
Abstract
Aim:
To examine trends in the treatment and rehabilitation of depression prior to disability pension application due to depression.
Methods:
This retrospective register-based study included 30,105 applicants for disability pension due to depression, and it is based on data from the Social Insurance Institution of Finland (Kela). The trends in antidepressant purchases and rehabilitation measures during the year preceding the application were analysed for 2010–2019 using linear regression analysis, with analysis of covariance to assess the interactions of age- and sex-based population groups with these trends.
Results:
A stable proportion of approximately 1 in 10 (9.2%–12.2%) applicants had had neither antidepressant purchases nor psychotherapy in the preceding year, with no statistically significant trend (p < 0.05). The proportion of applicants with a history of antidepressant use decreased slightly from 90.3% to 87.5%. However, the proportion of applicants with a history of psychotherapy or both psychotherapy and antidepressants doubled over the same period (from 6.1% to 13.5% and from 5.6% to 11.7%, respectively). Annually, estimated average antidepressant use declined by 0.25 percentage points, psychotherapy increased by 0.90 percentage points, and combined treatment increased by 0.75 percentage points, all statistically significant. A statistically significant interaction in psychotherapy trends was observed in population groups based on sex and age. The highest proportion of applicants receiving psychotherapy was among females under the age of 40.
Conclusions:
Background
Major depressive disorder is a disabling yet treatable condition. In fact, it has been ranked among the most disabling diseases worldwide [1]. Depression is associated with a high risk of sickness absence and disability pension [2,3]. Furthermore, cost-of-illness studies indicate substantial societal costs, particularly due to lost productivity [4–6].
The majority of individuals with depression recover within 1 year [7]. However, there is a risk of recurrent symptoms, and some individuals develop chronic symptoms and long-term disability [7].
Several treatment options have been established. The primary forms of treatment include evidence-based psychotherapies and antidepressive pharmacotherapies, which may be augmented with lithium or neuroleptics [8]. Additionally, neuromodulatory treatments are available [8].
However, many individuals with depression do not receive adequate treatment. A study conducted in 21 countries found that only one-sixth of people with depression had received minimally adequate treatment in the preceding year, and even in high-income countries, this proportion ranged from just one-sixth to one-third [9].
In particular, those with severe and disabling symptoms require effective treatment. However, previous studies in Finland have shown that treatment remains inadequate even among those applying for disability pension due to depression [10–13]. This is particularly concerning, as in the Finnish social security system, a disability pension is granted only when incapacity for work has lasted for over a year. It is, therefore, typically preceded by sickness allowance for approximately 1 year, providing ample time for treatment. Disability pension is intended as a last resort and should be preceded by appropriate treatment and vocational rehabilitation (e.g. a work trial, retraining), aimed at improving employment opportunities. Moreover, under Finnish legislation, vocational rehabilitation is prioritised over temporary or permanent disability pension [14].
In recent years, several actions have been implemented to improve the treatment and rehabilitation of individuals with depression. Since 2011, the Social Insurance Institution of Finland (Kela) has reimbursed psychotherapy treatment as a subjective right rather than as a discretionary benefit. A reform of occupational healthcare took place in 2012, recommending earlier assessments of rehabilitation needs and return-to-work possibilities through collaboration between occupational healthcare, employers and employees. Additionally, more accurate clinical guidelines and local treatment protocols were introduced between 2010 and 2019. Nevertheless, our previous study concluded that, in 2019, treatment and rehabilitation among individuals applying for Kela’s disability pension due to depression remained insufficient [13]. However, no conclusions could be drawn regarding the trends in treatment, as the results were not directly comparable with earlier studies due to significant differences in study settings and methodologies [10–12].
Aim
We aimed to examine trends in the treatment and rehabilitation of depression prior to disability pension application from Kela due to depression from 2010 to 2019.
Methods
Kela’s registries were utilised in this study. Decisions on disability pension applications were collected from Kela’s registry on national pension decisions. We determined new applicants for Kela’s disability pension for each year between 2010 and 2019. This was done by gathering disability pension applications with major depressive disorder (International Statistical Classification of Diseases, 10th Revision (ICD-10) F32) or recurrent depressive episode (F33) as the main diagnosis from Kela’s registries. Applicants who were previously granted permanent or fixed-term disability pension within 1 year from the application date were excluded. In addition, applications with additional diagnoses of psychoses (ICD-10 diagnoses F20–F29), manic or bipolar disorders (F30–F31), organic mental disorder (F00–F09), and intellectual disabilities (F70–F79) were excluded. Applicants who were not permanent residents in Finland at the end of the previous year had to be excluded because applied registries contain information only on people living in Finland. If a person had more than one application during a calendar year, only the first application with depression as the main diagnosis was taken into account. The exclusion criteria were checked for every calendar year separately.
Altogether, 34,923 applicants for disability pension due to depression were detected between 2010 and 2019. There were 3740 applicants who had been on disability pension during the previous year and were therefore excluded. Further, 662 applicants were excluded due to comorbidities. In addition, 416 persons were excluded due to not having been living in Finland at the end of the previous year. A total of 30,105 applicants were included in the analyses.
Further, information on age and sex was collected from Kela’s population register. All information on treatment was calculated in relation to the day the application was received by Kela. Information on pharmacotherapies was received from Kela’s register on reimbursed medicine purchases. Data on antidepressant purchases were gathered for the year preceding the disability pension application and organised by registered purchase date and Anatomic Therapeutic Chemical (ATC) code, including ATC code group N06A, which encompasses antidepressants.
Data on Kela’s rehabilitation were gathered from Kela’s registry for the year preceding the disability pension application based on payment periods. The data included a) all vocational rehabilitation interventions and b) psychotherapies. The psychotherapy data included all psychotherapies funded by Kela, regardless of whether they were reimbursed as rehabilitative psychotherapy or as demanding medical rehabilitation. These two forms differ in their legal basis, reimbursement level, and maximum duration. In practice, medical rehabilitation is used to cover more severe illnesses, where functional capacity is significantly reduced.
Shares of applicants for disability pension due to depression receiving antidepressants, psychotherapy, both antidepressants and psychotherapy, neither psychotherapy nor antidepressants, and vocational rehabilitation were calculated for each calendar year from 2010 to 2019. Linear regression analysis was used to examine linear trends in treatment and rehabilitation patterns separately in the following groups: males <40 years, males ⩾40 years, females <40 years, and females ⩾40 years. In addition, analysis of covariance was employed to assess the interaction effects of age- and sex-based population groups on treatment trends, each treatment form being assessed separately. A p-value less than 0.05 was considered statistically significant and was reported using the thresholds of less than 0.05, less than 0.01, and less than 0.001 to describe the level of statistical significance.
Results
The number of disability pension applicants due to depression ranged from 3127 to 3827 per calendar year without no clear trend (Table I). Approximately one-third of the applicants were male and two-thirds were female constantly during the studied period. Applicants were aged between 16 and 66 years, with the mean age ranging from 41.5 to 44.9 years. The share of younger applicants (<40 years) increased during the years 2010–2019.
Basic characteristics of the study population during years 2010–2019.
Number of disability pension applicants in the study population for each calendar year.
The share of disability pension applicants who had antidepressant purchases during the year preceding the application changed slightly (range 86.4%–90.3%) in the whole study population (Figure 1). However, there was a statistically significant (p < 0.05) decreasing trend with an estimated average annual reduction of 0.25 percentage points. In the subgroups, a statistically significant decreasing trend was observed among females <40 years (p < 0.01) with an estimated annual average reduction of 0.36 percentage points, and females ⩾40 years (p < 0.05) with an estimated annual average reduction of 0.39 percentage points. No statistically significant trend was observed among males <40 years or males ⩾40 years. Furthermore, males aged 40 or older had fewer antidepressant purchases than females and younger males. Population groups based on age and sex showed a statistically significant interaction (p < 0.05) with the trend in antidepressant treatment.
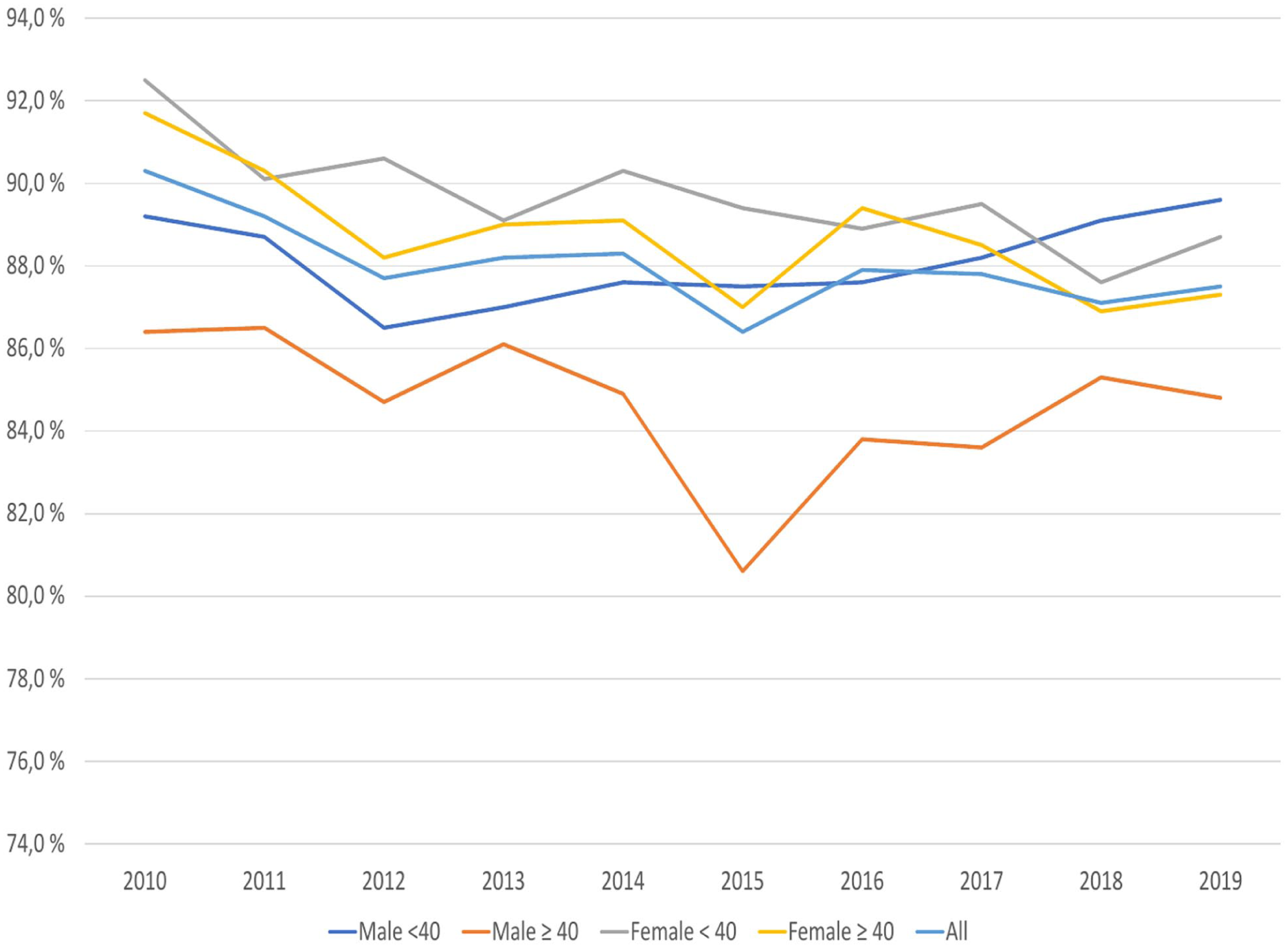
Proportions of applicants for disability pension due to depression from 2010 to 2019 who purchased antidepressants during the year preceding the application for disability pension from Kela.
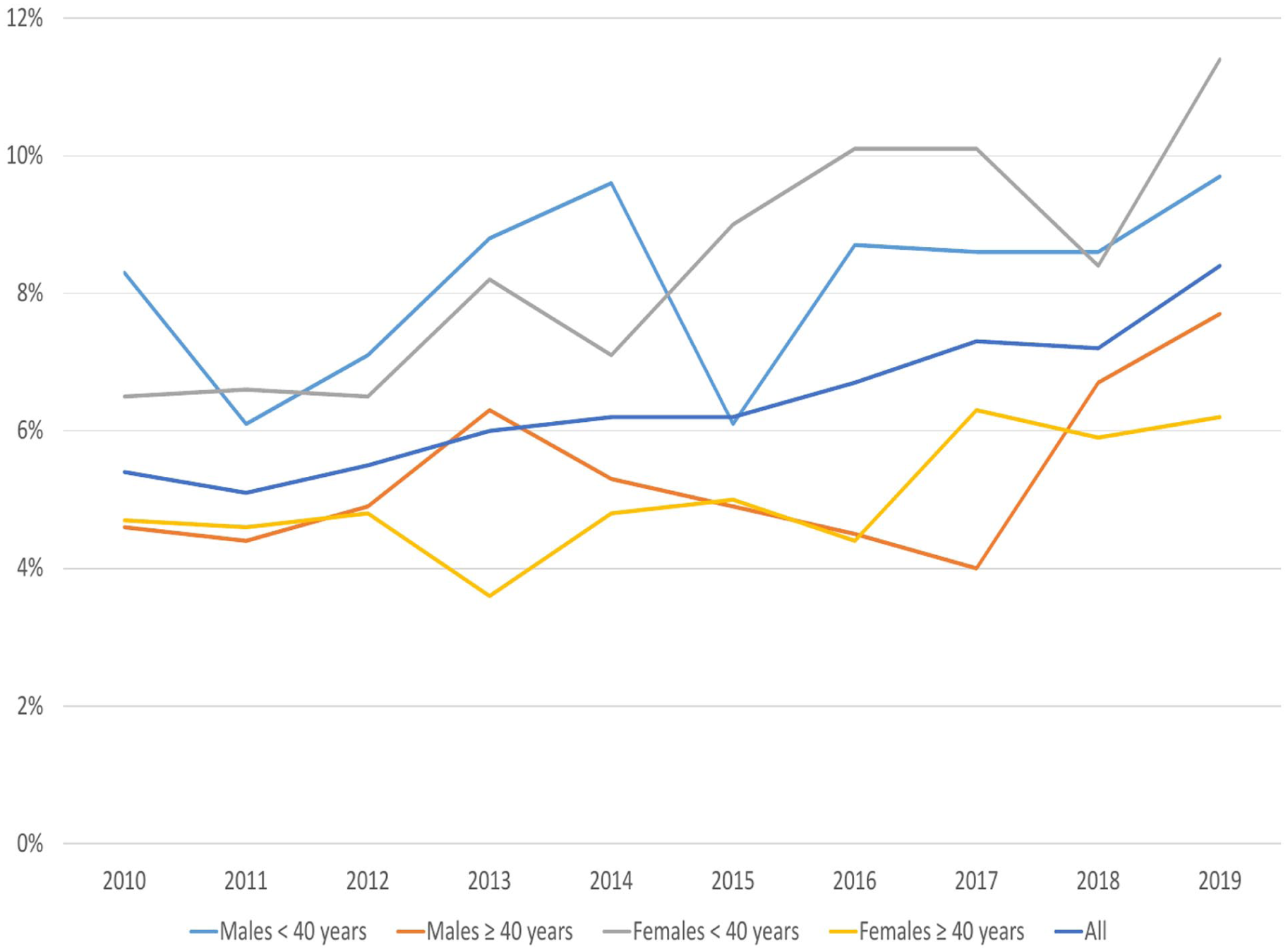
The proportion of disability pension applicants who received psychotherapy during the year preceding their application increased, with a statistically significant trend (p < 0.001) in both the total study population and in subgroups defined by age and sex (Figure 2). In the whole study population, the share of applicants receiving psychotherapy during the year preceding the application increased from 6.1% to 13.5% with an estimated annual average change of 0.90 percentage points. In the age- and sex-based subgroups, female applicants <40 years of age had received the most psychotherapy, while male applicants ⩾40 years of age had received the least psychotherapy. The estimated annual average increases in the shares of applicants receiving psychotherapy were 1.0% for females <40 years, 0.75% for females ⩾40 years, 0.85% for males <40 years, and 0.44% for males ⩾40 years. Population groups based on age and sex showed a statistically significant interaction (p < 0.05) with the trend in psychotherapies.
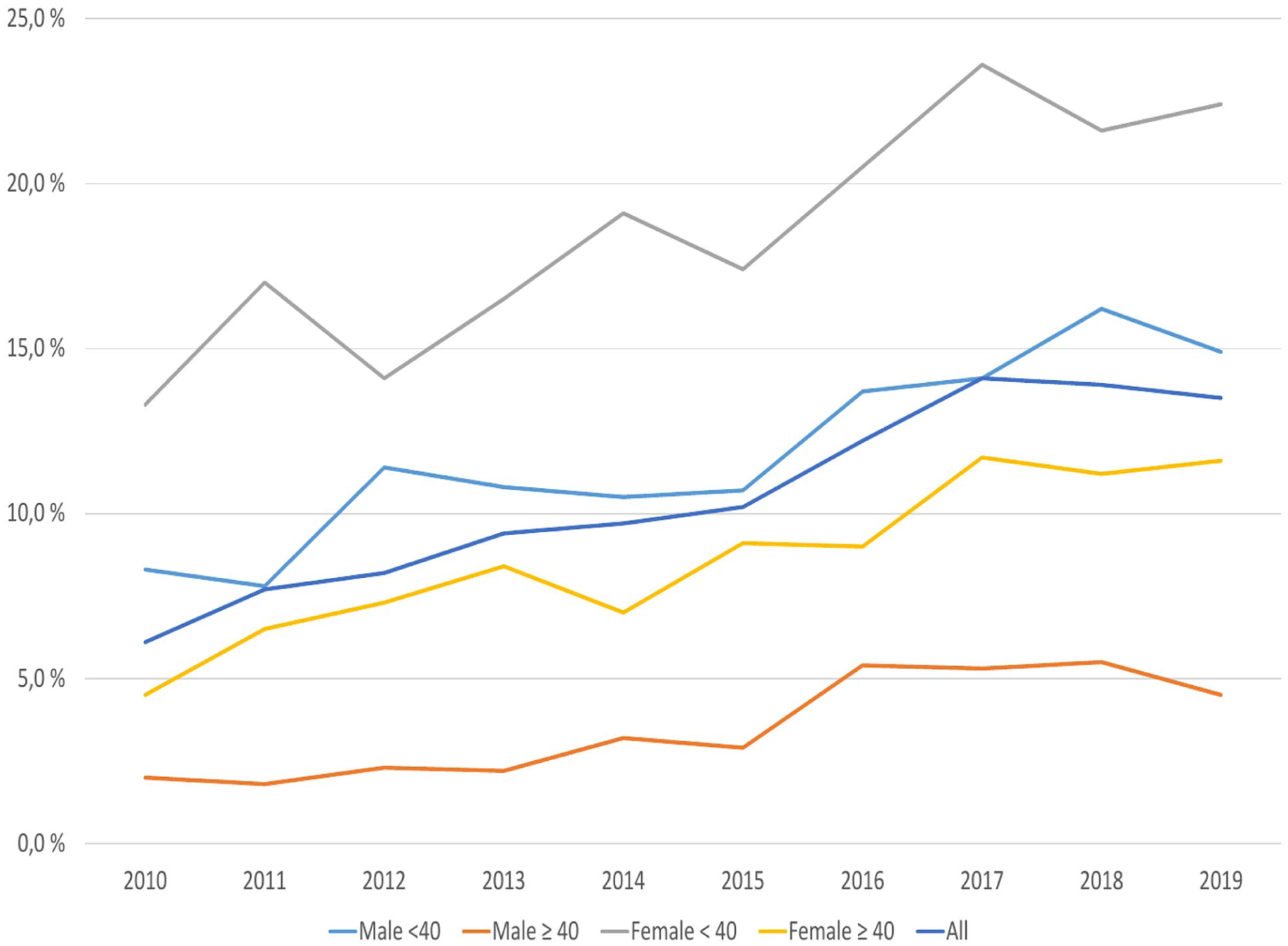
Proportions of applicants for disability pension due to depression from 2010 to 2019 who received psychotherapy during the year preceding the application for disability pension from Kela.
In the whole study population, the share of applicants for disability pension due to depression who received both antidepressants and Kela’s psychotherapy during the year preceding the application increased statistically significantly (p < 0.001) from 5.6% to 11.7% with an estimated annual average increase of 0.75 percentage points (Figure 3). A statistically significant increase was observed also among all age groups and sexes with an estimated annual average increase of 0.77 percentage points (p < 0.001) among males <40 years, 0.37 percentage points (p < 0.001) among males ⩾40 years, 0.79 percentage points (p < 0.01) among females <40 years, and 0.63 percentage points (p < 0.001) among females ⩾40 years. The interaction of population groups based on age and sex with the trend was not statistically significant.
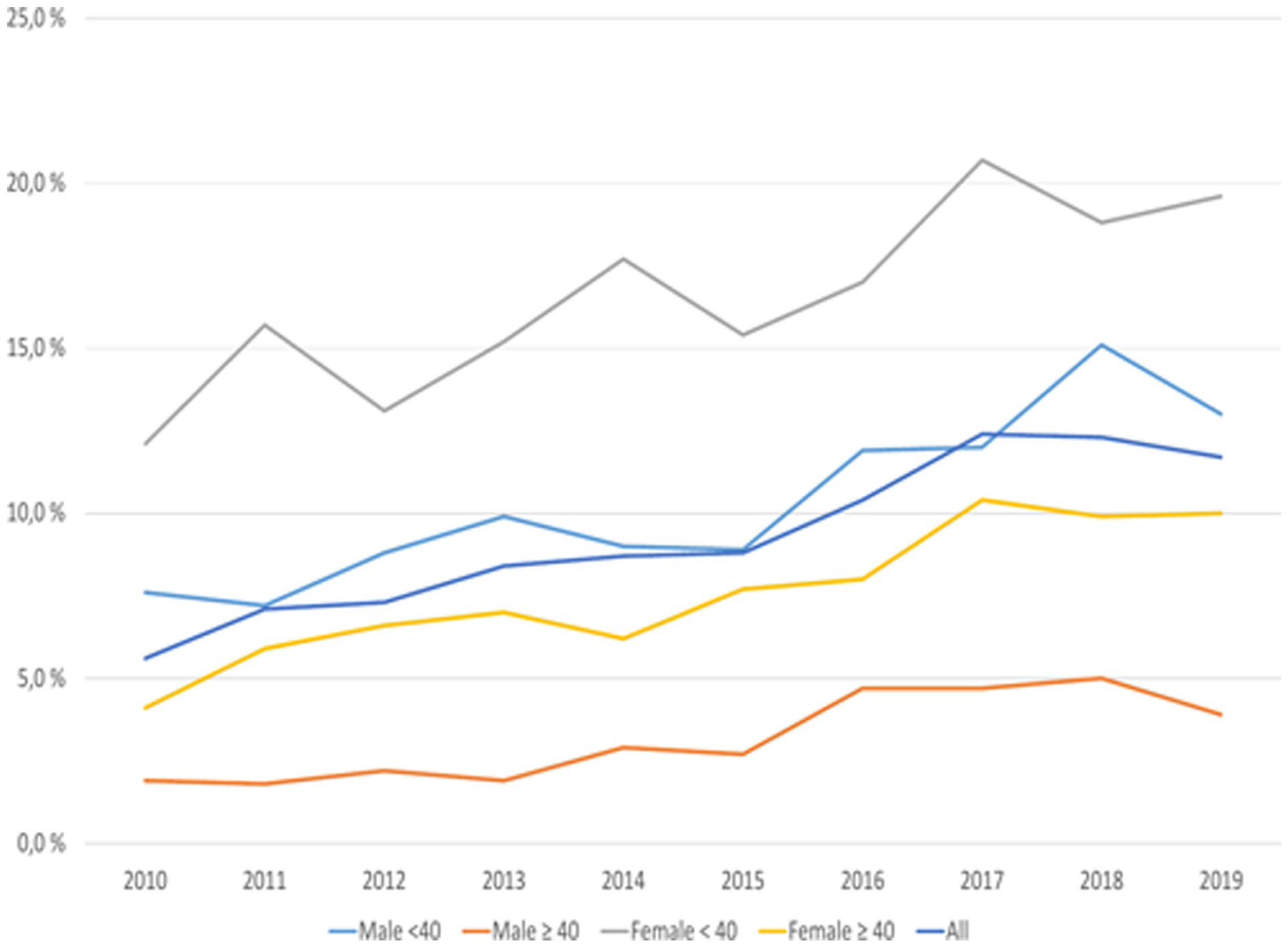
Proportions of applicants for disability pension due to depression from 2010 to 2019 who purchased antidepressants and received psychotherapy during the year preceding the application for disability pension from Kela.
In addition to the results presented in Figures 1 to 3, we analysed the share of applicants who received neither antidepressants nor psychotherapy. This share was quite stable (range 9.2%–12.2%) with no statistically significant trend in the whole study population. With an estimated annual average increase of 0.26 percentage points, females aged 40 or older was the only subgroup with a small statistically significant rising trend in the share of applicants receiving neither antidepressants nor psychotherapy (p < 0.05). No statistically significant trend was observed among females under 40 years of age, males under 40 years of age, or males aged 40 or older. The interaction of population groups based on age and sex with the trend was not statistically significant.
The share of applicants receiving vocational rehabilitation during the year preceding the application in 2010–2019 varied from 5.1% to 8.4% in the whole study population (Figure 4). It was more common among the younger age groups, that is, under 40 years of age. A statistically significant increasing trend (p < 0.001) was observed with an estimated annual average increase of 0.31 percentage points. In the subgroups, the trend was statistically significant only among females <40 (p < 0.01) with an estimated annual average increase of 0.50 percentage points and females ⩾40 years with an estimated annual average increase of 0.20 percentage points. However, among males, no statistically significant trend was observed among either <40 years or ⩾40 years. The interaction of population groups based on age and sex with the trend was not statistically significant. Supplementary Table 1 presents the detailed results from the linear regression analysis of treatment trends by treatment type and population group.
Proportions of applicants for disability pension due to depression from 2010 to 2019 who received vocational rehabilitation during the year preceding the application for disability pension from Kela.
Discussion
Most of the applicants for disability pension due to depression purchased antidepressants during the year preceding the application, but only a minority received psychotherapy and vocational rehabilitation. However, trends in the take up of both Kela’s psychotherapy and vocational rehabilitation were rising. The proportion of those who purchased antidepressants and received psychotherapy during the year preceding the application more than doubled from 5.6% in 2010 to 11.7% in 2019, as the share of persons attending psychotherapy rose from 6.1% to 13.5%. Nonetheless, constantly approximately 1 in 10 disability pension applicants received neither antidepressants nor psychotherapy. Utilisation of psychotherapy increased in both sexes and across all age groups, but it was significantly more common among females than males and among younger individuals compared to older ones. Vocational rehabilitation was also more common among younger individuals than older ones.
Previous studies in Finland across different disability pension systems have also found that treatment is often inadequate prior to applying for disability pension [10–13]. Data from the National Pension Register showed that the share of individuals applying for disability pension due to depression and not using antidepressants was 13% in 1993–1994 and 14% in 2003–2004 [10,11]. Similarly, data from the earnings-related pension system in 2012 showed that 17% of the applicants were not using antidepressants [12]. In our dataset, 9.7%–13.6% of disability pension applicants in different years had no recorded antidepressant purchases in the year preceding their application. Unlike earlier studies based on self-reported responses, our findings relied on comprehensive registry data, yet the proportions are quite similar and have remained relatively stable over the years.
Previously, the dataset from the Finnish Centre for Pensions has compared the provision of care between 1993–1994 and 2003–2004 for individuals who were granted disability pension due to depression, without significant changes in the proportion receiving treatment [11]. The current study, however, focuses on applicants for Kela’s disability pension and covers a later period, 2010–2019, during which significant changes were made, particularly to the availability of psychotherapies. Kela’s general statistics show that the share of people using antidepressants has increased by over 10% and the use of psychotherapies has tripled during the studied time period [15]. Compared to these statistics from the general population, the findings of the rising trend in the use of psychotherapies among applicants for disability pension due to depression in this study are modest, as this is a group of people with a clear need for effective treatment.
The results of studies on the proportion of people receiving different treatments for depression in general are inconsistent of their results. However, studies focusing only on depression patients are not available from Finland. A study in 19 European countries showed an increase in the use of antidepressants among depressed people in 2013–2019 [16]. In the U.S. population, there was no significant change between 2015 and 2020 in the share of depressed people who received prescribed medication (60.2%–61.2%) or in the proportion of those who were talking to a professional (47.9%–48.0%) [17]. However, earlier U.S. population samples from 1998 to 2007 showed a small increase in the share of depression patients using antidepressants (73.8%–75.3%), but the share of patients receiving psychotherapy decreased from 53.6% to 43.1% [18]. In Florida, antidepressant use increased from 80.6% to 86.8% from 1996 to 2006, while psychotherapy decreased from 56.6% to 37.5% [19]. The results from a Norwegian study on general practice between 2009 and 2015 showed an increase in the share of patients with depression receiving talking therapy (from 42.9% to 63.4%) and referrals to secondary care (from 16.6% to 21.6%), and a decrease in depression patients receiving pharmacotherapy (from 31.3% to 25.9%) [20]. However, these studies depict general trends in the treatment of depression and are not, therefore, directly comparable to our study, as our study population comprises persons with such severe depression to have caused them to apply for disability pension.
The observed sex- and age-related differences in psychotherapy use align with patterns in the Finnish general population: young women use Kela’s psychotherapies most and older men least, with young women showing the greatest recent increase. In 2019, 0.69% of men and 2.42% of women aged 16–64 received such therapy [15]. In contrast, international studies report smaller sex differences in depression treatment: in the United States, men and women received antidepressants and psychotherapy at comparable rates between 1998 and 2007 [18], and in Norway (2009–2015) both antidepressant and conversation-based therapies were similarly common, with only a slight female predominance in the latter [20].
A strength of this study is the reliable longitudinal registry data, which are comprehensive concerning medicine purchases and Kela’s rehabilitation services. However, our data lacked information on the other therapies besides pharmacotherapies that are provided within healthcare without Kela’s reimbursement. Furthermore, our data are restricted to those applying for disability pension from Kela and do not include those having the best pension accrual who are in a position to apply for disability pension only from the earnings-related pension scheme. Therefore, our data do not contain information on the vocational rehabilitation covered by earnings-related pensions either. This restricts the generalisation of our results to all applicants for disability pensions due to depression. Some applicants may be entitled to Kela’s pension in addition to their earnings-related pension if the earnings-related pension is small. They may be entitled to vocational rehabilitation through their employment insurance company, but we lack these data. This may affect the lower proportion of those who have received vocational rehabilitation among people aged 40 and over.
For each calendar year, this study focused on new disability pension applicants who had not received disability pension during the preceding year, therefore having had approximately 1 year for treatment during the sickness allowance period. However, there may be some heterogeneity in this respect, as some may have had sickness allowance days due to other diseases and therefore a shorter period of depression before applying for disability pension. Furthermore, some applicants may already have had sickness allowance or disability pension periods due to depression in previous years.
The results of this study highlight the need for focusing efforts on the effective treatment of depressed individuals who are incapable of working. Among applicants for disability pension due to depression, the proportion of individuals purchasing antidepressants had slightly decreased, even though the use of antidepressants has increased in the general population [15], new antidepressant molecules have become available, and the prices of older medications have decreased following patent expirations. The congestion of the Finnish health service system, particularly in psychiatric services, may partly contribute to this background. However, to certify disability, applicants for disability pension must have already been under a doctor’s care during the sickness allowance period. Assessment of implemented treatment, rehabilitation, and related plans, as well as the need for rehabilitation, is also carried out when processing disability pension applications and also during the sickness allowance period.
This study does not reveal to what extent deficiencies in treatment are due to a lack of treatment being offered and to what extent they are due to barriers to attending treatment. In healthcare, individuals’ needs may be inadequately identified, and there can be multiple barriers to receiving and engaging in treatment, such as financial, social or illness-related factors. In the case of rehabilitative psychotherapy and newer medications, the out-of-pocket costs can be substantial, potentially affecting the ability to access care particularly in the studied group.
The subjective right to Kela’s psychotherapies, implemented in 2011, has not increased the use of psychotherapies among applicants for disability pension due to depression as much as might be presumed based on the statistics from the general population. Therefore, the availability of psychotherapies should be secured for persons with problems related to work ability. Persons outside of the workforce do not have access to occupational health services, nor do they have similar requirements to provide an assessment of their potential to continue working, as those in the workforce have had since 2012. Therefore, sufficient support for work capacity should be available to all working-age persons. Lost work capacity is a tragedy from both individual and societal perspectives and, therefore, worth preventing through timely and evolving treatment and rehabilitation efforts.
In future research, qualitative methods are needed to more profoundly understand the reasons behind the insufficient realisation of treatment and rehabilitation year after year.
Conclusions
Compared to previous years, a larger proportion of individuals applying for disability pension due to depression has received psychotherapy and vocational rehabilitation. However, treatment and rehabilitation remain inadequate for the majority, as most receive only pharmacological therapy. There are differences in the implementation of treatment and rehabilitation between age groups and sexes, particularly in psychotherapy, which has been most frequently utilised by young females.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261422954 – Supplemental material for Trends in depression treatment of persons applying for disability pension due to depression: a register-based retrospective study from Finland
Supplemental material, sj-docx-1-sjp-10.1177_14034948261422954 for Trends in depression treatment of persons applying for disability pension due to depression: a register-based retrospective study from Finland by Tero Kujanpää, Sauli Jäppinen, Kirsi Suominen, Veera Pohjolainen and Riitta Luoto in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.