
Abstract
Aim:
To identify effective interventions designed to improve work ability and reduce early exit from the labor market of midlife and older workers.
Method:
Searches were conducted in PubMed, Cochrane Library, Scopus, Web of Science, and PsycInfo up to February 17, 2025, focusing on studies aimed at improving work ability and associated conditions (work productivity, work engagement, job performance, and work capacity) and reducing early exit from the labor market among participants aged ⩾40 years. Two reviewers evaluated the quality of studies. The effectiveness of interventions was evaluated using meta-analysis and, when not feasible, qualitative synthesis.
Results:
Of 17,505 publications, 41 studies were included, comprising 14 randomized controlled trials (RCTs, n = 4123) and 27 non-randomized studies (n = 4,616,452). Meta-analysis of RCTs showed that aerobic or strengthening exercises modestly improved work ability (pooled standardized mean difference 0.26, 95% CI 0.08–0.44). Qualitative synthesis indicated cognitive behavioral therapy (CBT) reduced productivity loss in workers with chronic health conditions. A meta-analysis of non-randomized studies showed policy reforms raising the eligible retirement age increased employment by 12 percentage points (pps) (95% CI 7–17) and decreased retirement by 29 pps (95% CI 8−50), but increased disability benefits by 6 pps (95% CI 1–11), unemployment by 7 pps (95% CI 2–12), and economic inactivity by 6 pps (95% CI 5–8). Policy reforms tightening unemployment benefit requirements increased employment and reduced unemployment, but increased disability benefits.
Conclusions:
Background
The aging workforce in many Western countries, coupled with declining fertility rates, pose challenges to labor availability [1]. In 2022, workers aged 45 to 64 constituted 41% of the OECD (Organisation for Economic Co-operation and Development) workforce, and by 2050, one in six workers on average is expected to be aged over 65 [1]. This demographic shift will result in a workforce increasingly composed of mid-career and older workers [1], whose health, functioning, and work ability might deteriorate with age [2, 3]. However, good perceived work ability has been found to be associated with extended employment beyond statutory retirement age [4]. These statistics and research results underscore the need to support the aging workforce’s work ability and prevent early exit from the labor market.
The labor shortage caused by shifts in population age structure and increased life expectancy has led several countries to raise the retirement age to address such workforce challenges [5 -8]. Beyond such regulatory measures aimed at extending working careers, it is essential to implement interventions at both individual and organizational levels to enhance work ability, enabling individuals to remain in the workforce longer [9]. By promoting healthy aging, providing opportunities for skill development [10], and making necessary work modifications, these interventions and policies could help mitigate the challenges for labor markets and public health posed by an aging workforce. Addressing these needs allows older workers to stay productive and engaged, benefiting both individuals and society.
To the best of our knowledge, three previous systematic reviews have evaluated interventions aimed at improving work ability or associated conditions and reducing early exit from the labor market among midlife and older workers [11 -13]. A systematic review of 18 studies found no effect of workplace health promotion on work ability, productivity, or job retention for older workers [11]. Another systematic review, which included two randomized controlled trials (RCTs) and three non-randomized studies among postmenopausal women, found that self-help cognitive behavioral therapy (CBT) reduced presenteeism and improved work adjustment [12]. A third systematic review of three RCTs and one quasi-experiment study showed a small beneficial effect of multicomponent workplace interventions in reducing early retirement [13]. However, these reviews did not provide convincing evidence of the effectiveness of interventions, due to the small number of included studies, their small sample sizes, and varying study designs [11 -13].
Despite the importance of the subject, currently there is no clear consensus on effective interventions to help aging workers maintain their work ability and remain in the workforce longer. While previous reviews have focused on either a specific target group [12] or intervention type [11 -13], there remains a significant gap in comprehensive information on different strategies aimed at extending the working careers of aging workers. This systematic review and meta-analysis aimed to identify RCTs and non-randomized studies to evaluate the effectiveness of any type of intervention designed to improve work ability and associated conditions (work productivity, work engagement, job performance, and work capacity), and to reduce early exit from the labor market among workers aged 40 years or older.
Methods
The review protocol was developed in accordance with the PRISMA statement [14]. It is registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration ID CRD42024605646.
Inclusion and exclusion criteria
This review included RCTs and non-randomized studies targeting individuals aged between 40 and 64. Eligible studies had either active or passive control groups, with at least 10 participants per group. These studies examined the effectiveness of any type of intervention (such as individual or workplace interventions or policy changes) in improving work ability, work productivity, work engagement, job performance, and work capacity, as well as reducing early exit from the labor market.
Search strategy
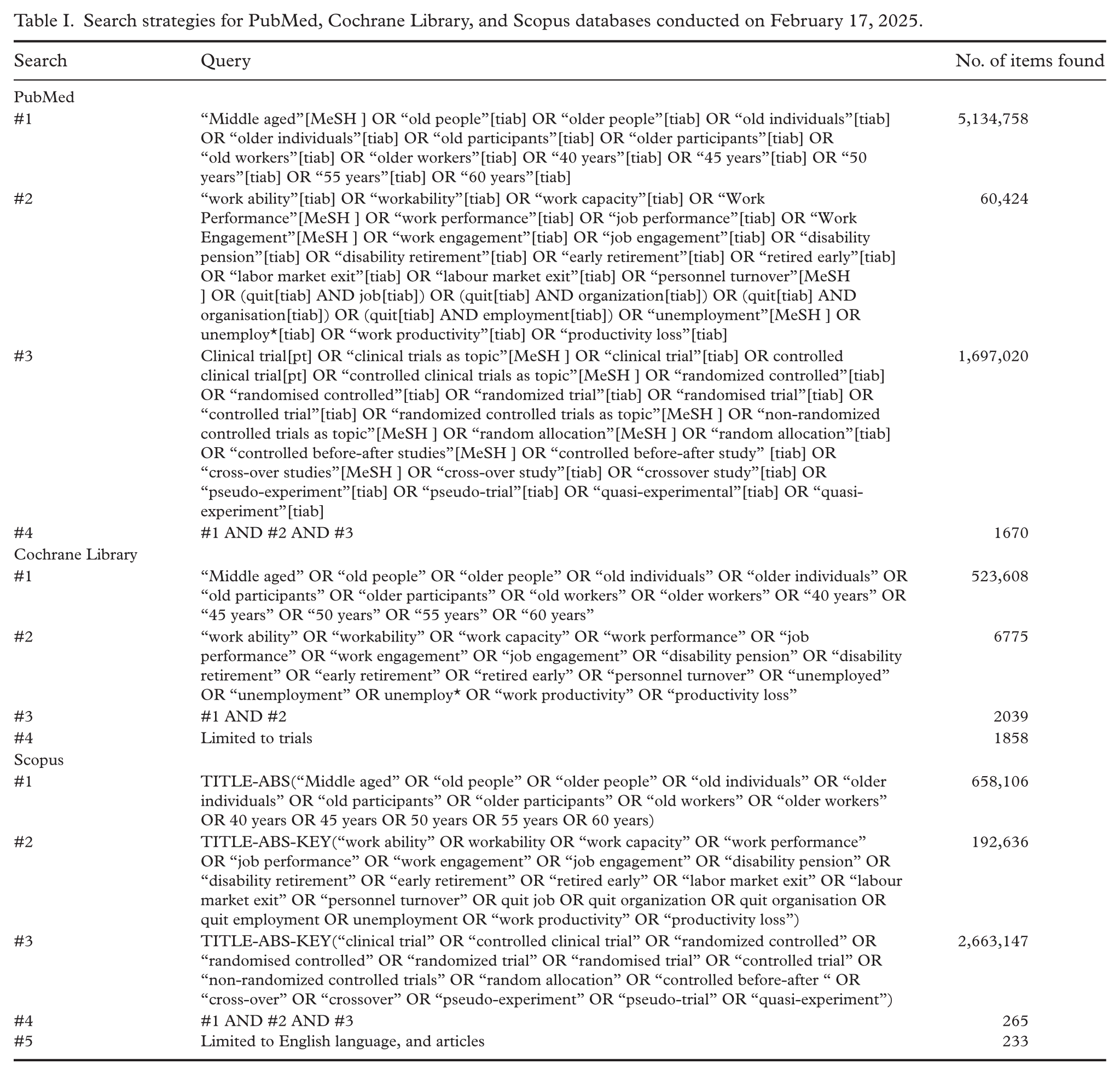
The primary literature search was conducted in PubMed, Cochrane Library, Scopus, and Web of Science databases from their inception until February 17, 2025. The search strategy combined MeSH terms and text words, as detailed in Table I and Supplementary Table S1. Furthermore, we expanded our search to include Google Scholar. To avoid missing relevant studies, we focused on “P” (Participants: middle aged) and “O” (Outcomes: work ability and associated outcomes, and early exit from the labor market) from the PICOTS (Participants, Interventions, Comparisons, Outcomes, Types of studies or Timeframe, Setting) framework. Searches were limited to RCTs and non-randomized studies. In addition, we conducted a separate literature search for observational studies analyzed as natural or quasi-experiments. The detailed search strategy for observational studies is reported in other systematic reviews [15, 16]. These publications were screened for any possible natural or quasi-experimental studies related to early exit from the labor market.
Search strategies for PubMed, Cochrane Library, and Scopus databases conducted on February 17, 2025.
Quality assessment
Two reviewers (JP and RS) independently evaluated the methodological quality of the studies. The Cochrane Risk of Bias Tool (RoB 2) for RCTs and the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) were used for the quality assessment [17, 18]. The evaluation of RCTs focused on five sources of bias: (1) the randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) the selection of the reported results [18]. The evaluation of non-randomized studies focused on seven sources of bias: (1) confounding, (2) selection of participants, (3) classification of interventions, (4) deviations from intended intervention, (5) missing data, (6) measurement of outcomes, and (7) the selection of the reported results [17]. Any discrepancies between the reviewers were settled through discussion. Assessment of methodological quality of the studies is presented in Supplementary Tables S4 and S5.
Data extraction
For the primary search of RCTs and non-randomized studies, all identified citations were exported into EndNote software and duplications were removed using an automation tool. Two reviewers (JP and RS) independently screened the titles, abstracts, and full texts for eligibility. For the searches of observational studies on early exit from the labor market, one reviewer (RS) screened the titles and abstracts. After the study selection, two reviewers (JP and RS) extracted relevant data from all included studies into a predefined table. The content of data included first author and year of publication, country, study population, follow-up time, age at baseline, sex, sample size (intervention, control, total), intervention (type, frequency, duration, and place), control group, outcome, results, difference in baseline characteristics, and adjustment for confounding factors for non-randomized studies. Any discrepancies between the reviewers were settled through discussion. We contacted the corresponding authors of three studies to provide us with confidence intervals or standard errors for their estimates, but we did not receive the required data [6, 8, 19].
Data synthesis
We estimated the standardized mean difference (Cohen’s d) by dividing the difference between the mean work ability of the intervention and control groups by their pooled standard deviation. For two trials, where mean work ability differed between the intervention and control groups at the start of the trial, we estimated the difference in the change in work ability from baseline to follow-up [20, 21]. For one study that did not report a confidence interval for the standardized mean difference [22], we calculated the standard error (SE) using the formula from the book [23]. We then calculated Hedges’ g to correct for small‑sample bias [23]. One trial [21] reported the 95% confidence interval (CI) for the mean value instead of the standard deviation. We used the formula suggested by the Cochrane Collaboration for small trials using the t distribution: SD = Sqrt(N) × (upper limit – lower limit)/t distribution [24].
To combine subgroups within a single study, we employed a fixed-effects meta-analysis. For synthesizing the results from multiple studies, we utilized a random-effects meta-analysis based on restricted maximum likelihood. To investigate publication bias, we created a funnel plot and used Egger’s regression test to evaluate its asymmetry. Furthermore, the trim-and-fill method was implemented to estimate the number of potentially missing studies due to publication bias.
Results not included in the meta-analysis were synthesized qualitatively due to the heterogeneity in the outcomes and interventions. Results were categorized by the following outcomes: (1) work ability, (2) productivity loss, (3) work engagement, job performance, and work capacity, and (4) early exit from the labor market. Studies were included in one or more categories based on their reported outcomes.
Results
The database searches and identification of studies are presented in a flowchart (Figure 1). The searches conducted in PubMed, Web of Science, Cohcrane Library, Scopus, and PsycInfo resulted in a total of 16,905 reports. In addition, the first 200 results from three Google Scholar searches were screened, amounting to a total of 17,505 reports. After excluding duplicates and ineligible reports based on titles and abstracts, 1151 full-text reports were assessed for eligibility and the final number included in the review was 43 publications (41 studies) (Supplementary Tables S2 and S3). The results of one RCT were detailed across three distinct reports. Among the included studies, 21 were natural experiment studies, 14 were RCTs (including one cluster RCT), five were quasi-experiment studies and one was pretest–posttest study.
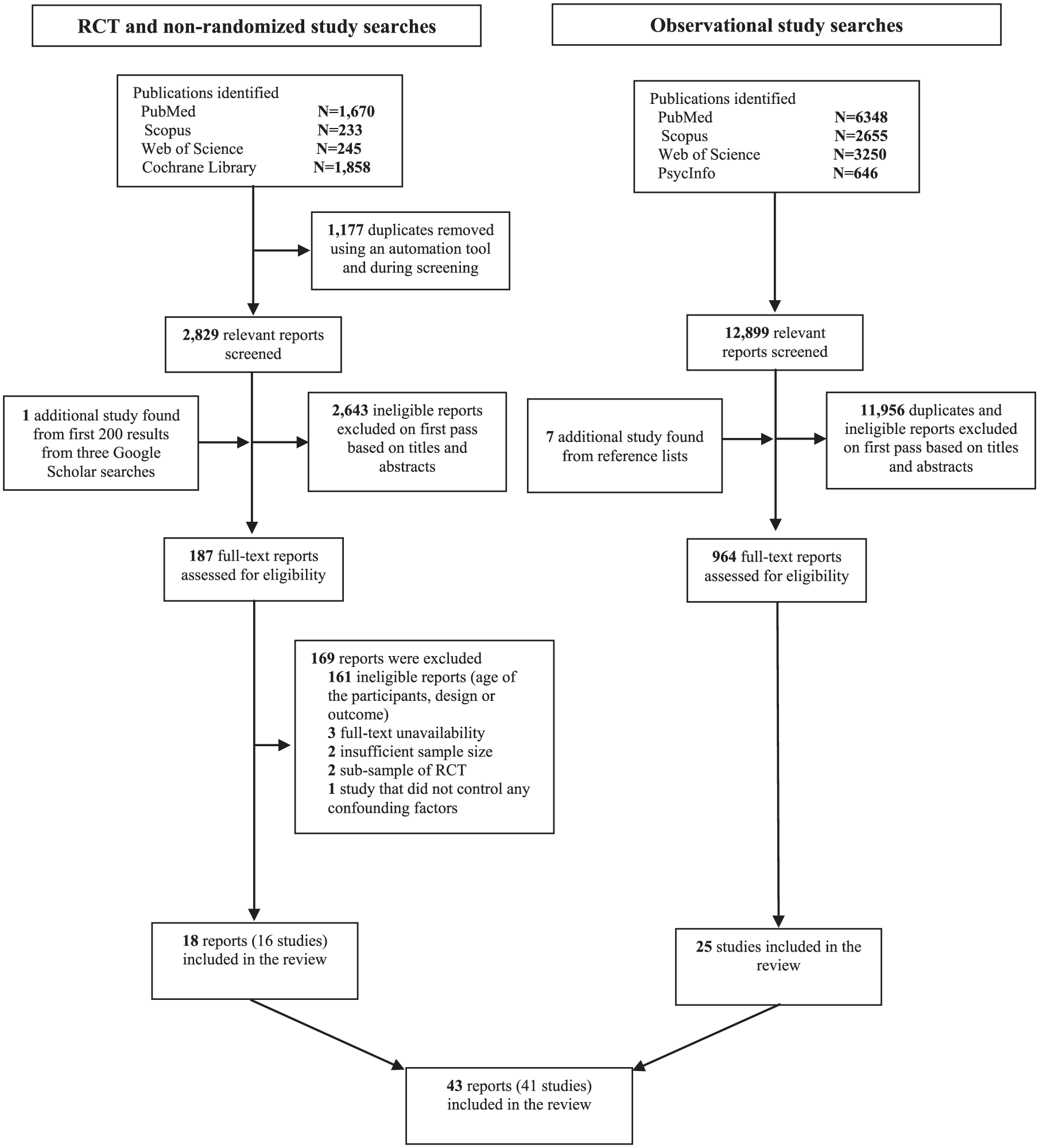
PRISMA flow diagram of the RCT and non-randomized study, and observational study selection.
Fourteen RCT studies (16 reports) included 4123 participants (range: 24 to 677), and 20 non-randomized studies involved 4,119,128 participants (range: 70 to 2,475,923). In addition, seven non-randomized studies reported only the number of observations or spells (such as unemployment spells) (total n = 497,324) instead of participants. Some studies included a small fraction of participants older than 64 years, which were not excluded from the review. The studies were published between 2004 and 2023. Geographically, seven studies were conducted in the Netherlands [25 -31], six in Finland [32 -37], five in Germany [20, 38 -41], four in the United States [42 -45], three each in Norway [46 -48] and Australia [8, 49, 50], two each in Austria [5, 51], France [7, 52], and Italy [6, 19], and one each in Spain [53], Denmark [21], Canada [22], the United Kingdom [54], Turkey [55], Switzerland [56] and Romania [57]. Among the RCTs, six reports had a moderate risk of bias, while 10 had a high risk of bias (Supplementary Table S4). For non-randomized studies, 22 had a low risk of bias, and five had a high risk of bias (Supplementary Table S5).
Work ability
Work ability was assessed in nine RCTs (11 reports) and in two non-randomized studies. Most studied interventions included aerobic or strengthening exercises (four studies, six reports) [20 -22, 34, 58, 59]. A meta-analysis of these four RCTs [20 -22, 34] (n = 466) indicated that aerobic or strengthening exercises had modest beneficial effects on perceived work ability (pooled standardized mean difference, 0.26, 95% CI 0.88–0.44) (Figure 2a), with no evidence of publication bias (p = 0.31). Two RCTs [20, 34] (n = 386) used the Work Ability Index (WAI), and a meta-analysis of these trials showed a 1.36 unit (95% CI 0.07–2.65) higher work ability in the intervention group compared to the control group (Figure 2b). Two reports [58, 59], not included in the meta-analysis, found no long-term effects of aerobic exercise on work ability at 2-year [58] and 4-year follow-up [59]. These reports had a high risk of bias due to incomplete data, as they included only participants without missing data.
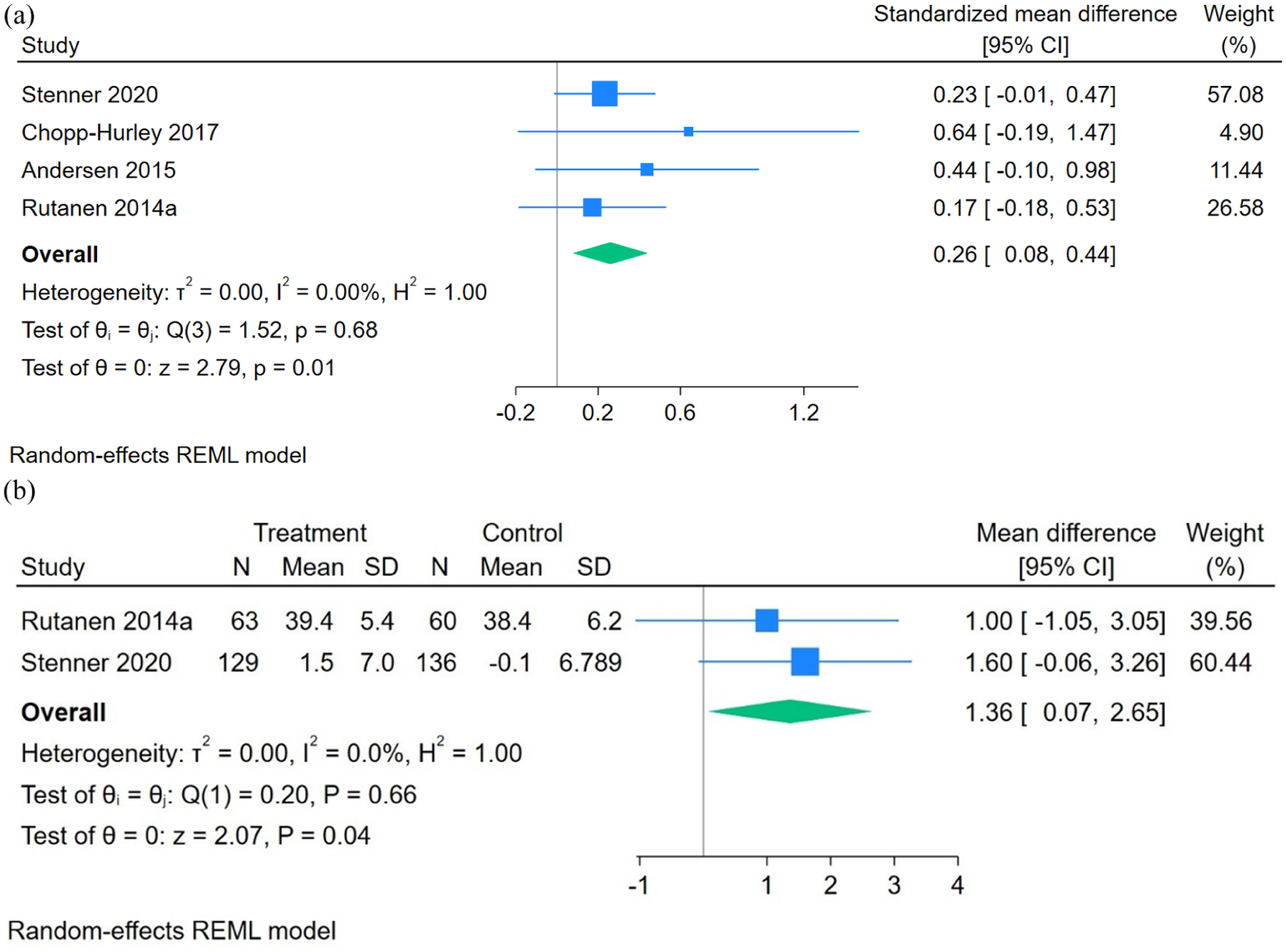
Meta-analysis of studies on the effect of physical activity interventions on work ability: (a) standardized mean difference; (b) mean difference.
Three studies evaluated multicomponent health promotion interventions [27, 30, 55]. An RCT found that a self-management health promotion program including health training, yoga, and nutrition counseling significantly improved nurses’ work ability (mean WAI score difference of 2.7 ± 3.5, p = 0.001) over 3 months [55]. A pretest–posttest study [30] found a program with menopause consultations, work-life coaching, and exercise had a marginal effect on current work ability (p = 0.072). A cluster RCT compared extended lifestyle coaching (additional seven individual sessions with an occupational health physician) to limited lifestyle coaching (web-based health risk assessment, health promotion suggestions, and a newsletter with healthy lifestyle tips) [27]. No significant difference in current work ability was found between the groups. A high dropout rate may have biased the results.
Several other studies examined the effectiveness of specific interventions not classified previously on work ability. An RCT evaluated an occupational health program, including identification of factors affecting the employee’s ability to work until retirement and the creation of an action plan [25]. The intervention group had better work ability compared to the control group at 6 months (mean WAI scores: 35.2 vs. 30.7, p < 0.001), but no difference was found at 2 years. The study had a high dropout rate at 2 years, potentially biasing the results. Morelock et al. found that a time and place management intervention, including a learning module for managers and employees, improved work ability, particularly for older workers with low baseline work ability [43]. However, the study had several limitations, including a high dropout rate. A pseudo-experiment study [35] found that participatory working time scheduling software, which allowed employees to choose their work shifts, had no effect on work ability compared to traditional scheduling by the head nurse. An RCT [37] evaluating a 16-h group-based training course on late-career management, self-efficacy, and seniority skills found no effect on work ability.
Productivity loss
Productivity loss was assessed in seven RCTs [21, 26, 27, 42, 44, 45, 49]. Three trials evaluated interventions including CBT [42, 44, 45]. Lerner et al. [42] found that a work-focused CBT, care coordination, and work coaching and modification significantly reduced at-work productivity loss in patients with depression over 4 months (mean difference: −3.2, 95% CI −4.2 to −2.3, on a 0−25 scale). Another RCT [45] showed that 6 weeks of CBT for insomnia or 2 weeks of sleep restriction therapy reduced productivity loss at postintervention and 6-month follow-up, compared to sleep education alone. The third RCT found that self-help CBT including psychoeducation about menopause, stress management, and relaxation techniques reduced productivity loss at 20 weeks (Cohen’s d = 0.65, p = 0.001) [44]. However, the trial had a high dropout rate, especially in the intervention group (28.3% vs. 7.8% in the control group).
Other RCTs evaluated multicomponent health promotion programs [26, 27, 49] and an exercise program [21]. A telehealth exercise program, with or without dietary weight loss, significantly improved perceived productivity at 12-months in overweight or obese individuals with knee osteoarthritis, though employment status and hours worked remained unchanged [49]. Two other multicomponent health promotion programs showed no beneficial effects on productivity [26, 27]. An RCT found that adding sessions with an occupational health physician to limited lifestyle coaching did not reduce productivity loss [27]. An intervention including lifestyle guidance, yoga, and aerobic exercise did not improve productivity, possibly due to a ceiling effect and low compliance [26]. A exercise intervention had no effect on productivity among healthcare workers with musculoskeletal pain [21].
Work engagement, job performance, and work capacity
Work engagement was evaluated in two RCTs [26, 37], job performance in one RCT [44] and in one pretest–posttest study [30], and work capacity in one pretest–posttest study [30]. Vuori et al. found that 16 h of group-based training on late-career management had minimal positive effect on work engagement at 6 months (Cohen’s d = 0.12, p < 0.05) [37]. Another RCT found no benefits of a health promotion intervention that included lifestyle guidance, yoga, and aerobic exercise on work engagement [26]. Self-help CBT had no effect on job performance [44]. Similarly, a health promotion program for women in low-paid jobs showed no effect on work performance or work capacity [30].
Early exit from the labor market
There were 25 non-randomized studies and one RCT that included outcomes related to early exit from the labor market. Most studies evaluated the raise of the retirement age (10 studies) [5 -8, 19, 38, 41, 50, 52, 54]. A meta-analysis of six non-randomized studies [5, 7, 41, 50, 52, 54] (n = 1,028,645) indicated that raising the retirement age increased employment among affected individuals by 12.3 percentage points (pps) (95% CI 7.2−17.4) (Figure 3a). There was no publication bias and the p-value for Egger’s test was non-significant (p = 0.46). However, the trim-and-fill method imputed two missing studies, reducing the pooled estimate from 12.3 pps (95% CI: 7.2−17.4) to 9.2 pps (95% CI: 3.2−15.2) (Supplementary Figure 1). A meta-analysis of three studies [7, 41, 54] (n = 80,262) showed that the reforms decreased retirement by 29.0 pps (95% CI 8.3−49.6) (Figure 3b). In a meta-analysis of six studies [5, 7, 8, 41, 50, 54] (n = 1,036,100), the reform increased disability benefits by 6.1 pps (95% CI 1.2−11.0, Figure 4). In addition, unemployment increased by 7.2 pps (95% CI 2.5−12.0, Figure 4) in a meta-anlysis of five studies [5, 7, 8, 41, 54] (n = 1,027,187). Lastly, economic inactivity increased by 6.2 pps (95% CI 4.8−7.5, Figure 4) in a meta-analysis of three studies [7, 41, 52] (n = 23,308). There was no evidence of publication bias in any of the latter four outcomes.
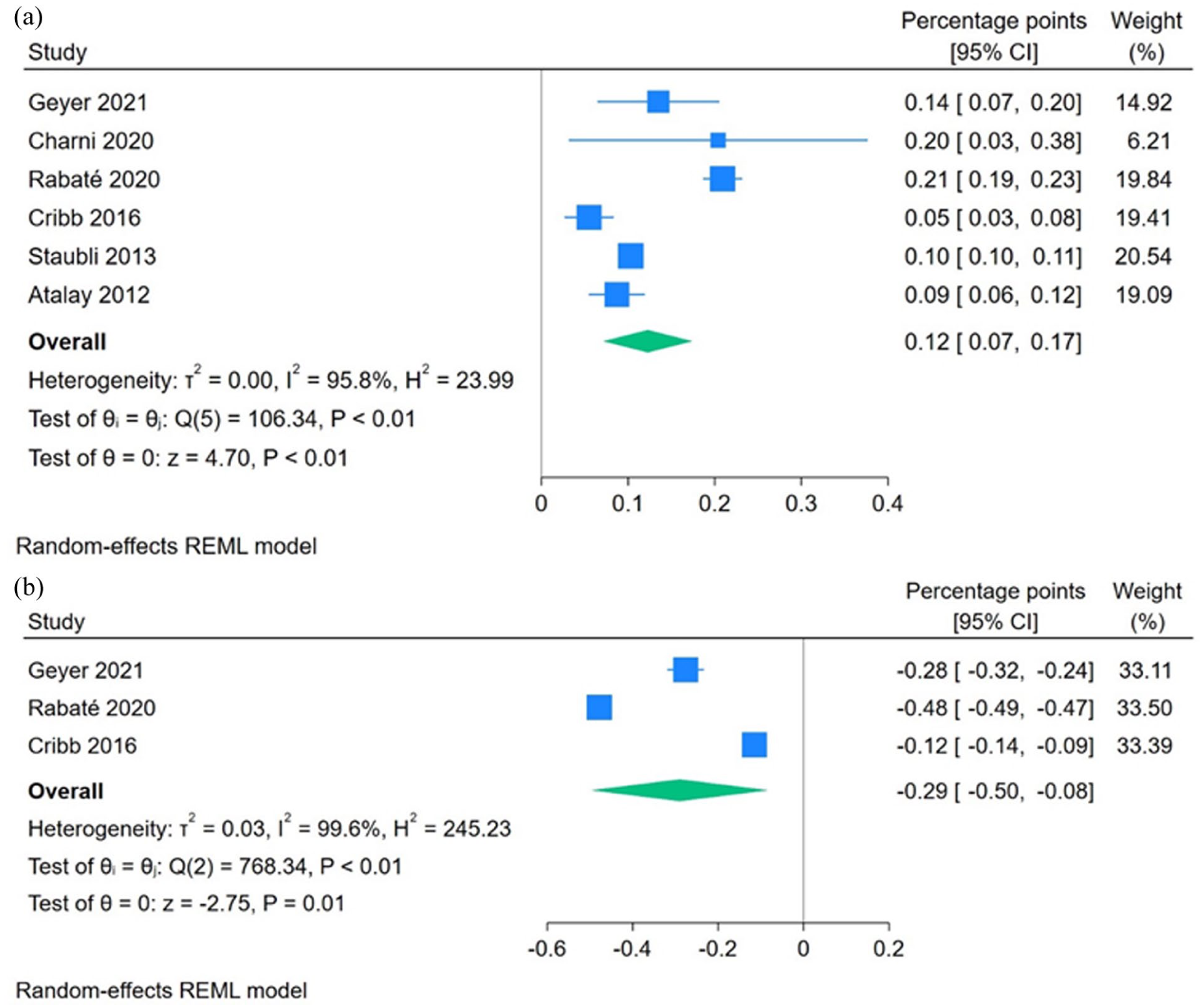
Meta-analysis of studies on the effect of raising the eligible retirement age on: (a) employment; (b) retirement.
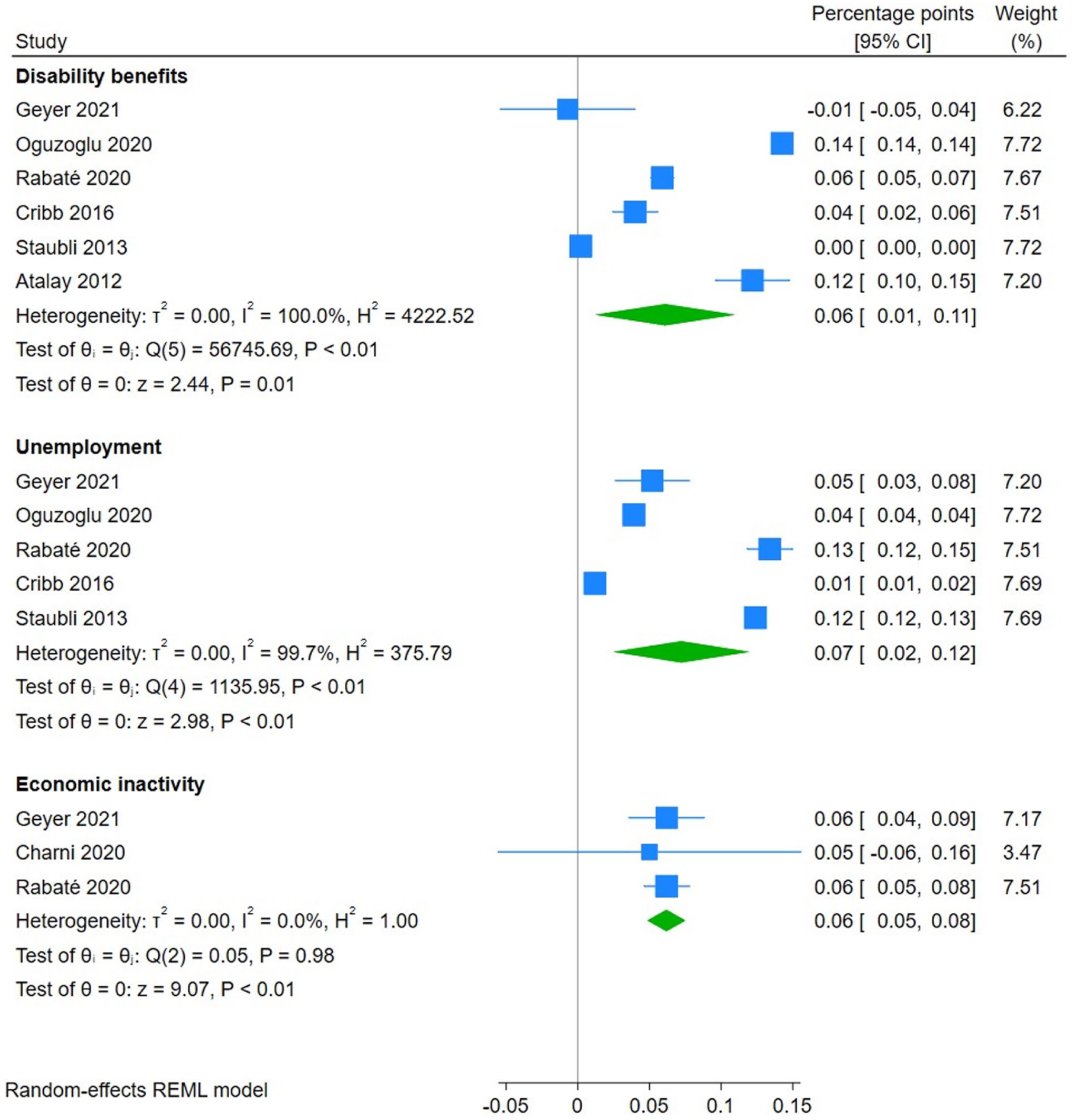
Meta-analysis of studies on the effect of raising the eligible retirement age on disability benefits, unemployment, and economic inactivity.
In addition, four studies [6, 8, 19, 38] not included in the meta-analysis on raising the retirement age due to missing required data showed similar results. Australia’s 1993 reform [8], which gradually raised women’s public pension eligibility age from 60 to 65 led to a 51.9 pp reduction in pension claims. Germany’s reforms in 1992, 1999, and 2001 gradually closed early retirement paths, raised the retirement age, increased penalties for early withdrawal from employment, and reduced public pension benefits [38]. These reforms delayed retirement and reduced unemployment, but those who were unemployed faced pension losses. In Italy, a gradual retirement age raise from 60 to 65 years among men reduced pension claims by 44 pps and increased employment by 8.7 pps, but also increased unemployment (1.6 pps), disability benefits (4.2 pps), and inactivity (13.4 pps) especially among those in poorer health and at lower occupational grades [6]. Another of Italy’s pension reforms, implemented in 2011, abruptly raised women’s retirement age from 60 to 67 and gradually for men from 65 to 67 [19]. For women aged 61−63, the retirement rate decreased by 21−28 pps, while employment (7−15 pps), unemployment/economic inactivity (8−9 pps), and disability benefits (2 pps) increased. For men aged 65−66, retirement decreased by 21−32 pps, while unemployment/economic inactivity (5−12 pps) and disability benefits (6−8 pps) increased. Also, employment increased by 14 pps at age 66, and by 5 pps at age 67.
Seven non-randomized studies evaluated policy reforms that tightened unemployment benefit requirements [28, 29, 32, 39, 40, 53, 56]. Overall, the results indicated favorable outcomes for employment, unemployment, and earnings. The 2004 unemployment insurance reform in the Netherlands required unemployed individuals aged 57.5 to 63 to report their job search efforts to the unemployment office to avoid a temporary cut in benefits [28]. The reform increased employment rates by 6.5 pps for men and 11.1 pps for women [28]. In addition, a natural experiment study on the same reform found it increased transition from unemployment to paid employment and self-employment and reduced transitions to unemployment [29]. Germany’s 2006 unemployment benefit reform, which shortened the maximum entitlement length from 32 to 18 months led to a 0.17 pp decrease in unemployment [39]. Switzerland’s unemployment insurance reform reduced the unemployment benefit duration from 24 to 18 months for individuals under 55 and led to a rise in employment rates, while unemployment benefits and economic inactivity decreased [56]. In Finland, postponing access to extended unemployment benefits by 2 years, from age 55 to 57, increased employment duration by 7.5 months and reduced unemployment duration by 8.6 months over a 10-year follow-up period [32]. However, the study did not adequately control for confounding factors. Germany’s 2006 reform, which shortened the duration of unemployment benefit payouts for workers aged ⩾45 increased the probabilities of staying employed and being re-employed, and decreased the probabilities of remaining unemployed and entering unemployment [40]. A quasi-experiment study showed that reducing the duration of potential benefits in Spain delayed the start of unemployment insurance benefits for older workers by 1 to 3 months [53]. Despite the favorable outcomes found in several studies, one study discovered a 4.3 pp increase in disability benefits for men and a 9.1 pp increase for women [28]. However, another study did not discover negative consequences on combined sickness absence and disability benefits [32].
Several other policy reforms were evaluated in studies. Two reforms focused on retirement benefits [31, 52]. In France, increasing the required contribution years for a full pension increased employment by 16.5 pps among women, with no change among men, while exit from unemployment to inactivity increased for both genders [52]. The other study, in the Netherlands, found that while reducing early retirement benefits delayed retirement, it increased exits through disability and unemployment benefits [31]. In Norway, Hermansen et al. evaluated the impact of a retention bonus [47] and additional leave [48]. A retention bonus for employees over 62 did not influence early retirement probability, but larger bonuses were associated with reduced early retirement [47]. Additional leave for employees aged 62 was found to reduce early retirement risk [48]. A quasi-experimental study evaluated active labor market policies in Romania, including subsidies for hiring unemployed individuals over 45-years old and subsidies for employers hiring unemployed persons with only 3 years left before retirement [57]. Employment increased by 12% for those over 45, but the other intervention had unreliable results due to high early retirement rates. A natural experiment study found that a regional extended benefits program (1988–1994) in Austria led to a 15.6 pp increase in early retirement [51]. A quasi-experimental study in Finland showed that partial sickness benefits reduced the decline in work participation compared to full sickness benefits, but the study had several limitations [33]. A natural experiment study in Norway found that active workplace policies for older workers, such as adapting job content and reduced working hours was not associated with reduced early retirement [46].
In addition to policy reforms, two studies examined the impact of workplace interventions on reducing early exit from the labor market. A quasi-experimental study on a senior health promotion program found it reduced early labor market exit risk, but the study had limitations in controlling confounding factors [36]. An RCT found that early retirement was lower (11%) in the occupational health program group versus in the control group (28%), though disability retirement was higher in the intervention group [25].
Discussion
The results of this review indicate that physical activity programs can enhance the work ability of midlife and older workers, and CBT can reduce productivity loss among those with chronic health conditions, based on the RCTs. In addition to these promotive interventions, multiple observational studies demonstrated that regulatory actions, such as raising the eligible retirement age or tightening unemployment benefit requirements, reduced early exit from the labor market by increasing employment. However, most of the studies on these reforms found negative spillover effects.
Most of the included RCTs evaluated single-component interventions aimed at enhancing work ability and associated outcomes. The beneficial effects of physical activity programs on work ability were modest. Furthermore, only two studies evaluated the long-term effects but found no evidence of the effectiveness of physical activity [58, 59]. However, these studies experienced high rates of sample attrition over time. Despite the lack of high-quality studies with longer follow-ups, it can be assumed that maintaining a physically active lifestyle after the discontinuation of the intervention is crucial to preserving the positive effects on work ability [60]. One study found that the physical activity intervention benefited only individuals with poor or moderate work ability, while those with better work ability saw no change [20]. This result indicates that these interventions should be specifically targeted at those with decreased work ability. Despite the modest effects observed in this review, physical activity remains an important factor in reducing the risk of early exit from labor market [15].
This review found that CBT can reduce productivity loss among midlife and older workers with chronic health conditions. CBT, a form of psychological treatment, has been extensively studied and applied to a variety of mental health conditions. Research has demonstrated its effectiveness in reducing both absenteeism [61] and presenteeism [62]. However, CBT can be applied only for workers who suffer from specific health conditions.
In promoting work ability and preventing work disability within organizations, we found evidence on interventions targeting individuals. The most established work ability model includes individual resources, and factors related to work and the external environment [63]. Due to the multifactorial nature of work ability, health promotion or single-component interventions alone are insufficient. Interventions should also target areas such as skill development. Work-related psychosocial factors, like low job control [15, 16], lack of opportunities for skills and knowledge development [16], and high workload [16] increase the risk of early exit from the labor market among middle-aged workers. However, only a few interventions have considered work-related factors, and the results have been mixed [25, 35, 37, 43]. To effectively support aging workers, future interventions should adopt a comprehensive approach that addresses both work and organizational levels, in addition to individual-level promotion.
In addition to promotive interventions aimed at helping older workers to remain in the labor force or extend their working lives, regulatory actions are crucial for addressing workforce challenges posed by the aging population. Unlike interventions that focus on enabling participation, some of these actions impose stricter requirements on individuals when aiming to reduce early exit from the labor market. This distinction between enabling and requiring older workers to remain employed represents two different approaches to preventing early labor market exit. We found that policy reforms raising the eligible retirement age reduced early exit from the labor market by increasing employment and decreasing retirement. However, these reforms also increased disability benefits, unemployment, and economic inactivity. Moreover, one study reported that the reform led to higher rates of sick leave and hospitalizations related to mental health and injuries, particularly among individuals with low health status, suggesting that raising the retirement age might harm the more vulnerable workers [19]. Raising the retirement age reduces the early exit from the labor market of those individuals who are already employed, but might negatively affect those with poor health and weak labor market positions, as they will remain outside the labor force for longer periods [7, 41]. The results of this review also suggest that policy reforms tightening unemployment benefit requirements increased employment and decreased unemployment. However, evidence of the negative spillover effects of these reforms was mixed. One study showed that the reform also led to an increase in disability benefits [28], while another study found that postponing access to extended unemployment benefits by 2 years had no consequences on combined sickness absence and disability benefits, indicating that spillover effects into these benefit types may not be a major concern [32]. As most of the studies on policy reforms included in this review had both positive and negative consequences for labor market participation, future studies should investigate the net employment effect of these reforms to evaluate whether the benefits of the extended working careers outweigh the negative spillover effects.
Limitations of the included studies and the review
The included studies had several methodological shortcomings. Many of them did not report CIs or SEs for their estimates, preventing their inclusion in the meta-analysis. Despite contacting the corresponding authors of some of these studies for additional results, we were unsuccessful in gathering the required data. Bias due to missing outcome data was high in some of the RCTs, potentially impacting the intervention effects. Furthermore, all the RCTs relied on self-reported data, which could be influenced by participants’ knowledge of the assigned intervention. However, there are no standardized objective methods to measure outcomes like work ability. Most observational studies failed to account for potential confounding factors such as lifestyle habits and physical and psychosocial factors at work. Furthermore, some observational studies did not employ appropriate statistical methods such as difference-in-difference analysis, propensity score weighting or -matching. Lastly, studies on policy reforms did not assess the net employment effects of the reforms.
This review also had limitations. A meta-analysis of all outcomes was not feasible due to the heterogeneity in study design, diversity of populations, types and intensity of interventions, diversity of control group, and variations in the duration of follow-up periods. In addition, only studies published in English were included in this review. It is possible that some relevant studies may have been published in local language journals, which were consequently left out of this review. Furthermore, some of the included studies are relatively old and it is possible that some of the findings may no longer be fully generalizable. Nevertheless, we chose to search the literature from the earliest available records in the databases to ensure comprehensive coverage of all relevant studies. It is also important to consider that most of the studies regarding early exit from the labor market were conducted in Europe, and that interpretating and generalizing these results can therefore be challenging due to the different contexts and complex political systems.
Despite limitations, a strength of this review is the use of two comprehensive searches: one for RCTs and non-randomized studies, and another for observational studies analyzed as quasi-experiments. Our second complementary search helped us to identify many natural experiments and limit the number of missing relevant studies.
Conclusions
This systematic review and meta-analysis identified promotive interventions that improved work ability and reduced productivity loss. Future studies should examine multifaceted interventions targeting various aspects of work ability at both individual and organizational levels to better address the needs of aging workers. Regulatory actions, such as raising the retirement age and tightening the eligibility criteria for unemployment benefits, resulted in higher work participation but also led to negative spillover effects. Despite the favorable outcomes, it is essential to consider the negative consequences of these reforms, especially for vulnerable workers. Both promotive measures that enable and regulatory measures that require older workers to remain employed are likely to be necessary to address the challenges posed by the aging population.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261422934 – Supplemental material for Interventions to improve work ability and reduce early exit from the labor market: a systematic review and meta-analysis among midlife and older workers
Supplemental material, sj-docx-1-sjp-10.1177_14034948261422934 for Interventions to improve work ability and reduce early exit from the labor market: a systematic review and meta-analysis among midlife and older workers by Joonas Poutanen, Tea Lallukka, Matti Joensuu, Eija Haukka, Jenni Ervasti, Mikko Härmä and Rahman Shiri in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Finnish Work Environment Fund funded this study (grant no. 230363).
Supplemental material
Supplemental material for this article is available online.