
Abstract
Aims:
As maternal distress has many negative consequences both for mothers and for children, support from child and family services could be very effective in preventing maternal distress from escalating into more serious problems, such as mental illness or parental burnout. We studied the longitudinal and cross-sectional effects of the reported unmet need of support to the levels of daytime tiredness, stress, and depressive and anxiety symptoms of mothers with young children.
Methods:
The study uses data from the Child-Sleep birth cohort (2011–2013). Mothers were evaluated at a prenatal measurement point (n=1667) and 8 months (n=1298), 24 months (n=1038), and 5 years (n=722) postpartum using self-report questionnaires. Logistic regression was used to study the association between reported levels of daytime tiredness, stress, and depressive and anxiety symptoms and the reported unmet need of support from child and family services.
Results:
We found that the reported unmet need had both a longitudinal and a cross-sectional association with increased depressive symptoms, stress and daytime tiredness among mothers with young children. Mothers who had reported unmet need at most timepoints had the highest odds of experiencing distress.
Conclusions:
Background
For the past century, western culture has placed a high value on the wellbeing of children and has sought to regulate parenting [1]. In recent decades, pressures related to parenthood appear to have increased in western countries. Parents feel more pressure to supervise and be highly involved in their children’s lives while struggling to set realistic boundaries in child rearing [2]. The increased demands of parenthood seem to affect parental wellbeing negatively and might increase mental health symptoms such as depressive symptoms [3,4].
Many European and North American studies find that mothers in particular are at risk of experiencing distress in the parenting role [5,6]. Mothers might experience more societal pressure associated with parenthood than fathers [7], and feel pressure to engage in time-consuming and demanding parenting styles [8]. Possibly because mothers are still primary caregivers in many families, having children seems to have a stronger effect on mothers’ than father’s experience of time pressure [9], and mothers report less happiness and more stress in relation to time spent with children than fathers [10].
Maternal psychosocial distress – defined here broadly as mental health symptoms, fatigue and stress – can have many negative effects both on mothers and their children. Maternal stress can increase the likelihood of maternal depression [11,12] and anxiety [13]. Additionally, maternal mental health symptoms are associated with children’s emotional and behavioural problems and lower social competence [14,15]. Intervening in maternal distress is therefore important not just for the sake of the mothers but also for the wellbeing of their children.
A strong social support network is an important protective factor against maternal distress [5,16]. Yet social support is not always available. In such instances, external support from society, such as child and family services, might be particularly important: support and early intervention might prevent maternal distress from escalating into mental illness or parental burnout [5].
In Finland, central common child and family services include maternity and child health clinics, daycare, and school healthcare. Targeted services for families with additional needs include home visits, early daycare support, family work, and counseling. Many families also participate in activities that support everyday life, such as clubs and cultural and sport activities [17].
In general, support received from society seems to increase parental happiness [18]. Many of the existing studies have, however, focused on families with children with special needs [19]. In Finland, mothers are generally satisfied with maternity services [20], although unmet needs for family services have also been reported [21]. One Finnish study has examined parents’ experience of societal support sufficiency and worries related to parenthood among the general population [17]. They found that parents with the most worries also experienced the most needs as well as the most unmet needs. However, to our knowledge, the association of maternal distress and reported unmet needs from family services has not been studied before.
Aims
Our aim is to study the longitudinal and cross-sectional associations between the reported unmet need of support and the levels of daytime tiredness, stress, and depressive and anxiety symptoms, which we refer to as psychosocial distress, of mothers with young children. In addition, we will examine the association between the cumulative unmet need of support at multiple timepoints and the level of psychosocial distress.
Methods
This study uses data from a longitudinal CHILD-SLEEP birth cohort, a large study on children’s sleep development and health, which has been approved by Pirkanmaa Hospital District Ethical Committee (9.3.2011, ethical research permission code R11032). Written informed consent was obtained from all the participants.
The sample
The families were recruited in Pirkanmaa Hospital District between April 2011 and December 2012. Recruitment, aimed to occur at the 32nd gestational week, was done by nurses in health centres during normal follow-up visits to maternity clinics. Infants who were born alive between April 2011 and February 2013 in the Tampere University Hospital were considered eligible for the study. The study design is described in detail in Paavonen et al. [22].
Out of all eligible families, a total of 2244 parents (approximately 29% of the target population) agreed to participate and received the prenatal baseline questionnaires. Of those, 1667 mothers returned the prenatal questionnaire. Mothers were evaluated again at 8 months (n=1298), 24 months (n=1038), and 5 years (n=722) postpartum using self-report questionnaires. Eight of the mothers had twins.
Outcomes
Depressive symptoms were measured using the 10-item version of the Center for Epidemiological Studies Depression Scale (CES-D) [23]. Sample items include ‘I felt depressed’ and ‘I felt that everything I did was an effort’. The participants were asked to rate each item based on how they have felt during the preceding month. All items are rated from 0 (rarely or none of the time (less than 1 day)) to 3 (most or all of the time (5–7 days)). Two of the items were reverse coded. The total score is calculated as a sum of all items (scale range 0–30). Higher scores indicate higher depressive symptoms. A maximum of three missing items was allowed in the sum score, replaced by the mean of the respondent’s available responses.
Anxiety symptoms were measured using a six-item anxiety questionnaire derived from the State-Trait Anxiety Inventory (STAI) trait anxiety scale [24]. Sample items include ‘I feel nervous and restless’ and ‘I worry too much over something that really doesn’t matter’. The participants were asked to rate each item based on how they have felt during the preceding month. All items are rated from 1 (almost never) to 4 (almost always). The total score is calculated as a sum of all items (scale range 6–24). Higher scores indicate greater anxiety symptoms. A maximum of two missing items was allowed in the sum score, replaced by the mean of the respondent’s available responses.
Stress was measured using a 5-item short version of the Perceived Stress Scale [25], which measures how unpredictable, uncontrollable and overloaded the participants find their lives. Sample items include ‘How often have you felt that you were unable to control the important things in your life?’ and ‘How often have you felt confident about your ability to handle your personal problems?’. The participants were asked to rate each item based on how they have felt during the preceding month. All items are rated from 0 (never) to 4 (very often). Two of the items were reverse coded. The total score is calculated as a sum of all the items (scale range 0–20). A maximum of one missing item was allowed in the sum score, replaced by the mean of the respondent’s available responses.
Depressive symptoms, anxiety symptoms and stress were all dichotomised at the 90th percentile at the prenatal measurement point to represent an increased level of symptoms (e.g. for anxiety symptoms, 10% with the highest scores on STAI at the prenatal measurement point were categorised as having increased anxiety, and in future measurement points the same cut-off score was used to indicate increased anxiety. The cut-off points were 10 or more, 12 or more and 11 or more points for increased depressive symptoms, anxiety symptoms, and stress, respectively). We have used dataset specific cut-off points to allow better the comparison of symptom levels among our sample.
Daytime tiredness was measured with the item: Do you consider yourself more tired than other people during the daytime?, with response options (1) yes, almost always, (2) yes, often, (3) no, and (4) do not know (250 (19%), 158 (15%), and 133 (19%) responded ‘do not know’ at 8 months, 24 months and 5 years, respectively). It was dichotomised into categories: yes (options 1 and 2) and no/do not know (options 3 and 4).
Child and family services
The use and unmet need of child and family services was surveyed with the following questions: How much support has your family received from the following services related to baby care and everyday life? (1) maternity care, (2) day care, (3) home services, (4) family work, and (5) other supportive services, with the answer options (a) not at all, (b) quite a little, (c) some, (d) quite a lot, and (e) very much, and Has the support you have received from society services been sufficient? (1) completely insufficient, (2) somewhat insufficient, (3) somewhat sufficient, and (4) sufficient. The latter was dichotomised into sufficient (options 3 and 4) and insufficient (options 1 and 2). Mothers reporting support being insufficient were considered to have an unmet need of support. To study the association between the unmet need of support across timepoints, a variable was created to assess the number of timepoints mothers had perceived support being insufficient, with the following categories: (1) sufficient at all timepoints, (2) insufficient at one timepoint, and (3) insufficient at least at two timepoints.
Covariates
Information on mother’s age and education were retrieved from the prenatal questionnaire. Education was categorised into three categories: (1) no education/courses, (2) vocational school/university of applied sciences, and (3) university. Information on the number of children and number of adults in the household was retrieved separately from the prenatal questionnaire and the questionnaires on child’s ages at 24 months and 5 years. As there were very few immigrants and underlying health conditions in the sample, we have not included these variables as covariates (see Supplemental Table I).
Statistical methods
Cross-sectional associations between the reported unmet need of support and the level of depressive and anxiety symptoms, stress and tiredness were studied using logistic regression. Separate models were run with data on child’s ages at 8 months, 24 months, and 5 years. Longitudinal analyses were run to study the associations of outcomes at later timepoints with unmet need at earlier timepoints using logistic regression. Logistic regression was also used to study the association between outcome variables at the child’s age at 5 years and the number of timepoints mothers had found support insufficient.
All observations with missing data on any of the variables were dropped from the models. All models were adjusted with mother’s age, education, number of children and number of adults in the household. For longitudinal analyses, also baseline adjusted (adjusted with the outcome measure at the baseline level in addition to other covariates) estimates were produced. Information on mother’s age and mother’s education was retrieved from the prenatal measurement point. Information on the number of children and the number of adults was retrieved from the same timepoint as the main independent variable. All the unadjusted estimates are available in the supplemental material (see Supplemental Tables II–IV).
As supplemental analyses we compared the reported service use of mothers who differed in their unmet need of support across timepoints using chi-squared tests (see Supplemental Table V). We also examined the association of dropout with the variables of interest (see Supplemental Table VI). As a sensitivity analysis multiple imputation was used to control for the effect of dropout using the R package mice [26], and the main analyses (longitudinal models) were replicated using the imputed data. All variables included in the original models were used in the imputation model. The number of imputed datasets was set to n=30 to reflect the proportion of missing data. The results using imputed data are presented in Supplemental Table VII.
All analyses were performed using R Statistical Software [27].
Results
The descriptive statistics are presented in Table I. The mean age of the women at the prenatal measurement point was 30.7 years. Over half of the women had the highest education of either vocational school or university of applied sciences. At the prenatal measurement point, most women had either no children (43.6%) or one child (32.6%). By the time of the child’s age at 5 years, most women had either two children (56.9%) or three or more children (29.2%). At the prenatal measurement point, only 1.9% of the women were the only adult in the household, but this figure steadily increased with time, and by the time of the child’s age at 5 years, 7.3% of the mothers were the only adult in the household. Except for daytime tiredness, which was highest at the child’s age at 8 months, all the other reported symptoms increased with time.
Descriptive statistics.
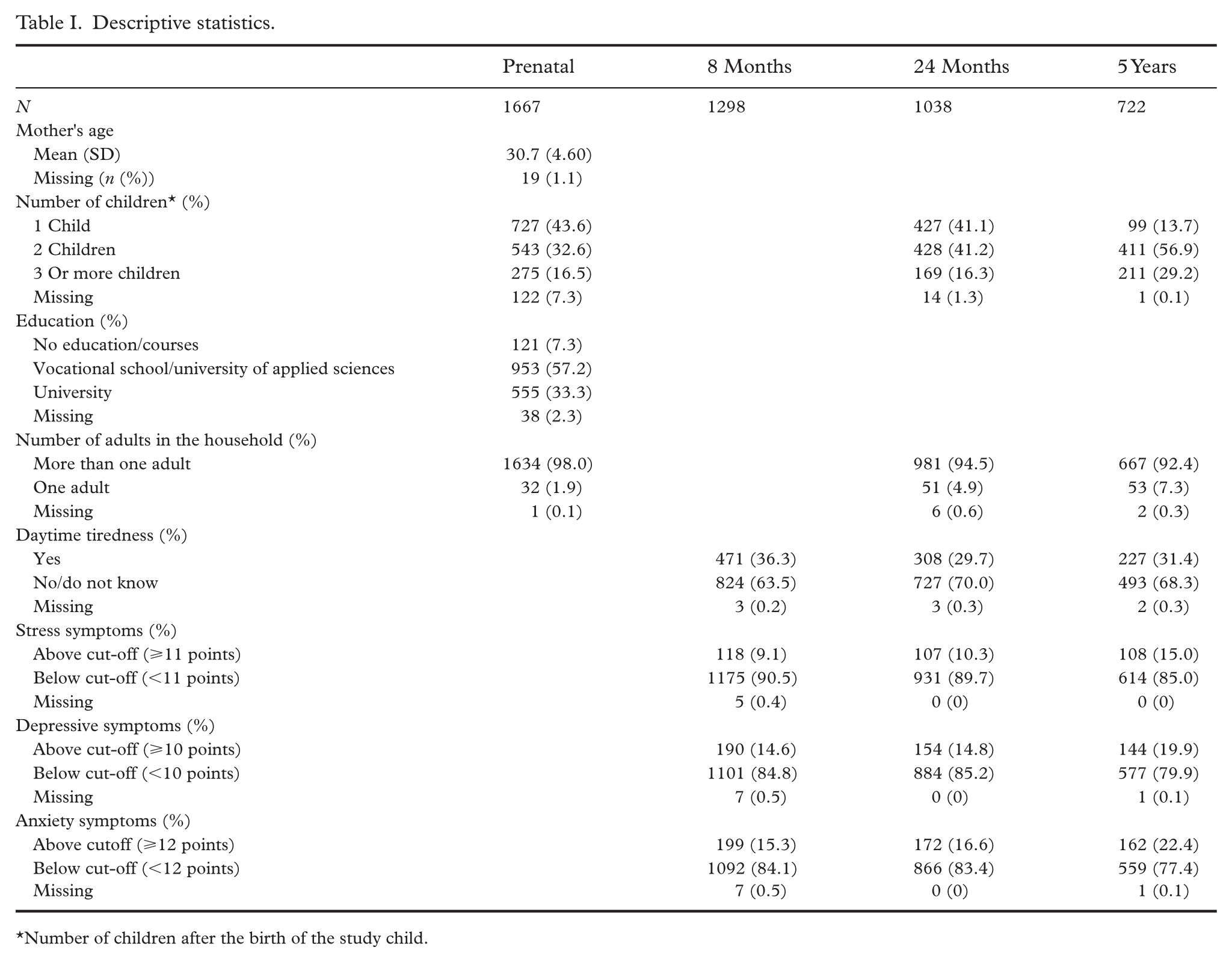
Number of children after the birth of the study child.
The distribution of reported sufficiency of support across timepoints is shown in Figure 1. At all timepoints, over half of the women found support completely sufficient, and about third of the women found support somewhat sufficient. At the child’s age at 8 months, around 10% of the women found support somewhat or completely insufficient, and this figure slightly decreased with time. Out of those who had provided responses at all three measurement points, most women found support completely or somewhat sufficient at all timepoints (81.2%).
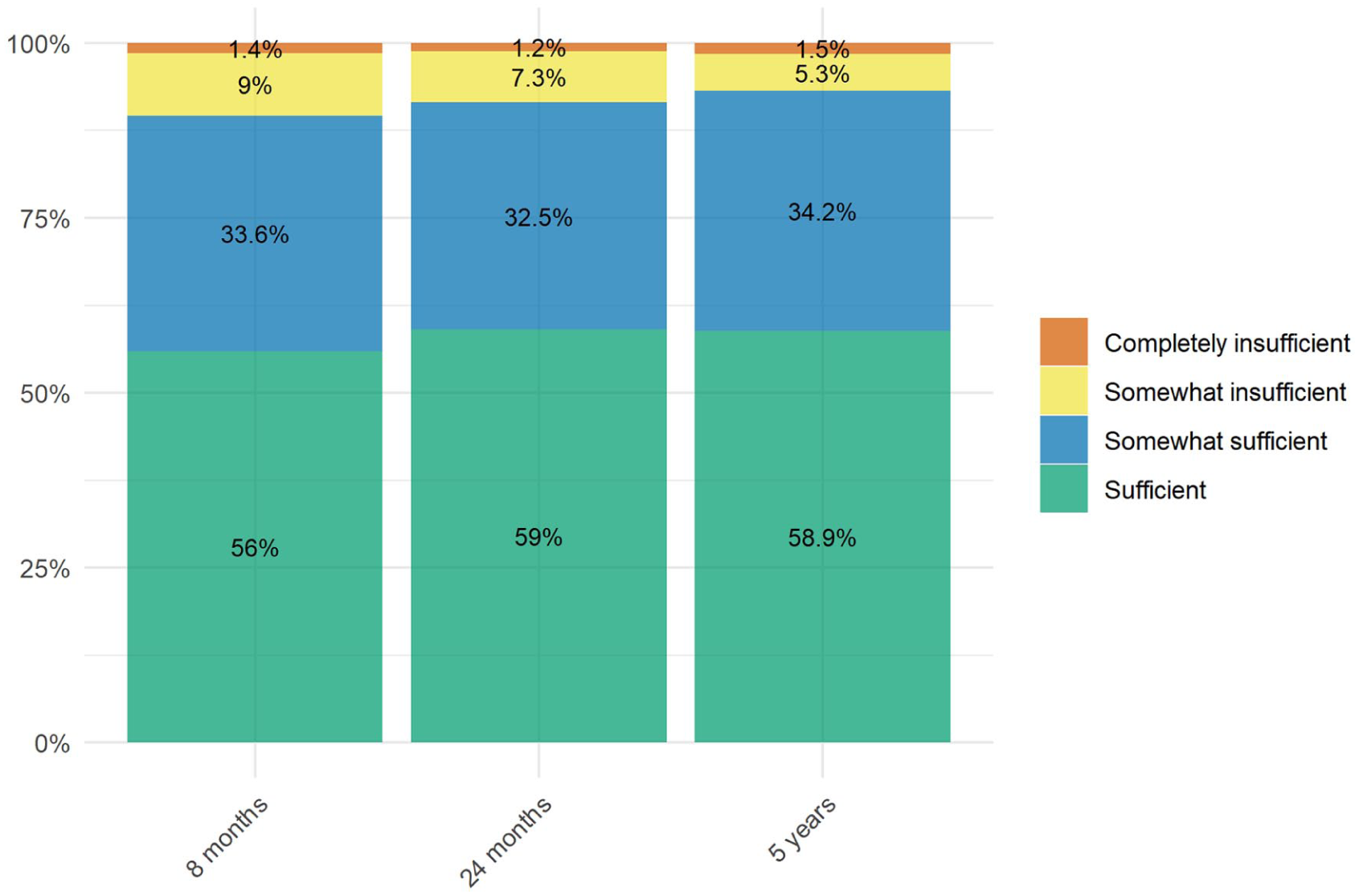
Perceived sufficiency of support among mothers across timepoints.
In the cross-sectional analyses (Table II), we found that the unmet need of support was significantly associated with all the outcomes of interest at all timepoints except of stress at the child’s age at 5 years. Table III shows the results of the longitudinal analyses. In the adjusted models, we found significant associations with daytime tiredness, stress and depressive symptoms and unmet need of support at several timepoints, although not all of these associations remained significant after adjusting for baseline symptoms. In the baseline adjusted models, the association between stress at 5 years and 8 months unmet need of support remained significant (odds ratio (OR) 2.04, 95% confidence interval (CI) 1.03–3.87), similarly to the association between daytime tiredness (OR 1.97, 95% CI 1.00–3.92) and depressive symptoms (OR 3.66, 95% CI 1.79–7.40) at 5 years and unmet need of support at 24 months. The results with the imputed data remained very similar (see Supplemental Table VII).
Cross-sectional analyses: daytime tiredness, stress and depressive and anxiety symptoms predicted by the unmet need of support at different timepoints.
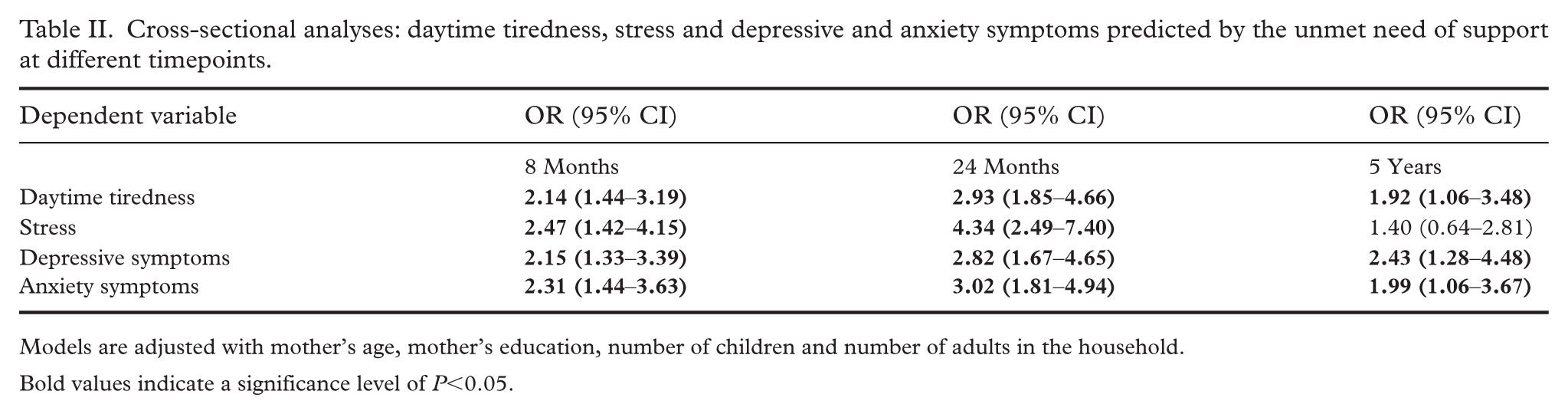
Models are adjusted with mother’s age, mother’s education, number of children and number of adults in the household.
Bold values indicate a significance level of P<0.05.
Daytime tiredness, stress and depressive and anxiety symptoms as predicted by the perceived sufficiency of support at earlier timepoints.
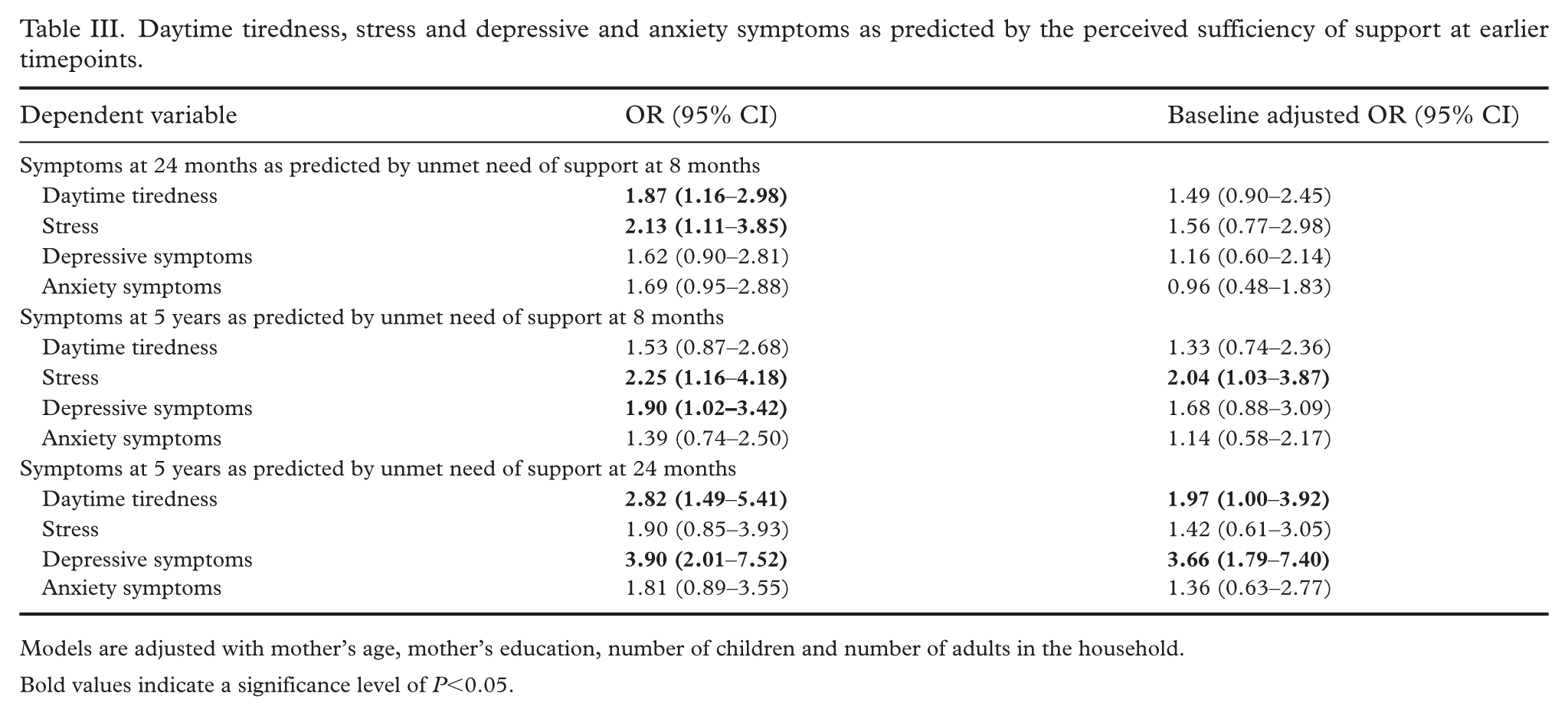
Models are adjusted with mother’s age, mother’s education, number of children and number of adults in the household.
Bold values indicate a significance level of P<0.05.
The results of the models studying associations between outcomes of interest at the child’s age at 5 years and the number of timepoints support was found insufficient are presented in Table IV. The unmet need of support at one timepoint was significantly associated with daytime tiredness (OR 2.03, 95% CI 1.22–3.35) and depressive symptoms (OR 2.22, 95% CI 1.24–3.88) and the unmet need of support on at least two timepoints was significantly associated with daytime tiredness (OR 3.43, 95% CI 1.42–8.66) and depressive symptoms (OR 4.96, 95% CI 2.00–12.26).
Symptoms at 5-year timepoint as predicted by the number of timepoints mothers found support insufficient.
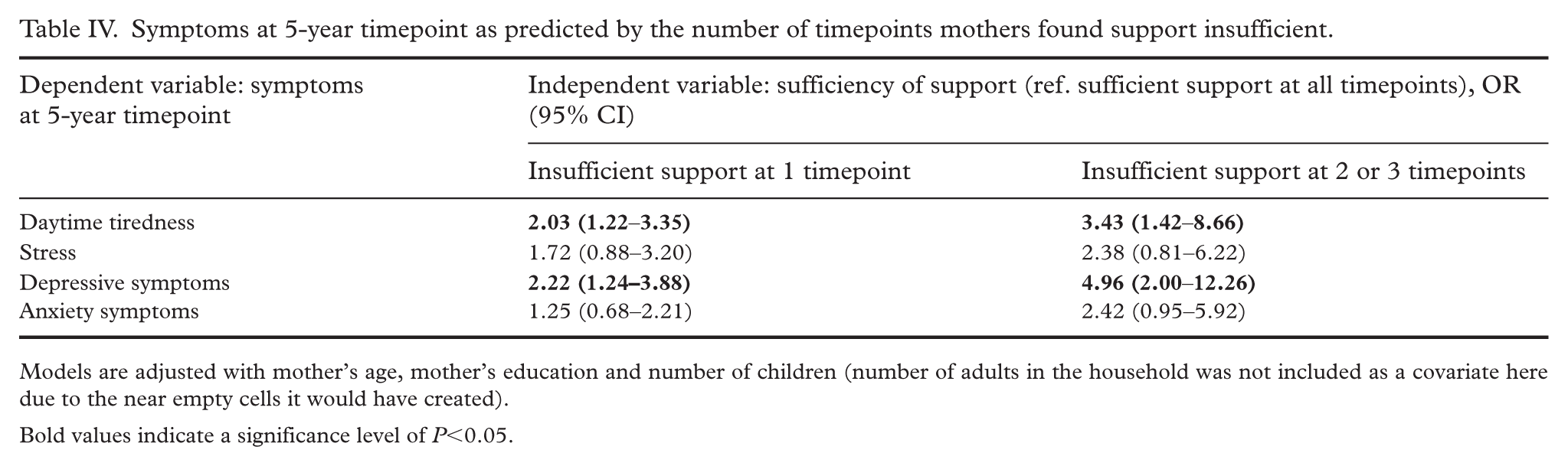
Models are adjusted with mother’s age, mother’s education and number of children (number of adults in the household was not included as a covariate here due to the near empty cells it would have created).
Bold values indicate a significance level of P<0.05.
Discussion
The main finding of the study was that unmet need of support at earlier timepoints was associated with symptoms of psychosocial distress at later timepoints. Even accounting for baseline symptoms, the unmet need of support was significantly associated with increased stress, depressive symptoms and daytime tiredness. In addition, mothers who considered support insufficient at most timepoints had the highest odds of experiencing distress.
Thus, our study demonstrates a clear association between the unmet need of support and maternal distress. As our study could not control for the service type, it is difficult to draw clear conclusions over the exact background mechanisms. An earlier study on the service experiences of Finnish families found that while most parents considered support from services sufficient, there were also experiences of insufficiency, particularly regarding the availability of targeted services, such as child upbringing and family counseling clinics [17], and parents with more worries related to parenthood or their children experienced the support from services as less sufficient [17].
In line with this, we found that mothers who reported unmet need had more often used targeted family services (see Supplemental Table V). Families using these services likely have special needs, suggesting that while the availability of general services may be good, those with the highest needs might experience the support as particularly insufficient, leading to the accumulation of distress.
Most mothers were satisfied with the support they had received: at all timepoints, nearly 90% of the mothers considered support sufficient or somewhat sufficient. There were no major changes in unmet need across timepoints, although the percentage of those considering services sufficient did slightly increase over time. However, symptoms of depression, anxiety, and stress increased with time – particularly between the child’s age at 24 months and the child’s age at 5 years – a worrying finding, as parental distress can negatively impact children [15,28].
Our results indicate that support received from society services might be important in preventing and intervening in maternal distress, and highlight that investing in maternal services, and possibly parental services in general, might have significant public health benefits. While more research is needed to identify the exact patterns causing unmet needs, our results give some indications of these patterns.
Almost all mothers had used maternity clinic services and most also considered the support they received sufficient. Mothers who had used fewer of these foundational services, however, found support more often to be insufficient. This suggests that maternity clinics are the strength of the Finnish service system, which is worth of investing in also in the future. In contrast, mothers who had used more of the targeted services reported overall more unmet needs, which indicates that the services for those with the highest needs might require strengthening.
There are several limitations associated with this study. Without knowing which services mothers found insufficient, we cannot draw further conclusions over the exact unmet needs of the mothers. We did not control for the children’s characteristics, which affect parental stress and service needs. Additionally, the association between the unmet need of support and psychosocial distress might be bidirectional: mothers who experience most distress might perceive the services more insufficient. Furthermore, there was some dropout during the follow-up. However, when dropout was accounted for using multiple imputation, the main results remained significant.
Future research should explore the type of support the mothers experience as inadequate, and how that relates to the distress they experienced. Also, examining children’s characteristics in relation to the unmet need of support and mothers’ distress could provide further insight into the underlying mechanisms. Other important directions could be studying the association of psychosocial distress and the perceived sufficiency of services among fathers, and how the unmet need of support relates to children’s psychosocial development.
Conclusions
We found that the unmet need of support had a longitudinal association with increased depressive symptoms, stress and daytime tiredness among mothers with young children. As parental distress has negative consequences for both parents and the children, and as mothers are at particular risk of distress, preventing and intervening in maternal distress has important implications for population health. While our study made the positive finding that most mothers considered services to be sufficient, there was also a clear association between the unmet need for support and maternal distress. This points towards the importance of the external support society can provide for families with small children.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261431891 – Supplemental material for Maternal wellbeing and perceived sufficiency of support from child and family services: a longitudinal study
Supplemental material, sj-docx-1-sjp-10.1177_14034948261431891 for Maternal wellbeing and perceived sufficiency of support from child and family services: a longitudinal study by Valentina J. Kieseppä, Olli H. Kiviruusu, Anneli Kylliäinen, Riitta H. Vornanen and E. Juulia Paavonen in Scandinavian Journal of Public Health
Footnotes
Author contributions
Authors VK, JP and OK designed the study. Author VK managed the statistical analyses and literature searches and wrote the first draft of the manuscript. All authors have contributed to and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Academy of Finland (#308588 and #342747 to JP), the Signe and Ane Gyllenberg foundation, the Yrjö Jahnsson Foundation, and the Foundation for Pediatric Research.
Supplemental material
Supplemental material for this article is available online.