
Abstract
Aims:
The existing literature lacks sufficient evidence concerning the role of personality traits in oral behaviour and their effects on oral health status (dental plaque, and dental caries) and dental visits. The aim of this study was to investigate the association between personality traits and oral health behaviour (OHB) in the adult Finnish population.
Methods:
This study utilised data collected from the Northern Finland Birth Cohort 1986 individuals who participated in all the follow-ups (n = 1807). Data were collected during pregnancy and later during follow-ups conducted at 1 year, 7–8 years, 15–16 years and 33–35 years using questionnaires and clinical examinations. Oral health status and number of dental visits collected in the last follow-up were considered as dependent variables. The explanatory variables included personality traits, educational background, employment, annual income, and lifestyle choices. A recursive bivariate probit model was used to model oral health status (dental plaque, and dental caries) while considering dental care utilisation.
Results:
Personality traits were associated with OHB (accumulation of dental plaque and regular dental visits). Individuals with a high degree of openness had a 13% lower probability of having teeth with dental caries. Similarly, highly neurotic individuals had a 5% lower probability of having teeth with visible dental plaque and also had a higher probability of dental visiting.
Conclusions:
Background
The link between oral health and various individual socioeconomic and family background factors has been well established in numerous studies [1,2]. However, a noteworthy yet scarcely explored area is the role of personality traits in shaping oral health behaviour (OHB). It is well known that dental plaque is primarily attributed to behavioural factors stemming from specific lifestyle choices. Dental plaque (biofilm) is a diverse community of microorganisms adhering to tooth surfaces. Generally, microorganisms in dental plaque are in a stable homeostatic state. However, changes in the oral environment can influence the microbial composition, thereby creating a dysbiotic environment that increases the risk of developing dental caries and/or periodontal diseases [3]. Changes in the oral environment are directly related to lifestyle factors, which are further associated with socioeconomic factors [4,5]. There is evidence showing strong correlations between oral diseases and various socioeconomic and behavioural factors [6,7]. Furthermore, studies have shown that sociobehavioural factors also predict dental care visits [8,9], and that inadequate use or the absence of dental care is related to poor oral health outcomes [10].
Most of the earlier studies that explored the relationship between personality and oral health have relied mainly on subjective outcome measures (i.e. self-reported oral health) [11,12]. In one notable exception, a study from New Zealand that included both self-reported oral health and clinical status concluded that those with negative emotionality had a greater risk of having dental caries and further consequences [13]. The existing body of evidence exploring the impact of personality on health indicates various pathways through which this relationship influences individuals. These include health-related behaviours, longevity, and social relationships [14]. Thomson and colleagues have suggested that (i) a direct predisposition, (ii) oral health-related behaviours, and (iii) symptoms interpretation are possible pathways through which personality traits can influence oral health [13].
Notably, numerous studies from the fields of psychology and health sciences have consistently shown that certain personality traits, such as conscientiousness, openness to experience, and agreeableness, generally have positive effects on both longevity and health behaviours [15 -18]. Nevertheless, to understand the role of personality traits in oral behaviour and their effects on dental outcomes and visits requires further investigation. Accordingly, the aim of this study was to investigate the association between personality traits and OHBs. The study hypothesis was ‘individuals with a higher level of openness have fewer teeth with dental plaque and dental caries and attend dental visits more regularly’.
Methods
Study participants
The Northern Finland Birth Cohort 1986 (NFBC1986) is a population-based birth cohort study conducted in the two northernmost provinces of Finland (Oulu and Lapland). The NFBC1986 includes all mothers (n = 9362) and their children whose expected dates of birth were between 1 July 1985 and 30 June 1986. A total of 9432 live-born children were included in the cohort. Using questionnaires and clinical examinations, data were collected during pregnancy and later during follow-ups conducted at 1 year, 7–8 years, 15–16 years and 33–35 years. All the cohort members living within a radius of 250 km from the centre of Oulu city were invited for clinical examination, including oral examinations, at the age of 33–35 years. Thus, this study utilised data collected from a sub-cohort of NFBC1986 individuals who participated in all the follow-ups (n = 1807) (Figure 1) [19,20]. Details of the NFBC1986 data collection are provided in Supplementary file S1.
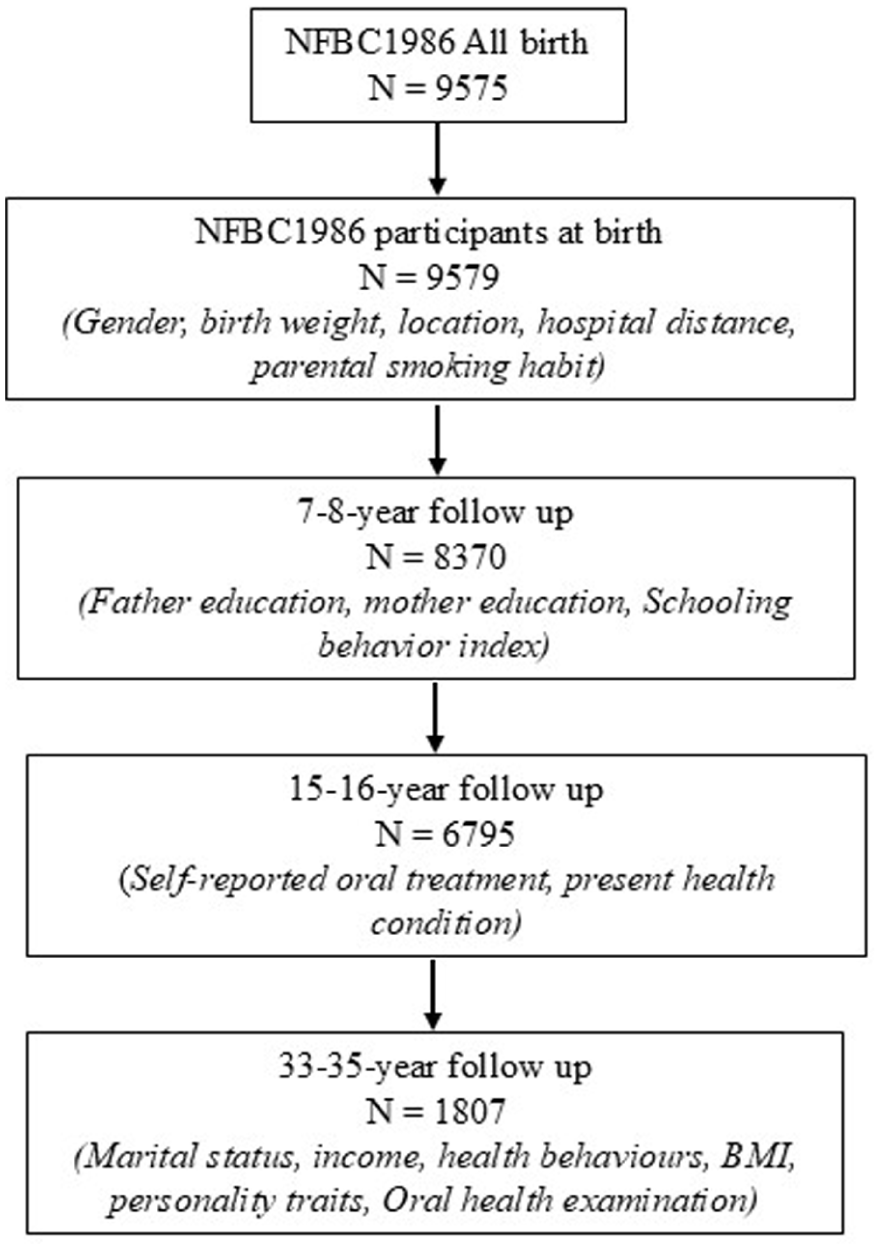
Flowchart illustrating study participants and variable used in the present study.
Ethical approval
The NFBC1986 study was approved by the Northern Ostrobothnia Hospital District Ethical Committee (108/2017).
Dependent variables
In this study, oral health status (dental plaque and dental caries) and the number of dental visits were considered as dependent variables. These variables were collected at the last follow-up of the cohort (during which the participants were 35 years old). Oral health status was based on clinical oral examinations performed by nine trained dentists, from May 2019 to December 2020 using a standardised clinical dental examination protocol. The detailed protocol and the quality assurance are provided in Supplementary file S2.
The presence of dental caries was registered utilising the International Caries Detection and Assessment System. Each surface was visually analysed, and its histologic depth was evaluated to score it between 0 and 6 according to the severity of the lesion [21]. Active lesions with a score of 3 or higher were considered to require restorative treatment and were therefore defined as coronal caries. Participants with at least one coronal caries lesion were classified as having dental caries. Likewise, teeth with dental plaque were also registered based on the presence or absence of visible dental plaque on the buccal surface. Participants with at least one tooth with dental plaque were classified as having dental plaque.
For the number of dental visits, a derived variable was created from a self-report questionnaire completed during the last visit to a dentist or dental hygienist/nurse in either private or public dental care. Participants were asked to fill out a survey on their oral health-related behaviours prior to clinical oral examination. Other dependent variables were bleeding on probing (BOP) and experienced jaw pain. BOP was registered from all the teeth present in the mouth. The extent of BOP was calculated by taking the total number of bleeding sites, divided by the total number of sites examined, and multiplying by 100. We used a question about jaw pain (‘Have you ever had pain in your jaw, temple, ear or in front of your ear on either side?’) with two responses (yes/no) to determine another dependent variable, namely, jaw pain. Definitions of the outcome variables are provided in Supplementary file S3.
Explanatory variables
Personality was the main explanatory variable. Personality traits (openness, conscientiousness, extraversion, agreeableness, and neuroticism) were constructed from the questionnaire related to opinions and experiences used in the NFBC cohorts project when the participants were 35 years old [20].
Other explanatory variables were sociodemographic characteristics: gender, place of residence at birth, number of household members, income, birth weight, parental education (at 7 years), parental smoking (at 7 years), schooling behaviour (at 7 years), oral treatment need (at 16 years), body mass index (BMI), physical exercise, number of missing teeth, brushing, and flossing, sugar consumption, alcohol, and smoking. Definitions of all explanatory variables are provided in Supplementary file S3.
Statistical analyses
To investigate the personality determinants related to oral health issues, we began by using the following specification to control for observable confounders:

where DHi represents a particular oral health issue of the ith individual; PTi′ is a vector of the personality variables, where k = 1,. . .,5 are the Big Five personality traits (i.e. openness, conscientiousness, extraversion, agreeableness and neuroticism); and Xi′ is a vector of an individual’s and his or her family’s characteristics. To facilitate the interpretation of our estimates, we began by standardising the Big Five variables to have a mean of zero and a standard deviation of ‘1’ in all the reported specifications of the baseline results. In the second part of our analysis, we focused on higher values by treating them as binary variables, specifically categorising individuals who belong to the third quantile of the variables as ‘1’.
In our models, we initially represented our dependent variables in their continuous form. Then, we shifted our focus towards evaluating the probability of individuals experiencing the most severe oral health issues, such as dental caries and plaque. We accomplished this by transforming these variables into binary outcomes, where a value of ‘1’ indicated a clinical diagnosis of at least one tooth with dental plaque. The same was applied for tooth with dental caries. To estimate this, we employed a linear probability model. For robustness, we also ran independent equation tests for dental caries, dental plaque, and dental visits.
We additionally employed a propensity score matching (PSM) strategy, which offers advantages over traditional methods because it does not rely on specific functional form assumptions. PSM was essential for addressing potential selection bias and ensuring more credible causal inferences between personality traits and oral health outcomes. Specifically, personality traits are not randomly distributed in the population and correlate with several socioeconomic, demographic, and behavioural characteristics [22, 15]. PSM allowed us to focus our analysis on samples in which there was sufficient overlap in the distribution of covariates between the treatment and control groups. This also allowed isolation of the effect of personality traits while avoiding the functional form of assumptions implicit in parametric models [23, 24]. In the PSM, we chose high openness as the treatment variable because of its stronger theoretical or empirical connection with health behaviours [14].
Finally, we investigated the full set of determinants for our dependent variables by using a recursive bivariate model strategy. Our method of analysis relied on a two-equation modelling of oral health outcomes and dental visits, which can be simply denoted as dh = f(x,v) and dv = l(g), where dh stands for caries or dental plaque, and dv stands for dental visits (i.e. both private and public dental sectors). Moreover, x and g refer to all the exogenous explanatory variables (i.e. personality traits, individuals, and family characteristics) in each case.
To investigate the interdependence between oral health status and dental care utilisation, we ran a recursive bivariate probit model (RBPM) introducing the variable ‘dental visits’ in the regression of oral health issues associated with caries and plaque [25]:

where Φ dh (.) refers to the bivariate normal cumulative distribution function and involves forming the joint distribution of two random variables and then maximising the full log-likelihood function. In addition to the variable for dental care visits, which appeared to be an explanatory variable in the oral health status models (i.e. dh), the equations of the introduced model were linked by their disturbances. Finally, we decomposed the effects by considering two kinds of effects on the probability of having dental caries or plaque, that is, one as a direct effect coming from the first model and the other as an indirect effect through dental visits. The total effect of each of our explanatory variables on the probability of having caries or plaque was given by the sum of these two variables. If a variable only appeared on the right-hand side of the first (second) model, then its direct (indirect) effect on the probability of having dental caries or plaque was also its total effect.
All analyses used STATA 18 and psmatch2, and appropriate tests were carried out to compare covariate distributions across our matched groups. We used PSM with the nearest neighbour method with replacement (as this approach has been shown to reduce bias relative to matching without replacement); we also used the common option, so that off-support observations were automatically excluded from the analysis, ensuring that only comparable treated and control units were matched.
Results
In this study sample, the mean (±SD) dental caries and plaque scores at 35 years were 0.9 (±1.9) and 2.1 (±4.2), respectively (Supplementary file S3).
In both models, openness was negatively associated with occurrence of dental caries, dental plaque and BOP percentage. Conversely, agreeableness was positively associated with occurrence of dental caries, dental plaque and BOP percentage (Table I).
Psychological determinants of oral health behaviour.
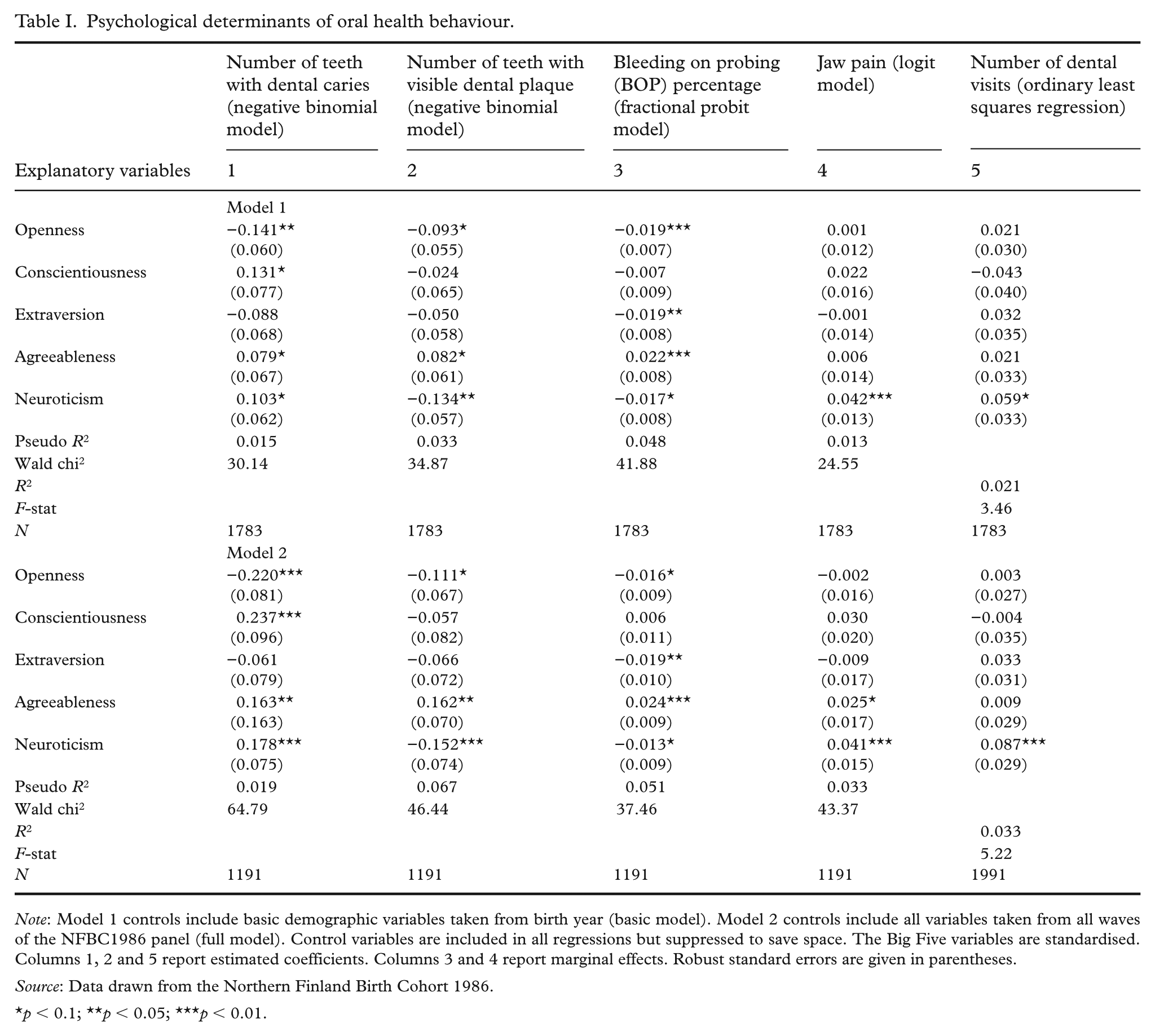
Note: Model 1 controls include basic demographic variables taken from birth year (basic model). Model 2 controls include all variables taken from all waves of the NFBC1986 panel (full model). Control variables are included in all regressions but suppressed to save space. The Big Five variables are standardised. Columns 1, 2 and 5 report estimated coefficients. Columns 3 and 4 report marginal effects. Robust standard errors are given in parentheses.
Source: Data drawn from the Northern Finland Birth Cohort 1986.
p < 0.1; **p < 0.05; ***p < 0.01.
The association between oral health status (dental caries and dental plaque), dental visits and higher levels of specific personality traits are shown in Table II. Individuals with a high level of openness had 8.4 percentage-point lower probability of having teeth with dental caries. Likewise, individuals with high levels of neuroticism had a 4.7 percentage-point lower probability of having teeth with visible dental plaque, potentially due to their tendency to attend dental visits more frequently (a 2.6 percentage-point higher probability). Finally, highly extraverted individuals had a 7.5 percentage-point lower probability of visiting dental services (Table II).
Personality determinants on the probability of an individual experiencing dental caries or plaque and having a dental visit: ordinary least squares (OLS) estimation results.
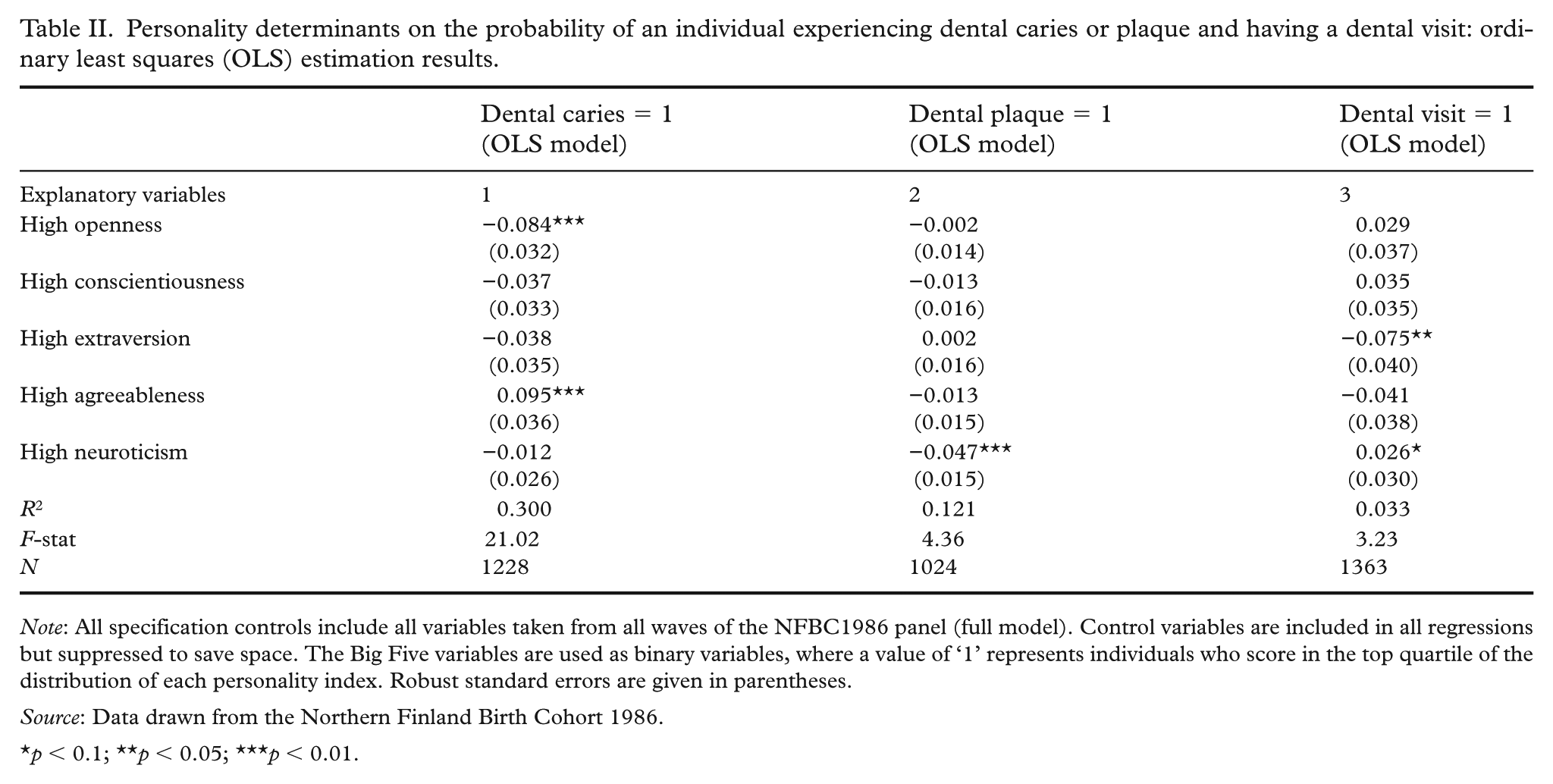
Note: All specification controls include all variables taken from all waves of the NFBC1986 panel (full model). Control variables are included in all regressions but suppressed to save space. The Big Five variables are used as binary variables, where a value of ‘1’ represents individuals who score in the top quartile of the distribution of each personality index. Robust standard errors are given in parentheses.
Source: Data drawn from the Northern Finland Birth Cohort 1986.
p < 0.1; **p < 0.05; ***p < 0.01.
The distribution of propensity scores across the treatment and control groups are presented in Supplementary file S5. Both graphs demonstrated sufficient overlap between the treatment and control groups.
Individuals with a high degree of openness had a 13% lower probability of experiencing dental caries, whereas those with high agreeableness had a 10.2% higher probability. Highly neurotic individuals had a 5% lower probability of experiencing dental plaque while simultaneously having a 2.7-fold greater probability of having a dental visit. Interestingly, highly extraverted individuals had a 7.4% lower probability of having a dental visit. The association between personality traits and OHBs remained highly consistent and stable (Table III). Moreover, the size and magnitude of these effects remained unchanged even when each personality trait was incorporated individually, as indicated in Supplementary file S6.
Personality determinants on the probability of an individual experiencing dental caries or plaque and having a dental visit: propensity score matching results.
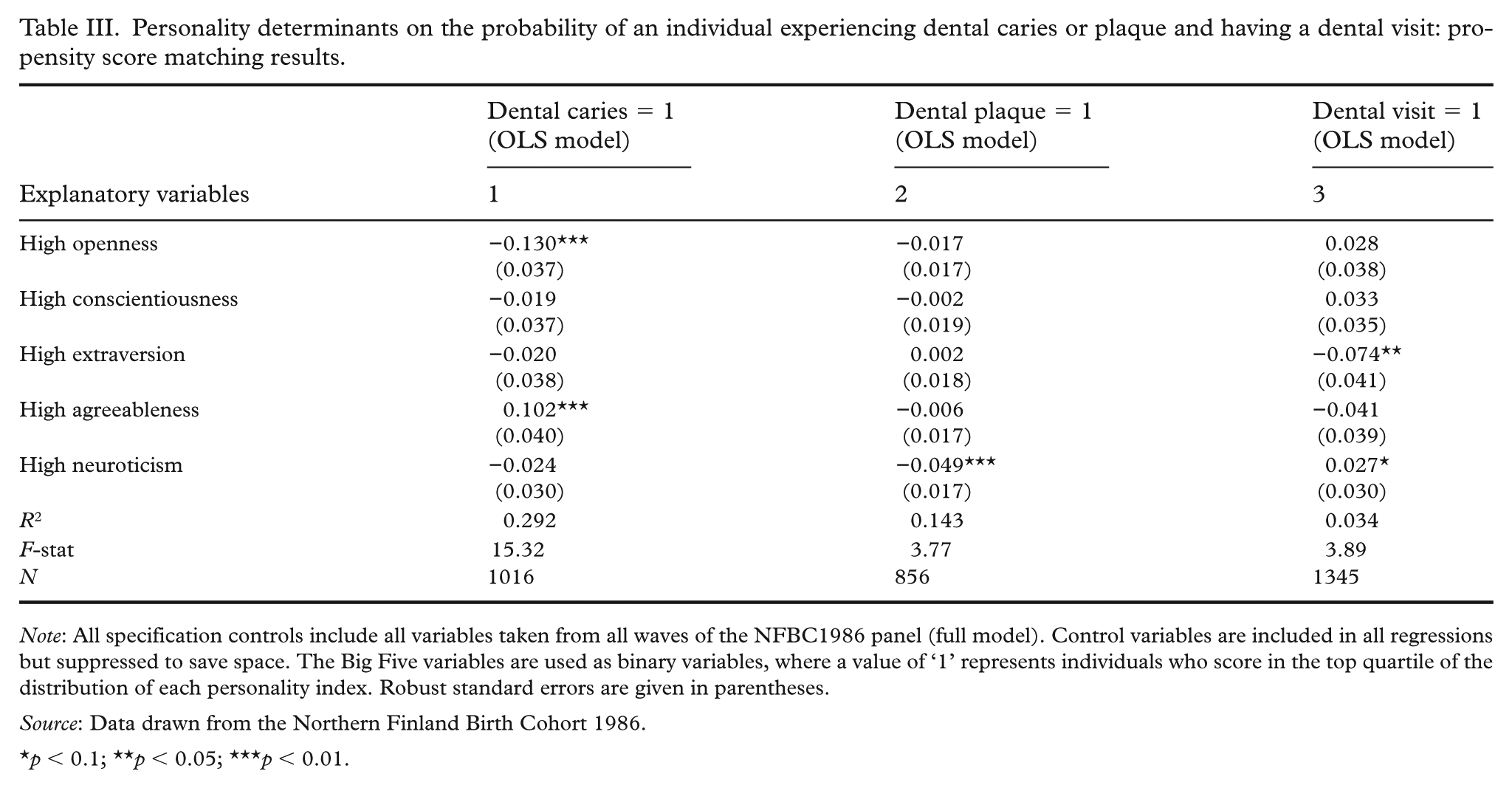
Note: All specification controls include all variables taken from all waves of the NFBC1986 panel (full model). Control variables are included in all regressions but suppressed to save space. The Big Five variables are used as binary variables, where a value of ‘1’ represents individuals who score in the top quartile of the distribution of each personality index. Robust standard errors are given in parentheses.
Source: Data drawn from the Northern Finland Birth Cohort 1986.
p < 0.1; **p < 0.05; ***p < 0.01.
The results of the RBPM for dental caries and dental plaque are presented in Table IV. The marginal effects of RBPM indicate that individuals with higher levels of openness had a greater likelihood of visiting a dentist and a lower likelihood of experiencing dental caries. Similarly, higher levels of conscientiousness were associated with a lower probability (0.8%) of having dental plaque but also a higher probability (1.8%) of visiting a dentist. Agreeableness was found to be associated with a higher likelihood of visiting a dentist and a higher likelihood of individuals experiencing dental caries. Finally, individuals demonstrating high levels of neuroticism had a higher probability of having a dental visit, resulting in a lower probability of dental plaque.
Estimation results from the recursive probit models for dental caries, dental plaque, and dental care use (visit).
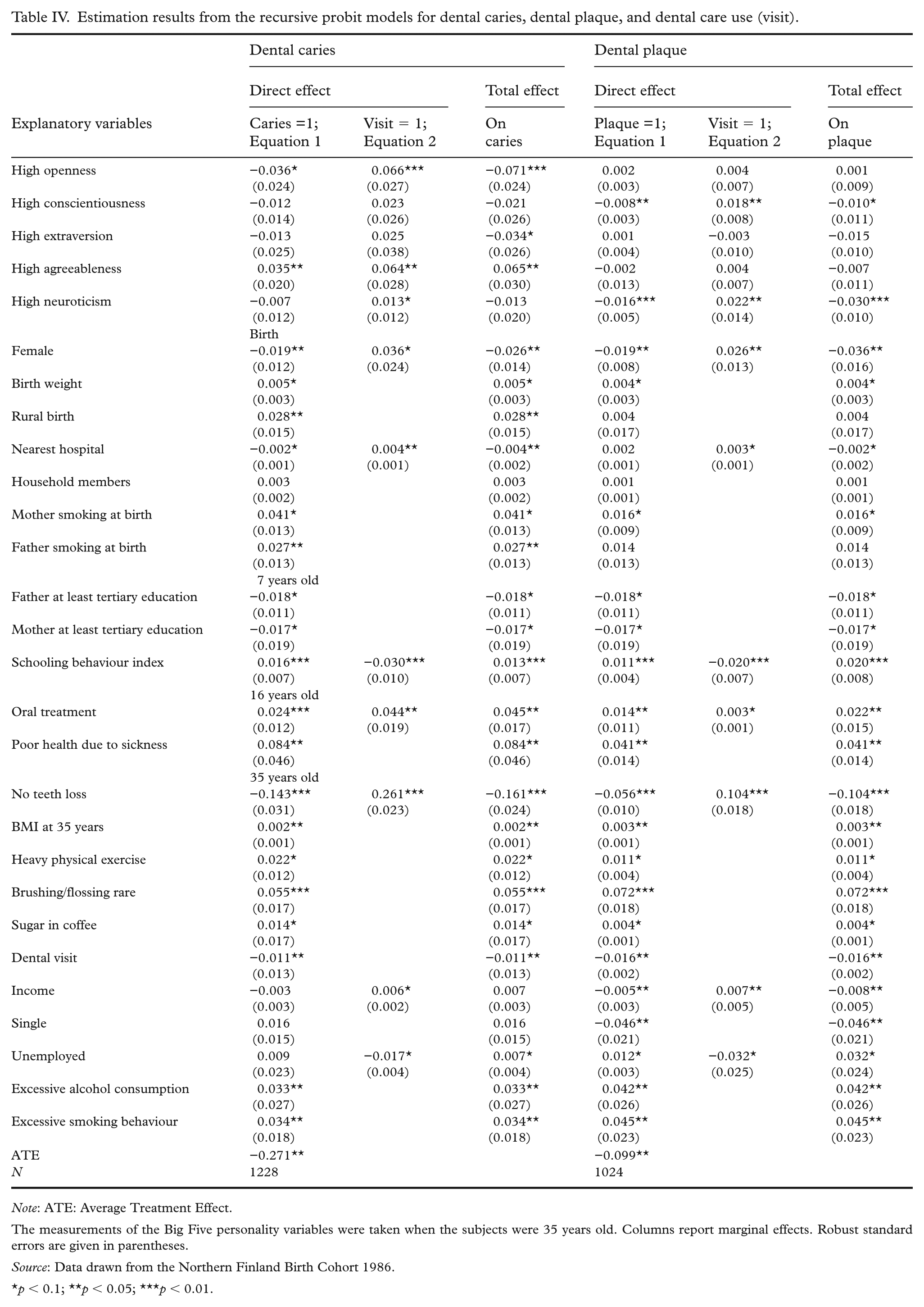
Note: ATE: Average Treatment Effect.
The measurements of the Big Five personality variables were taken when the subjects were 35 years old. Columns report marginal effects. Robust standard errors are given in parentheses.
Source: Data drawn from the Northern Finland Birth Cohort 1986.
p < 0.1; **p < 0.05; ***p < 0.01.
Discussion
This study aimed to investigate the association between personality traits and OHB. Our findings revealed that the individuals with heightened levels of openness had fewer teeth with dental caries and attended dental visits more regularly. Additionally, individuals demonstrating high levels of conscientiousness and those with high levels of neuroticism had a greater probability of having a regular dental visit, resulting in a lower probability of dental plaque accumulation. The main findings of the present study support our hypothesis: ‘individuals with a higher level of openness have fewer teeth with dental plaque and dental caries and attend dental visits more regularly’.
One of the strengths of the present study was the inclusion of a clinical oral health examination done by a team of trained and standardised dentists, thereby enhancing the accuracy and validity of the study findings. Another strength was the inclusion of a relatively large sample for investigating the association between personality traits and OHBs. However, it is important to acknowledge that there may still be sources of selection bias that could have influenced our findings. First, it is worth noting that the individuals who had dropped out before the last wave of data collection, or those with severe physical or mental health issues, were not considered in this study. Unfortunately, this means that we lacked personality trait information for these individuals because our personality assessment was conducted during the last wave, when the participants were 35 years old. Finally, the geographical restriction of our sample (i.e. cohort members living within a 250-km radius of the centre of Oulu city) in the dental clinical examination may have subjected to selection bias. However, to minimise any potential bias related to these factors, all the known confounders were adjusted for in the regression models.
In the present study, individuals with heightened levels of openness demonstrated a propensity for having fewer teeth with dental caries. This association seems to have been moderated by the dental visit patterns of these individuals. In line with the current study, a previous study concluded that individuals who are open to new experiences visit dental care regularly throughout their lifetime [26]. The most probable reason for this is that these individuals are concerned about their looks and will therefore be more likely to visit dentists and consistently follow good oral hygiene practices. Previous studies have also concluded that individuals indicating openness to experience adhere to healthy lifestyle choices such as high intakes of vegetables and fruit [27, 28]. Individuals with high levels of conscientiousness generally tend to follow social norms and are also self-disciplined. For instance, individuals who are high in conscientiousness are likely to be physically active and to eat healthily [29]. This may support our findings regarding regular dental visits and reduced dental plaque deposition among conscientiousness individuals, as toothbrushing at least twice daily is widely recommended and considered a social norm. It is also well known that brushing at least twice a day with fluoridated toothpaste helps to reduce dental plaque [5]. Surprisingly, our study indicated that individuals with high levels of neuroticism tended to visit the dentist regularly, thereby having less dental plaque. This finding is implausible, given the multiple facets of this particular personality characteristic, such as anxiety, depression, anger, and sadness experienced by those with high levels of neuroticism. Neurotic individuals tend to adopt harmful behaviours, such as smoking and alcohol consumption, and are likely to have unhealthy diets, be less physically active and therefore be at greater risk of cardiovascular diseases [29]. However, these regular dental visits may be due to the heightened anxiety and health concerns that are typical of neurotic individuals. Such feelings of anxiety are likely to make them more vigilant about their health, including their oral care, prompting them to visit the dentist regularly as a preventative measure. Another possibility is that the self-conscious, perfectionist nature found in individuals with high levels of neuroticism could further motivate them to maintain good oral hygiene and seek professional care to ensure good oral health. However, further study is necessary to confirm or rule out this relation, and a specific focus on the basic nature of neuroticism and oral health-related behaviours may help to reveal a causal pathway.
Our findings relating to the presence of dental caries and -plaque in relation to socioeconomic status were in line with previous studies that concluded factors such as sex (female), and social background factors such as higher educational attainment, living in urban areas, and higher annual income are associated with good oral health outcomes [30 -32]. Similarly, behavioural factors such as adequate oral hygiene practices (brushing with fluoride toothpaste and interdental cleaning or flossing) can effectively remove dental plaque, which in turn can reduce new carious lesions [33]. This relation was also evident here. Additionally, harmful habits such as excessive alcohol consumption and smoking being associated with the presence of dental caries and dental plaque in the present study corroborates with a recent systematic review [4].
Considering that dental caries and plaque accumulation are preventable, it is crucial to prioritise favourable oral health and capitalise on the long-term advantages of oral health promotion. This necessitates strengthening appropriate policies and public health measures that focus on enhancing dental health education, and mitigating the detrimental effects of common risk factors of oral health. Numerous evaluations of policies have demonstrated the effectiveness of interventions aimed at motivation and awareness. Our study underscores the immense advantages of such programmes, which encompass a wide array of health behaviours. Previous studies have found selective, personality-targeted interventions to be effective at reducing risky habits [34, 35]. Such interventions could yield significant, enduring benefits for individuals and society as a whole. However, for a fuller picture, further studies exploring the benefits and effectiveness of selective personality-targeted interventions in oral health must be conducted.
In conclusion, this study revealed an association between personality traits and OHB (accumulation of dental plaque and regular dental visit) and, consequently, an oral health outcome (presence of dental caries). By implementing robust policies and fostering comprehensive oral health initiatives, individuals could be empowered to achieve optimal oral well-being, which could lead to improved overall health outcomes for the individual and a wider positive impact on society as a whole.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261426166 – Supplemental material for Personality as a key driver of oral health behaviour: evidence from the Northern Finland Birth Cohort
Supplemental material, sj-docx-1-sjp-10.1177_14034948261426166 for Personality as a key driver of oral health behaviour: evidence from the Northern Finland Birth Cohort by Evangelos Mourelatos, Jaakko Simonen, Marja-Liisa Laitala and Saujanya Karki in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank all cohort members and researchers who participated in the study. We also wish to acknowledge the work of the Northern Finland Birth Cohort project center. The authors would further like to acknowledge Jesse Jokirinta for his help.
Author contributions
The authors confirm contribution to the paper as follows: study conception and design: E. Mourelatos, S. Karki; data collection: E. Mourelatos, S. Karki; analysis and interpretation of results: E. Mourelatos; draft manuscript preparation E. Mourelatos, J. Simonen, M.-L. Laitala, S. Karki. All authors reviewed the results and approved the final version of the manuscript.
Data availability statement
The data that support the findings of this study are available from the Northern Finland 1986 Birth Cohort (![]() ). NFBC data are available from the University of Oulu, Infrastructure for Population Studies. Permission to use the data can be applied for research purposes via an electronic material request portal (NFBCprojectcenter@oulu.fi). Restrictions apply to the availability of these data, which were used under license for this study.
). NFBC data are available from the University of Oulu, Infrastructure for Population Studies. Permission to use the data can be applied for research purposes via an electronic material request portal (NFBCprojectcenter@oulu.fi). Restrictions apply to the availability of these data, which were used under license for this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
NFBC1986 received financial support from the EU QLG1-CT-2000-01643 (EUROBLCS) Grant no. E51560, NorFA Grant no. 731, 20056, 30167, USA / NIH 2000 G DF682 Grant no. 50945. The oral health study was supported in part by the Research Council of Finland (former Academy of Finland, Grant no. 326189). The funder had no role in study design, data collection, analyses, and interpretation.
Supplemental material
Supplemental material for this article is available online.