
Abstract
Background:
During the COVID-19 pandemic in Sweden, individuals could claim compensation for the unpaid waiting day of a sickness absence spell, through a new waiting day reimbursement scheme. The factors associated with claiming this are unknown.
Aim:
To investigate factors associated with claiming the waiting day reimbursement among blue-collar workers in the retail and wholesale industry.
Method:
A prospective cohort study using nationwide linked registers in Sweden. All blue-collar workers in the retail and wholesale industry in 2019 (N = 297,378) were followed March 11 2020–30 September 2021 regarding waiting day reimbursement and sickness absence spells >14 days. Sickness absence spells were matched to waiting day reimbursement based on dates. A logistic general estimating equation model was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) of sickness absence spells having waiting day reimbursement, adjusted for sociodemographic and sickness absence-related factors.
Results:
Fifty per cent of the workers and 57% of all sickness absence spells had waiting day reimbursement. Longer sickness absence spells had lower odds of having waiting day reimbursement, with a gradient depending on spell duration (OR 0.44; CI 0.40–0.48 for spells ≥365 days compared to 15–21 days). Sickness absence spells with COVID-like diagnoses had higher odds of waiting day reimbursement (2.30; 2.12–2.49 compared to musculoskeletal diagnoses). Most differences regarding sociodemographic or work-related variables were non-significant.
Conclusions:
Keywords
Introduction
During the COVID-19 pandemic, several measures were enacted to stop contagion. One of these measures in Sweden was reimbursement for the otherwise uncompensated first waiting day of a sickness absence (SA) spell, to lessen the financial incentives for sickness presenteeism with symptoms of COVID-19 [1]. The waiting day was introduced in 1993 to prevent moral hazard from self-certification, since individuals might either change their behaviour and expose themselves to unnecessary risks knowing that their wage loss due to work absence would be reimbursed, or claim SA benefits without a medical need, since the first days of an SA spell usually do not require a medical certificate. It was hoped that the waiting day, a financial penalty of one day’s wages, would decrease unnecessary SA, although results from studies examining SA patterns following its introduction are equivocal regarding its success [2-4].
Waiting days have sometimes been considered unfair, especially in the context of infectious diseases where persons might have work capacity but be prevented from working to avoid infecting others [5]. During pandemics, this consideration becomes especially important [6], hence, Sweden introduced a flat-rate waiting day reimbursement (WDR).
During the period that WDR was available, 39% of all employees in the retail and wholesale industry had WDR, which was slightly below the average across all industry branches. At the same time, 8% had SA benefits from the Swedish Social Insurance Agency, both in the retail and wholesale industry and across all branches of industry [7]. However, both sales assistants and warehouse workers were among the 10 occupations with the most frequent WDR use [7]. This points to the presence of differences within this industry regarding WDR uptake, which has not been studied before.
According to the Social Insurance Agency, 55% of those who had a new SA spell >14 days when WDR was available used WDR [8]. This indicates a substantial mismatch between benefit eligibility and benefit receipt, whereby many people did not claim the WDR they were entitled to.
Most studies investigating uptake of benefits have focused on the other side of the coin, that is, non-uptake [9-11], since this can threaten the legitimacy of the welfare state and undermine the purpose of the benefits [12-14]. Take-up of benefits is affected by information, stigma, and administrative procedures [14]. There are several reasons why individuals might not receive benefits they are entitled to: they might lack awareness, decide not to claim, or not receive the benefits they claimed [15]. Previous research has shown that low education, being an immigrant, having children at home, and living in a small municipality are associated with a higher likelihood of non-uptake, as are a shorter expected benefit duration and lower expected amounts [12]. With regard to the WDR, whether the same factors are of importance for uptake is unknown. The WDR differs from several other benefits in Sweden, in that it is usually only expected to last for 1 day, and is neither means-tested nor proportional to lost earnings.
The aim of this study was to investigate which factors were associated with using the WDR among blue-collar workers in the retail and wholesale industry.
Methods
A prospective population-based cohort study of blue-collar workers in the retail and wholesale industry in Sweden was conducted, utilising microdata from four administrative registers.
Data and study population
We used pseudonymised linked individual-level data [16] from four nationwide Swedish administrative registers as follows: to obtain annual information on sociodemographic and work-related factors in the years 2018–2021 we utilised the Longitudinal Integration Database for Health Insurance and Labour Market Studies (LISA) register from Statistics Sweden [17]. We used the Microdata for the Analysis of Social Insurance (MiDAS) register from the Swedish Social Insurance Agency to acquire information on SA spells lasting ≥15 days in the period 2018–2021 [18]. We also used information from the Social Insurance Agency on WDR. Finally, we obtained date of death from the Cause of Death Register from the National Board of Health and Welfare [19].
The study population has been used for previous studies on similar topics [20]. It included all individuals aged 18–67 years who 1) were registered as living in Sweden all of 2019 and had an occupational code indicating a blue-collar occupation according to the Swedish Standard for Occupational Classification (SSYK, the Swedish version of the International Classification of Occupations); 2) were employed at a private sector company in 2019 in the retail and wholesale industry, as defined by the Swedish Standard Industrial Classification; and 3) had income from work, parental leave benefits, SA, and/or disability pension (DP) that amounted to at least 8370 Swedish Krona (SEK; approximately 790 EUR) [21]. Those who were self-employed, who died before 12 March 2020, or who had full-time DP during the entire period when WDR benefits were available were excluded. The final cohort included 297,378 individuals in 2019.
Public sickness absence insurance in Sweden
In Sweden, individuals with income from work, parental leave benefits, or unemployment benefits can claim SA benefits if their work capacity is reduced due to morbidity. After a first unpaid waiting day, employers provide sick pay during the subsequent 13 days of an SA spell. Thereafter, individuals receive SA benefits from the Social Insurance Agency. In this study we thus used information on SA spells >14 days. SA benefits cover 80% of lost income, up to a certain level, and can be granted part-time or full-time (i.e., 25%, 50%, 75%, or 100% of ordinary working hours).
In the period 11 March 2020 through 30 September 2021, individuals could claim reimbursement for the waiting day in the form of a flat-rate benefit (varying between 700 and 810 SEK). In the years studied there was no maximum duration of an SA spell.
Variables
The main variable of interest was having had WDR from the Social Insurance Agency, either alone or in conjunction with an SA spell >14 days with SA benefits from the Social Insurance Agency.
Three types of incident SA spells were identified during the period when WDR was available: spells with only WDR, spells >14 days without WDR, and spells >14 days with WDR, based on the starting dates of SA spells.
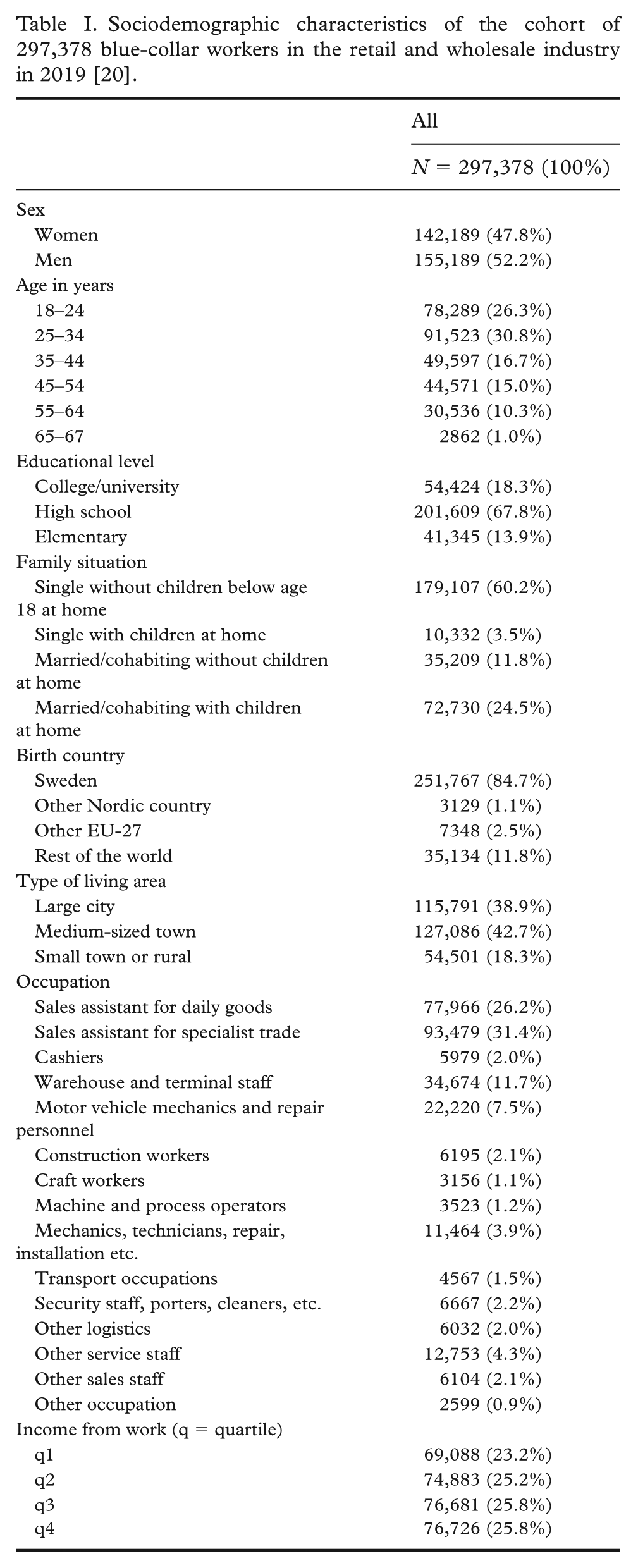
We included the following individual-level factors from 2019 (categorisation shown in Table I): sex, age, country of birth, educational level, family situation, type of living area, income, and occupation based on SSYK. We included the following factors on the SA spell level: number of gross SA days (categorisation shown in Table II); SA diagnosis based on ICD-10 [22] (categorisation shown in Table S1. The categorisation of COVID-like spells was in accordance with how the Social Insurance Agency categorised SA diagnoses related to COVID-19 during and after the pandemic [7]).
Sociodemographic characteristics of the cohort of 297,378 blue-collar workers in the retail and wholesale industry in 2019 [20].
Characteristics (n and column %) of spells with waiting day reimbursement (WDR), sickness absence (SA) spell >14 days without WDR, and SA spell >14 days with WDR, at the SA spell level, for incident SA spells, 11 March 2020 to 30 September 2021.
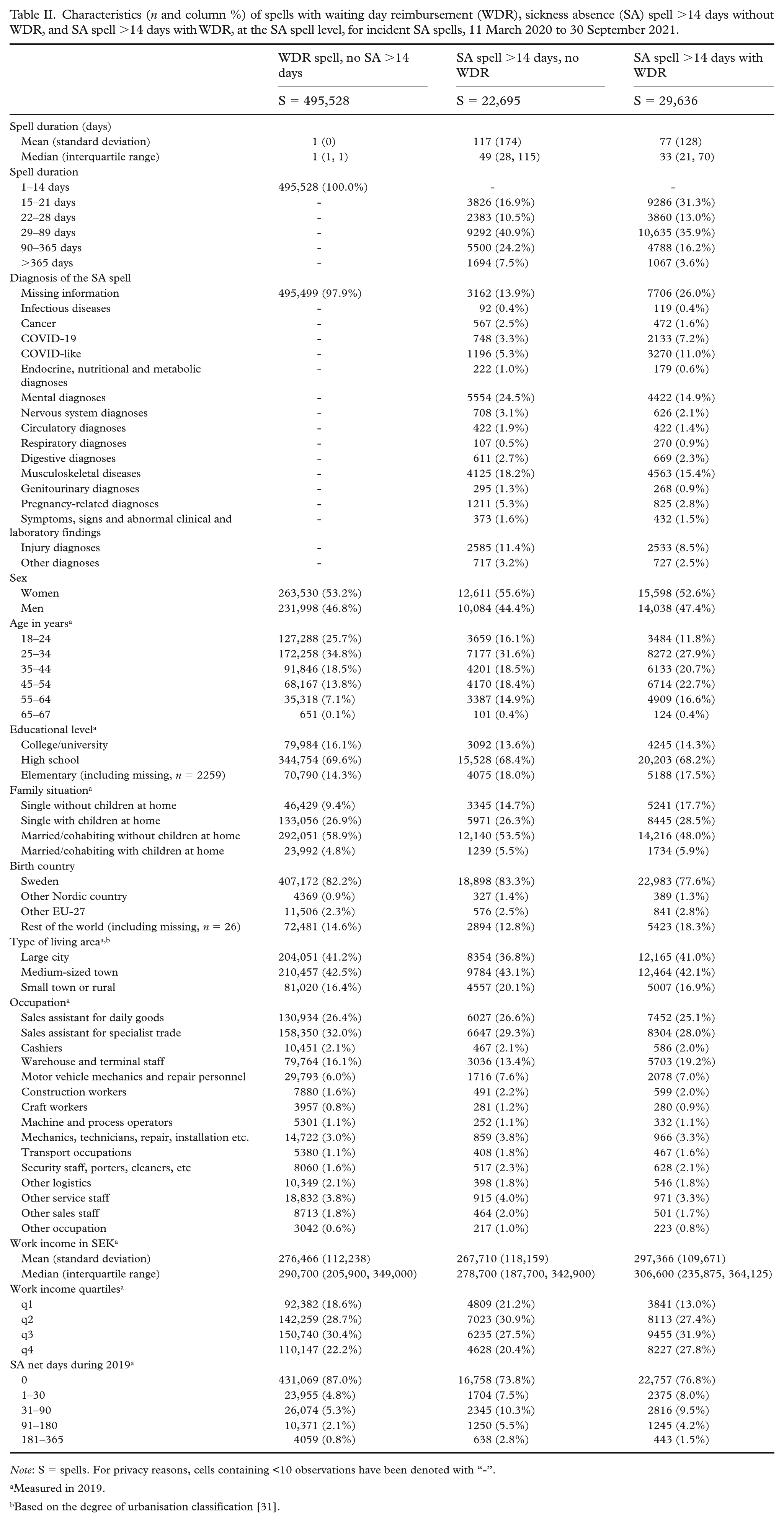
Note: S = spells. For privacy reasons, cells containing <10 observations have been denoted with “-”.
Measured in 2019.
Based on the degree of urbanisation classification [31].
Statistical methods
We calculated the number of incident SA spells with WDR only, SA spells >14 days without WDR, and SA spells >14 days with WDR, respectively, as well as the number of individuals with SA spells of each category (individuals could have more than one SA spell of different categories).
We compared the likelihood of having an SA spell >14 days with and without WDR using a logistic general estimating equation (GEE) model with an exchangeable working correlation structure Edited for sentence flow, which accounts for repeated observations within the same individual [23, 24]. The GEE framework, originally proposed by Liang and Zeger [25], models the marginal mean of the outcome while incorporating within-individual dependence through a working correlation matrix. This approach accounts for the correlation between repeated SA spells contributed by the same individual and provides population-averaged regression coefficients and appropriately adjusted standard errors.
An exchangeable working correlation structure was specified, assuming constant within-individual correlation across SA spells. Alternative working correlation structures (autoregressive and unstructured) were examined, and the exchangeable structure provided the best model fit based on the quasi-likelihood information criterion. Effect estimates were similar across specifications, indicating robustness to the choice of correlation structure.
The model was used to calculate odds ratios (ORs) with 95% confidence intervals (CIs) and probabilities of an SA spell >14 days having WDR. Analyses were first unadjusted (crude estimates), and thereafter adjusted for all included sociodemographic variables shown in Table I and the SA spell-level variables shown in Table II (all variables mutually adjusted).
Results
Table I (also seen in previous studies of this cohort [20]) shows the distribution of sociodemographic factors among the 297,378 blue-collar workers in the retail and wholesale industry in 2019 who were eligible for SA and WDR benefits at some point in 2020–2021. The number of WDR spells followed the COVID-19 waves, with fewer spells in the summer (Figure 1). However, the fluctuations were less noticeable for SA spells without WDR than for spells with WDR, either with or without SA >14 days.
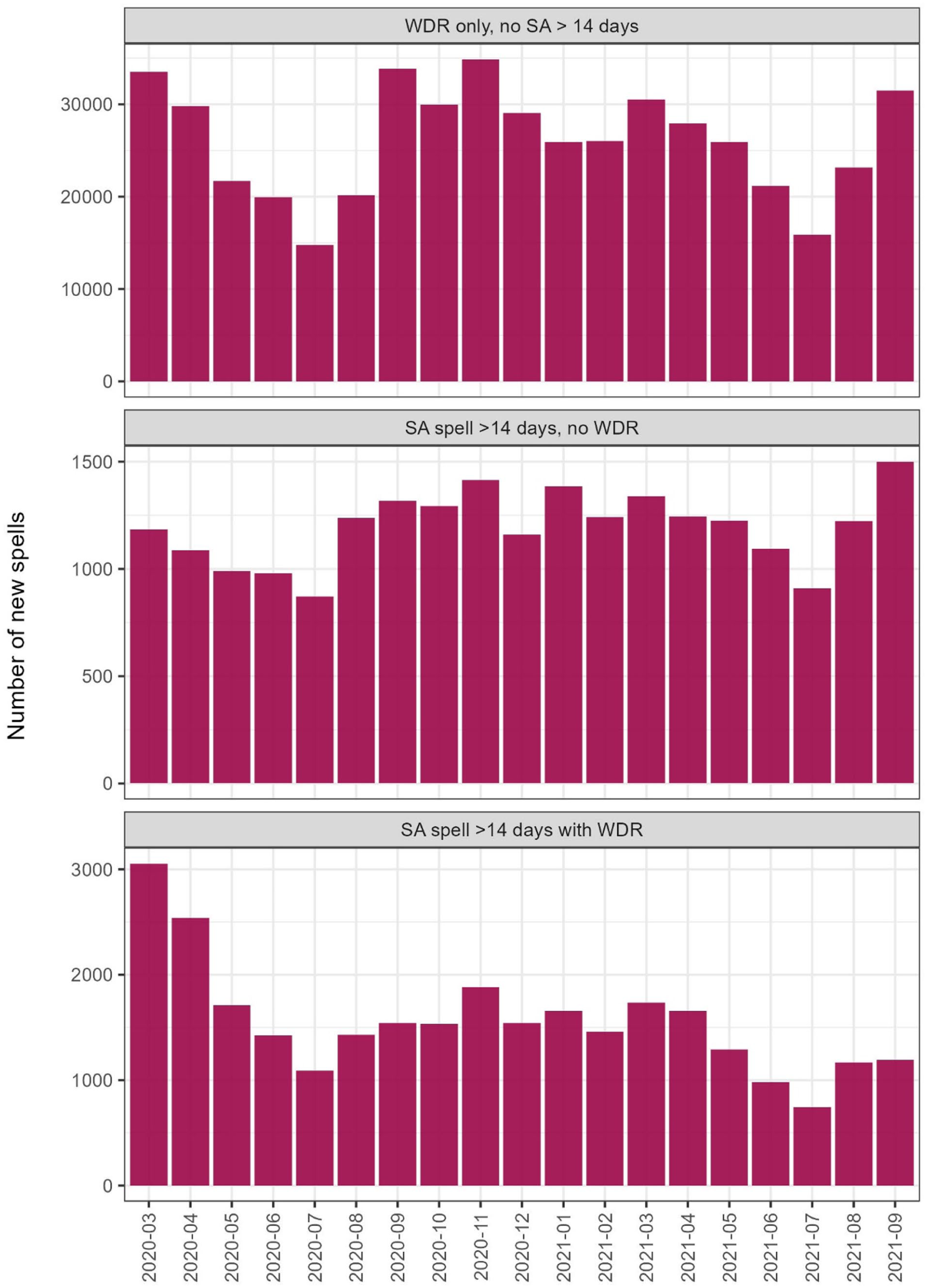
Number of incident SA spells with waiting day reimbursement (WDR) and sickness absence (SA) spells >14 days, with and without WDR, per month during 11 March 2020a to 30 September 2021 (note scale on each y-axis).
Table II shows the duration and diagnosis chapter of the SA spells with only WDR, SA spells >14 days without WDR, and SA spells >14 days with WDR, respectively, as well as the sociodemographic characteristics of the individuals with each type of SA spell. There were far more spells of only WDR than other SA spells. There were 495,528 spells with only WDR from 141,570 individuals, whereas for SA spells without WDR, there were 22,695 spells from 19,918 individuals, and for SA spells with WDR, there were 29,636 spells from 24,884 individuals. A total of 147,392 individuals had WDR, either in conjunction with SA >14 days or on its own (not shown in table). This corresponded to 49.6% of those at risk.
Approximately 57% of all incident SA spells >14 days had a WDR and those SA spells tended to be shorter than SA spells >14 days without WDR.
A slightly higher proportion of those with SA >14 days without WDR were younger. However, those aged 18–34 made up over half of those with only WDR.
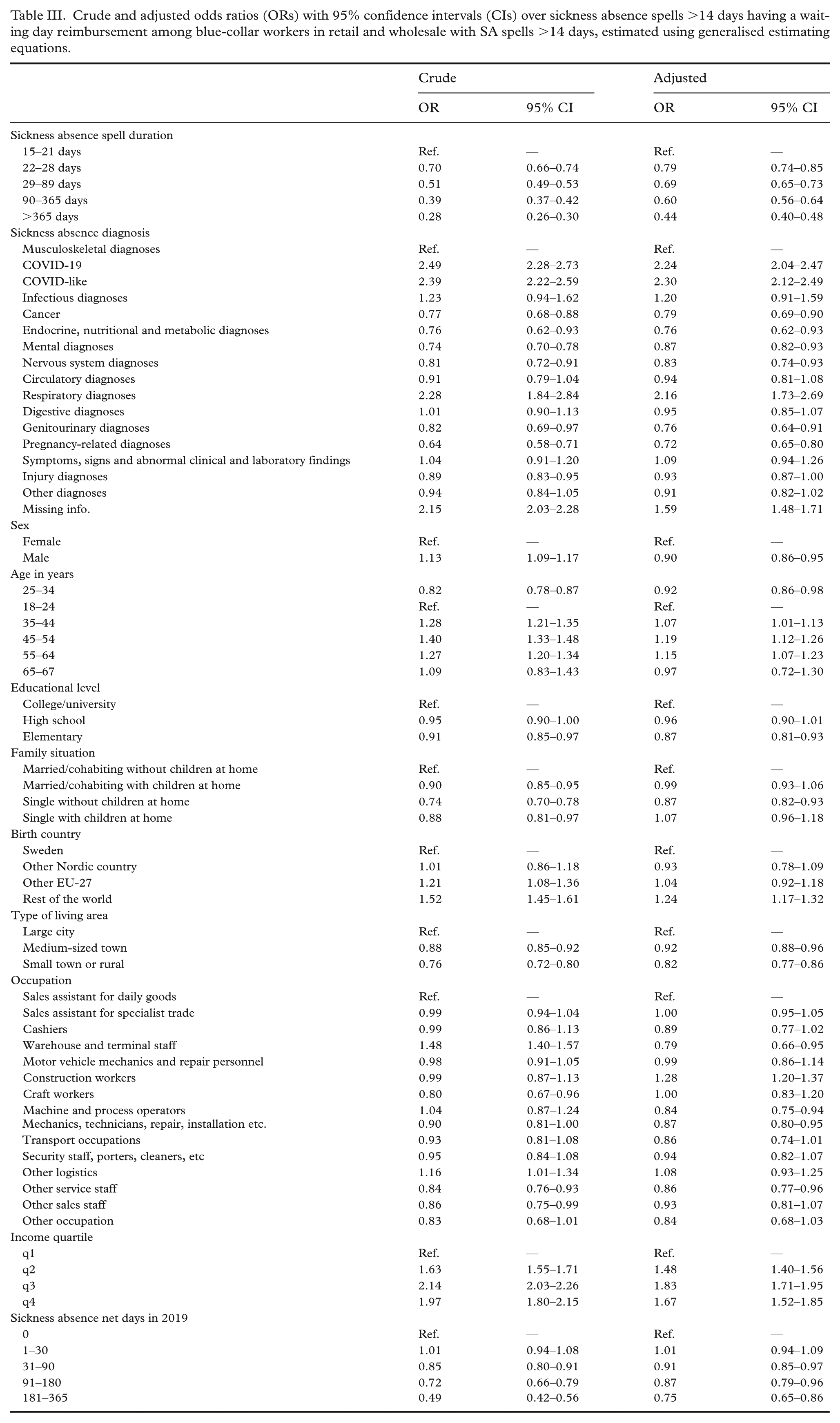
Table III shows the crude and adjusted ORs and 95%CIs over having an SA spell >14 days with WDR as opposed to an SA spell without WDR by sociodemographic-, SA- and work-related factors. SA spells due to COVID-19 (adjusted OR 2.24; 95%CI 2.04–2.47), COVID-like (2.30; 2.12–2.49), or other respiratory diagnoses (2.16; 1.73–2.69) were the most likely to have WDR compared to those with musculoskeletal diagnoses, followed by spells with missing information on diagnosis (OR 1.59; 1.48–1.71), while SA spells due to several other diagnoses had lower ORs (range 0.72–0.83). The longer an SA spell was, the less likely WDR was: spells >365 days had an OR of 0.44 (0.40–0.48) compared to spells lasting 15–21 days. Associations by sociodemographics were generally small or non-significant. Those in the lowest income quartile had the lowest odds of having WDR, (q2–q4 ORs range 1.48–1.83). Figure 2 shows the adjusted probability of an SA spell having WDR from the GEE model for each factor, including for the reference categories, and provides a visual illustration of the relationships described above. The exact numbers for Figure 2 can be found in Supplementary Table 2.
Crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) over sickness absence spells >14 days having a waiting day reimbursement among blue-collar workers in retail and wholesale with SA spells >14 days, estimated using generalised estimating equations.
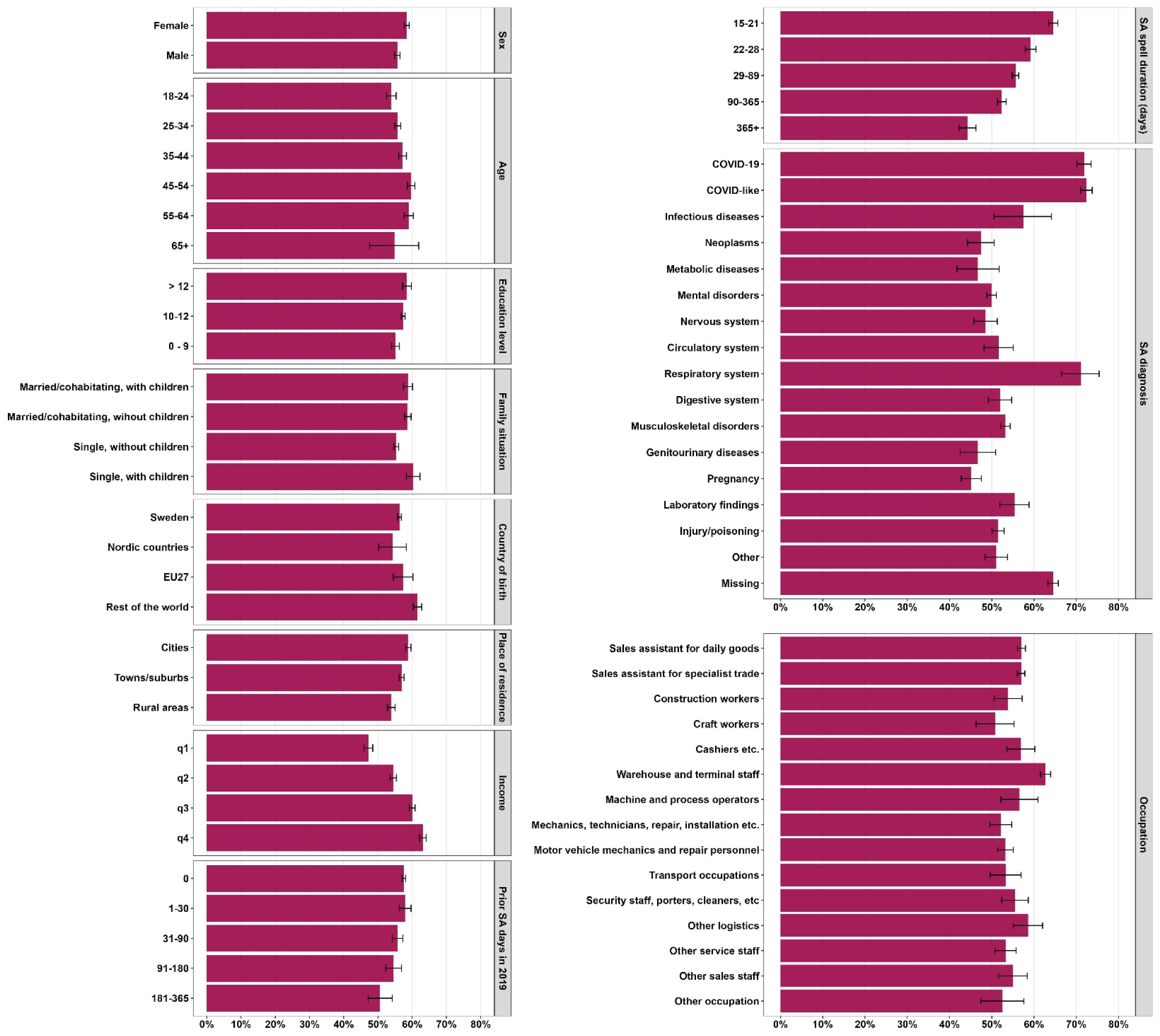
Adjusted probability and 95% confidence interval of an incident sickness absence (SA) spell >14 days having waiting day reimbursement (WDR), 11 March 2020 to 30 September 2021.
Discussion
In this large, prospective cohort study of the use of WDR among blue-collar workers in the retail and wholesale industry during the COVID-19 pandemic, we found that 147,392 individuals (49.6% of those at risk) had used the WDR at some time point. Comparing SA spells >14 days with and without WDR, spells due to COVID-19, COVID-like diagnoses, or other respiratory diagnoses, and shorter SA spells, regardless of diagnosis, were more likely to have WDR. Individuals with higher incomes were more likely to have SA spells with WDR than individuals with lower incomes. Other factors were only weakly, or not at all, associated with claiming WDR.
The Social Insurance Agency reported that 45% of all those employed used the WDR [8], a slightly lower proportion than in our study. One explanation for this might be fewer opportunities to work from home with minor symptoms in this industry. This is in line with results that indicated individuals in occupations that entail contact with patients, customers, or clients used the WDR more than others [8].
In our comparison of incident SA spells with and without WDR, we found that an SA diagnosis of COVID-19, COVID-like diagnosis, or other respiratory diagnoses were most strongly associated with claiming WDR, followed by the category missing information on diagnosis. That the WDR was more likely to be used for these diagnoses might indicate that WDR was seen more as a COVID-related benefit by absentees, healthcare, and employers, who might have been more likely to inform about the possibility to claim WDR for COVID-related absences, even though it was available for all SA diagnoses. The spells with missing information on diagnosis were most likely shorter spells, since a physician’s certificate was not required until day 21 for most of this period: therefore, they most likely did not have contact with healthcare providers for the condition leading to their SA spell. Furthermore, those who had more than 30 days of SA in 2019 were less likely to claim WDR in conjunction with incident SA spells than those without prior SA. Similarly, longer SA spells were less likely to have WDR (with a decreasing gradient by spell duration), even when adjusted for SA diagnosis. One important factor for the duration of an SA spell might be the individual’s own expectation of the duration [26]: it is possible that people valued the WDR differently depending on the expected duration, and that it was valued less when seen as a proportionally smaller part of the expected benefits. Alternatively, individuals with prior SA or who expected a long SA spell duration perhaps did not see themselves as the target group of the WDR, as the stated purpose was to disincentivise going to work with COVID-19 symptoms.
Research on non-uptake of social benefits shows that immigrants, those with lower incomes, low education, and single parents have higher non-uptake rates [12, 14]. When we investigated specifically non-uptake of WDR, a more complicated pattern emerged. For instance, we found an inverse association between income and WDR uptake. These associations were only partly attenuated when adjusting for other sociodemographic and SA-related factors. We also found that the differences by educational level were small and sometimes non-significant, and no significant differences were found regarding family situation.
A study on non-uptake of the collectively agreed additional SA benefits of 10% for individuals on SA spells >90 days in the public sector, found that men, young individuals, individuals with low income, those born outside Europe, living in large cities, with post-secondary education, and with mental SA diagnoses were less likely to claim them [27]. Moreover, in contrast to our study, the likelihood of not claiming benefits decreased with increasing SA duration: this might be explained by that fact that the additional benefit amount that could be claimed increased by every SA day. They also observed that the non-uptake was around 22% overall, lower than our estimated 43%, which might also be explained by the fact that the amount of money can be much higher than for 1 day of WDR.
Our results are thus only partly in line with studies of other benefits, such as social assistance, unemployment benefits, or collectively agreed additional SA benefits. This could be due to the different nature of the WDR benefit. Previous research has found that both the level and duration of benefits are important for claiming [12]: modest benefits are more likely to be deemed not worth applying for [15], furthermore, short-term benefits might be seen as not lasting long enough to be worthwhile [28]. These considerations both apply to WDR, which was a fixed-rate benefit to cover the first day of SA. That longer SA spells were less likely to have WDR supports this interpretation, since WDR then would constitute a smaller part of the expected total benefits.
Both the level of compensation and the duration of the benefits might affect groups differently. The WDR was a flat-rate reimbursement, whereas the waiting day salary deduction was proportional to the income: it should, therefore, theoretically matter more for people with low incomes [7]. However, contrary to expectations, those with higher incomes were more likely to have WDR, both when unadjusted and adjusted for other sociodemographic and socioeconomic factors. This means that existing inequalities may remain entrenched if the groups for whom benefits might make more of a difference are the most likely to miss out. However, it should be remembered that the study cohort is blue-collar workers within retail and wholesale, and that the associations especially regarding occupation might be different had the whole labour market been included. Furthermore, the actual waiting day salary deduction was higher in terms of SEK for people with higher income – and thus their monetary loss for the waiting day was higher, even when claiming WDR for that spell.
Strengths and limitations
The study’s strengths lie in its use of longitudinal data from high-quality registers over the total population of Sweden [17, 29, 30], thus, we have all people fulfilling the inclusion criteria, not a sample, and that there was no non-response or loss to follow-up. Other strengths are that all data were administrative, not self-reports hampered by possible recall bias, and the very large cohort, allowing sub-group analyses.
Limitations included that we had no information about those who had SA spells <15 days who did not claim WDR. This means that we could only study factors associated with non-uptake by comparing those who had SA spells >14 days with and without WDR. It is possible that the factors affecting non-uptake of the benefits differed between SA spells shorter or longer than 2 weeks. People with an ongoing SA spell that started before the possibility of WDR could not claim WDR.
Conclusion
The WDR for the otherwise uncompensated first days of an SA spell was used by a relatively large proportion (49.6%) of all blue-collar workers in the retail and wholesale industry; nevertheless, a large proportion (43.0%) of those with SA spells >14 days, who were known to be eligible for WDR, did not use this benefit. The characteristics of those who were less likely to use this benefit differed from the characteristics previously identified as associated with non-uptake of other benefits, indicating that this benefit differs from others in key ways. For the WDR, SA spell-related factors such as SA diagnosis and spell duration seemed to be more important than the sociodemographic characteristics of claimants.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948261434124 – Supplemental material for Waiting day reimbursement for the first sickness absence day among blue-collar workers in retail and wholesale during the pandemic
Supplemental material, sj-pdf-1-sjp-10.1177_14034948261434124 for Waiting day reimbursement for the first sickness absence day among blue-collar workers in retail and wholesale during the pandemic by Kristin Farrants, Emma Pettersson, Kristina Alexanderson and Lukasz Cybulski in Scandinavian Journal of Public Health
Footnotes
Author contributions
All authors contributed to study design. EP conducted the statistical analysis. KF drafted the first version of the manuscript. All authors revised the manuscript for intellectual content. All authors approved the final submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by AFA Insurance (grant no. 200362). We utilised data from the REWHARD consortium supported by the Swedish Research Council (grant no. 2021-00154).
Ethical approval and consent to participate
The project was approved by the Swedish Ethical Review Authority (Dnr 2021-06441-02) who also waived the need for informed consent. In this type of observational study, based on population-based register data, informed consent is not applicable [![]() ]. All methods were performed in accordance with the relevant guidelines and regulations.
]. All methods were performed in accordance with the relevant guidelines and regulations.
Availability of data and materials
The used data cannot be made publicly available due to privacy regulations. According to the General Data Protection Regulation, the Swedish law SFS 2018:218, the Swedish Data Protection Act, the Swedish Ethical Review Act, and the Public Access to Information and Secrecy Act, these types of sensitive data can only be made available for specific purposes that meet the criteria for access to this type of sensitive and confidential data as determined by a legal review. Contact
Supplemental material
Supplemental material for this article is available online.