
Abstract
Aims:
There is a strong achievement-gradient in attention-deficit hyperactivity disorder (ADHD), with a higher prevalence in children with low academic achievement. In Sweden, the prevalence of ADHD is also higher among native than immigrant children. The aim of this study was to investigate whether the change in diagnosed ADHD varies across different achievement levels, and whether this change in turn differs depending on students’ immigration status.
Methods:
Register data on all students graduating from compulsory school in Sweden between 2001 and 2018 were used. ADHD was measured by diagnosis in specialised care recorded in the year of graduation, and academic achievement by students’ grade point average. Logistic regression models with ADHD as the outcome were used. Changes in the association between achievement and ADHD over time were tested by including interactions terms for achievement and year.
Results:
There was a positive interaction between achievement and year in the pooled sample, meaning that ADHD increased relatively more among higher-achieving students and that the achievement-gradient in ADHD diminished over time. In stratified analyses, the greatest relative increase in ADHD was observed among higher-achieving native and second-generation immigrant students, and the smallest among low-achieving first-generation immigrants. The achievement-gradient was flatter, and diminished more, among immigrant students.
Conclusions:
Keywords
Introduction
The share of children diagnosed with attention-deficit hyperactivity disorder (ADHD) has increased globally [1 –3]. The Swedish increase is greater than in most comparable countries, including its Scandinavian neighbours [3], and Sweden now has among the highest consumption of ADHD-medications per child in the world [1,4]. The increase in diagnoses is not paralleled by a corresponding increase in self- or proxy-reported symptoms or in the share of children with clinical levels of symptoms [5 –9], raising questions concerning diagnostic expansion [8,10]. Diagnostic expansion may be understood as the broadening of disease boundaries or lowering of diagnostic threshold, either through explicitly relaxed diagnostic criteria or changed clinical practice [11]. Diagnostic expansion does not necessarily entail overdiagnosis but may also result from reduced underdiagnosis [12].
ADHD is best understood in dimensional terms, representing the extreme end of a spectrum but with no clear threshold separating pathological from healthy cases [13 –16]. The diagnostic expansion hypothesis entails that, as the prevalence of ADHD increases, a disproportionate number of cases will be at the milder end of the spectrum [17]. One implication is that the degree of functional impairment of diagnosed cases will be inversely related to the prevalence of, and diminish in tandem with the rise in, diagnoses. Several diagnostic criteria for ADHD refer to academic difficulties such as making careless mistakes in, or failing to finish, schoolwork, and school is also a key form of functioning against which the degree of impairment is assessed [18]. Consequently, ADHD is among the psychiatric disorders associated most strongly with low academic achievement [19]. The diagnostic expansion hypothesis predicts that this association should become weaker over time as the prevalence increases.
Given the negative association between ADHD and achievement, one might expect higher rates of ADHD among immigrant children, who are overrepresented among low-achieving students. However, this is not the case in Sweden, where both first- and second-generation immigrants have lower prevalence of ADHD than children with a native background [20]. The differences in diagnostic rates between native and immigrant children are not matched by corresponding differences in self and proxy-reported symptoms [7,21,22].
To our knowledge, no study has investigated whether achievement-related differences in ADHD differ by immigration status, and only one has investigated whether trends in ADHD differ depending on academic achievement: Nordmo et al. found that the negative association between ADHD and academic achievement weakened among Norwegian students between 2006 and 2019 [23]. We extend their work by focusing on the intersection between academic achievement and immigration background. Using Swedish register data on compulsory school graduates over the period 2001–2018, the aim of this study was to investigate whether the change in diagnosed ADHD in the year of graduation varies across achievement levels, and whether this change differs in turn depending on students’ immigration status.
Data and methods
Data on ADHD were extracted from the National Patient Register, data on academic achievement from the National Pupil Register and data on country of birth from the Total Population Register. All students graduating from the final year (year 9) of compulsory school in Sweden (aged approximately 16 years) with data on specialised out- or inpatient care (2001–2018) were included (N = 1,986,761). In cases where children graduated more than once (N = 7,331), only the first year was used in the analysis. Data were made available by the Umeå SIMSAM Laboratory [24]. The study was approved by the Swedish Ethical Review Authority (Dnr 2023-05360-02). Informed consent was not applicable as the study used register data.
Outcome: ADHD
The National Patient Register covers specialised outpatient or inpatient physician visits in public care and partially in private care. Specialised child- and adolescent psychiatry has primary responsibility for investigating and treating children with ADHD. Children were coded 1 if they had a specialised care visit at least once with International Statistical Classification of Diseases (ICD) 10 code F90 as the primary diagnosis in the year of graduation, and zero otherwise.
Independent variables
Academic achievement was measured using students’ final compulsory school grades. Students are graded in 16 or 17 different subjects, and their subject grades are totalled into a grade sum (henceforth: grade point average (GPA)). Students with fail-grades, or no grades because of absenteeism, obtain 0 credits but are kept in the analyses. Grades are the most salient measure of achievement in Swedish schools and are used to determine access to upper secondary schools or programs. GPA was transformed into quartiles (percentiles 1–25, 26–50, 51–75 and 76–100) within each cohort to account for grade inflation.
Time was operationalised as the year of graduation (2001–2018) and used as a continuous variable.
Immigration status was categorised into (a) Swedish-born with at least one Swedish-born parent (henceforth: native); (b) Swedish-born with two foreign-born parents (henceforth: second-generation immigrant), and (c) foreign-born (henceforth: first-generation immigrant); 87 students lacked data on immigration status.
Confounders included student sex (boy/girl), birth month and parental education (lower secondary, upper secondary or post-secondary). There was no missing data on sex or birth month. Parental education was missing for 13,648 (0.7%) students, most of whom (11,549) were first-generation immigrants. Missing data on education was used as a separate category in the analysis.
Statistical analysis
The following logistic regression model was estimated:
Where p(ADHD = 1) is the probability of ADHD,
Odds ratios (ORs) from logistic regression measure multiplicative interaction and thus relative differences. Relative differences are the most relevant measure given the theoretical framing of the study. The diagnostic expansion hypothesis predicts that a disproportionate share of new cases will be at the milder end of the spectrum, which implies that ADHD should increase relatively more among higher-achieving students. Absolute differences are less informative in this regard, as they are influenced heavily by baseline prevalence. Given the low prevalence of ADHD in the sample (1.5%), odds ratios approximate relative risks and can be interpreted as such.
Results
Table I shows summary statistics. The overall prevalence of ADHD during the period was 1.5%, and increased from 0.05% in 2001 to 3.95% in 2018 (Supplemental File A). Among the students, 82% had a native background, 8% were second generation immigrants and 10% were first generation immigrants.
Summary statistics (N = 1,986,761).
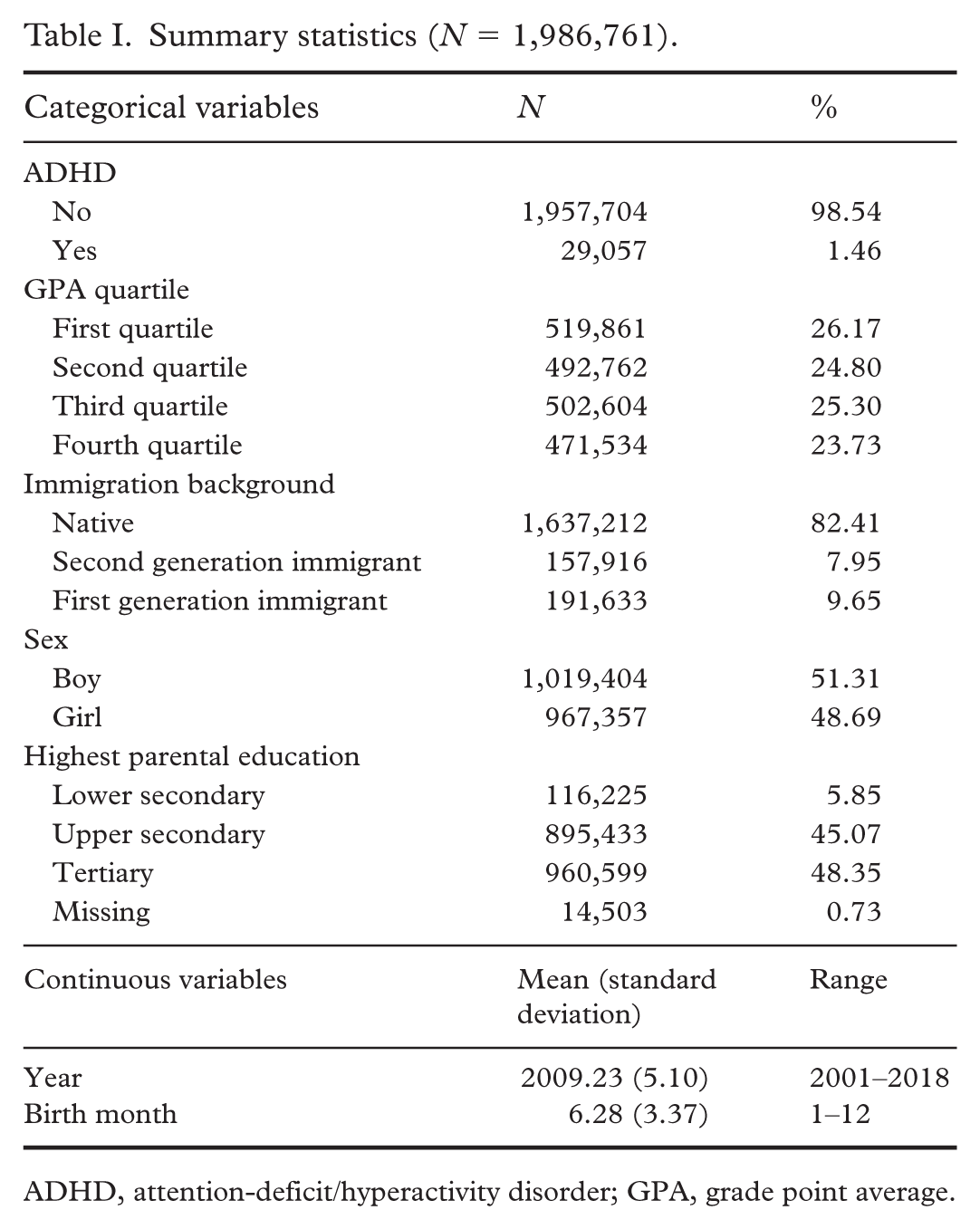
ADHD, attention-deficit/hyperactivity disorder; GPA, grade point average.
Table II shows results from Model 1. In the pooled sample, ADHD increased among low-achieving students (main effect of year; OR = 1.23, 95% CI [1.23,1.24]) and was associated negatively with achievement in the beginning of the period (main effects of GPA: second quartile: OR = 0.15, 95% CI [0.13,0.16]; third quartile: OR = 0.04, 95% CI [0.03,0.05]; fourth quartile: OR = 0.01, 95% CI [0.01,0.02]). The increase in ADHD was in relative terms greater among higher- than low-achieving students, meaning that the achievement-gradient in ADHD diminished over time (interaction between year and GPA: second quartile: OR = 1.05, 95% CI [1.05,1.06]; third quartile: OR = 1.08, 95% CI [1.07,1.09]; fourth quartile: OR = 1.09, 95% CI [1.07,1.11]).
Logistic regression models with specialised in- or outpatient care for ADHD as the outcome. a Stratified by immigration status.
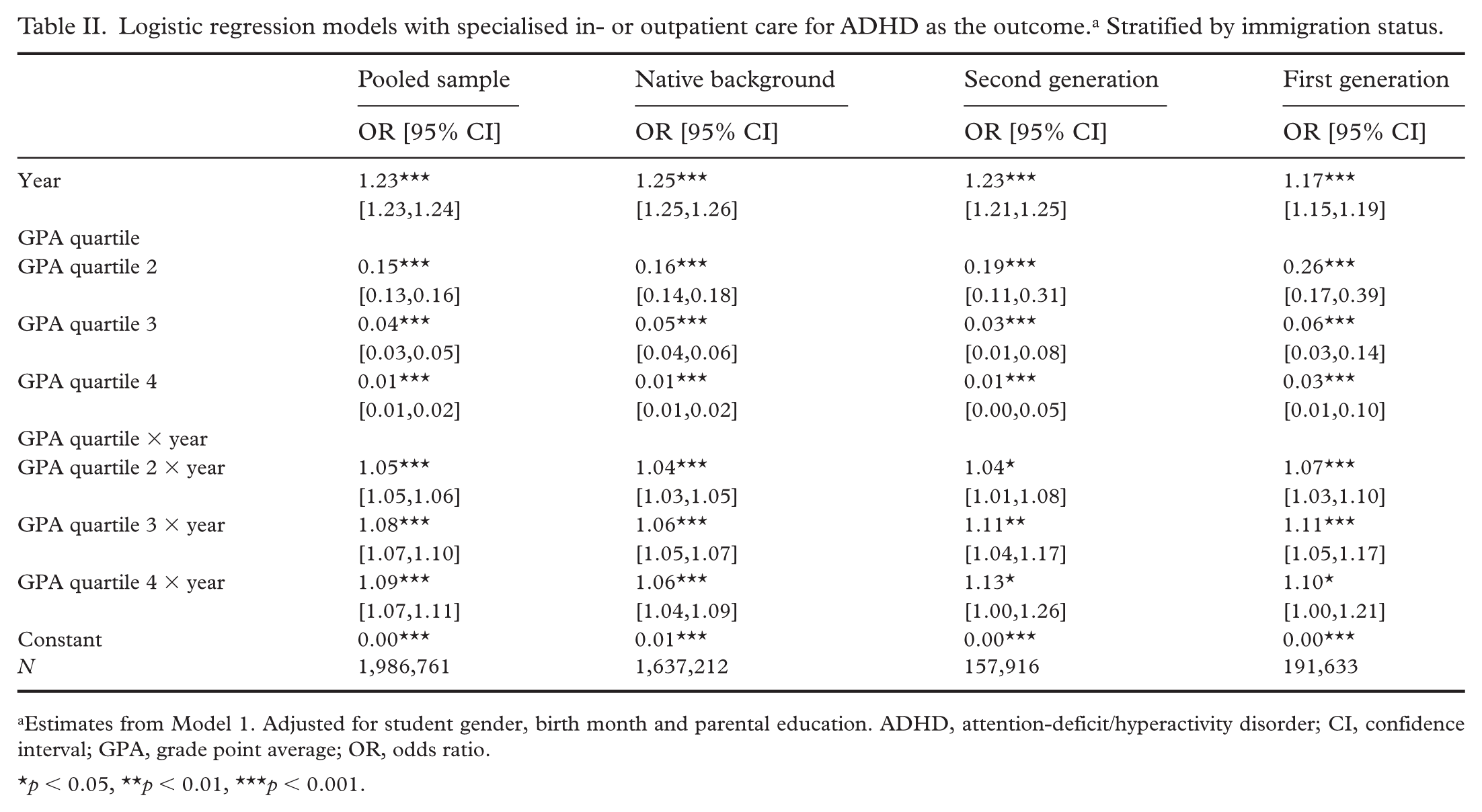
Estimates from Model 1. Adjusted for student gender, birth month and parental education. ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; GPA, grade point average; OR, odds ratio.
p < 0.05, **p < 0.01, ***p < 0.001.
Results stratified by immigration status show that the increase among low-achieving students was smallest for first-generation immigrants (main effect of year: native: OR = 1.25, 95% CI [1.25,1.26]; second-generation: OR = 1.23, 95% CI [1.21,1.25] first-generation: OR = 1.17, 95% CI [1.15,1.19]). The interaction terms between GPA and year are generally larger among both first and second-generation immigrants than among native students. For instance, the interaction between the fourth (highest) GPA quartile and year is 1.06 (95% CI [1.04,1.09]) for native-born students, but 1.13 (95% CI [1.00,1.26]) for second-generation and 1.10 (95% CI [1.00,1.21]) for first-generation, immigrants. Thus, the achievement-gradient diminished more among immigrant than among native students. The three-way interaction between year, GPA and immigration status was significant for first-generation (OR = 0.97; 95% CI [0.94, 1.00]) but not second-generation (OR = 0.98; 95% CI [0.95, 1.01]) immigrants when comparing the bottom with the remaining GPA quartiles (Supplemental File B).
Figure 1 shows results from Model 2 (exact coefficients in Supplemental File C). Within each group defined by immigration status, the smallest ORs for year are for the bottom GPA quartile, meaning that the increase over time in relative terms was smallest for low-achieving students. The largest increases are among the highest two quartiles, although these estimates are more imprecise.
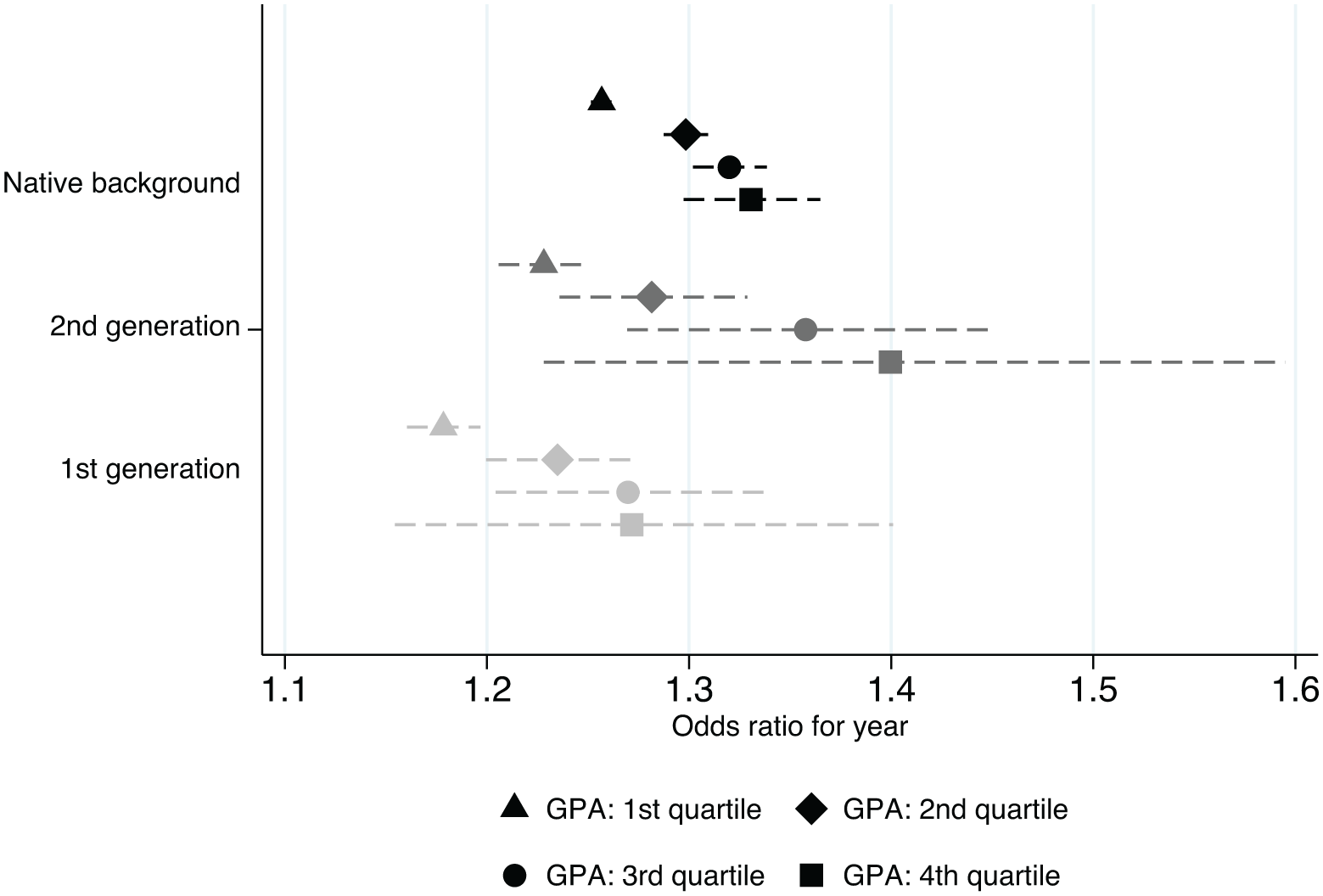
Logistic regression models with specialised in- or outpatient care for ADHD as the outcome. Stratified by immigration status. Markers show ORs, and dashed lines 95% CIs. Estimates from Model 2, adjusted for student gender, birth month and parental education. ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; GPA, grade point average; OR, odds ratio.
Table III illustrates the diminishing achievement-gradients by showing the prevalence of ADHD by GPA quartile (comparing the first with the second to fourth quartiles for brevity; full results in Supplemental File A) in an early (2001–2006) and a late (2016–2018) period, as well as the ratio between low-achieving (first quartile) and medium/high-achieving (second to fourth GPA quartiles) as a measure of the achievement-gradient. In 2001–2006, low-achieving native students had around 11 times higher prevalence of ADHD compared with medium-/high-achieving students, but this was reduced to around 6 in 2016–2018. The corresponding ratios for second-generation immigrants were around 10 in 2001–2006 and 4 in 2016–2018, and for first-generation immigrants around 4.5 in 2001–2006 and less than 2 in 2016–2018. Thus, the flatter achievement-gradient among especially first-generation immigrants relative to native students (see also Supplemental File D) became more pronounced over time. Note, however, that the greatest absolute increase was among low-achieving native students and that the achievement-gradient widened in absolute terms.
Prevalence of specialised in- or outpatient care for ADHD by academic achievement and immigration status.
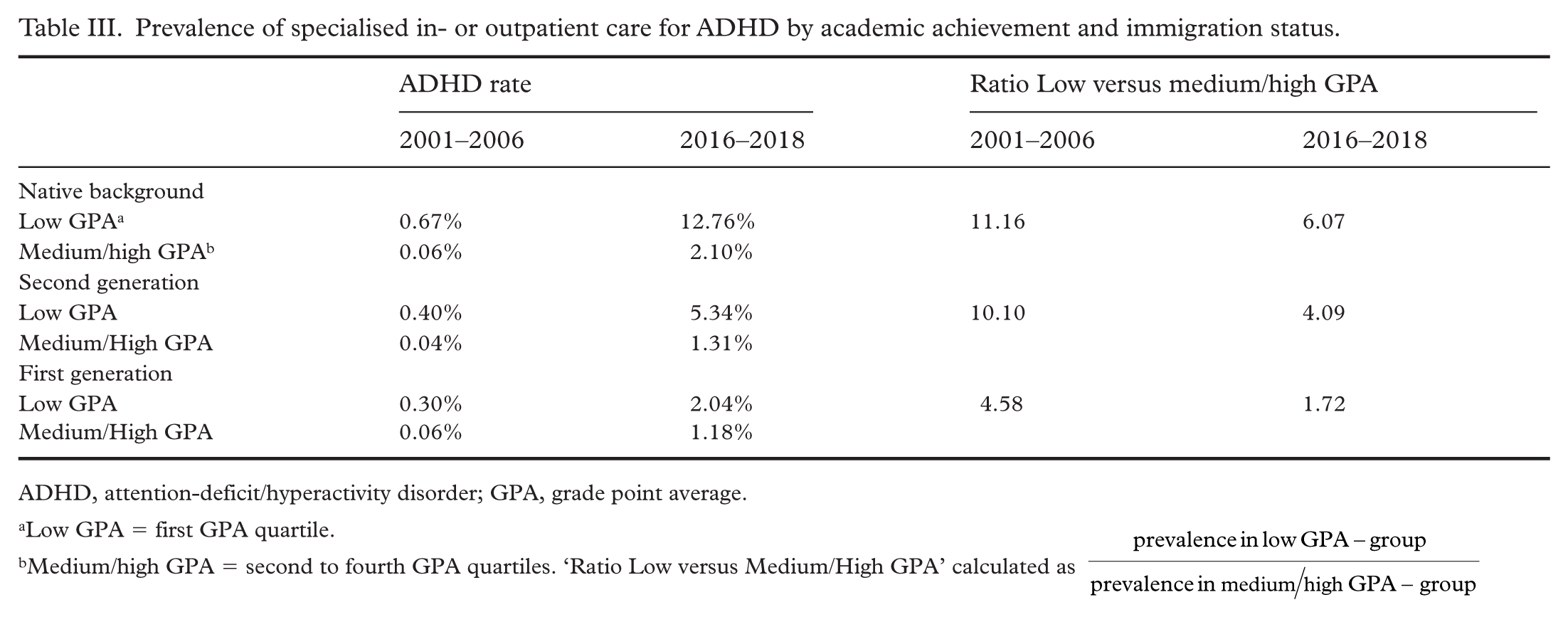
ADHD, attention-deficit/hyperactivity disorder; GPA, grade point average.
Low GPA = first GPA quartile.
Medium/high GPA = second to fourth GPA quartiles. ‘Ratio Low versus Medium/High GPA’ calculated as
Supplemental analyses
Results from supplemental analyses showed that the results were mostly similar when (a) excluding confounders and observations with missing data on parental education (Supplemental File E); (b) using data on pharmacological treatment, available from 2006, to measure ADHD (Supplemental File F); (c) requiring at least two visits when defining ADHD or measuring ADHD over the five years preceding graduation (Supplemental File G) and (d) that there were only minor gender-differences in the time trends (Supplemental File H). Investigation of non-linear time trends showed that most of the reduction of the achievement-gradient occurred after 2009 (Supplemental File I). Linear probability models showed that the achievement-gradient widened over time in absolute terms (Supplemental File J). There were no consistent changes in the achievement-gradient in other types of behavioural and emotional disorders (ICD-10 codes F91–F98; Supplemental File K). Stratification by Western and non-Western background (Supplemental File L) showed that the overall increase in ADHD among low-achieving first-generation immigrants was considerably smaller for those born in non-Western (OR = 1.14, 95% CI [1.12,1.17]) than in Western (OR = 1.23, 95% CI [1.20,1.25]) countries. The interaction terms between GPA and year were also generally larger among non-Western than Western first-generation immigrants, although estimates were imprecise due to small cell sizes in some subgroups. Thus, the disproportionate reduction of the achievement-gradient among first-generation immigrants was driven primarily by those with a non-Western background. This group also constituted a larger share of the immigrant population over the period, from approximately 5% to 11% of all students.
Discussion
Focussing on Swedish compulsory school graduates between 2001 and 2018, this study investigated whether the change in diagnosed ADHD in the year of graduation varied across achievement levels, and whether this in turn differed depending on students’ immigration status. We underscore three key findings. First, in relative terms, the increase in ADHD was greatest among higher-achieving students, resulting in a diminishing achievement-gradient in ADHD over time. Second, ADHD was more prevalent in low-achieving native compared with immigrant (especially first-generation) students, and the achievement-gradient in ADHD was also, on average, steeper among native students. Third, the reduction of the achievement-gradient over time was greatest among immigrant students, resulting in even larger differences in the achievement-gradients between native and especially first-generation immigrant students. This divergence was driven by a very small increase among low-achieving first-generation immigrant students. In fact, of all subgroups investigated, low-achieving first-generation immigrants exhibited by far the smallest, while high-achieving native and second-generation immigrant students exhibited the greatest, relative increase in ADHD.
A diminishing achievement-gradient in ADHD is in line with a recent study using Norwegian register data between 2006 and 2019 [23]. This pattern is, in turn, consistent with diagnostic expansion, driven in part by lower thresholds for diagnosis [8]. Several diagnostic criteria for ADHD refer to academic difficulties, and impairment is assessed in relation to school functioning. Thus, the finding that high-achieving students are increasingly diagnosed indicates that the degree of academic difficulties or impairment required for diagnosis may have become lower, or that the absence of academic difficulties to a lesser degree disqualifies children from diagnosis. This can also be related to a saturation effect: since a greater proportion of low-achieving students were diagnosed in the beginning of the period, there was less room for an increase in this group. Note that lower diagnostic thresholds do not imply overdiagnosis. Thresholds may previously have been too stringent, with more children that benefit from diagnosis and treatment now being detected.
While the pattern is consistent with diagnostic expansion, there are alternative explanations. Higher rates of ADHD among high-achieving students may indicate that treatments are effective in raising achievement [25]. Awareness of ADHD may have increased, prompting more families to seek diagnostic investigation [12]. Socioeconomically strong groups, with higher academic achievement, may disproportionately use the expanding private care market [10]. ADHD diagnoses may increasingly be caused by social rather than academic impairments, with social impairments being associated less strongly with academic achievement. Additionally, while the available evidence suggests that symptoms have not increased over time [5 –8], most of this evidence predates the latter part of the study period, and a genuine rise in ADHD symptoms among higher-achieving students cannot be ruled out.
While previous studies have established a lower prevalence of ADHD among immigrants in Sweden [20], differences in the achievement-gradient between native and immigrant children have not been studied previously. Lower rates among immigrant children overall could be because immigrant children are selected positively in terms of health [26], although the fact that immigrant children do not have lower ADHD symptoms speaks against this [22]. As for the flatter achievement-gradient among immigrants, this may be because schoolwork-related difficulties in these groups are to a greater extent caused by other factors besides ADHD, such as insufficient language skills. Alternatively, low-achieving immigrants may be underdiagnosed relative to native children. Immigrants, particularly with a non-Western background, face greater language barriers and greater challenges in terms of integration into Swedish society. The parents may be less knowledgeable about the Swedish school and healthcare systems, and hence less likely to seek medical treatment for their children’s problems [27]. School difficulties among immigrants may also be more normalised, making parents and teachers less likely to interpret such difficulties as symptoms of ADHD [28]. Our stratified analyses lend some support to these explanations, showing that the patterns observed for first-generation immigrants were primarily driven by those with a non-Western background, among whom the increase in ADHD was smallest and the achievement-gradient flattest. However, these subgroup analyses have limited statistical power and should be regarded as suggestive rather than definitive. The disproportionate flattening of the achievement-gradient among first-generation immigrants over time may further be explained by a growing share of the immigrant population having a non-Western background (see Supplemental File L).
It is noteworthy that we did not find a diminishing achievement-gradient in other types of behavioural and emotional disorders (ICD-10 codes F91–F98), such as conduct disorders. Our results concerning ADHD also contrast with recent Swedish findings showing a growing achievement-gradient in mood- and anxiety disorders [29,30]. Thus, the diminishing achievement-gradient in ADHD appears to be specific to ADHD and not part of a general trend towards smaller achievement-gradients in psychiatric disorders.
It should be noted that the achievement-gradient widened in absolute terms, with the greatest absolute increase observed among low-achieving students. This is expected given the substantially higher baseline prevalence in this group and is important from a public health and service planning perspective. However, relative differences are more informative for evaluating the diagnostic expansion hypothesis, as they better capture shifts in the composition of diagnosed cases.
Limitations
The register data used in the study have limitations. First, non-physician outpatient or primary care visits are not registered, and there may be under-reporting from clinics, especially from private care providers. Second, we measured ADHD only in the same year that the students graduated from school year 9, meaning that students that had been diagnosed earlier but no longer have specialised healthcare contact were not included. Third, we had data on only the primary, not secondary, diagnoses. Fourth, without data on symptoms or impairment, it is not possible to differentiate between a real change in the underlying disorder and changes in diagnostic practices, or to investigate underdiagnosis directly. Fifth, there may be heterogeneity in the immigrant population that we could not capture with the data, for instance, concerning reasons for immigration, ethnicity or trauma exposures. Finally, while the results are consistent with diagnostic expansion, there are alternative explanations that could not be tested with the data at hand.
Conclusions
This study found that, in relative terms, ADHD has increased more among higher-achieving than low-achieving students in Sweden, resulting in a diminishing achievement-gradient in ADHD over time. The trends varied by immigration status: higher-achieving native and second-generation immigrant students displayed the greatest, and low-achieving first-generation immigrants (especially those from non-Western countries) the smallest relative increase in ADHD. The limited increase in this group may indicate persistent barriers to diagnosis and care. Future research should investigate the causes of the diminishing achievement-gradient in ADHD, including diagnostic expansion and changes in underlying symptoms or healthcare-seeking behaviours.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261440445 – Supplemental material for Associations between academic achievement and ADHD in Sweden 2001–2018: differential trends for native and immigrant students
Supplemental material, sj-docx-1-sjp-10.1177_14034948261440445 for Associations between academic achievement and ADHD in Sweden 2001–2018: differential trends for native and immigrant students by Björn Högberg, Mattias Strandh, Karina Nilsson and Solveig Petersen in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Swedish Research Council for Health, Working Life (grant no. 2022-01062). The Umeå SIMSAM Lab data infrastructure used in this study was developed with support from the Swedish Research Council and strategic funds from Umeå University.
Data availability
Data are not available for public use. Please contact Umeå SIMSAM Laboratory for further information on data availability.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.