
Abstract
Aim:
The sim of this study was to quantify contributions of mortality from drugs, alcohol and suicide (termed as ‘deaths of despair’ (DoD)) to changes in life expectancy at birth across sexes and regions in Sweden.
Methods:
We obtained annual data on underlying causes of deaths by age, sex and region from the National Cause of Death Register. We constructed abridged life tables for two periods: 2001–2005 and 2020–2024. A continuous-change model was used to quantify the age- and cause-specific contributions of DoD to the changes in life expectancy at birth between these periods.
Results:
Between two periods, life expectancy at birth increased by 2.5/3.5 years for females/males. All three DoD combined had negligible but opposite contributions to the changes in life expectancy at birth among females (–0.017 years) and males (+0.101 years). In both sexes, drugs- (alcohol)-related deaths contributed to decrease (increase) in life expectancy at birth. In both sexes, deaths from suicide in the age group 10–19 years (negative contributions), drugs in the age group 30–39 years (negative contributions) and alcohol in the age groups 40–59 years (positive contributions) and 70–89 years (negative contributions) had a greater absolute contribution to the changes in life expectancy at birth than the other two DoD causes. Across regions, the changes in life expectancy at birth attributable to DoD ranged from −0.219 to +0.159 years among females and from −0.235 to +0.267 years among males.
Conclusions:
Background
Over the past century, there have been remarkable improvements in life expectancy across the globe. However, these life expectancy improvements have gradually slowed in many high-income countries [1,2]. In particular, life expectancy declined in the US in 2015 for the first time in more than two decades with subsequent declines in 2016 and 2017 [2]. This has prompted extensive investigations into the root causes of the phenomenon. As articulated by Case and Deaton, this trend is largely attributable to rising mortality from suicide, drug poisoning and alcohol-related diseases among middle-aged non-Hispanic white individuals with lower educational attainment [3]. They coined the term ‘deaths of despair’ (DoD) for these causes of death, arguing that these are caused by psychological distress induced by rapid social and economic changes including deteriorating labour market opportunities and weakening of traditional social structures [3]. Further studies showed comparable increases in DoD in almost all sex and race/ethnic groups in the US [4].
Increasing mortality rates from DoD are not unique to the US, as studies conducted in other countries have also reported rising trends in recent years [5,6]. Sweden is among countries with an increased mortality among those aged 20–44 years [7]. A recent study revealed an alarming mortality development among Swedish young adults aged 20–34 years, a trend that diverged from other Western European countries and more closely resembled the US pattern, mainly owing to deaths from substance use [7]. Indeed, whilst mortality rates due to DoD among those aged 20–34 years in Western Europe, as a whole, decreased from 16.3 to 13.1 per 100,000 person-years between 2001–2005 and 2016–2019, rates increased from 15.0 to 22.0 in Sweden and from 24.5 to 49.7 in the US over the same period [8].
Over recent decades Sweden has been facing social crisis, including rising income and wealth inequality, and crimes as well as employment insecurity and income inadequacy [9,10]. Moreover, Sweden has witnessed widening regional disparities in economic growth and well-being [11]. These ongoing changes can initiate or exacerbate psychological distress with profound consequences for population health. Despite these concerning trends, there is a significant evidence gap in our understanding of the influences of DoD on population health in Sweden. Specifically, the estimates of the contributions of DoD, as a combined phenomenon, to the changes in life expectancy over recent decades in Sweden and across its regions are non-existent. This study aimed to address this knowledge gap by quantifying the sex-, age- and cause-specific contributions of DoD to the changes in life expectancy at birth in Sweden and across its 21 regions since the turn of the 21st century.
Methods
Setting
Sweden is a high-income country with a population of approximately 10.5 million. Sweden is divided into 21 administrative regions which are mainly responsible for health care, transport and regional development [11]. The regions’ populations range from about 61,000 in Gotland to around 2.5 million in Stockholm. Moreover, population density across regions ranges from 2.6/km2 in Norrbotten in the north to 376.9/km2 in Stockholm (https://www.statistikdatabasen.scb.se/pxweb/en/ssd/).
Data sources
We obtained aggregated annual data on underlying causes of death by sex and age group (0-4, 5-9, 10–14, 15–19, . . . 90–94, 95+ years) in Sweden and across its 21 regions from the National Board of Health and Welfare’s database (https://sdb.socialstyrelsen.se/if_dor/val_eng.aspx). This public database covers all individuals who died during one calendar year and were registered as living in Sweden at the time of death, regardless of whether the death occurred inside or outside the country. The database currently provides data on underlying causes of deaths, classified according to the International Classification of Diseases, 10th revision (ICD-10), for the period 1997–2024. We extracted data for two five-year periods: 1) 2001–2005 and 2) 2020–2024. These periods were selected to explore the changes in life expectancy from the turn of the new millennium to the most recent years. Data were aggregated over five years to mitigate the effect of random year-by-year fluctuations, especially at regional level. The population data by sex, age group and region were extracted from Statistics Sweden (https://www.scb.se/en/).
Causes of death
We used ICD-10 codes to classify all deaths into the following underlying causes [5]: 1) drug-related deaths (F11–F16, F18–F19, X40–X44, Y10–Y14), 2) suicide (X60–X84, Y87), 3) alcohol-related deaths (F10, K70, K73–K74, X45), and 4) all other causes. The first three categories were considered as DoD.
Data analysis
Using death and population numbers, we constructed abridged life tables for each period and location (i.e. Sweden and each region) and computed the sex- and period-specific life expectancy at birth. Life expectancy at birth in each period indicates the average number of years a newborn can expect to live if the period mortality patterns continue to apply in her or his remaining life. We used a continuous-change model to decompose the change in life expectancy between different periods by age and causes of death [12]. This is a linear integral decomposition method relying on the assumption that life expectancy is a differentiable function of the age-cause-specific death rates and effects of these death rates are additive. It also assumes that the age-cause-specific death rates change proportionately along a dimension (e.g. time) [12]. We conducted separate analyses by sex and regions. Data analysis was conducted in RStudio using the package DemoDecomp.
Results
The proportion of DoD from all deaths among males and females in Sweden rose from, respectively, 4.1% and 1.5% in 2001–2005 to 4.3% and 1.9% in 2020–2024. The percentage of DoD from all deaths rose in all age groups between the periods (Figure A1 in Supplemental material online). Across age groups, the greatest proportions of DoD from all deaths were observed among those aged 20–29 years in both sexes. Across regions, Stockholm had the highest percentage of DoD among males in 2001–2005 (5.2%), while Jämtland (4.9%) had the highest in 2020–2024. Among females, Stockholm had the highest percentage of DoD from all deaths in both periods (2.1% in 2001–2005 and 2.3% in 2020–2024).
Among females life expectancy rose by 2.5 years from 82.3 years in 2001–2005 to 84.8 years in 2020–2024 in Sweden (Table I). The corresponding rise among males was 3.5 years from 78.0 to 81.5 years between the periods. Across regions, Halland had the highest life expectancy for both sexes in both periods. The increases in life expectancy in females ranged from 1.3 years in Blekinge to 3.8 years in Gotland. Corresponding rises in males ranged from 2.4 years in Västmanland to 4.1 years in Stockholm. While DoD contributed to life expectancy increases among males (+0.101 years), they contributed to the life expectancy decreases among females (–0.017) in Sweden, even though their contributions were negligible in both sexes. Across regions, DoD contributed to increases in life expectancy for both sexes in seven regions (Gotland, Halland, Jönköping, Stockholm, Uppsala, Örebro, Östergötland) and only for males in seven regions (Gävleborg, Kalmar, Kronoberg, Skåne, Södermanland, Västerbotten, Västra Götaland) (Figure 1). The most notable negative relative contributions of DoD to the change in life expectancy were seen in Belkinge in both sexes (–0.22 years out of 1.31 years among females and −0.24 years out of 2.62 years among males).
Life expectancy at birth and contributions of deaths of despair (DoD) to changes in life expectancy at birth over time, stratified by sex and region.
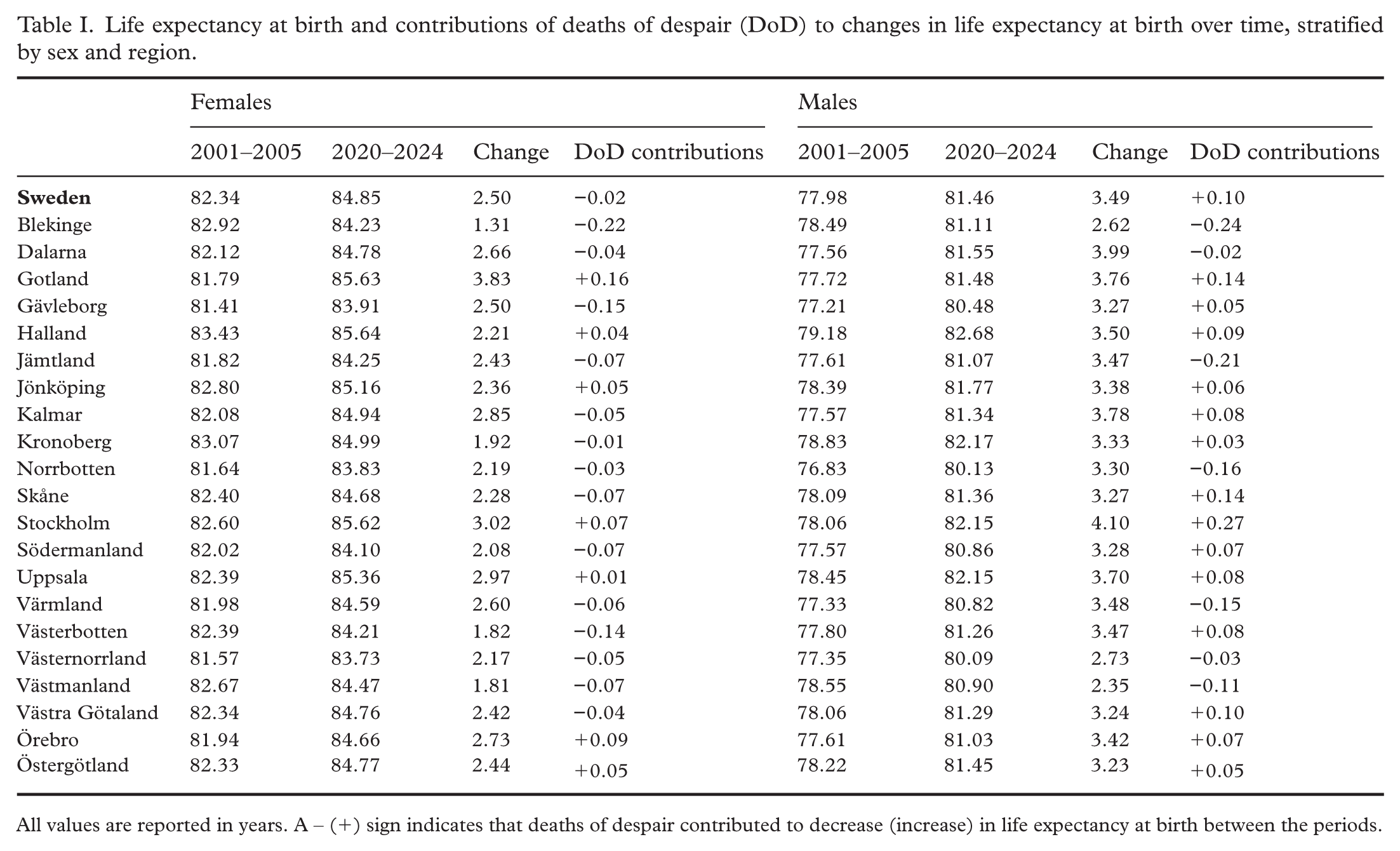
All values are reported in years. A – (+) sign indicates that deaths of despair contributed to decrease (increase) in life expectancy at birth between the periods.
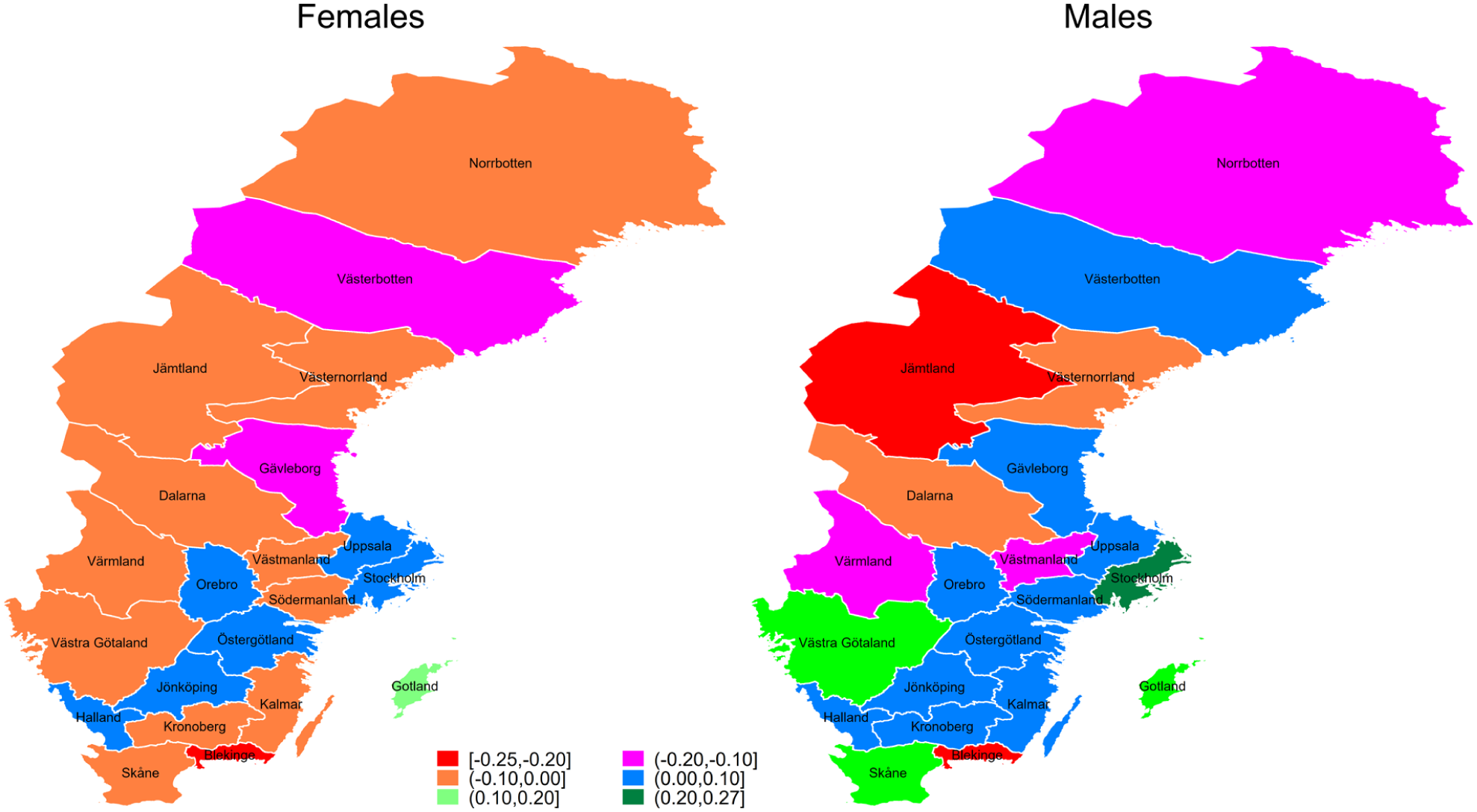
Regional variations in the contributions of deaths of despair to changes in life expectancy at birth between 2001–2005 and 2020–2024.
Age-specific contributions of DoD revealed that the age groups 20–59 years had the most notable contributions to the changes in life expectancy in both sexes in Sweden, with negative and positive contributions from the age groups 20–39 and 40–59 years, respectively (Figure 2). Across regions, the greatest absolute age-specific contributions of DoD to the change in life expectancy were seen in the age group 40–49 years in Gotland for males (+0.16 years) and in the age group 20–29 years in Blekinge for females (–0.08 years). Among females, the age groups 20–29 and 30–39 had the greatest absolute contributions to the change in life expectancy in 14 regions (seven regions each) with mostly negative contributions, while among males the age groups 40–49 (all positive) had the greatest contributions in eight regions.
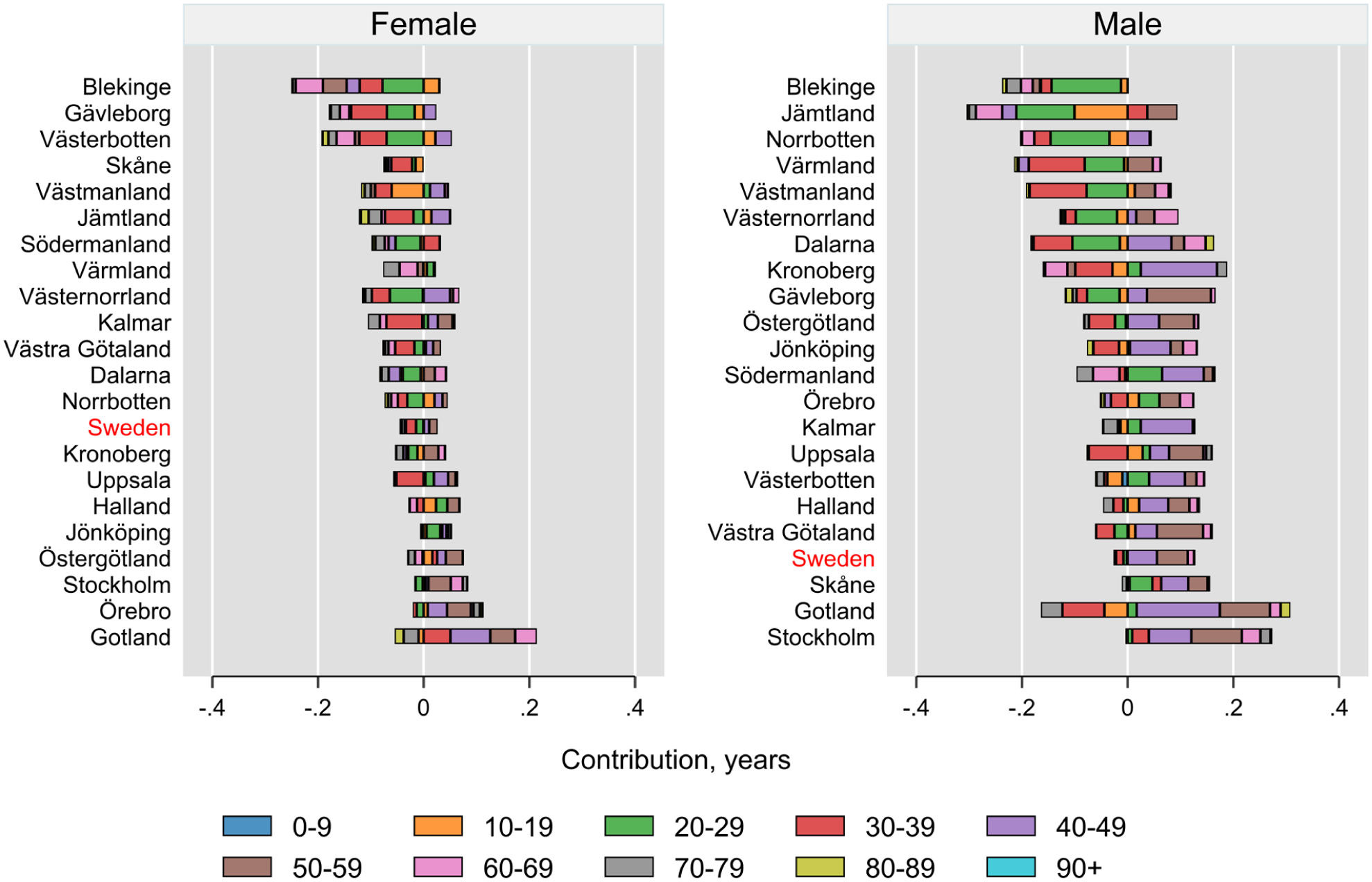
Age-specific contributions of deaths of despair to changes in life expectancy at birth between 2001–2005 and 2020–2024 in Sweden and across its regions, stratified by sex. Regions are sorted by the total contributions of deaths of despair.
While drug-related deaths accounted for 14.0% and 12.2% of all DoD in males and females, respectively, in 2001–2005, these percentages rose to about 19% in both sexes in 2020–2024. The cause-specific contributions showed that among DoD, deaths from drugs in both sexes contributed to decreases in life expectancy in Sweden (Figure 3). Across regions, the largest absolute cause-specific contributions were reported for drug-related deaths among females in Blekinge (–0.14 years) and for suicide among males in Jämtland (–0.21 years). Simultaneous negative contributions of all three causes of DoD to the change in life expectancy were observed across four regions (Blekinge, Skåne, Västerbotten, Västernorrland) among females and in one region (Blekinge) among males. On the other hand, simultaneous positive contributions were reported only for males in two regions (Skåne and Stockholm). Among males, alcohol-related deaths contributed to the life expectancy decrease only in Blekinge.
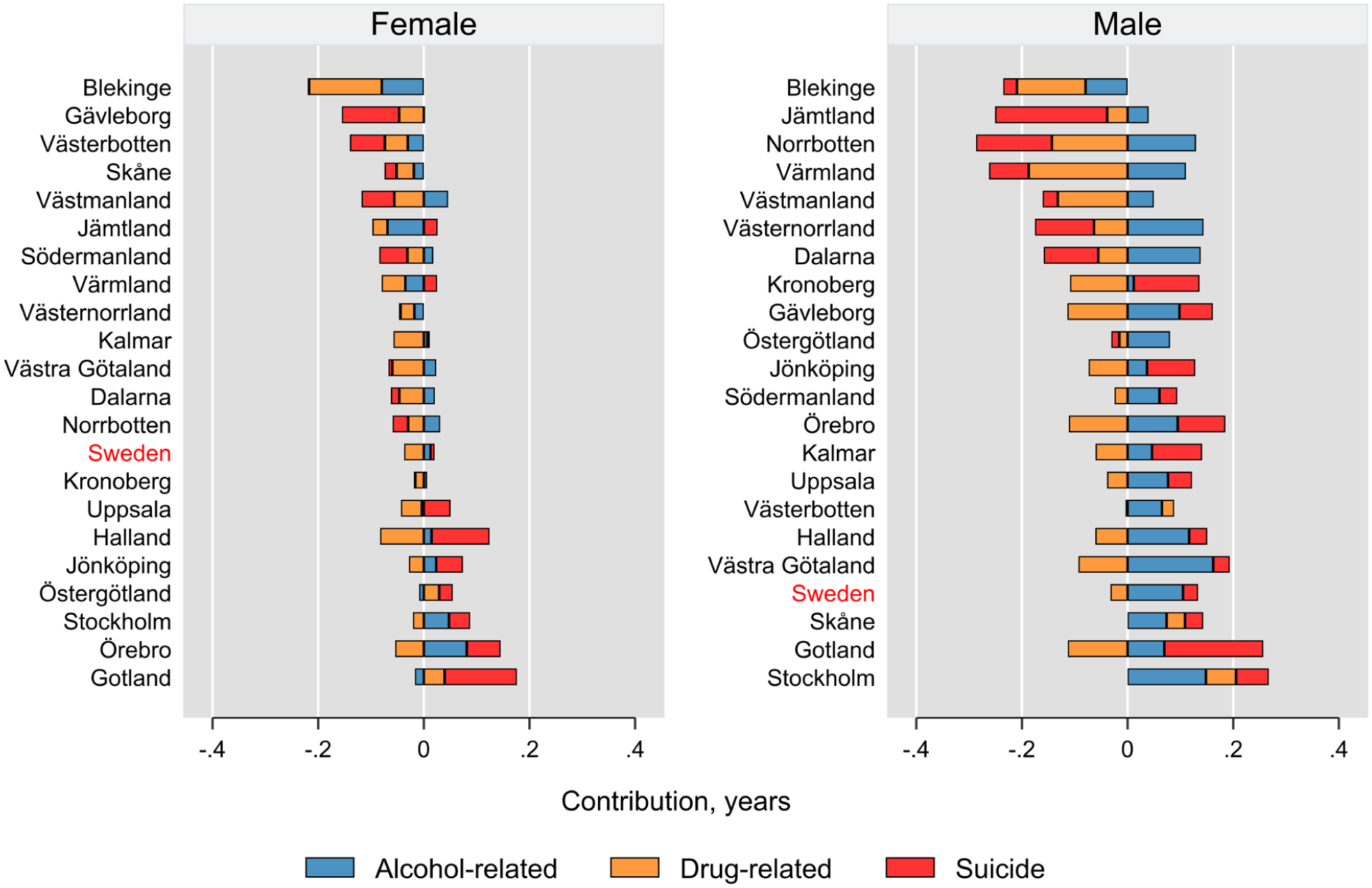
Cause-specific contributions of deaths of despair to changes in life expectancy at birth between 2001–2005 and 2020–2024 in Sweden and across its regions, stratified by sex. Regions are sorted by the total contributions of deaths of despair.
The age- and cause-specific contributions of DoD in Sweden revealed that drug-related deaths contributed to decreases in life expectancy among the age groups 20–79 years for females and among the age groups 30–44 and 50–79 years for males (Figure 4). In both sexes, suicide and alcohol-related deaths contributed to increases in life expectancy in the age groups 40–59 years. Alcohol-related deaths had negative contributions to the changes in life expectancy in the age group 70+ years in both sexes. Suicide in the age groups 10–29 and 80+ years, drug-related deaths in the age group 30–39 years and alcohol-related deaths in the age groups 40–79 years had the greatest absolute contributions to the changes in life expectancy in a larger number of regions among DoD causes (Figures A2–A3 in the Supplemental material).
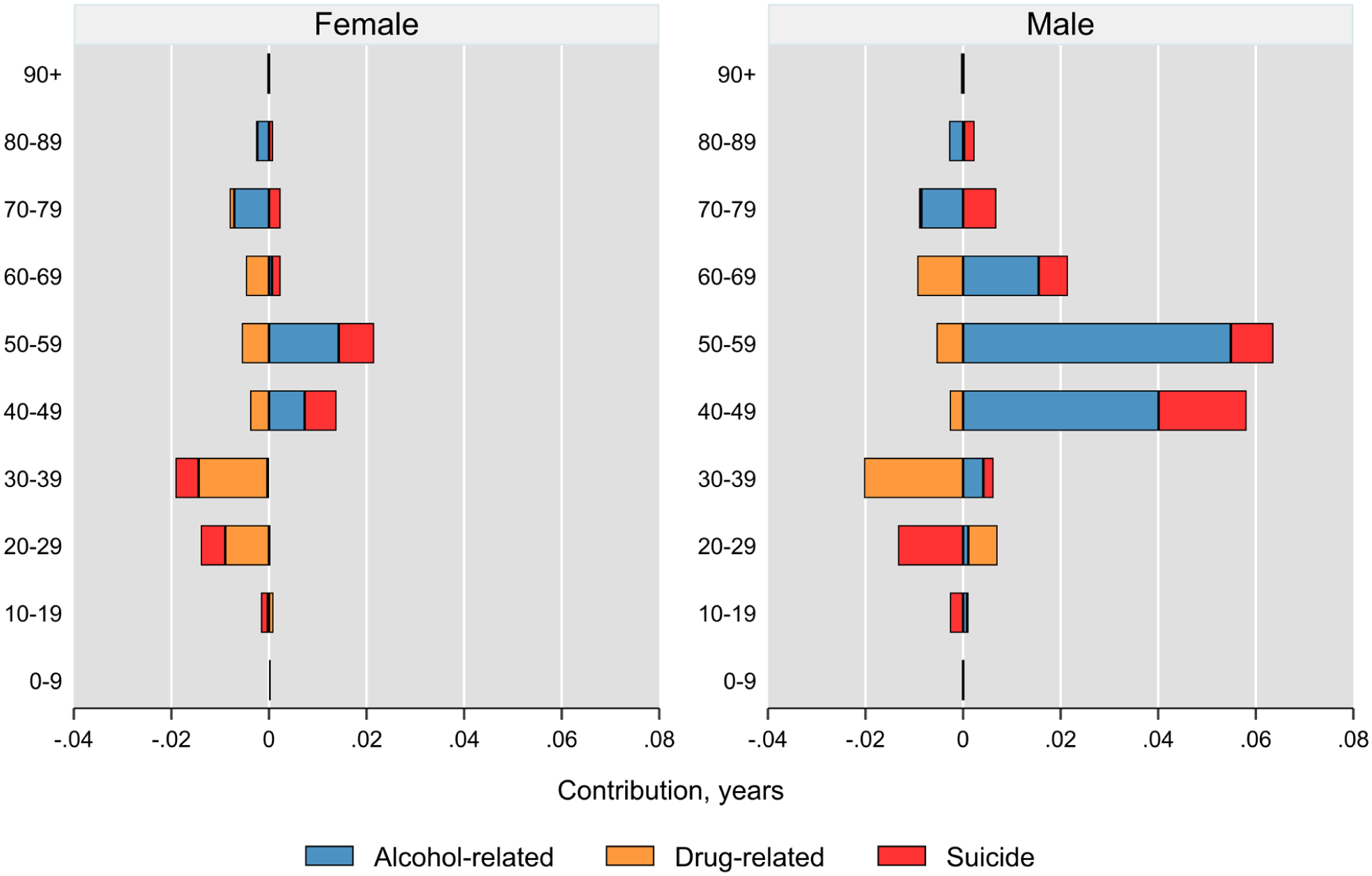
Age- and cause-specific contributions of deaths of despair to changes in life expectancy at birth between 2001–2005 and 2020–2024 in Sweden, stratified by sex.
Discussion
In this study, we investigated the contributions of mortality from drugs, alcohol and suicide to the change in life expectancy at birth in Sweden and across its regions during the 21st century. Our results showed that, overall, these deaths had negligible but opposite contributions to the change in life expectancy among females (negative) and males (positive) in Sweden. While DoD in the age groups 10–39 and 70–89 years contributed to decreases in life expectancy in both sexes, the opposite was seen for the age groups 40–59 years. Across specific DoD causes, drug-related deaths contributed to decrease in life expectancy, whereas alcohol-related deaths and suicide contributed to increases in life expectancy in both sexes. Our results also revealed substantial regional variations in age- and cause-specific contributions of DoD to the changes in life expectancy.
We are not aware of prior studies that explicitly quantified the contributions of DoD as a combined entity to changes in life expectancy over time. While the contributions of DoD components to changes in life expectancy have been examined, cross-study comparisons are constrained by differences in the list of ICD codes used to define these causes—particularly for drug- and alcohol-related deaths—and by differences in timeframes. For instance, using comparable ICD-10 codes for suicide, a recent analysis across the Group of Seven (G7) countries reported that the contributions of suicide to changes in life expectancy between 2001–2003 and 2017–2019 ranged from 0.061 year decrease (US) to 0.086 year increase (France) among females and from 0.118 year decrease (US) to 0.232 year increase (Japan) among males [13]. In comparison, Sweden’s estimates in the present study were closest to Italy among females (0.008 vs. 0.010 years) and to France among males (0.028 vs. 0.023).
Negligible contributions of DoD to the changes in life expectancy suggest that there has been little change in these causes of deaths, particularly drug-related deaths, compared with other causes over time in Sweden. These less favourable changes in DoD in Sweden are consistent with previous research [7,14,15]. Compared with other Nordic countries, Sweden experienced greatest growth in the age-standardized rate of years-of-life-lost attributable to drug use, which rose by 193% (97%) from 1990 to 2019 among males (females) [15]. In a study exploring the contributions of DoD to differences in life expectancy at birth between the US and 12 other counties, Sweden was the closest to the US in drug-related deaths in both sexes [14]. Another study documented unfavourable temporal trends in suicide and drug-related deaths among young adults in Sweden compared with other Western European countries [7]. A recent study also reported a stable temporal trend in the incidence rates of substance use disorders registered at inpatient and outpatient specialist care facilities among young and middle-aged adults in Sweden during 2004–2019 [16]. These findings are consistent with our findings suggesting that DoD, primarily drug-related mortality, among younger adults (20–39 years) contributed to decrease in life expectancy. These unfavourable trends might suggest growing psychological distress caused by increasingly complex social, environmental and economic challenges in Sweden. For instance, there has been a tendency toward increasing wealth and income inequalities in recent times in Sweden [9,17]. Moreover, precarious employment reflecting employment insecurity and income inadequacy has been rising in Sweden [10]. Sweden also underwent an educational reform in the 1990s that merged vocational and academic tracks, which has resulted in a greater mismatch between the educational institutions and the labour market and thereby has left many less academically inclined youths without viable career training [7,18]. Increases in drug prescription coupled with drops in the street price of illicit drugs in Sweden might have also contributed to these trends [7].
We observed variations in contributions of DoD to the changes in life expectancy by sexes in Sweden as well as within its regions. The positive contributions of DoD among males and negative contributions among females implies that DoD contributed to the narrowing sex differences in life expectancy in Sweden. This is consistent with recent evidence reporting the narrowing sex differences in life expectancy due to avoidable causes of death, including suicide and alcohol- and drug-related deaths in Sweden [19,20]. For instance, the sex gap in life expectancy at birth decreased by 1.85 years between 1997 and 2018 with suicide, alcohol- and drug-related deaths accounting for 0.24 years (12.6%) of this narrowing gap [19]. This sex difference might reflect varying risk factors, health-seeking behaviours and social norms between males and females. Moreover, owing to lower rates of DoD in females than males, their experiences might have been underrepresented or inadequately addressed in the formulation of policies and preventive interventions aimed at reducing DoD.
The observed regional variations in DoD are in line with previous studies highlighting regional disparities in health outcomes, including life expectancy at birth as well as DoD among youth in Sweden [8,21]. Specifically, Ågren and Bremberg reported regional variations in DoD among individuals aged 20–34 years with higher mortality rates observed in low population density regions—referred to as the ‘forest regions’, including Norrbotten, Västerbotten, Jämtland, Västernorrland, Gävleborg, Dalarna and Värmland [8]. Higher rates of attempted and completed suicides in rural compared with urban communities, especially among males, have also been reported in Sweden [22]. Our findings also support this pattern specifically among males, with five out of seven regions showing decreases in life expectancy from DoD within these forest regions. Geographic variations in level and temporal trends of DoD have also been documented in other countries [23 –25]. Regarding rural–urban differences in DoD, while many studies—particularly from the US—reported higher rates of DoD (or its components) in rural/remote or less densely populated communities compared with urban/higher densely populated areas [26], this is not a universal observation [23]. Regional variations in DoD might reflect regional differences in the mechanism underlying DoD, such as economic opportunities, social ties, access to and use of mental health services, cultural factors, rural/urban composition, and behavioural risk factors. Specifically, remote/rural areas generally have higher rates of socioeconomic disadvantages (e.g. poverty, unemployment), greater physical/social isolation, more stigmatization toward people with mental health problems and poorer access to resources, including mental health services [27]. Moreover, out-migration of younger and healthier individuals from rural/remote areas can increase economic disadvantages and creates a higher concentration of adults who are at increased risk of DoD [27].
Our findings might highlight the need for improving employment opportunities and enhanced mental health services and substance abuse treatment programmes, particularly for young adults and for the sparsely populated regions. For example, implementing targeted social support for young adults who are not in education, employment or training (commonly referred to as the NEET population), along with investments in youth centres, peer support initiatives and recreational programmes in vulnerable communities might help address the structural determinants of despair. Strengthening vocational training pathways may provide skills and jobs for those left behind by the 1990s’ educational reform.
Our study results should be interpreted in light of some limitations. The cause of death data are prone to coding errors, underestimation and misclassification. Given the social stigma surrounding DoD, these causes are particularly likely to be underestimated as underlying cause of death. However, a validation study reported that the coding of suicide deaths in the cause of death register in Sweden is reliable, with a high percentage of deaths registered as suicides being confirmed as being suicide [28]. Any temporal and/or regional patterns in these errors could introduce bias into our estimates. The concept of DoD has been criticized for aggregating distinct causes of death that share limited etiological commonalities [29]. Owing to data availability, regions were used as the geographic unit of analysis in this study, and the findings might be sensitive to this choice. In other words, an alternative geographic unit (e.g. neighbourhood or municipality) might yield different results. The second period (2020–2024) coincides with the COVID-19 pandemic, which might influence our estimates. However, a previous study from Sweden reported that trends in suicide and alcohol-specific mortality remained relatively stable during 2016–2021 and were not significantly influenced by the pandemic [30]. As this study is an ecological descriptive study, all explanations should be viewed as speculative with no causal implications.
Conclusions
Our findings suggested a small increase in the proportion of DoD from all deaths in Sweden over recent decades, mainly driven by drug-related deaths. DoD disproportionately affected younger age groups, with the highest percentage of DoD from all deaths observed in individuals aged 20–29 years. We found significant variations in the contributions of DoD to the changes in life expectancy by age, cause, sex and region. Notably, DoD had a marginal but opposing impact on the change in life expectancy for males and females. These results highlight the importance of addressing drug-related mortality, especially among young and middle-aged adults, to reduce regional disparities and enhance overall life expectancy in Sweden.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948261450785 – Supplemental material for How deaths of despair shape life expectancy across sexes and regions in Sweden
Supplemental material, sj-pdf-1-sjp-10.1177_14034948261450785 for How deaths of despair shape life expectancy across sexes and regions in Sweden by Ali Kiadaliri, Alexis E. Cullen, Oleguer Plana-Ripoll and Mohammad Hajizadeh in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AEC has received consultancy fees from Stratenym Inc. and Symmetron Ltd. Other authors declare they have no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the Crafoord Foundation. Mohammad Hajizadeh acknowledges the Canada Research (CRC) Program (grant # CRC-2020–00219; ![]() ) for their support.
) for their support.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.