
Abstract
Building-related health symptoms are multifactorial, hence a comprehensive study is needed to identify associations of such symptoms with building aspects. Previous studies have identified certain building characteristics as risk factors for both dry eyes and headaches, which are among the most prevalent symptoms suffered by office workers. This study investigated associations of dry eyes and headaches with building characteristics in outpatient areas because these conditions may vary between office and hospital buildings. A survey was performed in six hospital buildings, which included administering a questionnaire to 556 outpatient workers and an inspection of the building locations, services and 127 outpatient rooms. Multivariate regression models were produced for dry eyes and headaches. Both models were adjusted for personal and work-related aspects. The prevalence of self-reported dry eyes and headaches in outpatient areas was related to building-related aspects that affect the indoor air quality and visual quality, and to room types. In general, this study is consistent with previous office studies. However, a specific finding of this study is the association of the most frequently used room types and the presence of a window to the corridor with dry eyes and headaches.
Introduction
Since the demand on healthcare is growing, driven by an ageing population, risks for pandemics, and an increasing prevalence of chronic diseases, 1 the pressure on hospital staff is increasing. To better understand relations between comfort and health of hospital staff and the physical environment is important, because comfort and health of hospital staff may be affected negatively by the physical environment.2,3 Furthermore, the hospital workers’ satisfaction, production and wellbeing can be supported by the physical environment,4–7 while satisfaction of staff may be beneficial for patients as well.8–11 Among health problems, that can be influenced by building characteristics, are building-related symptoms. Building-related symptoms have been identified as a societal problem that may affect the occupants’ physiological and psychological health negatively. 12 Other adverse effects of building-related symptoms can be sick-leave13,14 or a decrease in productivity. 15
Building-related symptoms are symptoms of an unclear aetiology, related to the eyes, nose, throat, skin, headache and lethargy. 16 Self-reported health symptoms are defined as building-related symptoms that occurred when the occupants are in the building, and improved when away from the building. 16 The symptoms can be identified by a standardized questionnaire, administered to building occupants. 17
The prevalence and causes of building-related symptoms of office workers are mostly investigated, but also of occupants in schools, homes and hospitals. 18 Rashid and Zimring 2 suggested that comfort and health may vary between occupants in offices, hospitals and hospital departments (e.g., inpatient wards, intensive care units, operating rooms), due to differences in performed activities, duration of stay, etc. A review on field studies in hospitals concluded that hospital staff was generally less satisfied with comfort than patients, and outpatient areas were understudied as compared to other departments. 19 Previous studies indicate a higher prevalence of self-reported health symptoms in hospitals than in offices.20–22 Dry eyes and headaches are among the most reported building-related symptoms.
For example, in OFFICAIR, a study with 7446 office workers in Europe, almost one third of the office workers suffered from dry eyes or headaches, which were the most prevalent symptoms. 23 In a study with 556 outpatient workers of six hospitals in the Netherlands, half of the outpatient workers suffered from dry eyes, and more than one third from headaches. 21 Also in this study dry eyes and headaches occurred more frequently than other mucosal, skin or general symptoms. While previous studies on building-related symptoms have been performed in hospitals,24–28 analysis of building-related aspects with dry eyes or headaches was limited. Studies on associations of headaches or dry eyes with building-related aspects were mainly performed in office buildings.29–33
Dry eyes and headaches are common health complaints,34,35 that both have a multifactorial character, affected by genes, personal, work and environmental aspects.36,37 With regards to specifically building-related dry eyes and headaches, previous studies indicated that also building-related symptoms can be influenced by personal and work-related aspects.12,16 For example, the perception of building-related symptoms can be influenced by gender, smoking status, psychological state and work pressure of the occupants. Therefore, to identify possible causes of building-related symptoms, Bluyssen 38 has recommended studying comfort and health integrally, including personal and work-related aspects as well as building-related aspects.
Because of the high prevalence of dry eyes and headaches found in outpatient areas of six hospitals buildings, 21 the present study aims to investigate integrally possible building-related risk factors (building characteristics) for having headaches and dry eyes symptoms in those buildings. Therefore, a broad range of building-related aspects, as well as personal and work-related aspects were included.
Method
Study design
This study is part of a survey conducted in hospital buildings in the Netherlands. The survey comprised of a questionnaire regarding the health and comfort of outpatient staff and of a building inspection with the use of a checklist. Detailed information about the design of the questionnaire, selection of the population and buildings, and the procedure of the survey are reported in Eijkelenboom et al., 21 and therefore summarized. The study was performed in Spring 2019 at six locations of three hospital organizations (two locations per organization). Simultaneously to the administration of the questionnaire, the locations were inspected systematically by three researchers. The questionnaire was tested in a pilot study with outpatient staff in a general hospital in Winter 2018.
The Ethics committee of Delft University of Technology approved the study on 5 October 2018. Data security was assessed by a data manager. To respect privacy of the participants, measures were taken for protection of contact information, safe data storage and withholding of personal information. The workers had to give their informed consent for participation. Only participants who agreed to submit at the end of the questionnaire were included in the analysis.
Survey
The questionnaire was based on OFFICAIR 23 and new questions. OFFICAIR was developed to gain more insight in comfort complaints and building-related symptoms of occupants in European offices, with respect to personal, work and health-related aspects. The new questions were specifically developed for this study because no standardized questionnaire was found. To address building-related aspects from the building inspection to the outpatient workers, the questionnaire comprised questions about which location they mostly worked at, which department, which room type they used most frequently, and the presence of a window to the façade and to the corridor. Furthermore, the questionnaire comprised of questions on demographics, psychological aspects (e.g., positive affect (PA) and negative affect (NA)), 39 health (e.g., migraine diagnosed by a doctor), work-related aspects (e.g., effort reward imbalance (ERI), over-commitment), 40 comfort and building-related symptoms (e.g., dry eyes, headaches). The prevalence of building-related symptoms was defined as having occurred in the last four weeks, at least once a week, and that had improved when away from the building.
For an integral inventory of the building-related aspects, a layout checklist, cleaning checklist, building checklist and room checklist were composed. The cleaning checklist was based on national regulations for hospital cleaning. 41 The building checklist and room checklists were based on OFFICAIR and adapted with specific characteristics of outpatient areas, based on visits of hospital buildings, during the preparatory phase. The following aspects, that may affect the perception of comfort or health, were included: possible outdoor pollution sources, façade characteristics, characteristics and maintenance of air handling units, the characteristics of different rooms (e.g., finishing materials, direction of lighting, control of heater and lighting, height windowsill), layout characteristics (e.g., dimensions of building wings, size areas) and cleaning frequency of surfaces and amenities.
Procedure
The questionnaire was digitally distributed by the hospital organizations to all outpatient workers. Participation was voluntary. To systematically inspect aspects that could vary due to room type, the presence of a façade window or renovation periods, rooms were selected and marked on layout drawings, in advance of the building inspection. Facility managers provided explanations of the HVAC-systems in each building, during the building inspection. Observations and oral information were documented on the checklists, drawings and with images. To respect privacy of patients and hospital staff, no persons or patient information were included in the images. The cleaning protocol was provided by the hospital organizations. The data of the building inspection were manually put into a database. The sites and building services of six locations and 127 rooms were inspected.
Data analysis
Relations between building-related aspects and scale levels, such as organization, location, building wing, room type, presence of a façade window, were identified with crosstabs. Building-related aspects were assigned to the respondents, when the aspects identified on different scale levels were consistent.
For error analysis, the data of the questionnaire were checked systematically. Missing value analysis was performed with pre-validated scales, such as PA, NA, ERI and over-commitment, and all items, except for the embedded questions. Descriptive statistics were used to summarize the demographics of the hospital staff. Multivariate logistic regression was used to assess the risk of having headaches and dry eyes related to building-related aspects. Headaches and dry eyes were analysed separately.
First univariate analysis was performed for the building-related aspects, unadjusted and adjusted for confounding variables. Identification of confounding variables for dry eyes was based on literature. Because confounders, additional to the variables from literature, did not affect the inclusion of building-related aspects in the final model, no additional confounders were included. The value of categorical variables that was most likely to differ was used as the baseline value. Sex, age, education, smoking status, alcohol consumption and psycho-social work aspects were included for dry eyes. Due to limited literature on headaches in relation to building-related aspects, associations with building, personal and work-related aspects were adjusted for sex, age and migraine.
Subsequently, aspects associated with a p value of less than 0.20, 42 completeness of more than 80%, and variance of more than 10% for dichotomous variables 43 were used for the final models. The final model for dry eyes was based on three steps: constant only, confounding variables and building-related aspects. The final model for headaches was similarly produced, except for inclusion of additional personal and work-related aspects in the last step. In the last step, the variables with a p value larger than 0.20 were iteratively removed. Then, to assess the prediction of dry eyes and headaches the odds ratio (OR) and 95% confidence interval (CI 95) were calculated. Statistical significance of the OR was checked with the Wald Statistic. Associations were assessed statistically significant if the p value was less than 0.05. To check the reliability, the number of events per variable was calculated as degrees of freedom divided by the lowest number of outpatient staff per event, thus for ‘no headaches’ and ‘no dry eyes’. Values below 10 were considered to decrease the validity of the model. 44 Multicollinearity was checked with the Variance Inflation Factor; values below 5 were considered to have low multicollinearity. The linearity of the continuous variables was checked with interactions with the log transformation of each continuous variable in the final multivariate logistic regression models.
Goodness of fit was checked with the Hosmer and Lemeshow test (p value >0.05). To check whether there were cases that fitted poorly or had a dominant influence on the model, the following values were inspected: the values of Cook’s distance, standardized residuals (SR), the leverage and difference between the constant for all cases and one case excluded (DF Beta). Cook’s distance <1, DF beta <1, less than 5% of SR > ± 1.96 and less than 1% > ± 2.58 and leverage smaller than three times the average leverage were considered as good fit.
45
The average leverage was calculated according to equation (1)

Results
General characteristics of the outpatient workers
Five-hundred and sixty outpatient workers completed the questionnaire; four were excluded because they did not work at a location or department that was part of the survey. Missing values were scattered among the questions. No variables and constructs, such as ERI or NA, had more than 5% missing values.
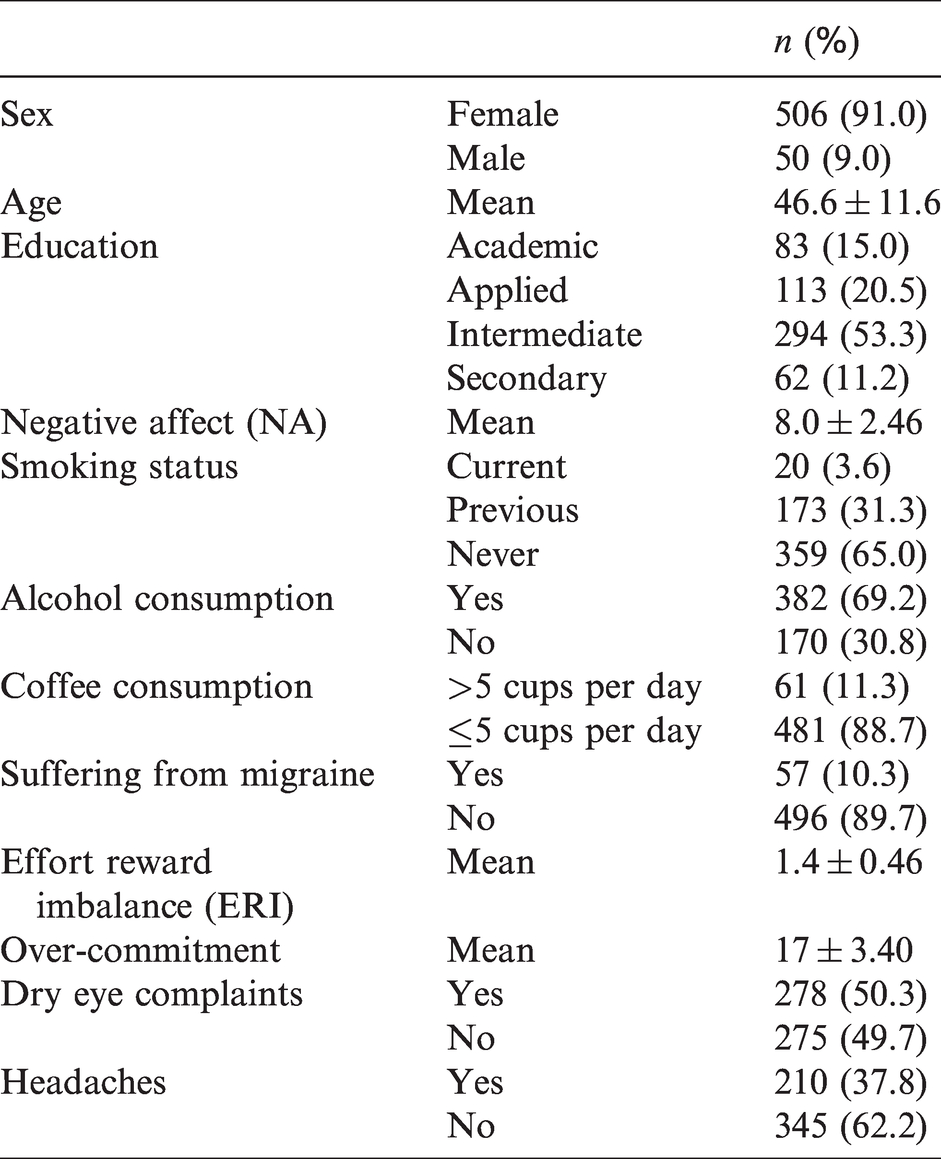
The personal aspects of the outpatient workers are presented in Table 1. The majority (91%) was female, the mean age was 47 years; the youngest was 19 years, the oldest 67. More than half of the outpatient workers (53%) had an intermediate education. The mean NA (scale 5 to 25) was 8. Low values of NA are considered positive. The average ERI was 1.4. Values larger than 1.0 are considered as a larger effort than reward. The average over-commitment (scale 6–24) was 17, with values larger than 14 considered as over-commitment. Half of the outpatient staff (50%) had dry eyes; the prevalence of headaches was 38%.
General characteristics of the outpatient staff.
General characteristics of the buildings
The survey was performed in outpatient areas at six locations of three organizations (two locations per organization). The buildings were built between 1980 and 2013. All buildings, except the building from 2013, comprised of parts that had been renovated and extension parts; three buildings had a temporary wing. Three locations were within 100 m of a highway and 1.5 km of industry, one location was near a forest. The main buildings of each organization had an outpatient area larger than 15,000 m2. Rooms with and without a window to the façade and a window to the corridor were present at all locations. All buildings had a balanced mechanical ventilation system, with air humidified by steam. One building had wings with a climate façade. All buildings had external solar shading. Rooms were heated with radiators, floor heating, or heated air, depending on the building (wing) and presence of a window to the façade. In consultation and treatment rooms blinds or curtains were present to control the view, while control of the view varied between building wings at receptions and in offices. All rooms had acoustical ceiling panels, the main floor covering was hard, with some exceptions for carpet at offices. The walls were mostly painted, while in some building wings the walls had a vinyl finishing. The cleaning schedules varied between the hospital organizations and room types.
Relations between building-related aspects and self-reported dry eyes
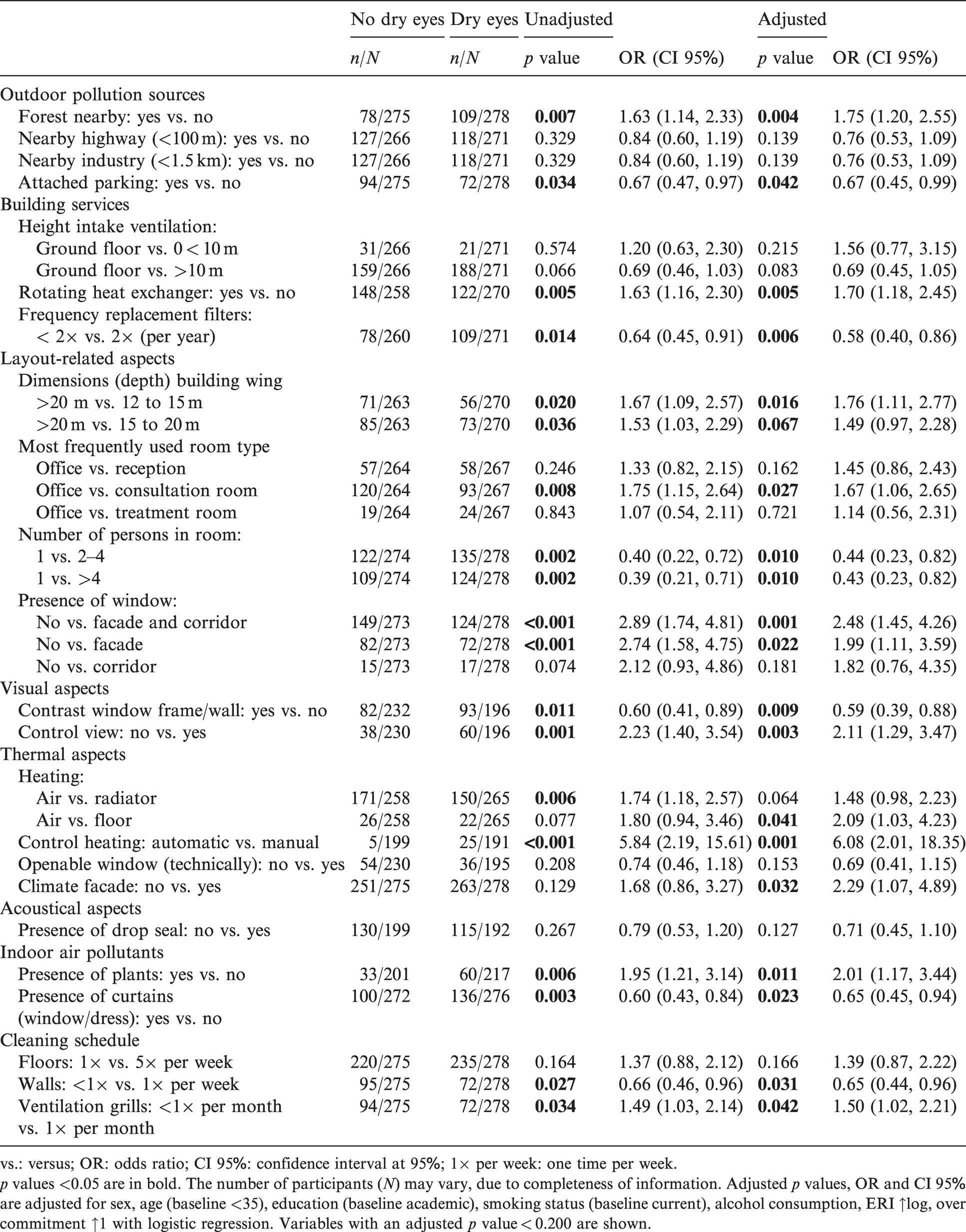
Table 2 shows associations of building-related aspects and self-reported dry eyes from the univariate analysis (fourth and fifth column) and after adjustment for the confounding variables (sixth and seventh column). The first column shows the building aspects with a p value larger than 0.200, because these were relevant for inclusion in the multivariate analysis. The second column shows the number of participants with no dry eyes for a building-related aspect compared to the total number of participants with no dry eyes. For example, of those who worked in a hospital building nearby a forest had 78 participants (n) no dry eyes, while of all participants 275 (N) had no dry eyes. The third column shows similarly the number of participants with dry eyes.
Associations between dry eyes and building-related aspects.
vs.: versus; OR: odds ratio; CI 95%: confidence interval at 95%; 1× per week: one time per week.
p values <0.05 are in bold. The number of participants (N) may vary, due to completeness of information. Adjusted p values, OR and CI 95% are adjusted for sex, age (baseline <35), education (baseline academic), smoking status (baseline current), alcohol consumption, ERI ↑log, over commitment ↑1 with logistic regression. Variables with an adjusted p value < 0.200 are shown.
Dry eyes symptoms were associated (p value >0.05) with location (forest nearby), potential outdoor pollutants (attached parking garage), layout (depth of building wings, most frequently used room types, number of persons in the room), building services (frequency of filter replacement, presence of a thermal wheel for heat recovery), visual aspects (the presence of a façade window and window to the corridor, the contrast of a window frame with the wall, control of the view), thermal aspects (heating by air, manual control of heating, climate façade), potential indoor pollutants (the presence of plants and curtains for the windows or curtains for the dressing area) and the cleaning protocols (cleaning frequency of walls and ventilation grills in the room). The strongest associations (p value ≤0.001, OR ≥2.00) were found for the control of heating and the presence of window to the façade and corridor, compared to rooms without a window.
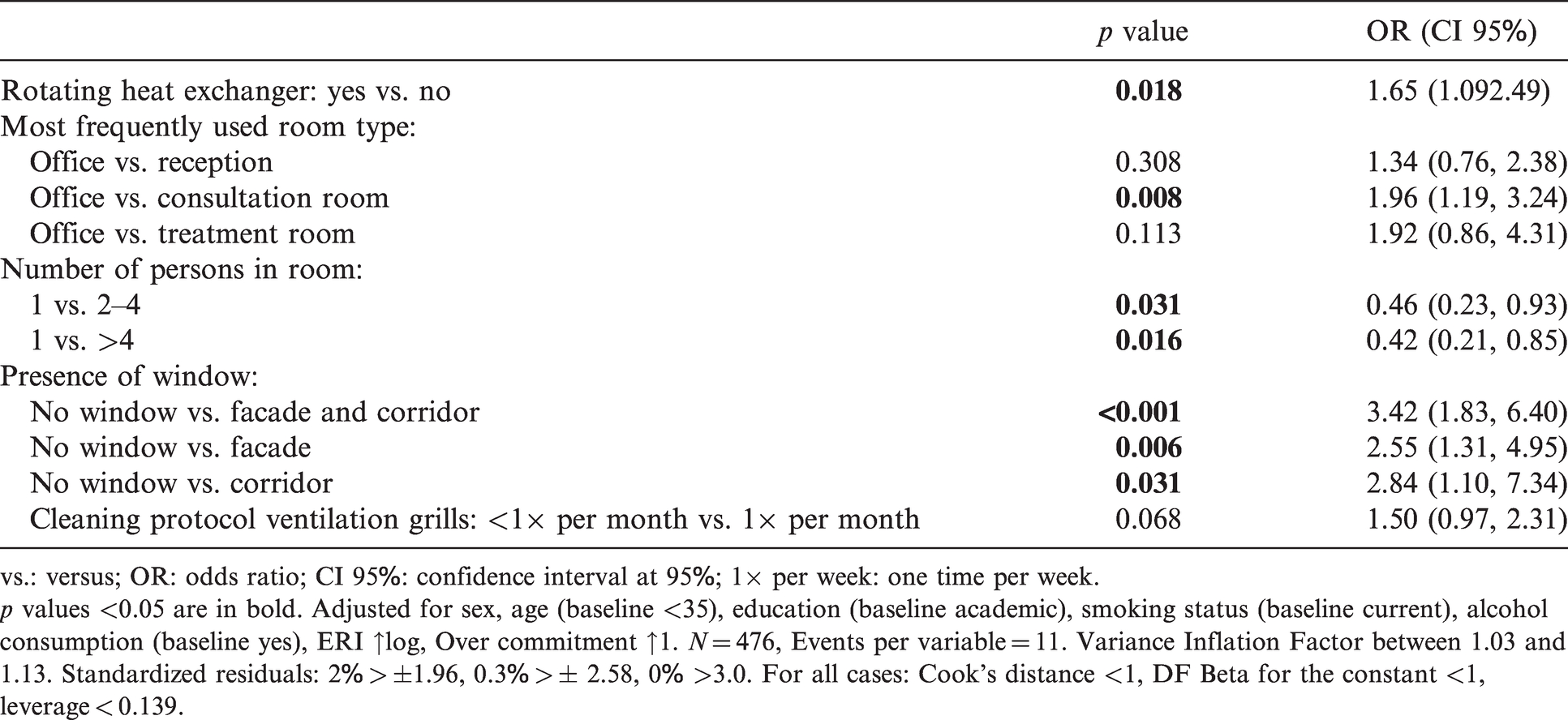
Table 3 shows the multivariate logistic regression model, after adjustment for the personal variables and building characteristics. Dry eyes symptoms were positively related to working in an office compared to working in a consultation room (OR 1.96, CI 95: 1.19–3.24). An increased risk for dry eyes was found for the presence of a rotating heat exchanger for heat recovery in the air handling unit (OR 1.65, CI 95: 1.09–2.49) and the absence of a façade window compared to rooms with a window to the façade and corridor (OR 3.42, CI 95: 1.83–6.40), with only a window to the façade (OR 2.55, CI 95: 1.31–4.95) and with only a window to the corridor (OR 2.84, CI 95: 1.10–7.34). Dry eyes symptoms were negatively associated with working mainly solely in a room compared to the presence of two to four persons in the room (OR 0.46, CI 95: 0.23–0.93) and more than four persons in the room (OR 0.42, CI 95: 0.21–0.85). There was a tendency of a risk for dry eyes (p value <0.20) with working in an office compared to a treatment room (OR 1.92, CI 95: 0.86–4.31), and the cleaning frequency of ventilation grills for air supply and exhaust in the rooms (OR 1.50, CI 95: 0.97–2.31).
Multivariate logistic regression model of associations between dry eyes and building-related aspects.
vs.: versus; OR: odds ratio; CI 95%: confidence interval at 95%; 1× per week: one time per week.
p values <0.05 are in bold. Adjusted for sex, age (baseline <35), education (baseline academic), smoking status (baseline current), alcohol consumption (baseline yes), ERI ↑log, Over commitment ↑1. N = 476, Events per variable = 11. Variance Inflation Factor between 1.03 and 1.13. Standardized residuals: 2% > ±1.96, 0.3% > ± 2.58, 0% >3.0. For all cases: Cook’s distance <1, DF Beta for the constant <1, leverage < 0.139.
Relations between building-related aspects and headaches
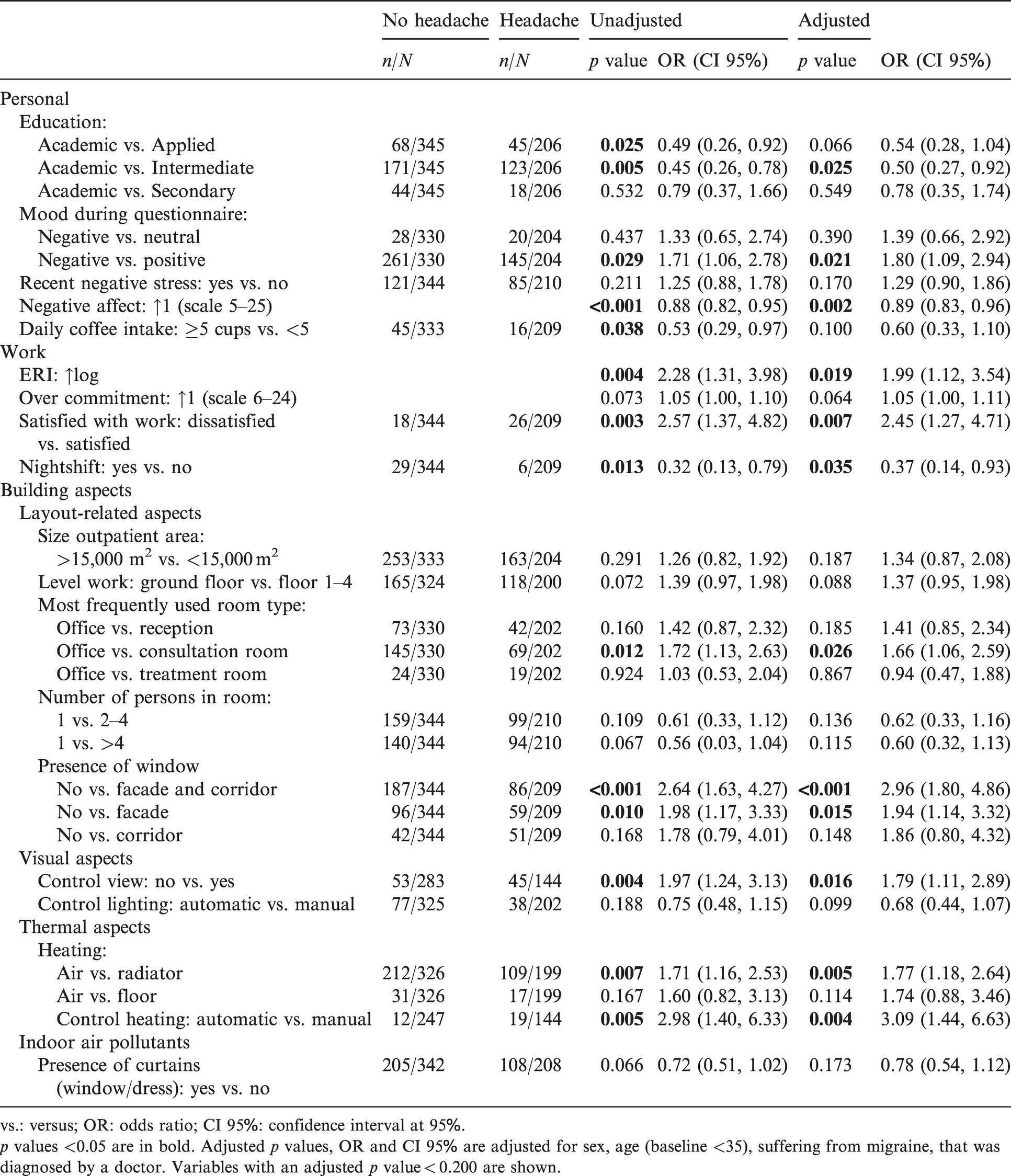
Table 4 shows the associations of personal, work and building-related aspects with self-reported headaches from the univariate analysis and after adjustment. Headaches, adjusted for sex, age and migraine, were associated (p value <0.05) with personal aspects (education, mood while completing the questionnaire and NA) and work-related aspects (ERI, work satisfaction and working in nightshifts). There were associations of headaches with layout (most frequently used room type), visual aspects (presence of a window to the façade and corridor, presence of a window to the facade, control of the view) and thermal aspects (the presence of a radiator, individual control of heating). The strongest association (p value <0.001, OR >2.0) was the presence of a window to the façade and corridor (in comparison to no window).
Associations of personal, work and building-related aspects with headaches.
vs.: versus; OR: odds ratio; CI 95%: confidence interval at 95%.
p values <0.05 are in bold. Adjusted p values, OR and CI 95% are adjusted for sex, age (baseline <35), suffering from migraine, that was diagnosed by a doctor. Variables with an adjusted p value < 0.200 are shown.
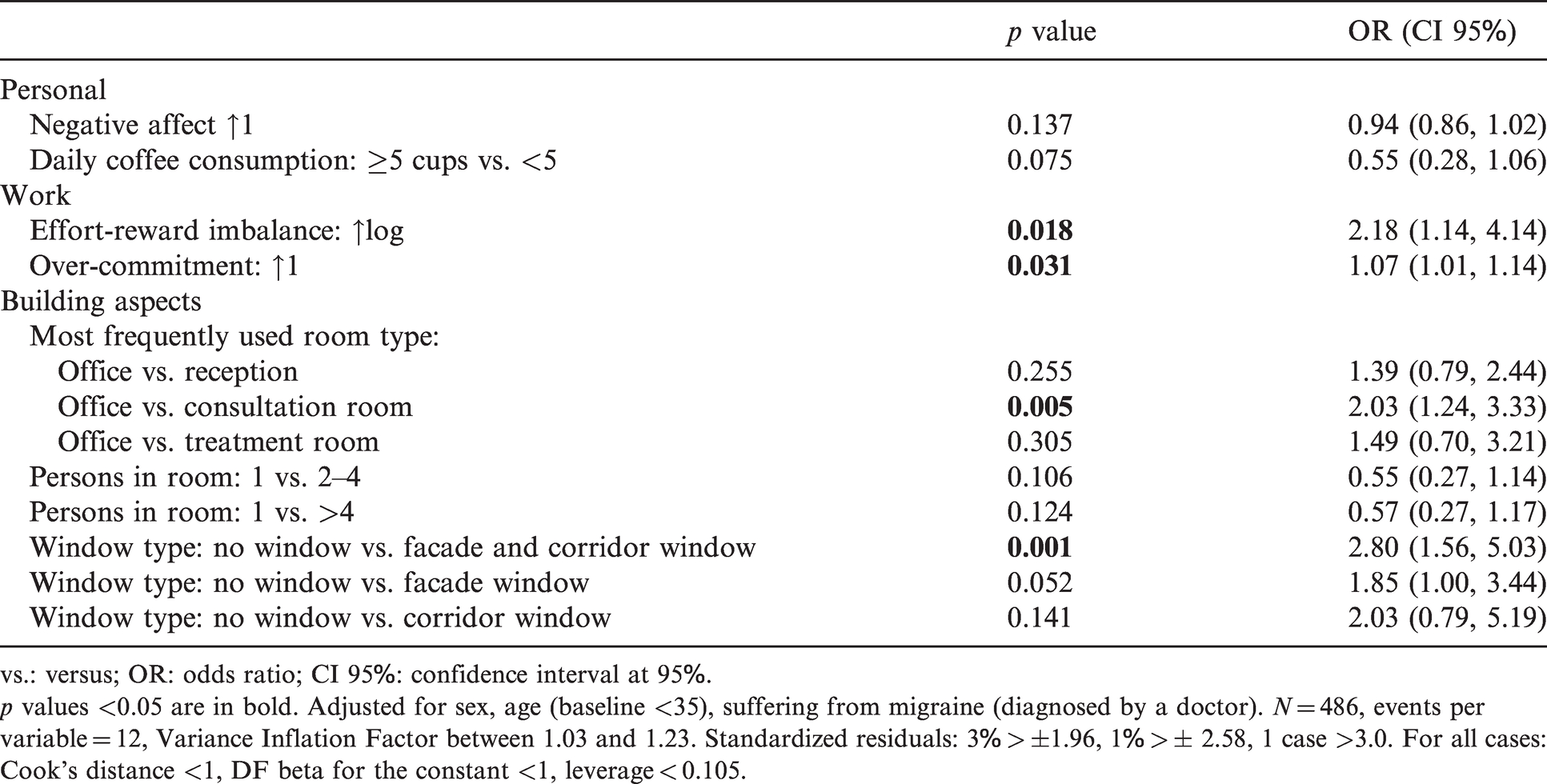
Table 5 shows the multivariate logistic regression model of associations between headaches and personal, work and building-related aspects. Concerning work-related aspects were ERI (OR 2.18, CI 95: 1.14–4.14) and over-commitment (OR 1.07, CI 95: 1.01–1.14) risk factors for headaches. The risk for headaches was higher for working in an office than working in a consultation room (OR 2.03, CI 95: 1.24–3.33). Also, the absence of a window was a risk factor in comparison to the presence of a window to the façade and corridor (OR 2.80, CI 95: 1.56–5.03). There was a tendency to increase the risk for headaches with the absence of a window compared to the presence of solely a façade window or corridor window. With regards to personal aspects, tended NA to increase the risk for headaches and coffee consumption to decrease the risk for headaches (p value <0.20). Also, the presence of others in the room tended to increase the risk for headaches.
Multivariate logistic regression model of associations between headaches and personal, work- and building-related aspects.
vs.: versus; OR: odds ratio; CI 95%: confidence interval at 95%.
p values <0.05 are in bold. Adjusted for sex, age (baseline <35), suffering from migraine (diagnosed by a doctor). N = 486, events per variable = 12, Variance Inflation Factor between 1.03 and 1.23. Standardized residuals: 3% > ±1.96, 1% > ± 2.58, 1 case >3.0. For all cases: Cook’s distance <1, DF beta for the constant <1, leverage < 0.105.
Discussion
The data allow a first assessment of associations between building-related aspects and dry eyes and headaches of outpatient workers in the Netherlands, accounting for an extensive range of building, personal and work-related aspects. As can been seen in Figure 1, the study identified building-related aspects that were a risk for dry eyes and headaches, building-related aspects that were a risk for dry eyes and tended to be a risk for headaches, and building-related aspects that were or tended to be only associated with dry eyes. No building-related aspects were indicated that were only associated with headaches. The building-related aspects that were associated with dry eyes and headaches were work in an office versus consultation room and the absence of windows to the façade and corridor. Additionally, the occurrence of dry eyes was associated with the presence of a rotating heat exchanger, absence of windows to the corridor, absence of windows to the façade and number of persons in the room. The last three tended to be associated with headaches. Dry eyes tended to be associated with the cleaning frequency of the ventilation grills and work in an office versus treatment room. These findings suggest that building-related aspects are a risk factor for the perception of dry eyes and headaches in outpatient areas of hospitals.
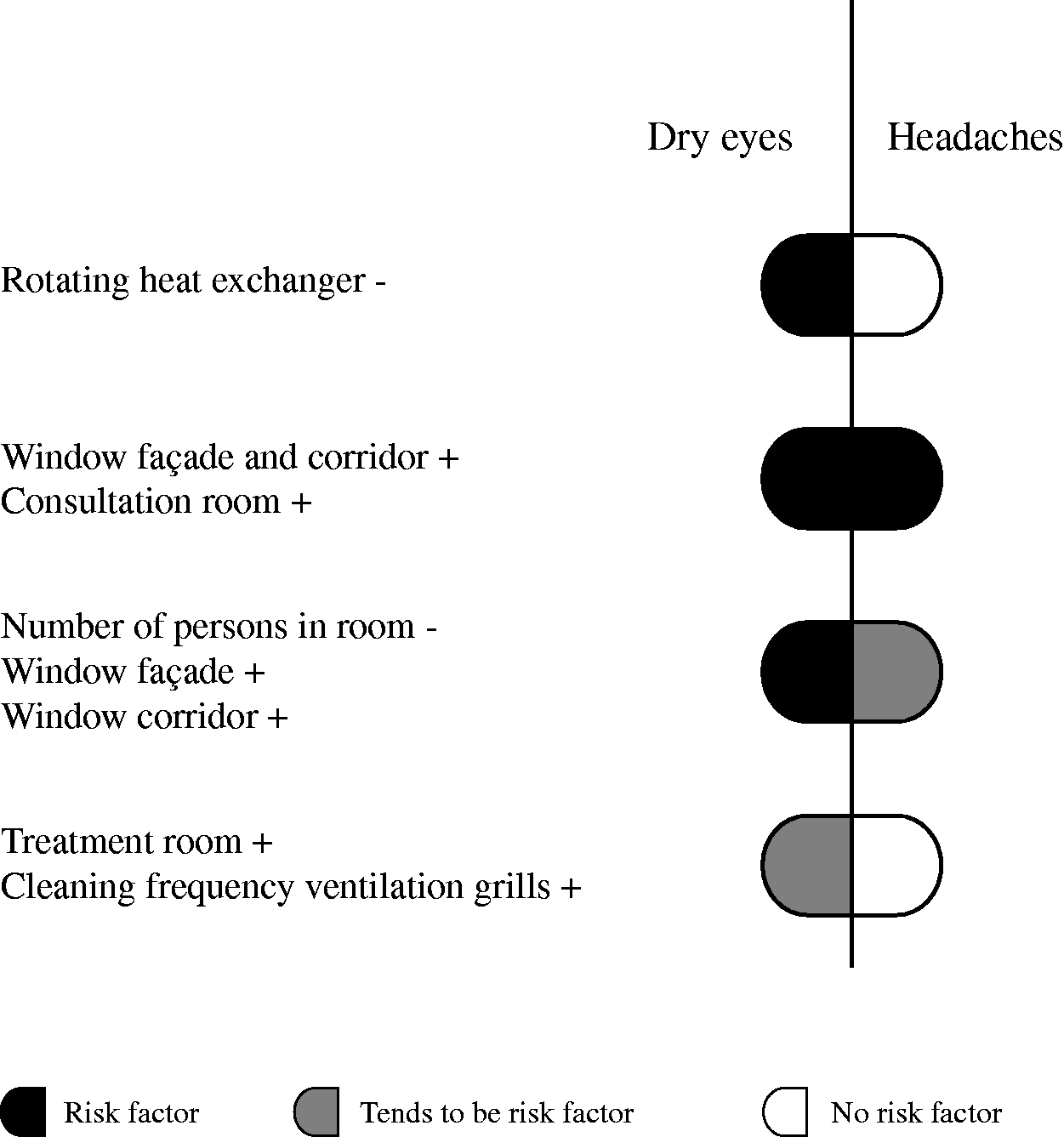
Risk factors for dry eyes and headaches.
Comparison with previous studies
Previous studies identified building characteristics as risk factors for dry eyes and headaches of office workers (see Table 6 for detailed information). All studies were cross-sectional, except the Boston Study 30 which was an epidemiological study. All studies used multivariate regression models, adjusted for personal confounding variables. However, the seasons and geographic locations varied. Also, the studied building characteristics varied between the studies. For example, in the US EPA study 31 maintenance and design of the heating ventilating and air conditioning (HVAC)-systems were studied. The Japan Office Study 32 included maintenance of the HVAC-systems and some general building aspects, such as floor area, number of storeys, construction year, 46 while the CHBS study 29 included ventilation type, general building aspects and measurements of indoor environmental parameters. The Boston study 30 included self-reported workplace characteristics and measurements of dust, while OFFICAIR 33 included a broad range of building-related aspects, such as maintenance and characteristics of HVAC-systems, finishing materials, cleaning protocol, number of floors and workers. In the US EPA study, 31 the Boston Study 30 and the Japan Office Study, 32 dry, itchy, irritated or dry eyes were asked as one symptom, while in OFFICAIR 33 and the present study watering, itchy eyes was a separate symptom. Because of the differences in the definition of dry eyes, seasons, geographics and inspected building characteristics, comparison is not straightforward.
Characteristics of previous studies on building-related dry eyes and headaches.
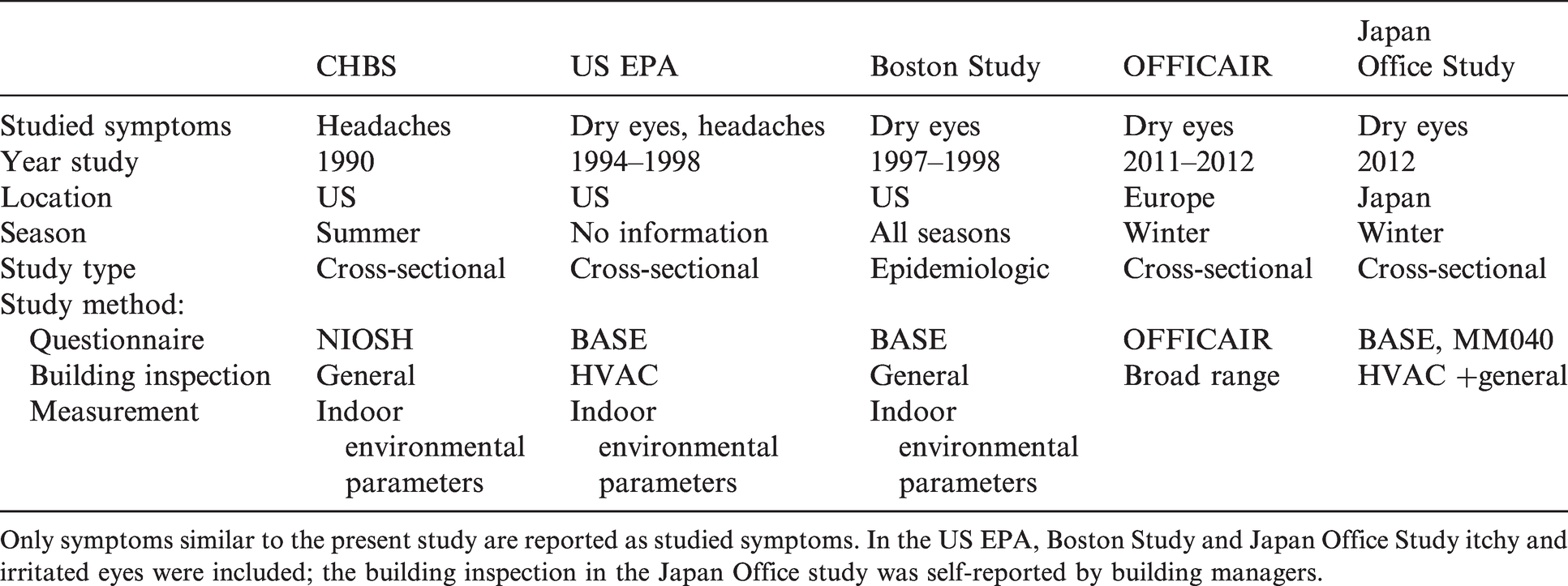
Only symptoms similar to the present study are reported as studied symptoms. In the US EPA, Boston Study and Japan Office Study itchy and irritated eyes were included; the building inspection in the Japan Office study was self-reported by building managers.
The association of dry eyes and the presence of a rotating heat exchanger may be explained by exposure to potential pollutants in the indoor air. Previous studies 47 found that pollutants in the exhausted air may be passed to the supplied air through leakage, adsorption and desorption in a rotating heat exchanger. For example, an experimental study in an auditorium and laboratory, indicated that some common building-related VOCs that were injected in the extract duct of the ventilated place, were recycled from the exhaust to the supplied air through adsorption and desorption in the rotating wheel exchanger. 48
Associations of dry eyes with HVAC aspects were also found in the OFFICAIR study 33 and the US EPA study. 31 The specific building-related aspects that remained in the multivariate analysis of previous studies (respectively the presence of portable humidifiers, the maintenance of AHUs and cleaning frequency of cooling coils) were different from each other and from the present study. This can be related to differences in the study design, variation of building-related aspects with previous studies. For example, in the present study no portable humidifiers were found during the building inspection, while all buildings were provided with steam humidifiers, with water heated above 100°C, to disinfect microorganisms. However, in line with previous studies, impurities that remain in the indoor air, due to characteristics of HVAC-systems, may be a risk factor for dry eyes in outpatient areas.
The negative associations of dry eyes and headaches with the presence of a façade window can be multifactorial. It might be related to the control of fresh air supply and the possible removal of contaminants in the indoor air through natural ventilation in rooms adjacent to the façade, with a technically openable window. In the present study, 81% of those working most frequently in a room with a façade window could ‘technically’ open the window. In OFFICAIR, 33 the presence of technically openable windows was also negatively associated with dry eyes. The occupants who worked at an office without openable windows were more likely to suffer from dry eyes. In contrast, the US EPA study 31 did not indicate increased eye symptoms and headaches with openable windows. However, they suggested that this could be explained by the strong correlation of sealed windows with air-conditioned buildings in that study. They considered air-conditioned buildings as a risk factor as opposed to naturally ventilated buildings, as has been supported by previous literature. 49
Another explanation for the positive associations of dry eyes and headaches with the absence of windows can be limited daylight access, in line with findings of the CHBS study. 29 They found that the risk for headaches increased, when the distance between workplace and façade window was larger than 5 m versus workplaces near the façade window. A possible cause is the influence of (higher) illuminance of artificial lighting needed at places without a window. Wilkins et al. 50 found that flickering of artificial lighting may increase the speed of small eye movements, that can cause eyestrain and headache. They studied the incidence of headaches and eyestrain with lighting tubes with a high fluctuation of the lighting frequency, versus tubes with a low fluctuation of the frequency. Although participants were not aware of the differences in the frequency, eye strain and headaches occurred less frequently (50%) when they had lighting with lower fluctuation. Also, those who had higher daylight access in their office were less likely to have headaches. A more recent study 51 suggested that the flickering frequencies of both fluorescent lighting tubes and LED may affect headaches, because the fluctuation of LEDs is higher than most fluorescent lamps. In the present study, 94% of the inspected rooms were lit by fluorescent lighting tubes, LED, or a combination of fluorescent lighting tubes with LED or medical lighting.
Also, as suggested by Aries et al. 52 the full spectrum of daylight, fluctuations in intensity and wavelength of daylight and view to the outside have a beneficial effect on health. For example, they indicated that a distant view, e.g., to the outside through a façade window, provides relaxation of eyestrain. However, further study is needed to better understand the negative association of dry eyes and headaches with a window, particularly with the presence of a window to the corridor.
The negative association of dry eyes and tendency of a negative association of headaches with single person rooms is partly in line with previous studies. In the present study, there was a difference between single person rooms and rooms for more than one person, while the risk for dry eyes did not increase for persons working with one to three others, as opposed to those working with more than three others in a room. Similarly, in the CHBS study 29 positive associations of headaches with offices for more than one person compared to single person offices were found. In the Boston Study 30 and Japan Office Study 32 no associations were found for dry eyes and the number of people in the offices. These studies found associations of non-specific symptoms (including headaches) and upper respiratory symptoms with the number of persons in the office. A possible explanation for the association of dry eyes with the presence of others is the exposure of organic pollutants emitted by other humans, as suggested by Wolkoff. 53 For example, an experimental study with 25 college students 54 indicated relations of exposure to human bio-effluents with physiological stress reactions. The students were exposed to different levels of CO2 and CO2 generated by human subjects (from 500 to 3000 ppm). Stress reactions, such as increased heart rate and blood pressure, occurred when the concentration of metabolically generated CO2 increased. The incidence of acute symptoms, such as headaches increased only with an increased concentration of metabolically CO2, as opposed to CO2 without bio-effluents. 55
In this study, those who worked most frequently in offices were more likely to have dry eyes and headaches, than those who worked most frequently in consultation rooms. This partly confirms the comparison of main symptoms in different room types at the outpatient area in a previous study with the same dataset, 21 where building-related aspects were not included in the analysis. Dry eyes were associated with offices, for headaches there was a tendency of a negative association. The outpatient workers who worked most frequently in offices were also more likely to be dissatisfied with the indoor air quality and they were more likely to perceive dry and stuffy air, than those who worked most frequently in consultation rooms. The dissatisfaction with indoor air aspects might have contributed to differences associated with room types. However, as indicated by Brauer et al. 56 the association of symptoms and indoor air quality can be two-directional. Possibly, the perception of dry eyes and headaches might have contributed to dissatisfaction with indoor air quality aspects.
Also, occupational aspects might have contributed to the differences between those who work more frequently in offices and in consultation rooms. For example, variation in sedentary behaviour and intensive use of a visual display unit (VDU) may increase the risk for dry eyes. 37 More than 25 h of VDU use per week was positively associated with dry eyes in OFFICAIR. 33 In a study with 425 office workers in Osaka, those with a low tear film stability were generally sitting a larger number of minutes per day, than those with a normal tear film stability. 57 Hours of VDU use and sedentary behaviour were not included in the present study. Further research is needed to better understand why those who work more frequently in offices were more likely to have dry eyes or headaches in comparison to those working more frequently in consultation rooms.
Surprisingly, variables related to outdoor air pollution did not remain in the multivariate models of dry eyes and headaches. For example, in the OFFICAIR study, 33 associations of dry eyes with the proximity of potential sources of outdoor pollution were found. Mendell et al. 31 found associations of headaches and dry eyes with the height of outdoor air intake; grills lower to the ground level were a risk factor for dry eyes and headaches. Also, in the cross-sectional study of Smedbold et al. 24 on environmental parameters in relation to measurements of the tear film stability of 176 inpatient workers in geriatric hospitals, associations with nearby heavy traffic and increasing tear-film instability were found. Jung et al. 58 concluded in a literature study that air pollutants, such as NO2, particulate matters and dioxin influence the condition of the ocular surface. Variables, such as the presence of a nearby highway or industry, related to the exposure to outdoor air pollutants in the present study were not included in the final multivariate models, due to the presence of nearby traffic and parking places at all locations.
Strengths and limitations
This study included a broad range of building-related aspects at different scale levels, from organization, location, building wing, to room. One limitation can be the limited number of building locations, where the respondents worked. This may have affected the variance in building-related aspects. However, because buildings on locations were complex, due to differences between room types, between rooms with or without a window to the facade, or different renovation periods, building-related aspects varied within buildings. Some building-related aspects had an (almost) equal distribution. For example, highway and industry nearby, the presence of an attached parking garage and the cleaning protocol of the ventilation grilles for air supply and exhaust in the rooms, were equally distributed. Also, the presence of a forest nearby and cleaning frequency of the filters of the AHU’s were equally distributed. The most plausible risk factors, with a logical direction of the association, were selected for inclusion in the multivariate model. Also, the specific rooms of which the outpatient staff reported their comfort were not identified, due to privacy and practical reasons. Therefore, discrepancies between building aspects of the inspection and the exact location of the outpatient workers might have occurred. This was accounted for in the study design, as the building inspection was performed systematically, and building-related aspects were included when variation was consistent within a building wing, room type and adjacency to the façade.
Another limitation of this study can be the unequal distribution of gender. The large proportion of female workers is representative for hospitals. Some previous studies in hospitals excluded male workers from the study,24,59 but this study intended to provide a representative overview of the outpatient workers. Therefore, the logistic regression calculations were adjusted for gender. Also, the type of hospitals can be a bias. Only top clinical (teaching) hospitals were invited for participation, to restrict the possible influence of organizational aspects. Therefore, caution is needed for generalization of the results to the entire Dutch outpatient staff.
The study was cross-sectional and can therefore only indicate associations of risks for dry eyes and headaches. The study design did not allow determining cause – effect relations. Also, indication of dry eyes and headaches was based on self-reported data. However, Burge et al. 60 compared the prevalence of self-reported building-related symptoms with building-related symptoms that were diagnosed through medical interviews. Self-reported dry eyes and headaches were among symptoms that correlated with the medical diagnosis.
Conclusions
The high prevalence of self-reported dry eyes and headaches in outpatient areas may be explained by building-related aspects, in particular aspects that affect the indoor air quality and visual quality, as well as the functionality of rooms (e.g., offices). An overlap was found of building-related aspects that were associated with both dry eyes and headaches.
This study in general showed overall consistency with previous studies in offices. Specific for this study was the association of dry eyes and headaches with room types. Results suggest that taking the specific room type into account is important in future studies. Also, the association of dry eyes and headaches with a window to the corridor, which was a specific finding in this study, needs further investigation. Because the symptoms were associated with building services, the building layout and work-related aspects, this study strengthens the importance of close collaboration of hospital organizations, engineers and architects during the design phase of outpatient areas. As the prevalence of building-related symptoms of hospital workers is generally high and may affect sick-leave and productivity, further studies can help hospital organizations to accommodate a supportive physical environment.
Supplemental Material
sj-pdf-1-ibe-10.1177_1420326X211023125 - Supplemental material for Building characteristics associated with self-reported dry eyes and headaches of outpatient workers in hospital buildings
Supplemental material, sj-pdf-1-ibe-10.1177_1420326X211023125 for Building characteristics associated with self-reported dry eyes and headaches of outpatient workers in hospital buildings by AnneMarie Eijkelenboom, Marco Ortiz and Philomena M. Bluyssen in Indoor and Built Environment
Footnotes
Acknowledgements
The authors would like to thank Dadi Zhang and Dong H Kim for assistance with the building inspection. They also thank the project leaders and all outpatient workers of the hospital organizations who participated in the study.
Authors' contribution
All authors conceived the presented idea. The first author carried out the statistical analysis, the second author checked the statistical analysis. The first and third authors wrote the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Daikin Nederland and EGM Architects as part of the PhD project ‘user experiences and preferences in health care centres’ at the Delft University of Technology under the chair of indoor environment at the Faculty of Architecture and the Built Environment.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.