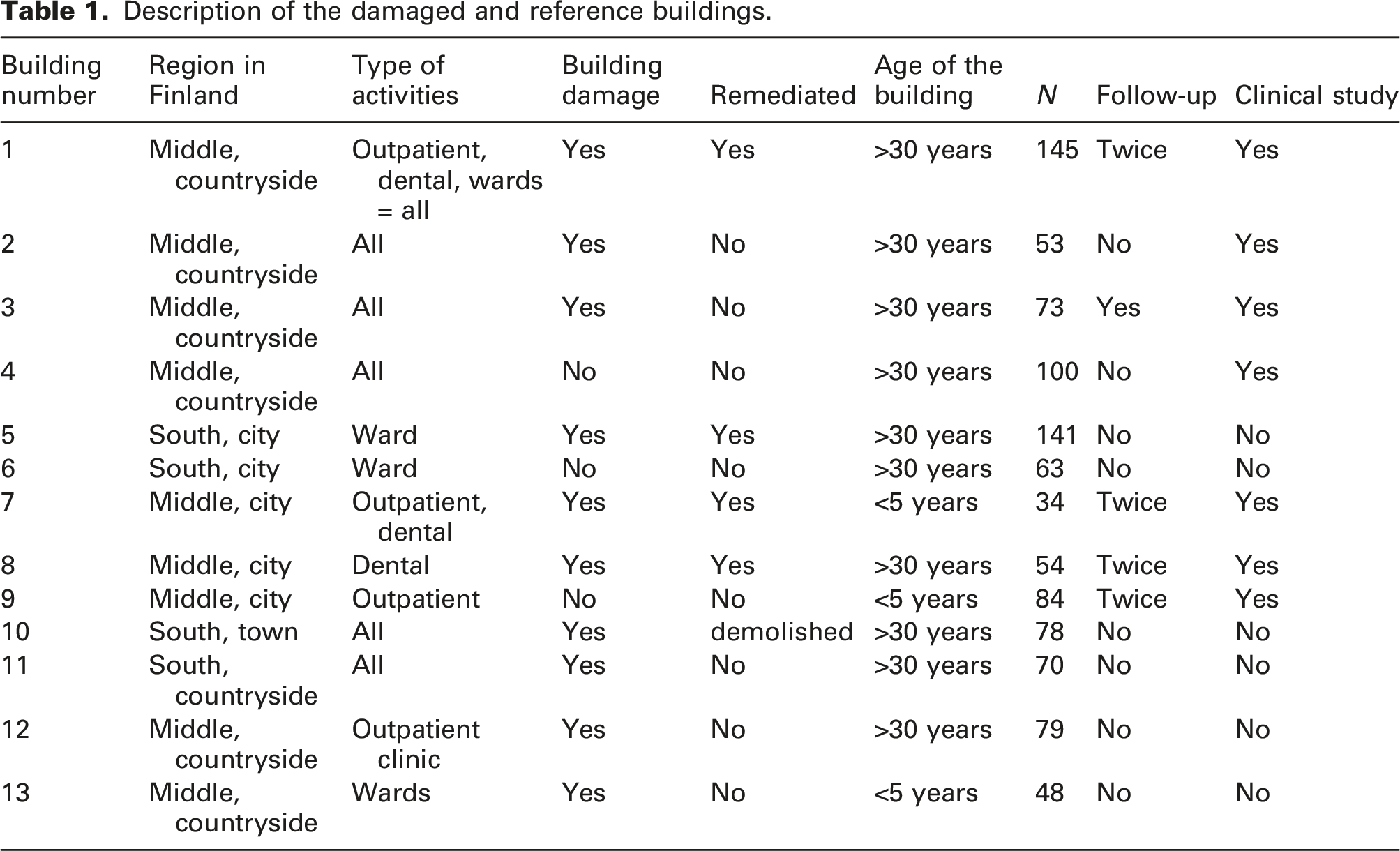
All buildings were inspected by trained construction engineers and several microbial samples were taken from the buildings’ structure according to national guidelines. 11 The samples were cultivated on 3 agar plates for 7–10 days, and colonies were counted and identified with light microscopy by a trained environmental microbiologist in a laboratory with FINAS accreditation. In the study, the respondents working in the buildings with microbial damage are called the exposure group and the workers in the buildings with no major damage are called the reference group. The dental care units were included in both groups.
The same symptom questionnaire was used at all sites before the remediation and afterwards in the follow-up surveys. The questionnaire comprises 53 questions, and it includes the so-called Örebro questionnaire which is commonly used in indoor air research and validated in Sweden. 12 Both used questionnaires are publicly available.13,14 The questions on respiratory infections have been validated in the Finnish materials. 15 In the questionnaire, the answers about the occurrence of hoarseness, throat irritation, rhinitis and coughs are expressed using four alternatives, ‘daily or almost daily’, ‘every week’, ‘more seldom’ and ‘never’. In the analysis, the first two and the last two alternatives were combined to achieve a dichotomous variable. Smoking was defined as a ‘yes’ alternative if the respondent had smoked at least one cigarette per day for at least 1 year. Ex-smokers and non-smokers were combined. Individuals who had stopped smoking for less than 6 months were classified as smokers. In addition to the work environment, questions were also asked about the home environment, whether or not the respondent has had moisture, mould or unpleasant odours at home and if the damage had been remediated. In addition, the respondents were asked whether they were exposed to compost or organic dust during leisure time and if the respondent has or has had pets at home. Questions were also asked about job strain, well-being at work and perceived general health status. Furthermore, the respondents were questioned as to the occurrence of respiratory infections during the previous 12 months and diseases diagnosed by a doctor and any currently prescribed medication.
The blood samples were collected from all volunteers in five buildings, three with damage and two without indoor air problems. All serum samples from the damaged and reference buildings were drawn by a trained laboratory nurse, and the samples were analyzed in laboratories with no knowledge of possible exposure. Serum microbe-specific immunoglobulin levels were assessed with a FINAS-accredited enzyme-linked immunosorbent (ELISA) method at the Finnish Institute of Occupational Health (Kuopio Regional Office, Kuopio, Finland). Microbe-specific IgE used for a moisture damage microbial panel contained the following microbes: Aspergillus versicolor, Chaetomium globosum, Fusarium merismoides, Stachybotrys chartarum, Streptomyces albus, Streptomyces halstedii, Trichoderma citrinoviride and Tritirachium oryzae. All the immunological samples were analyzed in laboratories in local university hospitals. Lymphocyte populations were analyzed utilizing flow cytometry and immunostaining with standard fluorescent cellular markers, which is considered to be the most exact and reliable procedure. 16
A skin prick test (SPT) is a basic examination of immediate allergic reactions. It is usually the primary method in confirming sensitization in IgE-mediated allergic disease because of its reliability, safety and convenience.17,18 SPTs were performed with ALK-Abello extracts, and the same experienced laboratory nurse made all the tests. All wheals with a diameter of >3 mm were considered positive when the negative control solution was negative. 18 In addition to common environmental allergens, such as pollen and animal dander, tests were also carried out for dust mites, storage mites and microfungi (moulds and yeast).
Three buildings were thoroughly remediated and the health status in these buildings was compared with the situation before the remediation. One of the remediated buildings was less than 5 years old, the others were 30–40 years old. One of the reference buildings was new and the others were approximately 30 years old. All the buildings had concrete and bricks as the bearing construction. All buildings had a mechanical ventilation system. The buildings selected for this study have been chosen to be as comparable as possible, taking into account the purpose of use, building type and materials and the problems found.
The study setting was an open cohort, and the follow-up surveys were done at 2-year intervals. All the drop-outs could not be traced (the individuals had moved away or retired). Some individuals were moved to cleaner buildings in the same municipality. When new workers were recruited, they were allowed to participate in the follow-up surveys. Some of the respondents answered without giving a name and that is why their health data could not be combined with their laboratory data or the follow-up questionnaire data. After the combination of all data, the answers were pseudonymized. The flow chart illustrates the collection of data (Figure 1). Flow chart of the collection of the study material.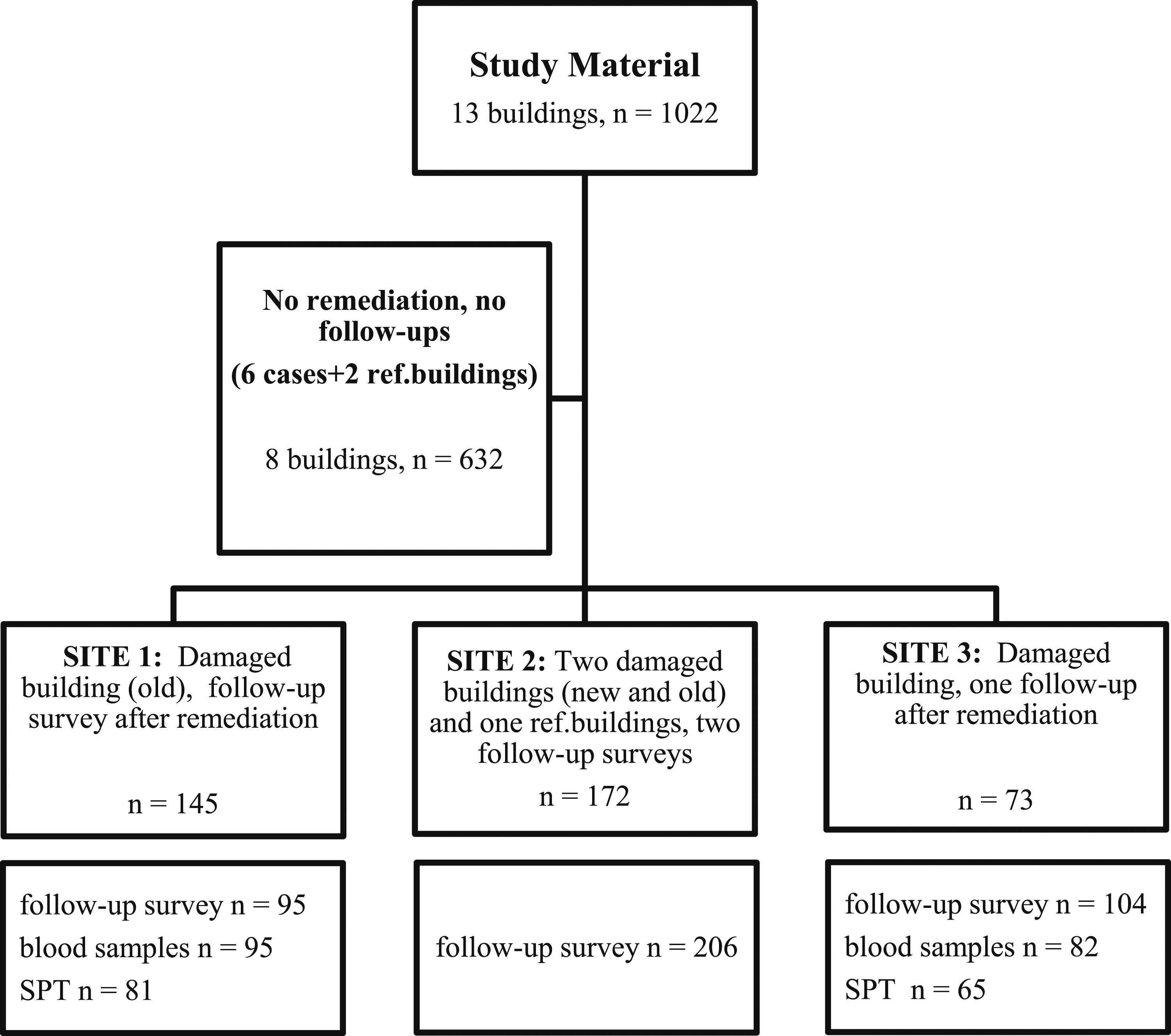
In the statistical analysis, the SPSS Statistics 26-programme was used (IBM Corp. Armonk, NY). Respondents from the buildings with indoor air problems were compared with the respective data from the reference buildings. In the follow-up study, the data before the remediation was compared with the corresponding health data from the same building 2 years and 4 years after the remediation. Statistical significance for dichotomous variables was calculated with a Chi2-test and continuous variables with a t-test. Odds ratios with 95% confidence intervals for risk factors for hoarseness were calculated with logistic regression models (dichotomous variables) and variance and covariance analysis for continuous variables.
Results
Exposure data
The microbial samples showed high concentrations of moisture indicator microbes in the basement and 1st floor of Site 1 and also in the basement and walls of Sites 2 and 3. In all three sites, microbial growth was also found in the insulation materials in the basement and outer walls. Additionally, the ventilations (HVAC) of these buildings were not operating properly, and impurities and building wastes were found in the ventilation ducts in all damaged buildings. The damages in all buildings with indoor air problems were similar to each other with the addition of sewer water flooding on the floors in the basement of one building (not included in the follow-up because the building was later demolished).
The microbial concentrations exceeded the national guideline values by several orders of magnitude, and the microbes identified were typical for moisture damage according to the international classification by Samson et al. 19 and adopted into Finland’s National Guidelines and Finland’s by-laws. 11 The most common microbes identified in the material samples were Penicillium sp., Geotrichum, Acremonium, Aspergillus versicolor, Fusarium, Chaetomium, Rhodotorula and other yeasts, with the addition of Actinomycetes sp. bacteria.
In the remediation, the mould contaminated materials were removed and replaced with dry and clean materials, and the ventilation ducts were cleaned.
Subjective indoor air quality
Subjective indoor air quality factors (daily or every week) and signs of moisture damage in the problem and reference buildings (N and %).
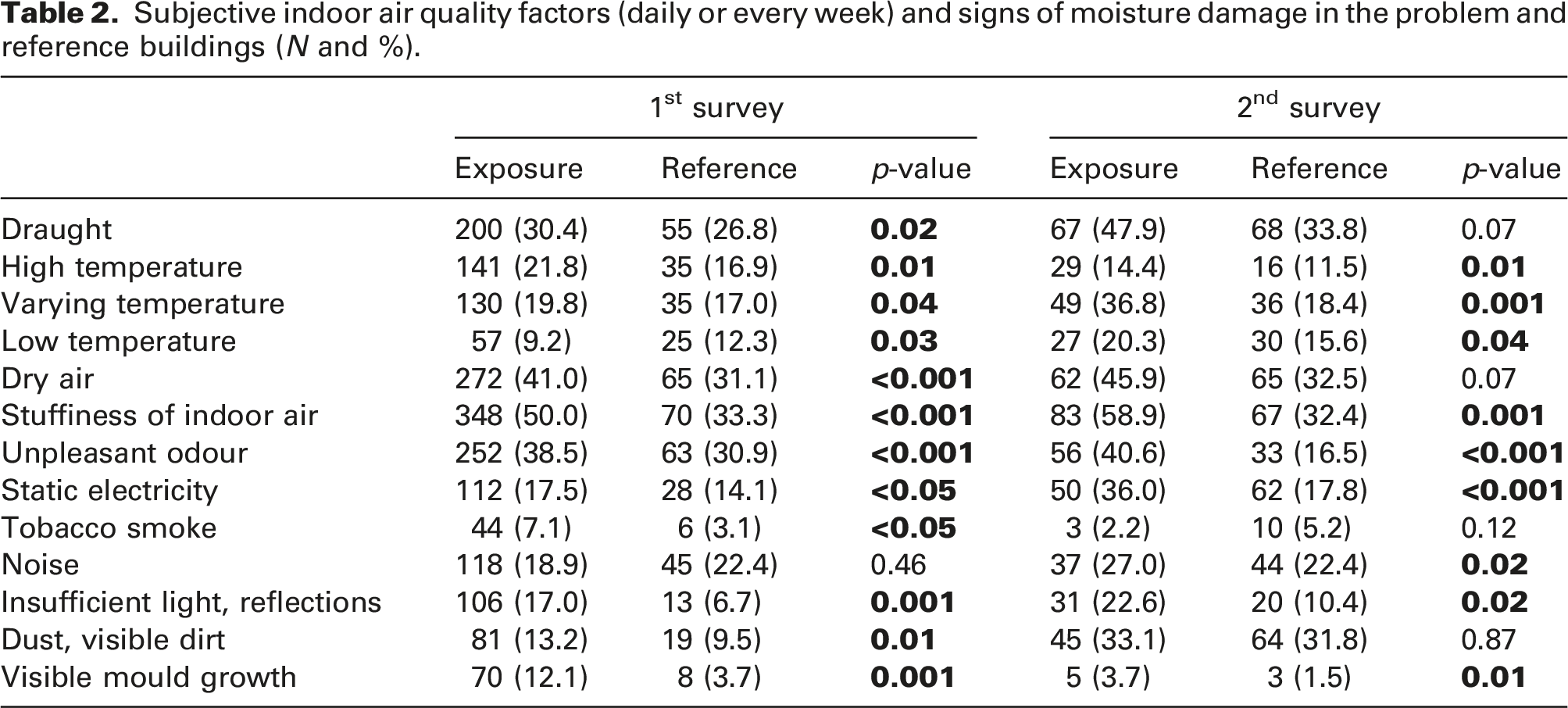
After the remediation, high temperatures, tobacco smoke and observations of visible mould had diminished. Other indoor air factors had increased or remained at the same level. Subjective indoor air quality had also become worse in the reference buildings, and the differences were no longer statistically significant with regard to annoyance by draughts, dry air and visible dust or dirt. In the follow-up survey, most of the annoying factors in the problem buildings were still at a significantly higher level than in the reference buildings.
Health data
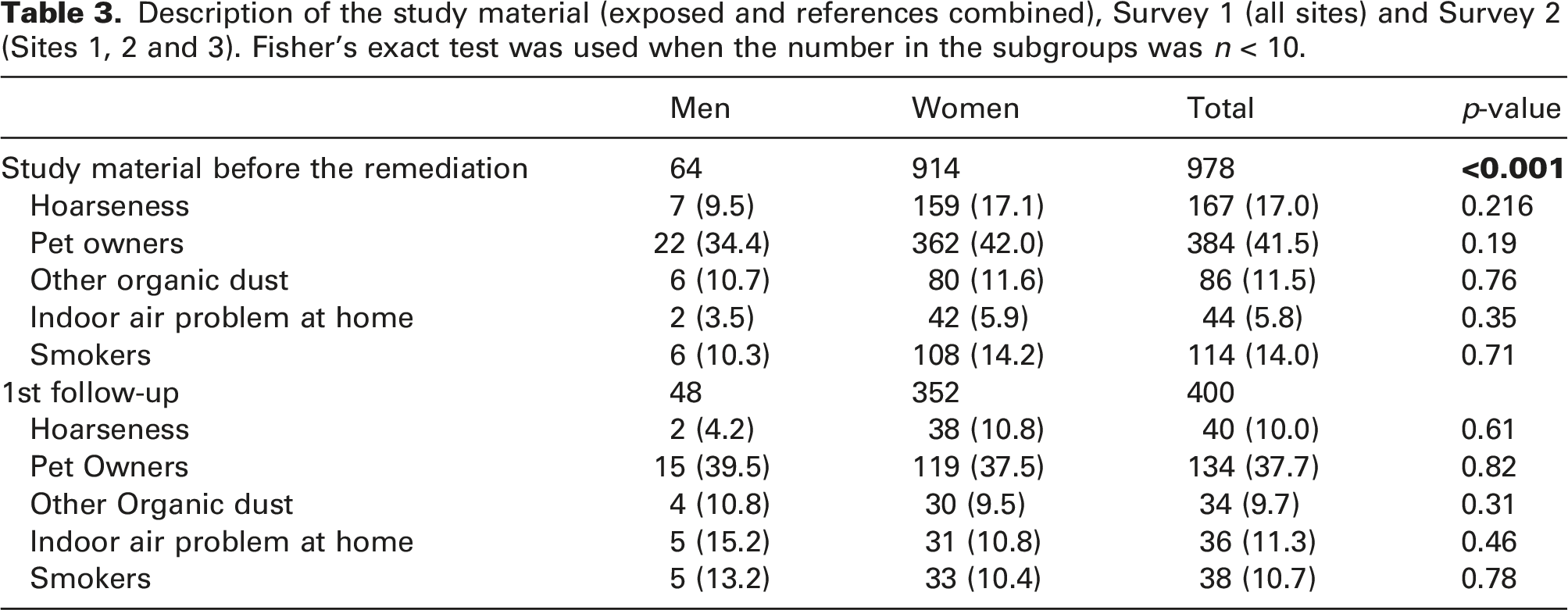
Description of the study material (exposed and references combined), Survey 1 (all sites) and Survey 2 (Sites 1, 2 and 3). Fisher’s exact test was used when the number in the subgroups was n < 10.
Prevalence and risk factors for hoarseness
Overall, 17.0% of respondents reported hoarseness at least every week, 9.5% of men and 17.1% of women. The difference between the genders persisted during the follow-up, but the difference was not statistically significant. Hoarseness did not correlate significantly with moisture damage at home, current smoking or having pets. The highest prevalence of hoarseness was amongst ex-smokers (24.0%, p = 0.07, data not shown).
When considered by the main profession, the following had hoarseness at least every week before the remediation: 11% of the cleaners, 21% of the secretaries, 20% of the nurses, physiotherapists and assistant nurses, 16% of the dentists, 18% of the physicians and 10% of the dental nurses and 10% of the kitchen staff. The differences between the occupational groups were not statistically significant (data not shown).
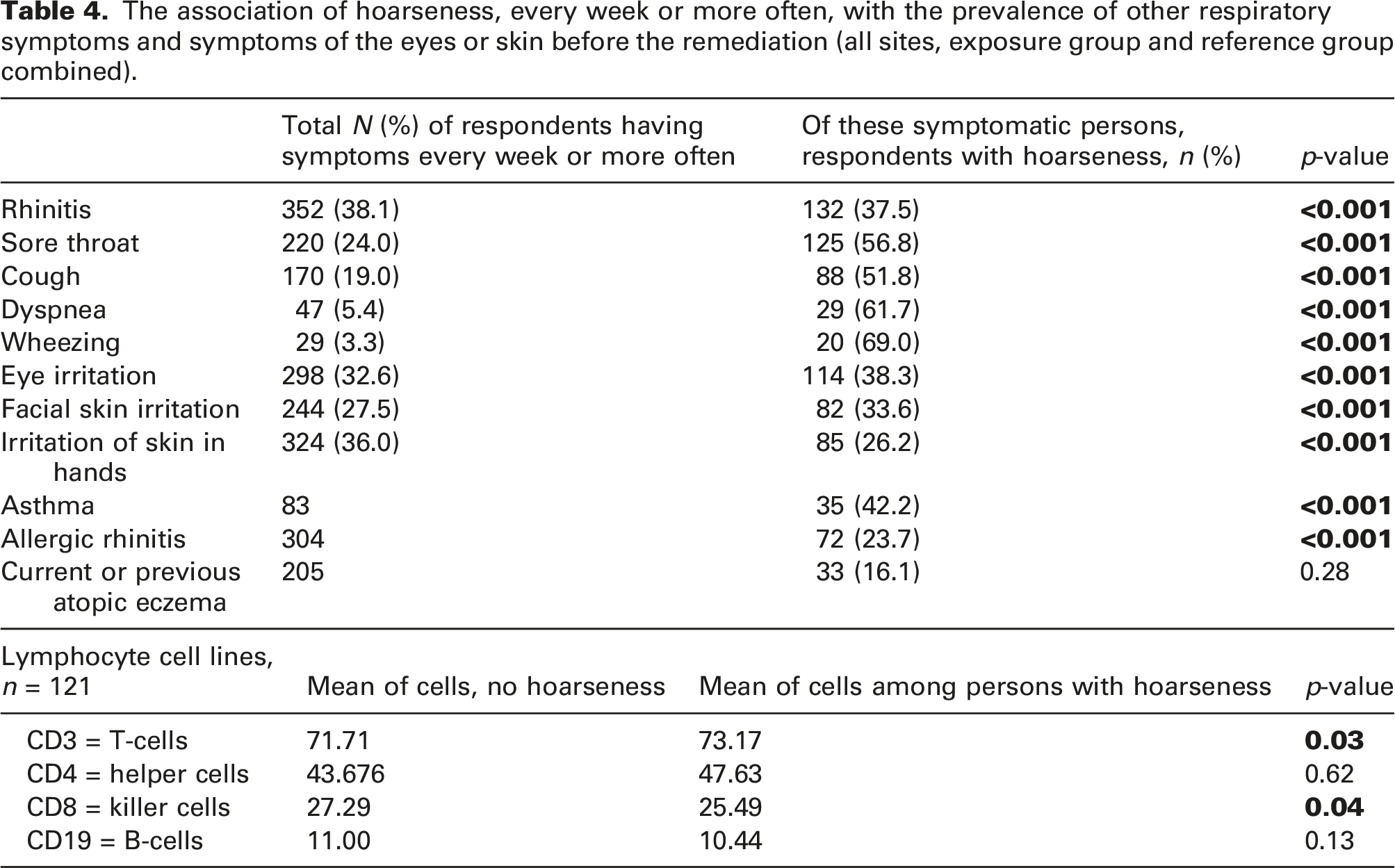
The association of hoarseness, every week or more often, with the prevalence of other respiratory symptoms and symptoms of the eyes or skin before the remediation (all sites, exposure group and reference group combined).
Before the remediation, the hypersensitivity tests of the 212 individuals using the prick test method and ALK extracts did not show any correlation with the reported hoarseness. However, there was often less SPT positivity in the respondents with hoarseness than in respondents with no hoarseness, but the difference was not significant.
Of the 284 persons tested, only 2% were IgE positive against mites and 2.8% IgE positive against moulds, but none of the respondents with hoarseness had IgE positivity against mites or moulds (p = 0.20 and 0.54, respectively, data not shown).
Respondents with hoarseness had significantly higher T-lymphocyte (CD3+) levels in their peripheral blood than non-symptomatic participants (p = 0.03 and p = 0.04, respectively). Both T helper-cell (Th) (CD4+) and T regulatory-cell (Treg) (CD4+CD25+) populations were significantly higher and the level of the T killer cell (Tk) (CD8+) population was significantly lower amongst those with hoarseness compared to those with no hoarseness. No significant difference was observed between these two groups when B lymphocyte (CD19+) populations were compared (Table 4).
Before the remediation, the associations with hoarseness and building damage and unpleasant smells in the indoor air remained consistent and statistically significant when adjusted for age, gender, smoking and asthma in a logistic regression model. Age, smoking and asthma were significant risk factors as well (age: OR 0.96, CI 0.94–0.98; smoking OR 1.50, CI 1.18–1.90; asthma: 8.44, CI 4.49–15.84, respectively). The risk of building damage causing hoarseness was 2.57 (CI 1.63–4.05) and for unpleasant smells in indoor air causing hoarseness was 1.48 (CI 1.22–1.79).
Respondents who had unpleasant smells in the indoor air at their workplace had significantly higher T-cell levels (CD3-cells) in the peripheral blood than individuals who less often or not at all were subjected to indoor smells (115 persons tested, p < 0.05). The difference in CD3-cells in buildings with technical damage compared to the reference buildings was similar, but not statistically significant (p = 0.26).
After the remediation, the reduction in hoarseness amongst nurses and assistant nurses was more evident (7.5% and 8.4%, respectively) than amongst medical doctors or dentists (10.5% and 10.7%, respectively). The prevalence of hoarseness remained relatively high after renovation amongst the secretaries (15%) and physiotherapists (15%), but the number of respondents in these groups was very small. The differences between professions were not statistically significant (data not shown).
Hoarseness and work environment factors
The overall prevalence of hoarseness had a strong correlation with the indoor air problem. Hoarseness was strongly associated with indoor air damage assessed by construction engineers (p < 0.001). After remediation, the follow-up showed a clear reduction from 19% to 10%, while in the reference buildings hoarseness was reported by 9% of respondents. After the 4-year follow-up, the prevalence was 8%, but the drop-out rate was high and only 38 individuals responded to the last survey.
Hoarseness correlated significantly with subjective annoyance due to indoor air factors, but the association was not linear. The highest prevalence of hoarseness was in the category of annoyance ‘more seldom’ and the lowest in the category ‘never’. If the annoying factor occurred ‘daily’ or ‘every week’, the hoarseness was considered to be on an intermediate level. On the other hand, mould odour which had a strong correlation with hoarseness before the remediation was no longer significant after the remediation; only 5 respondents mentioned mould odour after the repair. The same association was observed with cellar-like odour, and the significant association (p < 0.001) became non-significant after the repair. Other smells did not correlate with hoarseness. Visible signs of moisture damage or leaks correlated strongly with hoarseness before remediation, but not after the repair work (p < 0.001 and p = 0.57, respectively). Hoarseness did not correlate with visible mould growth, which was rare and difficult to observe. Hoarseness was strongly associated with a perceived lack of or insufficient ventilation and this association remained after the remediation.
We found an association between the floor on which the employee worked and the prevalence of hoarseness. In the undamaged buildings, the highest prevalence of hoarseness was found in the basement and lower numbers on the upper floors. No similar trend was observed in the moisture damaged buildings.
Hoarseness was associated with poor general job satisfaction (p = 0.048), but not with respondents’ opinion of the job being generally interesting and inspiring (p = 0.44). Hoarseness was associated with an excessive workload (p = 0.02) and poor possibilities of controlling one’s work or working conditions (p < 0.001). Good support from peers was also correlated with a high prevalence of hoarseness before the remediation, but not after the repair work.
Hoarseness was strongly correlated with irritation symptoms in the airways, the eyes and the skin, and these symptoms diminished after the remediation (data not shown). Respondents with hoarseness often consumed more prescribed medication than respondents with no hoarseness. Body mass index (BMI) did not correlate with hoarseness.
After the remediation in three of the buildings, hoarseness diminished to 10.4%. Age, gender and smoking were no longer significant risk factors. Working in a former problem building was no longer a significant risk factor, either (data not shown).
Discussion
In our study material from approximately 1000 workers in 13 buildings, almost one fifth of the health care workers had hoarseness at least every week or more often. Female gender was also a clear risk factor for health care professionals, similar to the findings for other professionals, for example, teachers. 1 Amongst health care professionals, smoking was relatively rare, and it did not explain hoarseness, neither did pet owning or indoor air problems at home.
We found relatively large differences between different occupations, for example, secretaries, assistant nurses and cleaners, compared with medical doctors, dentists and nurses. Our findings are in line with recently published large national data on nurses; however, for health care centres, the prevalence of hoarseness was clearly shown to be on a lower level than amongst nurses in general in Finland. 20 Vertanen-Greis et al. 1 found a much higher prevalence of hoarseness and voice problems amongst teachers in a recently published paper. 1 Based on international data, we suspect that the prevalence of hoarseness and other voice problems are probably increasing, but currently on a national level there is too little data to draw any conclusions about this trend.
The pathophysiological mechanisms behind hoarseness remain partly obscure, but previous publications suggest that noise in the work environment, irritant gases, dust, respiratory infections, stomach problems and certain medical drugs may have an effect on the origin of hoarseness.9,10 Our data supports the hypothesis that hoarseness is more often due to irritation of larynx than an allergic reaction. We found no significant correlation between hoarseness and sensitization to common aeroallergens, dust mites or moulds. Chemicals used in dentistry are unlikely to cause large scale voice problems, as the results in our material show that secretaries, cleaners and physiotherapists often had more voice problems than dentists or dental nurses. Medical doctors and dentists had hoarseness equally often in the health care facilities in our material.
In previous publications, moisture and mould damages have been connected with several respiratory symptoms, and also with hoarseness. Hellgren and coworkers 4 found a connection with symptoms and insufficient ventilation in hospital buildings and Vertanen-Greis 1 in school buildings.1,4 Indoor air problems have been investigated less often in primary health care centres or wards.
Follow-up studies on indoor air research are rare. Several studies have been published showing the beneficial health effects on pupils and teachers after remediation,21–25 and the benefits in office buildings.26,27 In a 6-year follow-up study of one health care centre, no beneficial health effect was found in spite of remediation. 28 All previous studies have been conducted using relatively small amounts of reference materials, a short-time follow-up or where only one building was investigated with no reference materials. Hoarseness is a typical symptom in facilities with indoor air problems amongst both children and adults.1,29 In some cases, the remediation processes are poorly documented. Therefore, it is difficult to analyze why the remediation is sometimes successful and sometimes fails.
According to Mori and coworkers, 30 the risk of hoarseness is high in professions, such as arts and entertainment (RR 4.98, CI 4.18–5.95), law (RR 3.24, CI 2.48–4.23), education (RR 3.08, CI 2.70–3.52) and social services (RR 2.07, CI 1.57–2.73). In contrast, many occupations had significantly reduced risk of the presentation of laryngological disorders, for example, maintenance (RR 0.25, CI 0.15–0.42), food preparation (RR 0.35, CI 0.26–0.48) and administrative support (RR 0.49, CI 0.41–0.57). Our study findings contradict Mori’s 30 material, because, for example, secretaries in health care centre wards had a high prevalence of hoarseness.
Our study material showed no association between hoarseness and IgE-mediated hypersensitivity. This is somewhat surprising because many indoor air researchers have been focused on the documentation of IgE-mediated asthma and allergies amongst the exposed.31–35 Many previous studies have investigated children, and they might more often have IgE-mediated responses than adults. Only a proportion of adult-onset asthma has an IgE-mediated origin. In our study, hoarseness was strongly associated with asthma but not with SPT positivity or an IgE response. Impaired voice quality and various grades of dysphonia occurred in almost every sixth of asthmatics, caused by either respiratory decline, or as a side effect of medication or both together. 36 Even though asthma medication may irritate the larynx and cause hoarseness, 37 the association between hoarseness and asthma might be due to other mechanisms than IgE-mediated hypersensitivity.
Instead of IgE-mediated hypersensitivity, we found an interesting association between lymphocyte levels and hoarseness. We found lower levels of T-cells and higher levels of killer cells in patients with hoarseness. Killer cells were also found to be at a higher level in buildings with moisture damage, but the difference was not statistically significant. In workplaces where indoor air has unpleasant smells, T-cells were at a significantly higher level than in work environments with no smells. To the best of our knowledge, this is the first study to show a simultaneous association with lymphocyte cell lines, symptoms experienced by workers and working conditions defined objectively by construction engineers and microbial samples. The odds ratio for indoor air problems examined by trained construction engineers was 2.6 (CI 1.63–4.05) when age, gender, asthma and smoking were controlled with a logistic regression model. The risk factor, moisture and microbial damages in a building are biologically plausible as an irritant but were found to be lower than, for example, in Mori’s 30 highest occupational groups and higher than, for example, teachers or social services.
When considering the immunological data, although it is quite inadequate to draw conclusive deductions, it is still interesting enough to discuss the role of the immune system as one effective agent in hoarseness. Firstly, it was observed in this study that the IgE levels were not elevated against the measured antigens in the hoarseness group, which seems to exclude the Th2 type I hypersensitivity reactions.38,39 Secondly, the elevated microbe-specific IgG levels in the serum were observed in the patient group without hoarseness indicating a Th1-type immune pattern. This seems to have a protective effect in the case of hoarseness, as it has been shown earlier amongst teachers. 23 Further analysis is already ongoing in our research unit. More evidence is required, but it is plausible that the Th1 orientated immune pattern guards the human body at least against type I hypersensitivity reactions also in the case of indoor exposure to microbes and other allergens.8,40,41 We have previous experience from a similar phenomenon in our earlier study, when increased microbe spore–specific IgG levels in building users correlated with the severity of microbe damage, but not with the severity of building users’ symptoms at the group level. 42 Thirdly, it was observed that the T-lymphocyte level was significantly higher in peripheral blood in respondents with hoarseness compared to that of the non-symptomatic participants. This divergence was assumed to be the result of the elevation of Th cell and Treg cell populations and the decrease of the Tk cell populations in patients with hoarseness. However, there was no difference between the peripheral blood B cell populations. While the significance of these findings for hoarseness is somewhat speculative, we can discuss the type IV hypersensitivity reaction in this respect. Because the mechanisms behind hoarseness and other voice problems are largely unknown, we hypothesize that this reaction which is derived from T-cells (Th1 cells) may be related to hoarseness. This is supported by the empiric observation that systemic corticosteroids tend to reveal voice symptoms better than antihistamines. In order to find the relevance, deeper immunological research with a larger cohort and a longer follow-up is needed to reveal the Th1/Th2 distributions, in order to differentiate T-cell subpopulation and other immune cell populations like macrophages and to define the existing cytokines and other inflammatory markers. At this point, we have no cell analysis in the follow-up material after the remediation process.
Strengths and weaknesses
The strength of our study is its relatively large amount of data representing typical primary health care facilities in several municipalities and towns in different parts of Finland. A further strength is that the exposure assessment of buildings was performed by trained professionals and not simply by respondents themselves. Microbiological samples from the buildings, SPT tests and the collection of blood samples are objective measurements of the exposure and the immunological status of the study population as a proxy of subjective annoyance and adverse health effects. All the surveys were conducted with the same validated questionnaire that has been in use for several decades in Nordic countries and elsewhere.12,15 The surveys were repeated at the same time of the year to avoid the effect of the pollen season and other seasonal variations, and the recall period was 12 months. As all building condition reports were done by experts outside of our study group, variables like the time of sampling of microbiological samples, or the effects of seasons on the buildings, or the architectural forms of the buildings, were therefore not taken into account. Another strength is a sufficient follow-up period of two to 4 years to enable a recovery process after the remediation and removal of building dust and chemicals used during the repair.
On the other hand, only a part of the original study population took part in the follow-up, and the follow-up procedure should have included a more thorough monitoring of exposure, follow-up measurements of clinical lung function measurements and immunological parameters. Many municipalities were reluctant to participate in the follow-up because they either had no resources for remediation or because the problem building had been demolished (one case). Clinical follow-up studies are costly and require a long-term commitment from all participants in the process, both employers and employees.
One of the weaknesses of the study is that the participants were aware of the exposure. This cannot be avoided in situations where the damage is visible, for example, leakage through the roof, flooding, visible mould growth on surfaces or strong unpleasant smells. On the other hand, medical and nursing staff are used to smells, microbes and chemical exposure related to their work and take everyday risks more calmly than laymen involved in office work or, for example, teachers who are often concerned about their pupils’ health as well as their own. On the other hand, the individuals participating in the follow-up had a positive attitude to the remediation and were anticipating that the situation would improve.
In the future, longer follow-up periods will be needed to discover the long-term effect of the remediation techniques and the recovery time as well as the final effect on respondents’ work ability and length of careers. Karvala and coworkers 8 have previously shown the harmful effects of long-term exposure on the length of working life in a 10-year follow-up study. Her material consisted of more than 1000 workers with diagnosed or suspected work-related asthma and the risk of an early pension was six times higher than amongst those not exposed. 8
Conclusions and recommendations
This study shows a relatively large difference in the occurrence of hoarseness amongst health care personnel in buildings with indoor air problems and building damage compared with health care professionals carrying out similar work but in buildings with no damage. We found no association with IgE-mediated sensitization, but a preliminary finding of an association with lymphocyte cell lines amongst the exposed. The follow-up shows the beneficial effect of the remediation of buildings without any other therapeutic intervention or treatment. Prompt and effective remediation of moisture damaged buildings is recommended before the occurrence of irreversible diseases such as asthma or impairment in workability. Longer follow-up studies with larger datasets are needed.
Footnotes
Acknowledgements
The study group greatly appreciates the financial support from the Finnish work environment fund (no: 210375) and the Parliament of Finland. The study group thanks all persons who participated in the study and the municipalities who financed the thorough remediation of the buildings.
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Työsuojelurahasto (210375) and Parliament of Finland.