
Abstract
Purpose
The International Commission on Illumination (CIE) recommends researchers to investigate a wide variety of behavioural and health outcomes. However, researchers often investigate only a part of occupational health (OH) in relation to light. A literature study (2002–2017) regarding the relationship between office lighting conditions and OH was performed to identify gaps and methodological issues.
Method
The OH outcomes investigated in this paper were grouped according to the International Classification of Diseases and analysed per category: physical and physiological health, mental health, eye health, sleep parameters and visual comfort.
Results
Findings from the literature study (20 eligible papers) showed that all OH aspects were mostly but not exclusively measured subjectively. Furthermore, most studies investigated only a fraction of office lighting parameters and OH aspects.
Conclusions
It seems that Correlated Colour Temperature (CCT) and illuminance mainly correlate with OH. However, this may also be explained by gaps and methodological issues in studies described in eligible papers. Based on the literature study, an overview was composed elucidating gaps and methodological issues of office lighting and OH studies. It can be used to design and target the purpose of light and health research.
Introduction
Light is essential for human health and well-being. Light does not only enable people to see and perceive their environment. it also induces non-image-forming (NIF) effects that subsequently trigger health effects. 1 NIF effects range from cell division and hormone production to changes in behaviour, none of them depending on image processing of the visual system. 2 All three photoreceptor types in the eye, rods, cones and (intrinsically) photosensitive retinal ganglion cells (ipRGc), can, when light has been captured, initiate these biochemical processes in the brain affecting human health.3,4
Light and health
Before the discovery of the ipRGc in 2002, NIF effects of light were called light effects.5,6 Currently, a growing number of researchers are investigating NIF effects of light and knowledge in this field is rapidly increasing. For example, Smolders et al.7,8 demonstrated the correlation between illuminance levels and alertness. They found that participants felt less tired, more vital and happier when exposed to bright light, even under usual conditions (i.e. neither sleep nor light deprived). However, they investigated NIF effects of light using photopic terms like illuminance to express potential relationships between lighting conditions and human health. Photopic terms are weighted to the spectral sensitivity of human cones. The ipRGc have different spectral sensitivities; therefore, photopic terms may not be relevant to express NIF effects. For example, the ipRGc are maximally sensitive in the short-wavelength light (480 nm) whereas these three types of cones (L-, M- and S-cones) and rods are maximally sensitive at respectively 420 nm, 535 nm, 565 nm and 507 nm. 4 Researchers are considering new terminology and methods on how to express and measure light that activates NIF effects, which subsequently influences human health.9,10 The International Commission on Illumination (CIE) suggests to refer to luminous radiation instead of light and they have defined a number of terms that can be used to describe effective radiometric quantities.11,12
Changes in workforce
Alongside with the advancement of scientific knowledge in the field of light and health, the workforce is changing itself. 13 Nowadays, the workforce is digitalizing, and office workers use computers, laptops and smartphones more often than before. In addition, in the last four decades, Western-European individual offices have been transformed into office landscapes. This transformation fits seamlessly in the new working principle introduced to stimulate flexibility at work. Especially for the design of office landscapes, ambient environmental factors such as office lighting and privacy issues are relevant aspects to elucidate the interaction between work and health. The aspect of office lighting is more complex in office landscapes compared to individual offices because an office landscape is shared with multiple employees with potential different preferences.
Satisfaction and occupational health
Although researchers have indicated a link between environmental satisfaction and job satisfaction,14,15 the ideal physical work environment for employees’ satisfaction and health remains unclear. Based on occupant satisfaction measures, Newsham et al. 16 provided recommendations for environmental aspects within the office environment to reduce the risk of dissatisfaction. However, office lighting is only one of the investigated important aspects mentioned in this study; satisfaction with office lighting was already shown to be important for OH in the 1990s. 17 The World Health Organisation (WHO) defines ‘occupational health’ (OH) as a combined term which includes all aspects of health and safety in the workplace, ranging from prevention of hazards to working conditions. 18
Light sources
Satisfaction with lighting conditions in offices is often divided into satisfaction with daylight or with electric light. In most offices, the employee's luminous exposure consists of a combination of electric light and daylight. Galasiu and Veitch 19 discussed several studies investigating subjective issues linked to daylight and their main conclusion was that the majority of the population believe daylight is good for their general health, visual capabilities and productivity. However, it seems that it is difficult for individuals to estimate the amount of daylight availability at their workplace.20,21 Light with shorter wavelengths could trigger the greatest ipRGc response 2 and since daylight is rich in this bluish part of the spectrum, this may explain why individuals prefer daylight during the day. In 2013, Aries et al. 22 presented an overview of all proven effects of daylight exposure on human health and reported rather limited scientific evidence of the association between daylight and its health consequences. They recommended further research to focus on the nature of why some individuals prefer daylight and others do not, how the dose–response curves for alertness, performance and mood should be interpreted, and the effect of daylight on human health in the general population. Moeller et al. 23 described a research plan for the investigation of differences in user experience and perception when exposed to different lighting situations. They also highlighted that until now, insufficient attention has been paid to potential OH effects in relation to lighting situations in the workplace.
Objective of this study
For this paper, a literature study was performed with the aim of identifying gaps and methodological issues regarding studies that have investigated the relationship between office light conditions and OH. This literature review would address the following research question: Do lighting conditions among office workers influence occupational health, and in what way?
Methodology used for literature review
The overview is based on articles that describe studies investigating the interaction between office light conditions and OH.
Eligibility criteria
All studies reviewed were performed in an office environment in order to be eligible for this review. All articles in the qualitative synthesis were published English articles. Of the 37 eligible articles, 17 were excluded because they were published before 2002. The considered years were from 2002 until 2017. 2002 was chosen since this was the year in which the functionality of the ipRGc was discovered. 3 Only articles published between January 2002 and August 2017 were collected. In total, 20 research papers were included in this qualitative synthesis.
Information sources
Four online scientific databases were used to execute a literature search (PubMed, ScienceDirect, Scopus and Web of Science). Databases PubMed and Scopus focus on human-related research, while ScienceDirect and Web of Science are broad and combine technical and health publications. On 24 August 2017, the last search was performed.
Search and study selection
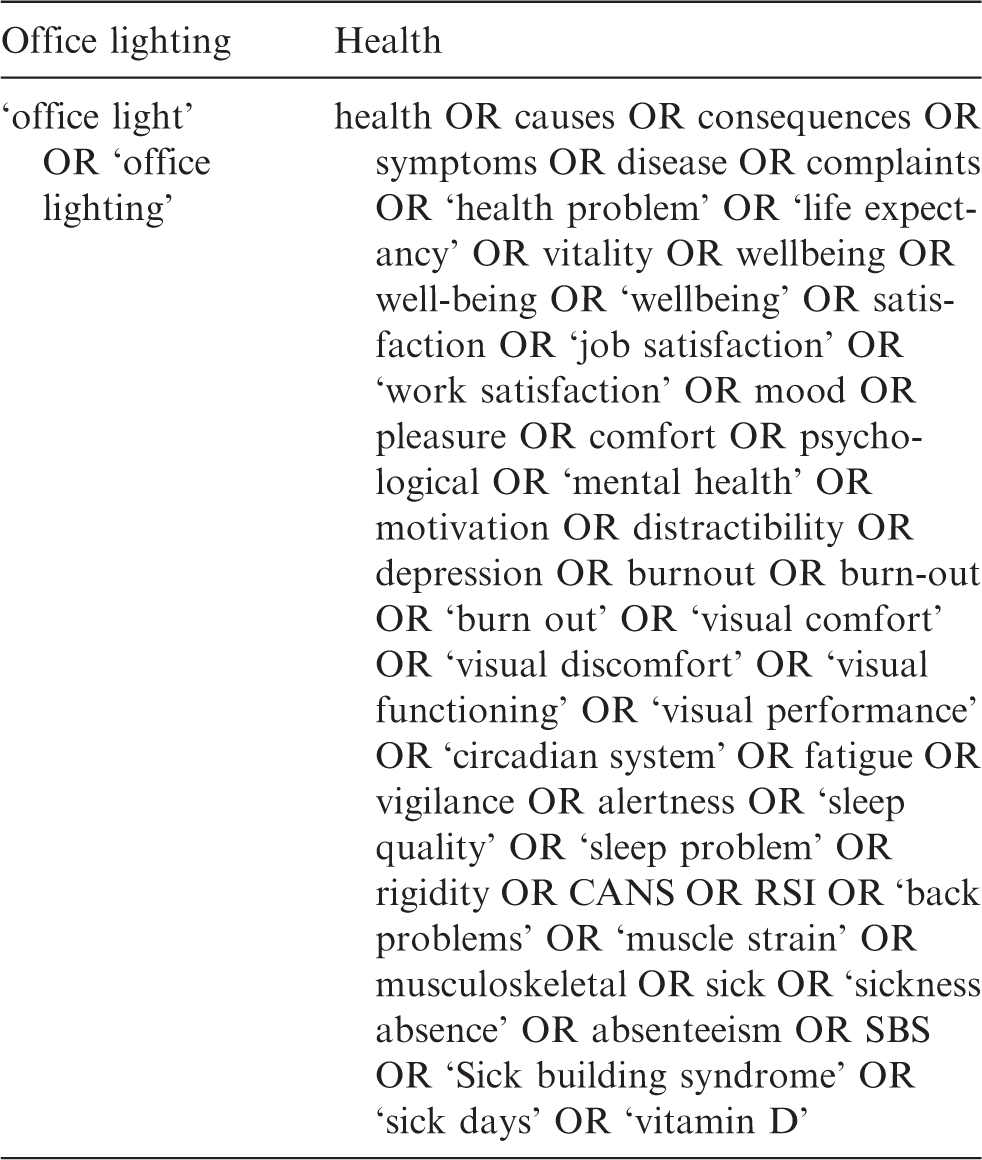
The base of the literature search was the word combination: ‘Office Lighting’ and ‘Health’. Both aspects had to be present in potentially eligible articles. The search terms – in full text – are provided in Table 1. The CIE recommends researchers to investigate a wide variety of behavioural and health outcomes that might reasonably be affected by light exposure.
24
Therefore, a wide interpretation of OH was employed, ranging from sleep quality to sickness absenteeism. The interpretation focuses on health whereas safety of employees is excluded in this study. The quotation marks were used to exclude studies regarding lighting in other buildings or regarding offices without focus on lighting. The search terms related to health aspects are based on
the definition of the WHO: Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity
25
; the separation of health into psychological, physiological and physical health; eye health issues
26
; and Applied search terms for the literature search in the four online databases: PubMed, ScienceDirect, Scopus and Web of Science. Quotation marks '.' indicates that two words should be combined in order to find results in the database.
The definition of health of the WHO has been criticized by multiple researchers. Huber et al. 29 suggested to change the emphasis from ‘complete’ to the ability to adapt or self-manage social, physical and emotional challenges.
The term ‘glare’ was not included in the search terms for this literature study. Glare is often restricted to visual comfort for people with healthy eyes. People with eye diseases might experience more glare; however, these papers were included in this literature study when searching on visual functioning. Articles investigated glare should include other search terms (e.g. visual comfort or visual functioning) to be relevant for our literature study.
Screening
The screening process is demonstrated via the flow diagram in Figure 1. To discard articles on office light conditions and OH with another focus than the intended, the filter TKA (Title-Keywords-Abstract) was applied on both the lighting- and the health-related search terms. By this, articles were excluded that investigated the workplace in general and that happen to just mention office lighting as one of the aspects which influences the health of employees. Among the 225 articles collected, there were 62 duplicates which were subsequently removed. Abstract analysis of the remaining 163 articles further reduced the number of articles characterized as eligible for the scope of this literature study to 37. Reasons for article exclusion were a focus other than health or the fact being a conference paper. Two of the excluded conference papers were literature reviews and therefore have been checked whether they needed to be excluded. In 2000 and 2013 these reviews were published regarding office lighting research.30,31 Since the review from 2000 is before the discovery of the functionality of the ipRGcs, it can be assumed that the knowledge regarding office lighting and OH has improved significantly. The review paper from 2013 presented office lighting studies from around and after the year 2000 and was related to a Scandinavian context. Kronqvist
31
concluded that there are a number of problematic issues resulting in difficulties comparing similar studies claiming to study the same phenomenon in office lighting. Both reviews were excluded from this study. Of the 37 eligible articles, 17 were excluded because they were published before 2002.
Flow diagram demonstrating the search methodology for the literature study. The boxes at the left side display the steps in the search process: identification, screening, eligibility and included. The ‘n values’ are the number of articles. TKA: Title-Keywords-Abstract.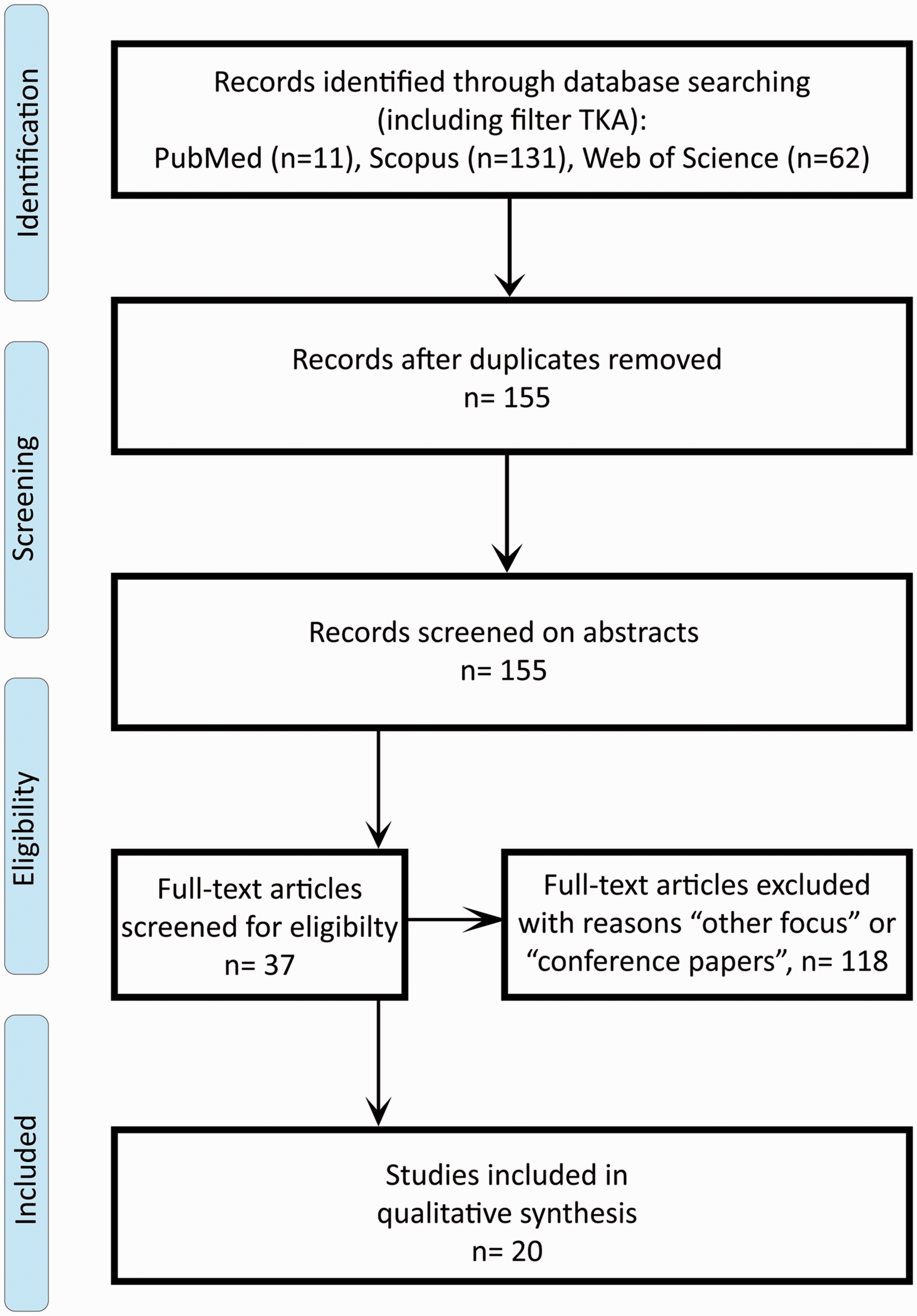
Data collection process
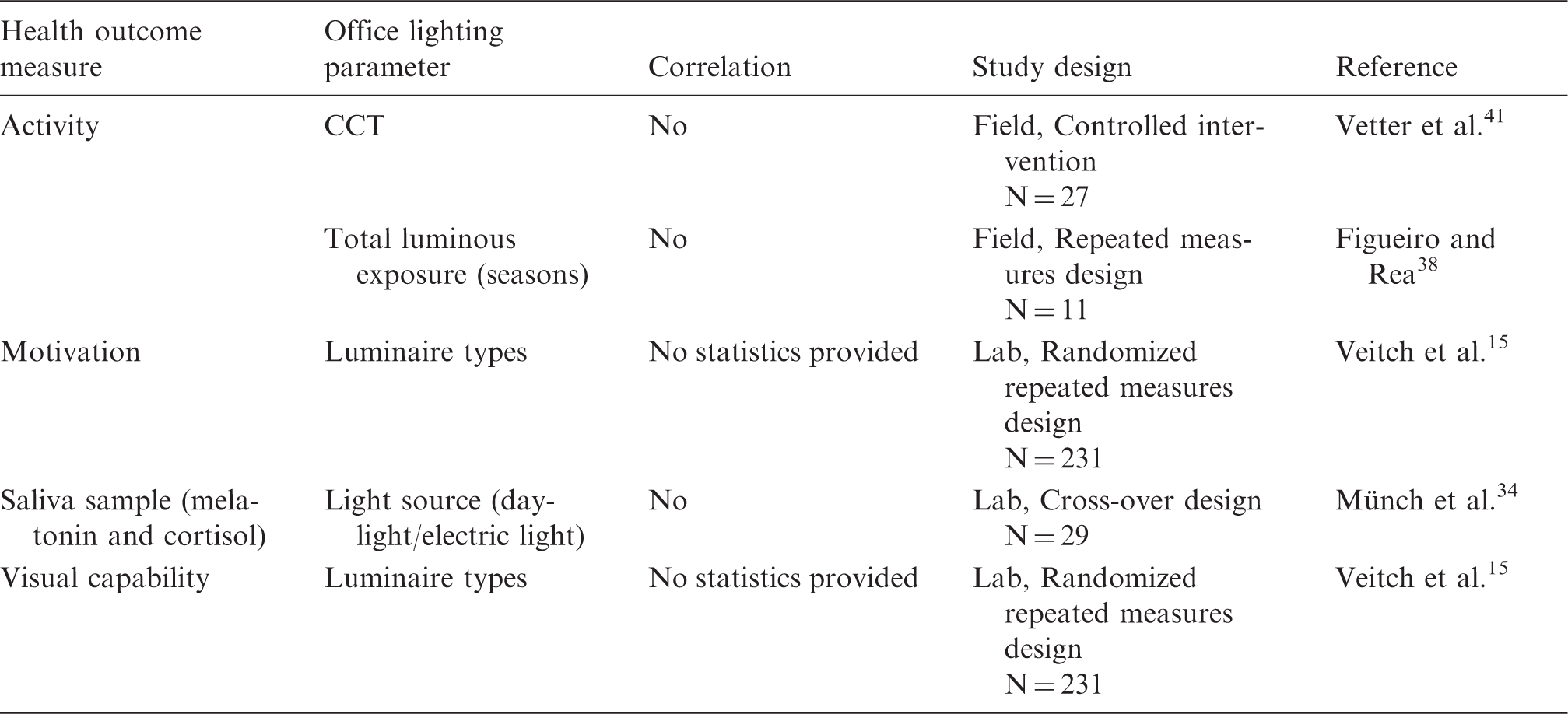
Overview of all investigated subjective and objective health outcome measures used in each article included in this research paper.
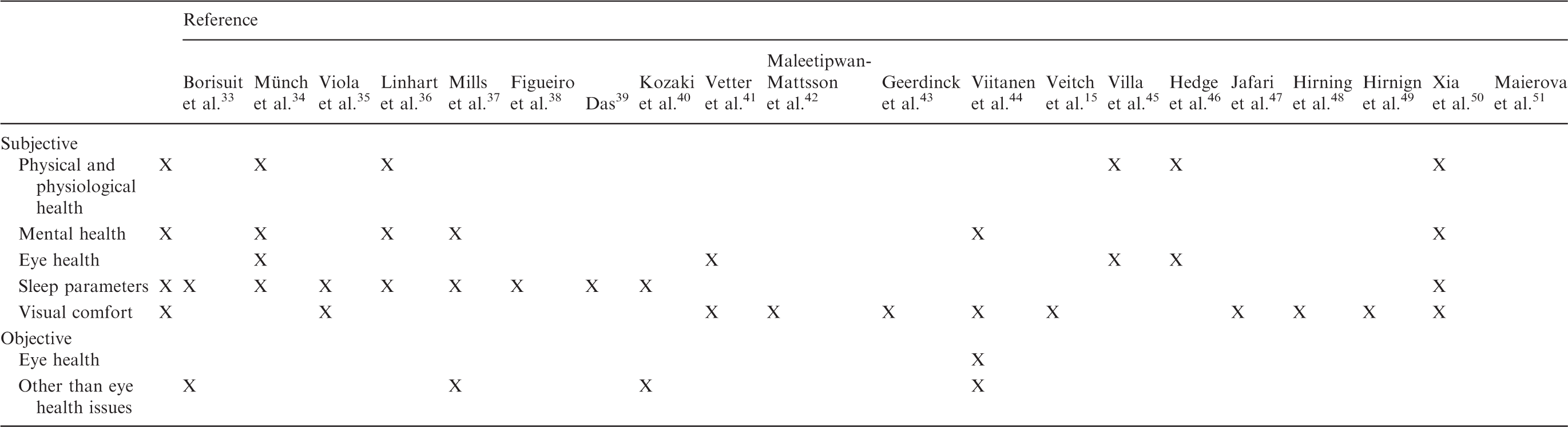
An X indicates that the health outcome was investigated; it does not give any indication on the strength or significance of the correlation between that health indicator and the office light conditions.
The category ‘visual comfort’ has been included because the definition of health uses the term ‘well-being’. 25 OH does not only prevent diseases in employees, but also provides a comfortable workspace. Visual comfort (i.e. the absence of visual discomfort 2 ) is a potential contributor towards a comfortable work environment.
Summary measures and synthesis of results
All included articles were analysed regarding their methods and results. All indicated significant correlations regarding the relationship office lighting and OH were reported in the results section. Studies investigating similar OH outcome measures were synthesized in separate sections and discussed in detail.
Results
All 20 included articles investigated the influence of lighting conditions on the six groups of OH outcomes: physical and physiological health, mental health, eye health, sleep parameters, visual comfort and objective health measures.
OH category ‘physical and physiological health’ and in included articles indicated correlations between this health outcome measure and office lighting parameters.
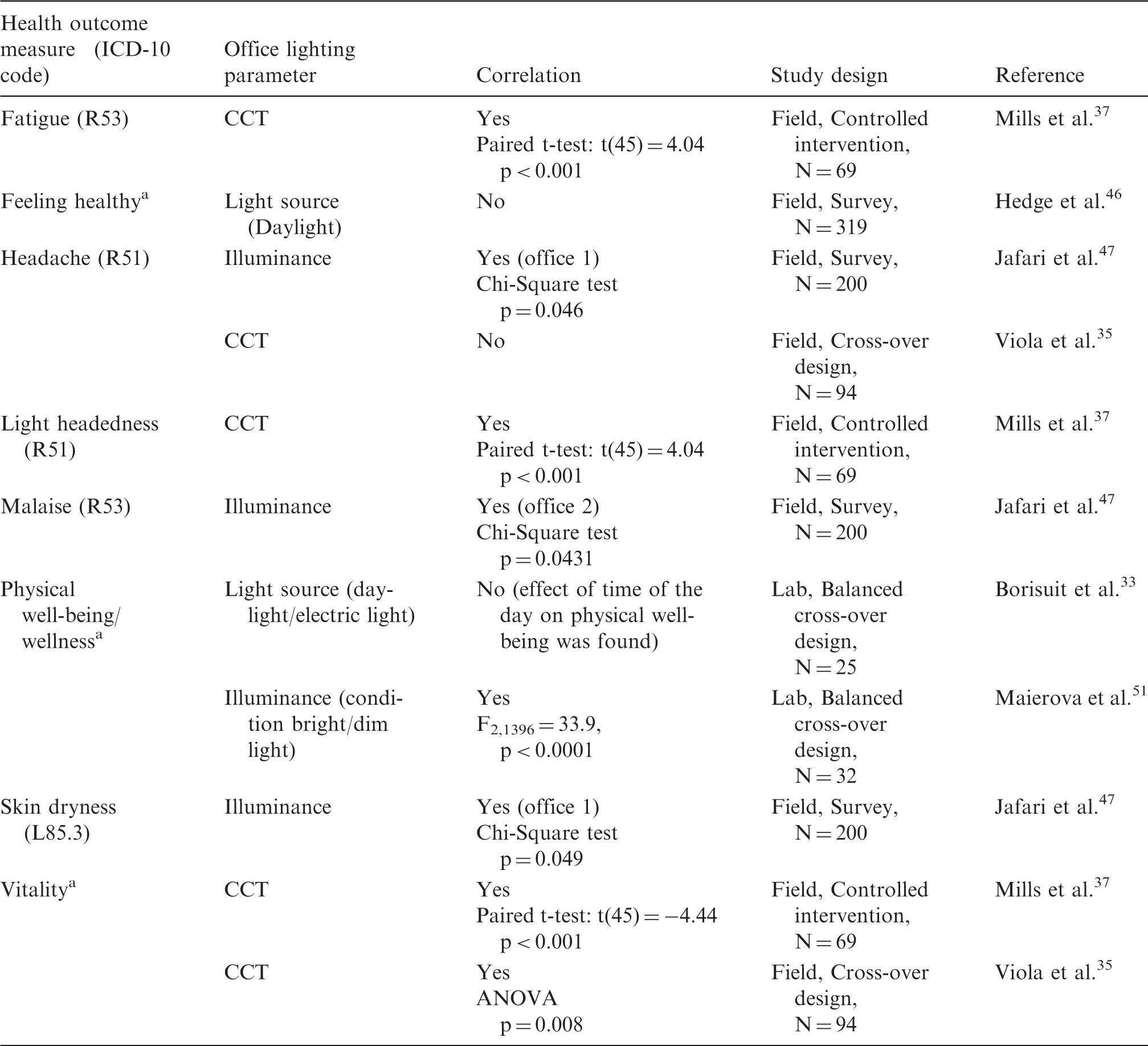
CCT: Correlated Colour Temperature; OH: occupational health.
No ICD-10 code was directly corresponding to the health outcome measure. All outcome measures presented as such in literature.
Physical and physiological health
‘Physical and physiological health’ was investigated in 6 of the 20 included articles reviewed in this paper. Eight different measures for physical and physiological health were used to investigate this health outcome (see Table 3 and Figure 2). Maierova et al.
51
reported that physical well-being was significantly higher in bright light (i.e. Ev = 1000 lx) compared to the dim light conditions (i.e. Ev < 5 lx). Borisuit et al.
33
found that after exposure to electric light for 1 h, participants felt significantly less well compared to the beginning of the study. They stated that this change in physical well-being was not found under daylight conditions. However, this effect was related to the time of the day and not specifically to condition daylight or electric light. Self-reported vitality could also be improved after an intervention of 17,000 K lighting.35,37 In addition, Mills et al.
37
showed an effect of bright light (17,000 K lighting) on fatigue and light headedness, measured by the Columbia Jet Lag Scale. Hedge et al.
46
found that under daylight conditions people felt healthier. This relation was based only on questionnaire results and thus the self-reported health cannot be related to actual (measured) lighting conditions. From their survey study results, Jafari et al.
47
showed a significant relationship between illuminance levels and skin dryness, headache and malaise. Viola et al.
35
reported no statistical correlation between their measured CCT values and headache. All indicated significant correlations between the OH aspect ‘physical and physiological health’ and lighting conditions were beneficial for human well-being.
Overview based on all ‘physical and physiological health’ conclusions. The heart shaped term is the occupational health-related aspect and the terms in the rectangles are the office lighting parameters. Arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.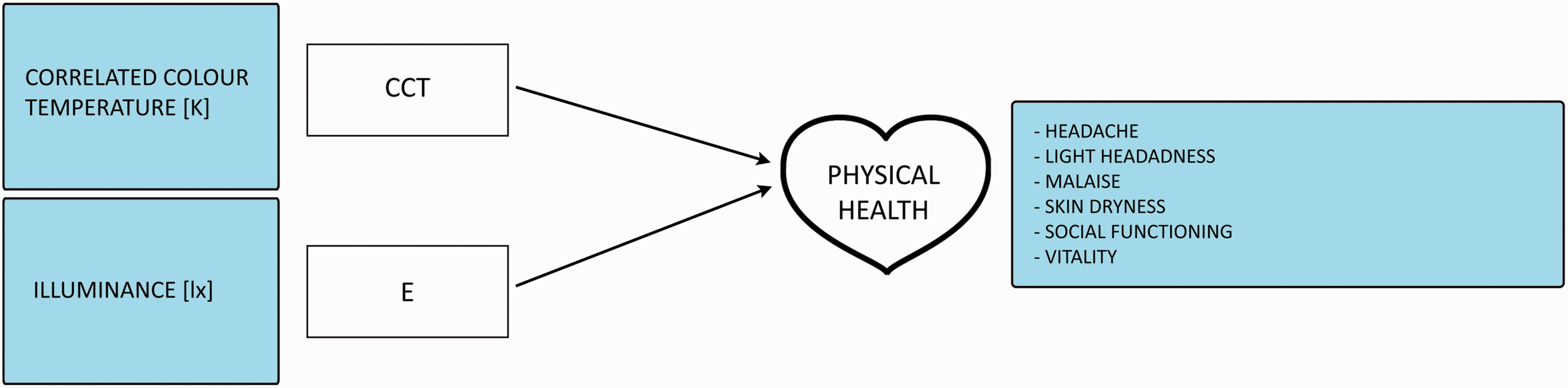
Mental health
OH category ‘mental health’ and in included articles indicated correlations between this health outcome measure and office lighting parameters.
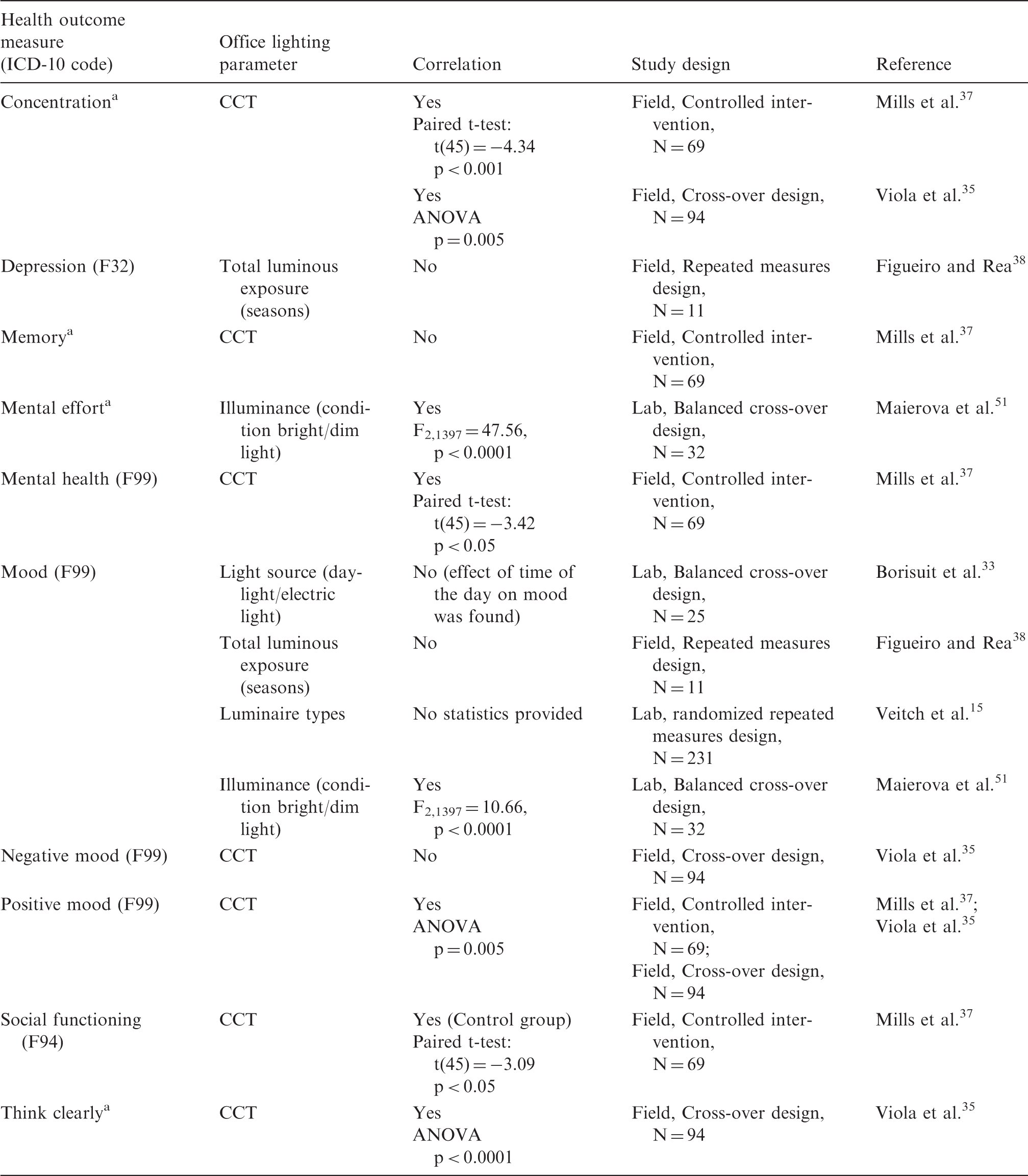
CCT: Correlated Colour Temperature; OH: occupational health.
No ICD-10 code was directly corresponding to the health outcome measure. All outcome measures presented as such in literature.
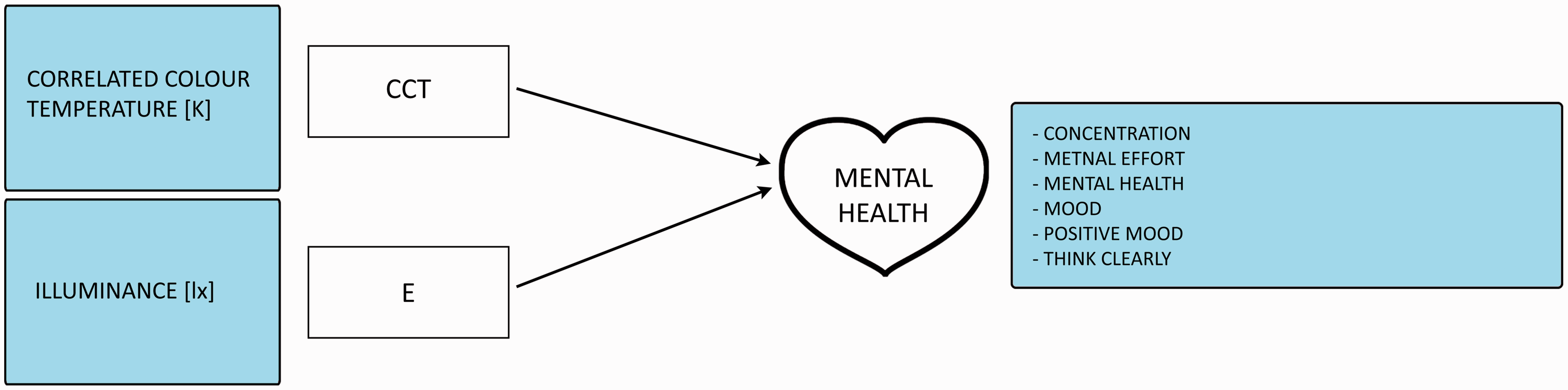
Overview based on all ‘mental health’ conclusions. The heart shaped term is the occupational health-related aspect and the terms in the rectangles are the office lighting parameters. Arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.
Eye health
OH category ‘eye health’ and in included articles indicated correlations between this health outcome measure and office lighting parameters.
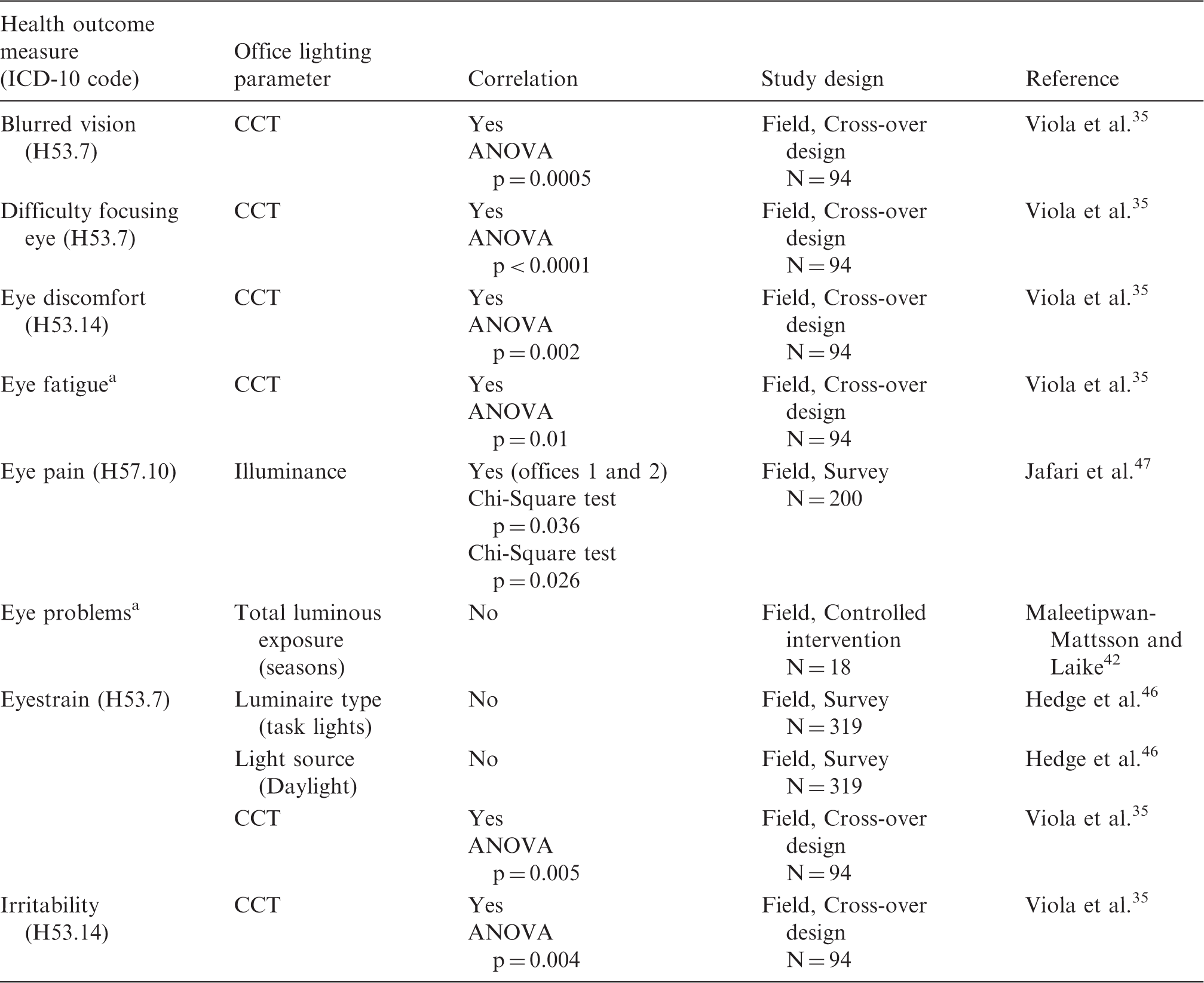
CCT: Correlated Colour Temperature; OH: occupational health.
No ICD-10 code was directly corresponding to the health outcome measure. All outcome measures presented as such in literature.
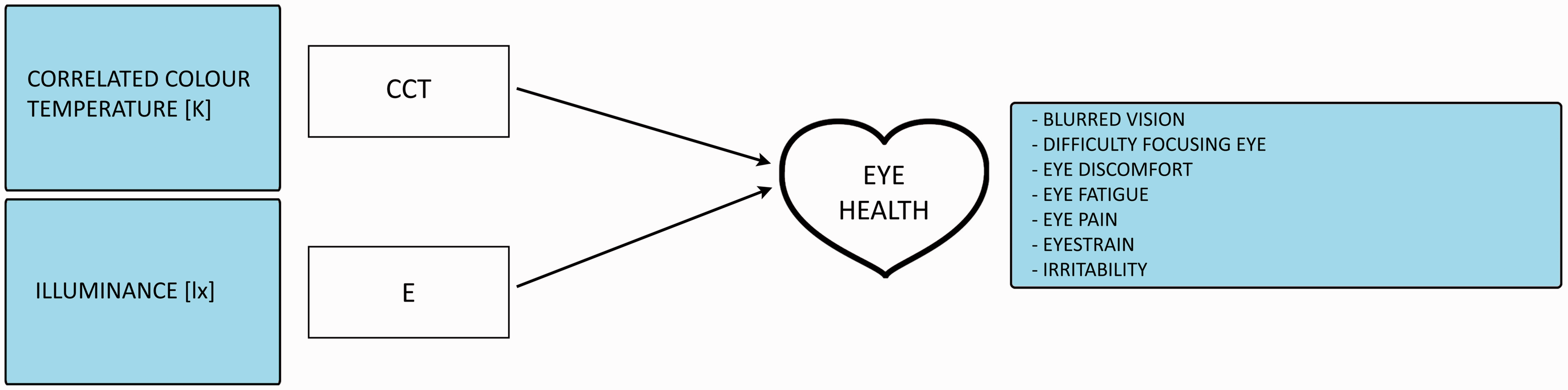
Overview based on all ‘eye health’ conclusions. The heart shaped term is the occupational health-related aspect and terms in rectangles are office lighting parameters. Arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.
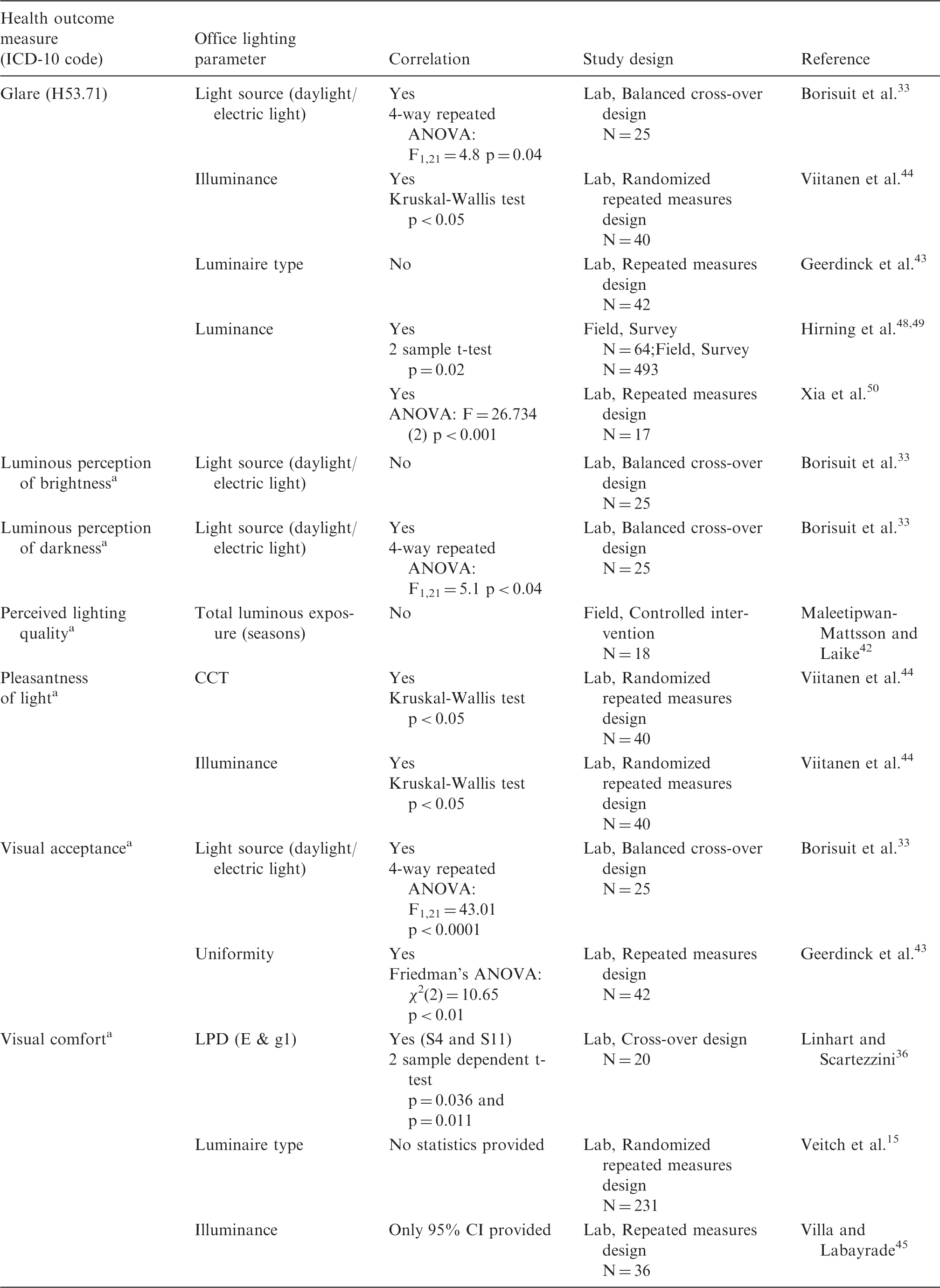
Sleep parameters
OH category ‘sleep parameters’ and in included articles indicated correlations between this health outcome measure and office lighting parameters.
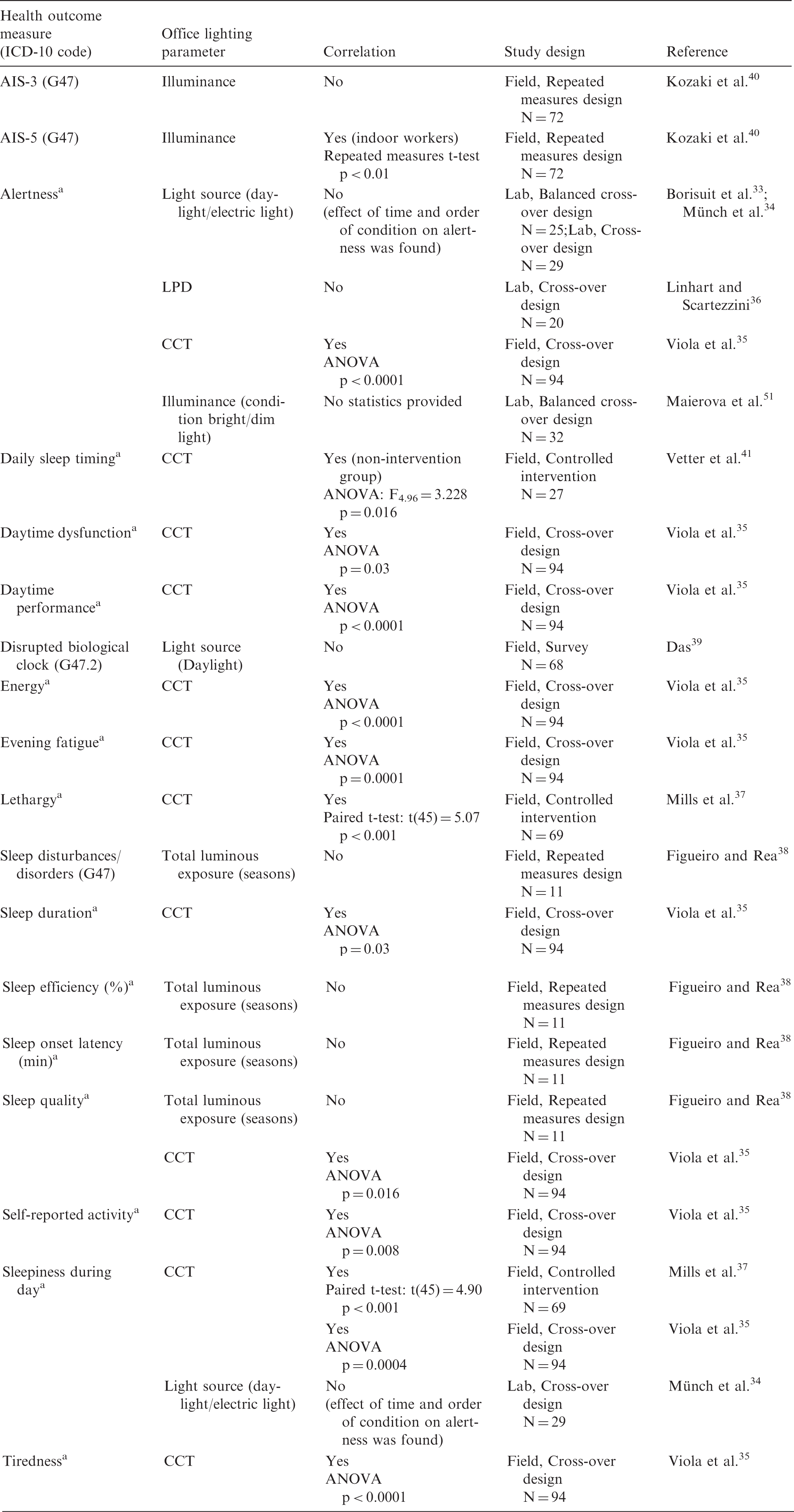
CCT: Correlated Colour Temperature; OH: occupational health; LPD: lighting power density.
No ICD-10 code was directly corresponding to the health outcome measure. All outcome measures presented as such in literature.
Health outcome measure ‘visual comfort’ and in included articles indicated correlations between this health outcome measure and office lighting parameters.
CCT: Correlated Colour Temperature; LPD: lighting power density.
No ICD-10 code was directly corresponding to the health outcome measure. All outcome measures presented as such in literature.
Overview based on all ‘Sleep parameters’ conclusions. The heart shaped term is the occupational health-related aspect and terms in rectangles are office lighting parameters. Arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.
Alertness and sleepiness
The article from Münch et al. 34 forms the study prior to the balanced cross-over study from Borisuit et al. 33 They both showed that alertness could be reduced over the course of the afternoon and that this decline in alertness came earlier after exposure to electric light compared to the daylight condition. They concluded that a higher illuminance, higher CCT and a lower CRI at 1 p.m. accounted for a higher subjective sleepiness at the same time. Borisuit et al. 33 discussed that this conclusion, based on an insignificant correlation, was in contrast to their hypotheses and previous literature and that the post-lunch-dip could be the cause leading to this conclusion. In another study, Viola et al. 35 showed that following exposure to an illuminant with a CCT of 17,000 K for four weeks, there was a significant increase in subjective alertness 35 (measured using the Karolinska Sleepiness Scale (KSS) 55 ). Differences in geographic location and time of the year could explain the divergent results of these studies. Borisuit's experiment 33 was executed in Switzerland (latitude: 46°N) between September and February while Viola's study took place in North-England (latitude: 52°N) between January and March. Borisuit et al. 33 and Viola et al. 35 both investigated alertness based on differences in daylight/electric light or CCT in their cross-over studies, while Linhart and Scartezzini 36 applied a different lighting power density (LPD) in a cross-over design. However, regarding subjective alertness, they did not find significant differences between the reference LPD of 4.5 W/m 2 (Ehor = 232 lx and g1 (illuminance uniformity) = 0.79) and the test scenario of 3.9 W/m 2 (Ehor = 352 lx and g1 = 0.90) in a Swiss experiment between April and May. Viola et al. 35 used questionnaires to measure alertness, as well as the term sleepiness during the day, energy, tiredness, self-reported activity level and evening fatigue and found for each term an improvement after exposure to 17,000 K lighting. 35 Mills et al. 37 used outcomes ‘sleepiness during the day’ and lethargy was derived from the Columbia Jet Lag Scale. 56 They also found an improvement for all outcome measures after a three-month exposure to 17,000 K lighting compared to the control situation of 2900 K. The improvement on sleepiness during the day after the intervention was more than 30%. Viola et al. 35 also reported improvements after 17,000 K luminous exposure on self-reported daytime dysfunction and daytime performance.
Sleep quality
Viola et al. 35 assessed alertness levels and daytime functioning, as well as measures ‘sleep duration’ and ‘sleep quality’. They demonstrated beneficial effects of 17,000 K lighting on duration and quality of sleep, both measured as a global and component Pittsburgh Sleep Quality Index (PSQI) score. 57 In the US, Figueiro and Rea 38 conducted a repeated measures study to investigate the influence of different seasons on sleep parameters using the PSQI and the Patient Reported Outcomes Measurement Information System (PROMIS) questionnaires.38,58 They concluded that their participants reported poorer sleep quality in winter compared to summer. In addition, they found more sleep disturbances in winter. However, correlations between Circadian Stimulus (CS) values and self-reports of sleep disturbances or sleep quality were not significant. Figueiro and Rea 38 found significant differences in sleep efficiency and sleep onset latency between two seasons. These differences, however, are differences in sleep parameters between two seasons and are not directly related to the total luminous exposures in these seasons. These differences between luminous exposures in winter and summer can be explained by daylight hours, illuminance levels and the spectrum of light. Das 39 argued that IT-professionals have a self-reported lack of sleep due to a lack of daylight exposure. This implies a possible correlation between daylight and human biological clock; however, in this study, light measurements were not analysed in combination with the questionnaire responses. Vetter et al. 41 investigated the sleep-wake rhythm as part of the biological clock as well. They found that the MSW (Mid-Sleep on Workdays) did not change in either the control (4000 K) or the intervention group (8000 K). However, they found that the MSF (Mid-Sleep on Free days) became significantly earlier, but only in the control group. The participant's sleep-wake rhythm was measured by filling in daily sleep logs. The last study which investigated sleep parameters is the repeated measures study from Kozaki et al. 40 They studied the influence of horizontal illuminance levels at desk height during an occupant's sleep. The main conclusions from their study were that a decreased illuminance level might induce insomnia for indoor office workers (based on the sleep difficulties outcome measure AIS-5 from the Athens Insomnia Scale 59 ). However, they did not find any impact of reduced illumination on well-being, functioning and sleepiness during the day (AIS-3).
Visual comfort
Visual comfort was investigated in 11 of the 20 articles included in this review. Seven different measures for visual comfort were used to investigate this health outcome (see Table 7 and Figure 6). Maleetipwan-Mattsson and Laike
42
presented that ‘hedonic tone’ and ‘brightness’ were perceived slightly higher in spring-summer compared to autumn-winter. However, this correlation was not found to be statistically significant. Borisuit et al.
33
investigated the perception of brightness and darkness and visual acceptance on VAS scales. They found that a higher perceived brightness was explained by a lower CCT (not significant correlation) and that a higher perception of darkness correlates significantly to a lower illuminance level. In addition, the participant's visual acceptance (average rating of ‘I like the light in this room’ and ‘Overall, the light in this room is comfortable’) overall was better for daylight than for electric light and that a lower visual acceptance correlates with higher vertical illuminances, higher CCT values and lower CRI values. In a repeated measures design using rating scales, Geerdinck et al.
43
investigated the visual acceptance of different lighting settings under laboratory conditions. They reported that the visual acceptance of small spots (lower uniformity) was significantly lower compared to homogenous settings. Viitanen et al.
44
performed a randomized repeated measures study investigating preferences about lighting. They found that the illuminance levels 600 and 1000 lx were equally pleasant, while there were significant differences between 300 lx and 600 lx and between 300 lx and 1000 lx. In addition, the CCT of 6000 K was significantly less pleasant than 3000 K. Linhart and Scartezzini
36
found that the difference in LPD resulted in significant differences in visual comfort. They measured visual comfort using the Office Lighting Survey (OLS) by Eklund and Boyce.
60
The significant differences were found for questions ‘This office seems too dim’ and ‘The ceiling-mounted luminaires are too bright’. At the end of the experiment, more people preferred the test scenario (LPD = 3.9 W/m2) over the reference scenario (LPD = 4.5 W/m2). Villa and Labayrade
45
investigated visual comfort using 16 different lighting situations (consisting of different dimming levels for the ceiling lighting and the desk light). Results from a paired-comparison test indicated that the most suitable situation should have: a ceiling luminous flux higher than 66% and a switched-on desk light. For the first group of participants, rating the different lighting conditions resulted in the conclusion that the luminous environment is the cosiest when the ceiling lighting is switched off or presents a low-level and the desk light is switched on. Conversely, the second group of participants indicated that the situation in which the ceiling luminous flux is higher than 66% was the most comfortable situation. In this article, the p-values of correlations were not reported, only 95% confidence intervals were provided to compare different situations. In another study, Veitch et al.
15
investigated visual comfort based on different lighting systems in their repeated measures design. Direct-indirect luminaires were found comfortable for 80% of participants, while direct-only luminaires were found comfortable for only 70%. They did not provide statistics on their results in their research paper. Finally, Maierova et al.
51
reported that visual comfort was evaluated as being highest in the self-selected lighting condition compared to constant dim or bright light.
Overview based on all ‘Visual comfort’ conclusions. The heart shaped term is the occupational health-related aspect and terms in rectangles are office lighting parameters. Arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.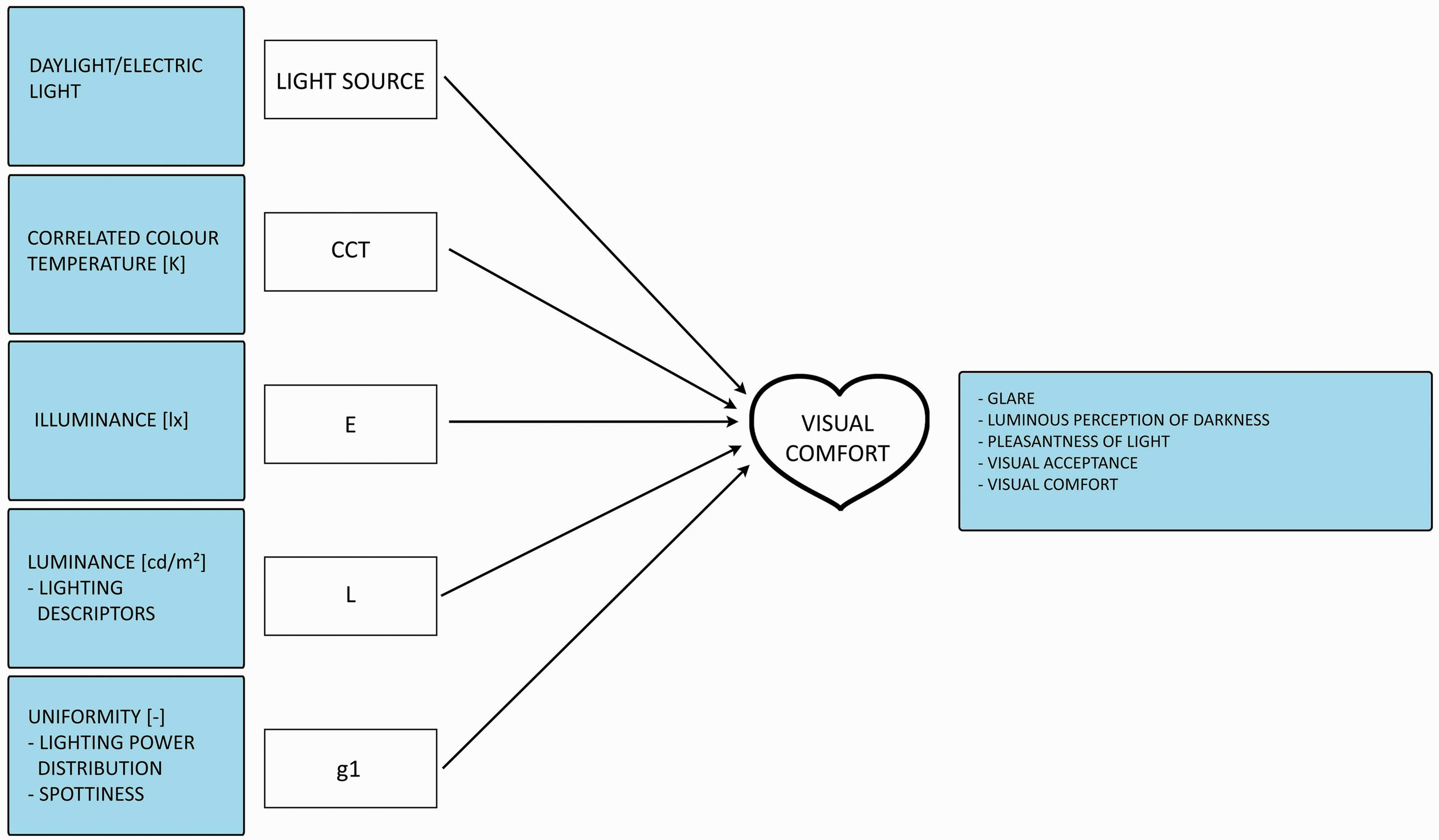
Glare
In addition to the previously mentioned visual comfort measures, humans may experience glare as visual discomfort as well. Borisuit et al. 33 found that subjective glare was rated significantly higher under electric light conditions compared to daylight. Viitanen et al. 44 found that a higher illuminance level led to a higher experienced glare. Geerdinck et al. 43 found, based on acceptance scores, that luminaires with non-uniform luminance patterns provoke more discomfort glare than uniform light sources in office landscapes. Xia et al. 50 agreed with Geerdinck et al. 43 and highlighted, based on their repeated measures design, that the luminance level of the exit window of the LED luminaire has a significant effect on perceived overhead glare. Hirning et al. 48 investigated discomfort glare in a field study. They collected High Dynamic Range (HDR) images and distributed questionnaires. From responses of 64 participants, 36 reported discomfort glare and 28 reported comfortable lighting conditions. Eighteen out of 20 participants who felt their workplace was glary also reported discomfort glare at the time of the survey. In the extended study from Hirning et al., 49 there was a significant relationship between the mean luminance calculated from the HDR images and participant's experienced discomfort glare. In a larger study from Hirning et al., 49 the averaged field of view (FOV) luminance was significantly higher for discomfort occupants. The average vertical illuminances at eye level were on average 502 lx for discomfort and 389 lx for comfort occupants. In addition, it seemed that the three general lighting descriptors (lighting, exterior view and period of time working under these conditions) appear to strongly correlate with discomfort about lighting.
Objective health measures
Objective health outcome measures and the in the included articles indicated correlations between these objective health outcome measures and office lighting parameters.
CCT: Correlated Colour Temperature.
None of the indicated correlations were statistically significant.
All indicated correlations in the included articles were not significant. The article from Veitch et al. 15 did not provide information about the statistical analysis.
Lighting conditions and OH
The literature study demonstrated indicated correlations (see Tables 3 to 7) regarding the relationship between office lighting conditions and OH categories. All results are summarized in this section. The italic definitions are definitions described as such in the corresponding literature.
Physical and physiological health
Light source (daylight/electric light) does not influence feeling healthy nor physical well-being; Correlated colour temperature influences fatigue, light headedness and vitality, but it does not influence headache; Illuminance influences headache, malaise, physical well-being and skin dryness; The influence of luminance on physical and physiological health was not investigated in included articles; The influence of uniformity on physical and physiological health was not investigated in included articles.
Mental health
Light source (daylight/electric light) does not influence mood. Correlated colour temperature influences concentration, mental health, positive mood, social functioning and thinking clearly. It does not influence negative mood and memory. Illuminance influences mental effort and mood. The influence of luminance on mental health was not investigated in included articles. The influence of uniformity on mental health was not investigated in included articles.
Eye health
Light source (daylight/electric light) does not influence eyestrain. Correlated colour temperature influences blurred vision, difficulty focusing, eye discomfort, eye fatigue, eyestrain and irritability. Illuminance influences eye pain. The influence of luminance on eye health was not investigated in included articles. The influence of uniformity on eye health was not investigated in included articles.
Sleep parameters
Light source (daylight/electric light) does not influence alertness, a disrupted biological clock nor sleepiness during the day. Correlated colour temperature influences alertness, daily sleep timing, daytime dysfunction, daytime performance, energy, evening fatigue, lethargy, sleep duration, sleep quality, self-reported activity, sleepiness during the day and tiredness. Illuminance influences AIS-5. It does not influence AIS-3. Statistics were missing to show significance for the relationship between illuminance and alertness. The influence of luminance on sleep parameters was not investigated in included articles. The influence of uniformity on sleep parameters was not investigated in included articles.
Visual comfort
Light source (daylight/electric light) influences glare, luminous perception of darkness and visual acceptance. It does not influence the luminous perception of brightness. Correlated colour temperature influences the pleasantness of light. Illuminance influences glare, the pleasantness of light. Statistics were missing to show significance for the relationship between illuminance and visual comfort. Luminance influences glare; Uniformity influences visual acceptance and visual comfort.
Based on findings from the literature study, an overview was derived to place lighting conditions in relation to OH, see Figure 7. The overview consists of two types of symbols: (1) the health indicators displayed in hearts and (2) the office lighting parameters displayed in rectangles. Each arrow stands for a significant correlation (p < 0.05) found in literature. Effects of combinations of light parameters were not investigated in articles included in the literature review; therefore, these potential relations are not demonstrated in the overview.
Overview based on all conclusions drawn in the results sections. All conclusions are based on the accompanying literature study. The heart shaped terms are occupational health-related aspects and terms in rectangles are office lighting parameters. All arrows indicate expected interactions. The outer boxes provide additional information corresponding to the lighting or health term. CCT: Correlated Colour Temperature.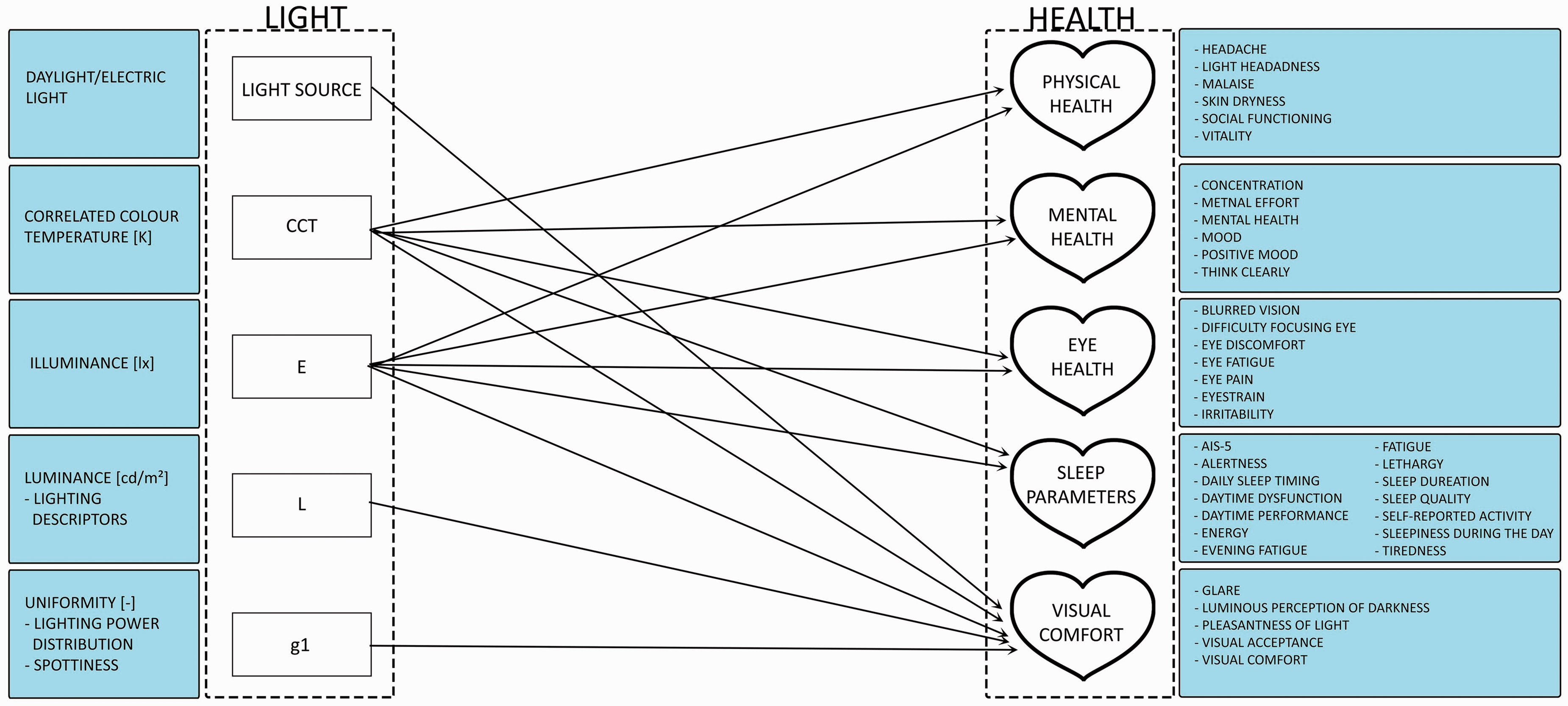
Discussion
This paper reviews literature studies that have investigated the relationship between office lighting conditions and OH. Based on this thorough literature study, a graphical overview has been composed. The lighting parameters included in the overview are: type of light source, CCT, illuminance, luminance and uniformity. We need to understand why these lighting parameters appeared under literature search using ‘office lighting’ as the lighting search term. Previous research has, for example, shown effects of light flicker on human health.61,62 Nevertheless, lighting parameters such as the spectrum of light, luminance distribution or flicker did not appear in our literature search.
The health indicators are divided into physical and physiological health, mental health, eye health, sleep parameters and visual comfort. Only subjective OH outcomes are included in this overview.
Occupational health
The absenteeism causes in the Netherlands are roughly divided into three pillars: psychological, physical and ‘unknown’. 63 The ‘unknown’ group consists of sickness reports from employees who did not see the occupational physician; thus, the reason for their sick leaves could not be categorized. All our literature studies included in this review, there were only six articles33,35,37,46,47,51 discussed and investigated physical or physiological health issues and six articles investigated on mental health15,33,35,37,38,51 aspects when reviewing the influence of office light conditions on OH. The fact that there were 11 articles related to visual comfort15,33,36,42–45,48–51 and 10 articles related to sleep parameters33–51 indicates the focus of current office lighting research. This also highlights that sleep disorders and visual comfort are assumed to be important for OH.
In addition to subjective methods to measure OH outcomes, several objective measures were used in the included articles. The search term: objective health measures (e.g. saliva samples 34 ) did not lead to significant correlations in the corresponding studies.
Gaps
The results from the literature review show a focus in the included articles on lighting parameters illuminance and CCT. This immediately show the gap of research investigating the lighting parameters light source, luminance and uniformity. Besides lighting parameters used in included articles, there are more aspects which are not even included in this review (e.g. spectrum of light, luminance distribution, directionality of light, or flicker). In addition to that, not every aspect within an OH category (i.e. physical and physiological health, mental health, eye health, sleep parameters and visual comfort) was investigated in relation to every office lighting parameter.
One example of a gap is the investigation of the relationship between luminance and eye health. Luminance has been shown to have an influence on glare which has been assumed to have an influence on eye health (e.g. too much glare might deteriorate eye health 1 ). However, the link between luminance and eye health was not directly investigated. This is just one example of a gap in the state-of-the-art of light and health research. Figure 7 provides the complete overview and demonstrates the relationships between lighting conditions and OH, and thereby, the missing links as well.
(In)Consistencies
Although several studies reported correlations in the same direction or between same variables, these studies cannot always be compared due to differing methodologies. For example, Mills et al. 37 and Viola et al. 35 both investigated health aspects based on changes in CCT in a field study. The study of Mills et al. 37 compared illuminants with CCT of 2900 K and 17,000 K while Viola et al. 35 used illuminants of 4000 K and 17,000 K. Although both studies found a beneficial effect on OH with the higher CCT compared to the lower CCT, these results cannot be completely compared due to differences in CCT values.
Two studies reported correlations between (the lack of) daylight and health aspects. Das 39 reported inadequate daylight exposure to be a potential cause for several health issues. However, these specific health issues linked to this inadequate daylight exposure were not reported. Headache and eyestrain are examples of health issues that were measured in the study. The conclusion given by Das 39 was unclear whether this was based on objective light measurements or on subjective questions regarding office lighting. In contrast, Hedge et al. 46 did not perform objective light measurements in their study and found no significant correlation between satisfaction with daylight and headaches or eyestrain. Therefore, it is possible that Das' conclusion 39 was based on the objective light measurements. Another possible explanation of this contradiction is the difference in geographic locations. The conclusion on inadequate daylight exposure as a potential cause for ailments in offices, drawn by Das, 39 may be related to their local climate in India. Another explanation of these differences in outcomes between studies from Das 39 and Jafari et al. 47 and Hedge et al. 46 could be related to the economic situations in their surveyed countries. It is possible that, due to the economy and subsequently the money invested in lighting systems, lower quality of lighting systems in studies given by Das and Jafari et al. could be used. In that case, correlations between the office lighting and occupational ailments may have been easier to detect.
In all types of experiments (field and lab studies), daylight availability has been shown as important for employees. Based on objective light measurements, Das reported a variation of lighting level between bright and dark outdoor conditions of less than 20% in all cases. 39 This meant that daylight penetration is marginal and at the same time, from subjective measurements, occupants were appeared to become deprived of their view and natural light. Figueiro and Rea 38 demonstrated differences in sleep problems of office workers between summer and winter seasons. The applied portable measurement devices in their studies recorded higher exposures to CS after work in summer, which is consistent with the longer daylight availability in summer compared to winter. Borisuit et al. 33 and Münch et al. 34 mentioned the importance of daylight availability for occupant's work satisfaction and alertness during the day. This unanimous agreement in the importance of daylight is in accordance to Galasiu and Veitch 19 as well as Aries et al. 22
Differences in lighting conditions or contrasts between laboratory and field studies may cause inconsistencies. However, those were only a few examples. In addition, differences in participant's user characteristics (e.g. age, gender, job type, working hours) may also influence research outcomes.
Methodological issues
An interesting difference among investigated studies is the level of detail in the health measures. Sleep parameters were often analysed comprehensively, while headache or ailment symptoms were investigated using one general question regarding their frequencies. Health aspects are shown to be measured subjectively and/or objectively. In contrast, lighting aspects can only be precisely measured with objective assessments. Although it is possible to estimate lighting conditions with subjective measures, only objective assessments can provide a precise measurement of lighting aspects. Only one study included in this review did not use an objective measure of lighting conditions. Only 9 out of 18 articles included descriptions of which measurement equipment was used to measure lighting conditions. Two studies used portable measurement devices.33,38 They measured the luminous exposure per person and close to the eye. Both aspects (measuring person-bound and close to the eye) lead to a more accurate measurement of individual luminous exposure and conclusions drawn based on effects of office lighting on OH will be more correct. Van Duijnhoven et al. 64 and Aarts et al. 65 demonstrated the importance of measuring individual luminous exposure by using portable measurement devices and they provided recommendations for selecting the most appropriate measurement device.
Besides describing the measurement methodology, it is of high importance to be precise about what aspect of the lighting condition that was measured66,67. Jafari et al., 47 for example, mentioned that poor office lighting was the leading cause for malaise in offices. Unfortunately, the term poor lighting is not defined and may be related to quality or quantity of the office light conditions or both. In addition, this literature review describes five studies mentioning the term bright light. This term is, in these papers, related to illuminance levels, correlated temperatures, or a combination of both. It is highly essential to define terms being applied in a research paper for other researchers to understand the work. A third issue in describing lighting conditions is to be as specific as possible while describing the lighting parameters. Three articles described lighting conditions as illuminance levels; however, it was not specified whether this value was the horizontal or vertical illuminance. Vertical illuminances are often measured to investigate health aspects, whereas horizontal illuminances are measured to determine both visual comfort and health aspects. This is in accordance with Vetter et al. 41 They reported that vertical levels are supposed to be relevant for biological effects, while horizontal data is important for good vision.
Although describing and measuring lighting conditions may be challenging in the health research field, the same applies for lighting experts; for them it is challenging to describe and measure health aspects. From included articles reviewed, there were only a few cases in which the group of authors included experts with knowledge in health and lighting aspects. The majority of authors of papers given in this review have a background in lighting but not really in health. The fact that either the lighting condition or the health condition were not described entirely in detail, suggests that the field of light and health research is multidisciplinary. It is important, therefore, to share knowledge and to collaborate with experts from other fields when performing light and health research.
Workplace development
Alongside with the advancement of scientific knowledge in the field of light and health (e.g. the discovery of the ipRGc), the workforce is also changing itself. Approximately 30 years ago, Konz and Yearout 68 recommended that the lighting exposure should be different in Visual Display Unit (VDU) offices compared to offices in which paper-based work is performed. At that time, approximately 25% of the workforce was using computers. They stated that office tasks were changing and that the need for specific types of lighting became more complex. In addition, they discussed that office lighting could affect the ability to perform visual tasks, the visual comfort and the aesthetics of an office space. Presently, the office tasks are continuing to change: in 2013, 26% of all employees in the Netherlands were working on a computer for at least 6 h a day. 69 Therefore, the question should be, whether working in this amount of time with a computer would require a higher alertness level compared to, for example, paper work. Beneficial effects of lighting on alertness are often demonstrated.33–37 Linhart and Scartezzini 36 investigated the influence of different lighting situations on employee's work performance. They found that the performance for a paper-based task was better under the test scenario (lower LPD, higher illuminance level, higher uniformity) compared to the reference scenario. They did not find any significant difference between lighting scenarios for the computer-based task. Linhart and Scartezzini 36 concluded that it might be that the light environment has a much smaller influence on computer-based tasks or that the applied lighting systems were optimized for paper-based horizontal tasks instead of the vertical screen-based tasks. This conclusion is highly important for the current evolution towards working in a digital world.
This digital world is regularly accommodated in larger office spaces, so called office landscapes. Former research is mostly performed in conventional offices. This review includes seven articles that did not provide information about the office environment, i.e. there was no information on whether the research was carried out in a single or multiple user office. The majority of studies of which the environment was specified in articles was performed in single occupant offices. Nearly all single occupant offices were simulated offices (i.e. lab test rooms offering not the exact office setup participants would be used to in their own work environment). There were slightly more laboratory studies included in this review (five articles regarding surveys, six articles regarding field studies and nine articles regarding laboratory studies) and these studies have shown different aspects that were investigated compared to field studies. In most cases, there was an agreement between results from three types of experiments (e.g. the importance of daylight availability which is highlighted in articles of all three types of experiments).
Recommendations
Under laboratory conditions it is easier to adapt lighting conditions in order to seclude one single aspect and draw potential relationships between this single lighting aspect and OH outcomes. While a laboratory study allows for a controlled experimental environment, a field study is often more realistic as it automatically includes multiple possible influential variables (e.g. illuminance and CCT, but also variables not related to the lighting conditions). The limitation of a field study is that one cannot exclusively investigate the effect of one specific lighting aspect on a potential health outcome. In order to investigate the interaction between office light conditions on OH, field studies in realistic office environments are recommended. Challenges of field studies are that those studies are usually demanding and costly.
In addition to the research design, we need to share knowledge and to collaborate with experts from other fields when performing light and health research. Health experts can help lighting experts in defining criteria for selecting a participant sample, and lighting experts can help health experts in measuring and describing lighting conditions properly.
Conclusion
This research investigated studies on office light conditions and its relation to OH outcome measures based on literature. Showing a causal relationship between office light conditions and OH outcomes is beyond the scope of this paper. However, the review summarizes correlations from 20 eligible studies that carried out research on this relationship and based on this literature study, an overview of office light conditions and OH has been proposed. All health aspects were mostly but not exclusively measured subjectively.
This literature review recommends to
measure and describe conditions (both light and health) as comprehensive as possible; investigate a wide variety of behavioural and health outcomes; collaborate with researchers from other field of studies.
Measuring health aspects in combination with measuring lighting conditions requires knowledge of both fields. Light and health research is a multidisciplinary field. Therefore, it is highly recommended to measure and describe conditions as comprehensive as possible. Elaborative descriptions and explanations of research methodologies enable researchers to reproduce studies. Researchers often investigate a part of OH in relation to lighting conditions, whereas the CIE recommended researchers to investigate a wide variety of behavioural and health outcomes. 24 The overview in this article includes all OH outcomes that were subject in the past and potentially assailable by lighting parameters. This overview, together with the complete literature review, will be used to place all research findings (including future experiments) in relation to each other, to design new study objectives and to conduct further research.
Footnotes
Authors' contribution
All authors contributed equally to the manuscript. The first draft of this manuscript was written by J. van Duijnhoven and afterwards all co-authors revised and supported significantly in improving the manuscript.
Acknowledgement
This research was performed within the framework of the strategic joint research program on Intelligent Lighting between TU/e and Koninklijke Philips N.V. and the Impuls II SPARK program. Dr. Kelly Ann Mulder is recognized for her contributions in the language check.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.