
Abstract
Aims:
Historically, Oslo has experienced the world’s highest hip fracture incidence. Preventive measures for falls and fractures have been implemented during the last decade, which has also seen demographic and societal changes. We aimed to describe trends in incidence rates of hip fracture in older adults in Oslo during the period 2012–2022 and to examine variation by sex, age, educational level, marital status and ethnic background.
Methods:
Annually updated information for the population aged 70+ years in Oslo 2012–2022 from Statistics Norway was linked with information on hip fractures from the Norwegian Patient Registry. Age-adjusted annual incidence rates by demographic characteristics were estimated using Poisson regression.
Results:
A total of 7905 hip fractures occurred in the 11-year period. Age-adjusted (95% confidence interval (CI)) incidence rates in 2012 were 106 (91, 120) per 10,000 men and 198 (183, 214) per 10,000 women. Rates declined steeply over time. The lowest rates were observed in 2020—the year characterised by reduced activity level due to strict COVID-19 restrictions. By then, incidence rates had declined by 37% (95% CI: 31, 44) since 2012. The decline was consistent across age, marital status and educational level, except for a steeper decline in women with college and university education (P = 0.021). By 2022, incidence rates had rebounded to pre-pandemic levels and were 78 (95% CI: 68, 89) per 10,000 men and 141 (95% CI: 128, 154) per 10,000 women.
Conclusions:
There was a dramatic decline in hip fracture incidence in Oslo during the last decade, which was consistent across sociodemographic subgroups.
Background
The incidence of fragility fractures is exceptionally high in Scandinavian countries [1]. The highest hip fracture rates ever reported have been seen in Oslo—the capital of Norway [1–3]. In recent decades, there has been a downward trend in age-specific hip fracture incidence in many Western countries [4,5], including Norway [6]. The decline seems to have been driven largely by temporal trends in population risk factors such as, e.g. increased body mass index and reduced smoking prevalence, while increased uptake of fracture-preventive treatment in high-risk groups appears to have contributed to a lesser degree[7]. Within the sparsely populated country of Norway, Oslo distinguishes itself in terms of population size and density as well as demographic and ethnic composition. The population of Oslo is, on average, younger than the overall population of Norway and has a higher proportion of immigrants. In Oslo, immigrants (not counting Norwegian-born with immigrant parents) comprise 26% of the total population, compared with 16% of the country as a whole. Within Norway, Oslo has had the highest age-standardised incidence rates of hip fractures, although the within-country geographic variation has diminished over time since the 1990s [8]. High-quality data on hip fractures in the Oslo population collected for one calendar year approximately 10 years apart over five decades, showed that the incidence rates have declined since the 1980s in women and since the 1990s in men [3].
Several initiatives for fall and fracture prevention in older adults have been implemented during the last decade, both on a national level and locally, including both community-based fall prevention initiatives and a large secondary fracture prevention project implementing fracture liaison services [9,10]. The city’s largest orthopaedic ward, including the Oslo Accident and Emergency Outpatient Clinic, participated in the latter. Furthermore, unanticipated changes have affected society. The population of Oslo underwent the country’s strictest COVID-19 restrictions both in spring 2020 and from November 2020 to May 2021. It has so far not been reported how these abrupt societal changes to normal daily life affected long-term trends of the older Oslo population. Hence, there is a need to examine the recent year-by-year rate of decline more closely, including the period impacted by COVID-19 restrictions, while quantifying any potential influence of sociodemographic composition that may have contributed. We aimed to describe trends in incidence rates of hip fractures in older adults (70+ years) living in Oslo during 2012–2022, and to examine the role of sex, age, educational level, marital status and ethnic background.
Methods
Study population
Individual-level information for the annually updated population of Oslo aged 70+ years by 1 January each year from 2012 to 2022 was obtained from Statistics Norway, including residence status and dates of death or emigration from the National Population Register.
Hip fractures
Information about hip fractures treated in hospitals in Norway 2012–2022 was obtained from the Norwegian Patient Registry—a mandatory national health registry containing information on all patient contacts in the specialist healthcare services [11]. In Norway, all patients with an acute hip fracture receive surgery in a public hospital. All hospital admissions that included the International Classification of Diseases, 10th edition (ICD-10) diagnosis codes S72.0, S72.1 and S72.2 were retrieved.
Relying on diagnosis codes without additional information would overestimate hip fracture incidence due to false positives at recurring visits with a previous hip fracture, while requiring the presence of surgical procedure codes would introduce false negatives and likely underestimate the true incidence. Rather, we applied a comprehensive algorithm to more precisely identify the hospitalisations that were likely to represent a newly occurred hip fracture. The algorithm considered the presence or absence of other diagnosis codes (e.g. complications, rehabilitation), surgical procedures (codes typical for a primary hip fracture surgery versus codes typical for a revision surgery) and time between hospitalisations (3-week limit). This was done to minimise overcounting of hip fracture diagnoses from readmissions while allowing up to two incident hip fractures per person over the period. The method has been described previously [6,12].
Sociodemographic characteristics
Annually updated information about sex, age, attained education level, marital status and country background (grouped by world region) was available from Statistics Norway. Educational level attained was classified according to the Norwegian Standard Classification of Education 2000 [13], and combined into three groups representing completed primary school (compulsory education, typically 8–10 years), secondary school (typically ⩾12 years) and college or university education (typically ⩾15 years). Marital status in nine categories was dichotomised into married or registered partner versus single; the latter included unmarried, separated, divorced and widowed. Country background was defined as Norway for people without an immigrant background. For people with immigrant background, country background was defined as the person’s own, parents’ or alternatively grandparents’ country of birth, following the definition by Statistics Norway (https://www.ssb.no/a/metadata/conceptvariable/vardok/1919/en). Country background was grouped into three categories: (1) Norway; (2) Europe, USA, Canada, Australia and New Zealand and (3) the rest of the world, hereafter referred to as non-Western ancestry. For visual presentation in plots of marginal effects (presented in the Supplemental material), the latter two groups were combined.
Statistical methods
The data were analysed in Stata MP version 17.0 for Windows. To obtain annual incidence rates of hip fracture, we used individual-level data on the Oslo population aged 70+ years by 1 January each calendar year in the denominator. While up to two incident hip fractures could occur in a person during the period, persons who had two hip fractures in the same calendar year were counted only once in the numerator for that year. Age-adjusted incidence rate ratios (IRRs) with 95% confidence intervals (CI) for hip fracture in each calendar year compared with 2012 were estimated in Poisson regression, entering hip fracture as the outcome variable and calendar year as a categorical explanatory variable [14]. We subsequently predicted the incidence rates with 95% CI for each respective calendar year from this Poisson model using the ‘margins’ command. Annual percent decline in incidence rates was obtained by including calendar year as a linear (continuous) variable in the Poisson model.
In addition to describing overall trends in men and women, we compared age-adjusted rates across groups of attained educational level (primary, secondary, tertiary), age (70–79, 80–89 and 90+ years), marital status (married/registered partner versus single) and country background grouped in three categories. Possibly differential rates of decline by sex, age, educational level, marital status or country background were tested by a likelihood ratio test comparing the models with and without a statistical interaction term between calendar year and the sociodemographic characteristic.
For comparison with national trends, we used readily available previously published data on national hip fracture incidence rates up to 2019, prepared using the same algorithm for hip fracture ascertainment [6]. We extracted the population size and incident hip fractures in the Norwegian population aged 70+ years for the period that overlapped between the two data sources, 2012–2019. In this comparison, age-adjusted rates for both Oslo and Norway were obtained by direct age standardisation using the sex-specific population in Norway on 1 January 2019 in 5-year age strata from 70–74 to 95+ years as standard population. The sex-specific age-standardised incidence rates with 95% CIs for 2012–2019 in Oslo and Norway (presented in the Supplemental material) were plotted using the function ‘ggplot’ in the package ‘ggplot2’ in R for Windows version 4.5.0.
Results
Study population characteristics
The population aged 70+ years in Oslo increased progressively from N = 49,145 in 2012 to N = 63,106 in 2022. In total, 98,603 people (56.7% women) entered the population during this period. Population characteristics overall and by sex in the first and final year of observation are shown in Table I. Mean (SD) age decreased from 80.0 (6.9) years in 2012 to 78.7 (6.6) years in 2022, and there was a corresponding reduction in the proportion of ‘older-old’ (aged 80 years and older). Mean age was higher in women, and the proportion of married was considerably higher in men, but in women it increased over the period. The proportion of inhabitants with non-Western ancestry increased from 4.0% to 7.6% (Table I).
Characteristics of men and women aged 70+ years residing in Oslo by 1 January 2012 and 2022.
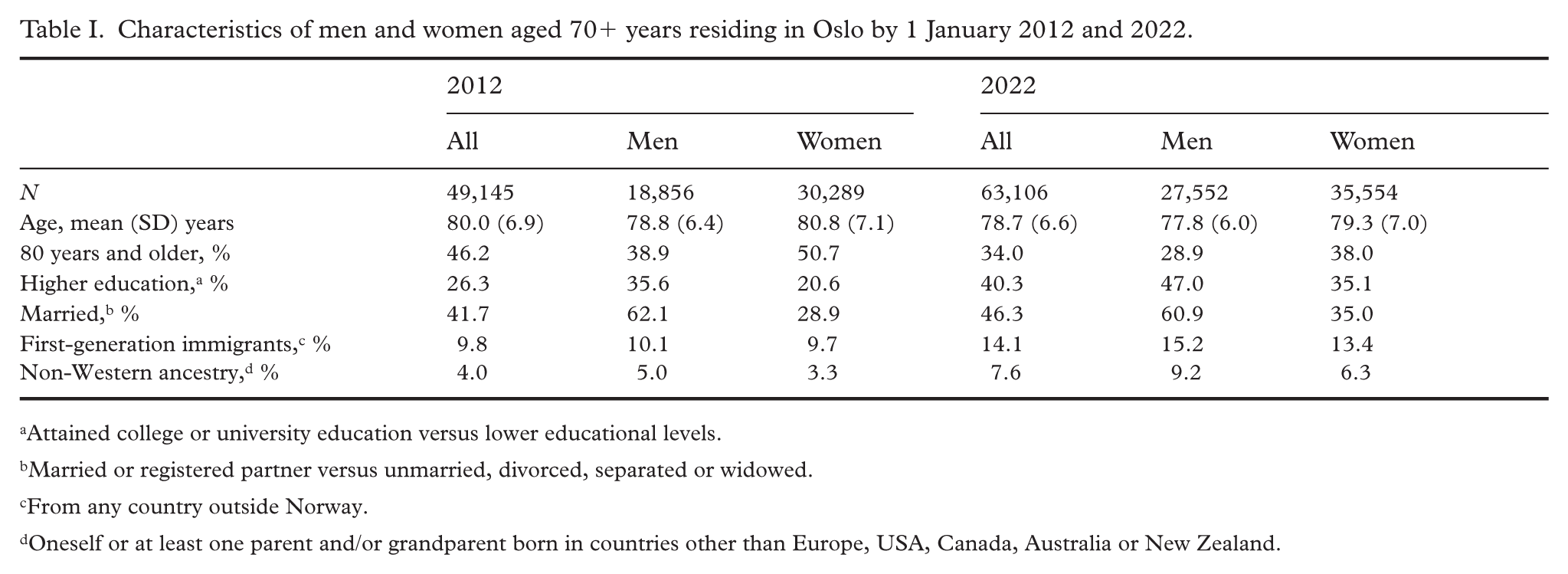
Attained college or university education versus lower educational levels.
Married or registered partner versus unmarried, divorced, separated or widowed.
From any country outside Norway.
Oneself or at least one parent and/or grandparent born in countries other than Europe, USA, Canada, Australia or New Zealand.
Incidence rates
A total of 7905 hip fractures (2227 in men and 5678 in women) occurred in the 11-year period. Overall (SD) mean age at hip fracture was 84.7 (7.1) years, and the mean age decreased slightly from 2012 to 2022: from 83.7 to 81.9 years in men, and from 85.6 years to 85.0 years in women (P < 0.001 for both sexes). Age-adjusted incidence rates with 95% CIs in men and women are shown in Figure 1 and Supplemental Table S1. The overall annual percentage decline was 4.3% (95% CI: 3.6% to 4.9%) and it was similar in men and women (P = 0.71 in likelihood ratio test). A nadir was observed in 2020, representing a clear drop compared with the previous year. By 2020, the rates had declined by 37% (95% CI: 31% to 44%) since 2012. In the subsequent 2 years, the overall rates increased by 15% (95% CI: 3% to 28%) and in 2022 the incidence rates were comparable with 2019 levels. Additional adjustment for marital status and country background yielded similar results, with only a slight attenuation of the declining trend: annual percentage decline 4.0% (95% CI: 3.2% to 4.7%) when adjusted for age, sex, marital status and country background. When comparing the rates in Oslo with national rates for the period 2012–2019, both standardised to the age distribution of the Norway population aged 70+ years by 1 January 2019 in sex- and 5-year age groups, the incidence rates in Oslo were similar to national rates in 2012 but clearly lower toward the end of the period (Supplemental Figure S1).
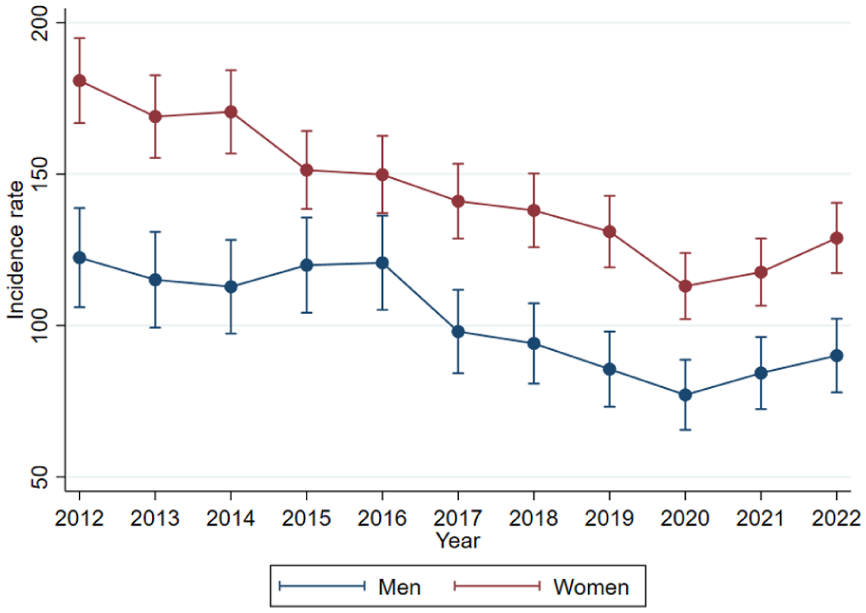
Age-adjusted annual number of hip fractures per 10,000 men and women aged 70 years and older residing in Oslo with 95% CIs, 2012–2022. Values are predicted from age adjusted Poisson regression. Direct age standardisation yielded similar results. CI, confidence interval.
Sociodemographic variation
Incidence rates were higher in women and in older age groups but, generally, the rate of decline was similar across sex and age (P = 0.71 for sex; P = 0.64 for age group). The decline was consistent across marital status and education level. While there was insufficient statistical power to appraise consistency across country background, the point estimates suggested a decline in all groups (Table II). In women, the decline tended to be steeper at younger ages (70–79 years) and in those with college and/or university education, but with overlapping CIs between subcategories of age and education (Table II). The drop in 2020 was particularly pronounced in the youngest women (70–79 years) and in women with tertiary education (Supplemental Figure S2).
Age-adjusted percent decline with 95% CIs in hip fracture incidence rates from 2012 to 2020 by sex, age, marital status, attained educational level and country background. a
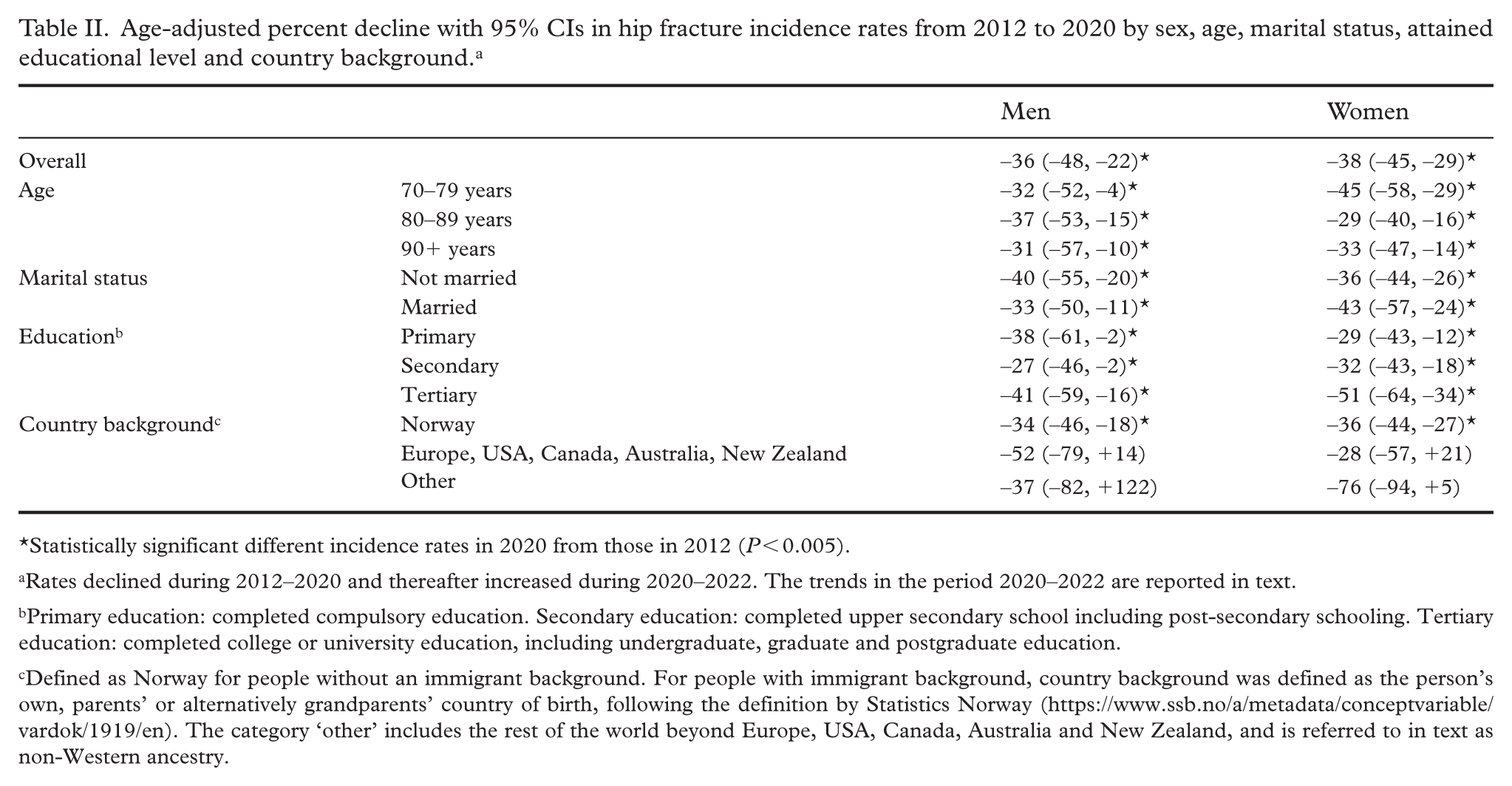
Statistically significant different incidence rates in 2020 from those in 2012 (P < 0.005).
Rates declined during 2012–2020 and thereafter increased during 2020–2022. The trends in the period 2020–2022 are reported in text.
Primary education: completed compulsory education. Secondary education: completed upper secondary school including post-secondary schooling. Tertiary education: completed college or university education, including undergraduate, graduate and postgraduate education.
Defined as Norway for people without an immigrant background. For people with immigrant background, country background was defined as the person’s own, parents’ or alternatively grandparents’ country of birth, following the definition by Statistics Norway (https://www.ssb.no/a/metadata/conceptvariable/vardok/1919/en). The category ‘other’ includes the rest of the world beyond Europe, USA, Canada, Australia and New Zealand, and is referred to in text as non-Western ancestry.
The annual age-adjusted incidence rates of hip fracture in 2012 through 2022 by groups of age, marital status, country background and educational level attained are shown in Supplemental Figure S2. Regarding marital status, the incidence of hip fracture was lower in married people, while the rate of decline did not differ by marital status (P = 0.31). Regarding country background, incidence rates were highest in people with Norwegian background and lowest in people with non-Western ancestry, while the incidence rates in people with background from Europe, USA, Canada, Australia and New Zealand were in between. There was a clear educational gradient with lower incidence rates throughout the period in people with tertiary education. The diverging trends by educational level was statistically significant in women (P = 0.021) but not in men (P = 0.57). In women, annual percentage decline was 3.0% (95% CI: 1.5%, 4.4%) in those with primary education only and 5.6% (95% CI: 3.8%, 7.4%) in those with tertiary education.
Discussion
In this open cohort study of all inhabitants 70 years and older in Oslo during 2012–2022, including both home-dwelling older adults and nursing home residents, we described the time trends in incidence rates of hip fractures during 2012–2022 across sex, age, educational level, marital status and ethnic background. We are not aware of any similar reports published from other Scandinavian countries. We observed a sharp decline in incidence rates of hip fracture in this period. Compared with national trends in Norway, the decline up to year 2019 was considerably steeper than that observed for the country as a whole in the corresponding period. There was a particular drop in the pandemic year 2020, and this was observed most notably in women with higher education. Oslo saw two extensive periods with limited activity level, and the corresponding drop in fracture rates is likely a consequence of the reduction in normal daily-life activities outside the home, limiting exposure to falls, which is expected to affect the more active ‘younger-old’. By 2022, the incidence rates had rebounded to pre-pandemic levels.
Located at 60°N, Oslo is the capital and largest city of Norway—a long-stretched sparsely populated country with currently 5.5 million inhabitants, of whom just over 700,000 (13%) live in Oslo. The Oslo population aged 70 years and older currently comprises 9% of the age 70+ population of Norway (https://www.ssb.no/en/befolkning/folketall). Oslo has previously had the highest observed incidence rates of hip fracture globally [15], with higher rates than other, less urban, areas in Norway [8].
Influence of sociodemographic factors
The rate of decline was consistent across subgroups of sex, age, marital status and education level. The strong decline seen also in the ‘oldest-old’ is notable and suggests that hip fractures have been prevented successfully across all age groups rather than merely postponed until older age.
Women with tertiary education exhibited the largest decline from 2012 to 2020, but with overlapping CI with lower education groups.
There have been changes over time in ethnic composition, with increasing proportions of people with immigrant background among the older population. A lower risk of hip fracture has been observed among immigrant groups from non-Western countries [16]. In the older Oslo population, the proportion with country background other than Europe, USA, Canada, Australia or New Zealand, was modest but increased from 4.0% to 7.6% during the study period. Accounting for the population’s composition of country background attenuated the overall observed rate of decline only slightly during the period, from an annual percent change of 4.3% to 4.0%.
Drivers of declining trends
As discussed by others [3], it is plausible that the declining fracture risk observed is a result of several coinciding changes in the population. It may be attributable partly to secular trends in population factors with a fracture-protective influence, such as increasing body mass index, reduced smoking prevalence and increased physical activity [7].
Healthcare interventions
Several initiatives with specific attention to fall and fracture prevention directed toward the older Oslo population have been implemented in the period. The municipality of Oslo has offered the ‘Strong and Steady’ program since 2016. This is a national structured fall-preventive group exercise program for home-dwelling older adults, targeting balance, muscle strength, mobility and endurance [17,18]. The program is based on the Otago Exercise Program and the Falls Management Exercise (FaME) Program, respectively, which have both been shown effective in preventing falls among home-dwelling older adults [19,20]. At the same time, a collaboration has been carried out between the Oslo Accident and Emergency Outpatient Clinic and municipal primary healthcare locally, to intensify fall-preventive interventions for older adults who present with a fall injury, improving the pathways of care between primary and specialist healthcare [21]. The Norwegian Capture the Fracture Initiative (NoFRACT)—a multicentre secondary prevention study offering fracture liaison services to patients aged 50 years and older with fractures [10]—was introduced in 2015 in the city’s largest orthopaedic ward in Oslo University Hospital, also including the Oslo Accident and Emergency Outpatient Clinic [9]. Consequently, the uptake of secondary fracture prevention with intravenous zoledronic acid has increased. Fall outpatient clinics and orthogeriatric services have emerged and, broadly, there appears to be a growing culture for sharing knowledge between the various professions and medical specialties with competence in fall and fracture prevention. Finally, the governmental Norwegian Patient Safety Strategy was introduced in 2014, aiming to reduce the risk of injuries and harm inflicted in the health and care services [22].
Societal changes
Larger unanticipated interventions have affected society in the last decade. Due to its relatively high population density and the rapid early spread of the SARS-CoV-2 virus, the population of Oslo underwent the country’s strictest lockdown restrictions both in Spring 2020 and November 2020 to May 2021, with closing of workplaces, shops and restaurants, and cultural and social arenas, including exercise offers. Consequently, the activity level was reduced among many home-dwelling older adults [23]. The coinciding drop in hip fracture rates are a likely consequence of the reduction in normal daily-life activities outside the home, limiting exposure to falls. By 2022, the incidence rates had rebounded to pre-pandemic levels. In Norway as a whole, the rate of hip fracture surgeries in those aged 70 years and older did not appear to be acutely affected by the lockdown restrictions introduced in March 2020 [24]. Notably, there was a drop in the rate of hip fracture surgeries during the first 2 weeks after lockdown, driven by reduced rates in people younger than 70 years and particularly apparent in men, which rebounded during the subsequent 2 months [24]. It is conceivable that, among the younger and more physically active older adults, reduced exposure to activity and movement outside the home due to the societal restrictions prevented some falls in the short term. However, the reduced activity level and accompanying decline in health may contribute to frailty and possibly increased fall risk in the longer term [23], and it is not known to which extent such consequences may be transitory. Monitoring future trends will therefore be important.
Strengths and limitations
Strengths of this study include the population-wide registry data covering all inhabitants, for whom data have been linked individually to outcome data in mandatory health registries based on their national personal identification number. Standardised and objective sociodemographic information for all inhabitants is available. The outcome data have been validated and are comparable with other publications presenting national data on hip fracture incidence [6,12]. A limitation is the broad grouping of country background (world region). However, the relatively low numbers of hip fractures among immigrant groups would hardly have allowed for more granular comparisons across groups.
In our analysis, the study population aged 70 years and older residing in Oslo was updated each year to also include people who had moved to Oslo in the previous year. However, this did not apply to the data in the years 2020–2022, solely for reasons related to data procurement. This limitation is expected to have a negligible numerical influence in the age range studied. In 2013–2019, recent citizens comprised only 0.6% to 0.8% of the study population each year.
Conclusion
There was a dramatic decline in hip fracture incidence in older men and women in Oslo during the last decade, likely resulting from a combination of changes in demographic composition, secular trends in risk factors and targeted fall- and fracture preventive initiatives both in the municipality and specialist healthcare services. The rate of decline was generally consistent across sex, age, marital status and education level. However, the decline tended to be steeper in women who were younger (aged 70–79 years) and who had attained college- and university education. By 2022, the fracture rates had rebounded to pre-pandemic levels.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261416811 – Supplemental material for Trends in hip fracture rates in Oslo 2012–2022 across sociodemographic characteristics
Supplemental material, sj-docx-1-sjp-10.1177_14034948261416811 for Trends in hip fracture rates in Oslo 2012–2022 across sociodemographic characteristics by Kristin Holvik, Ruth Aga, Anne-Johanne Søgaard and Haakon E. Meyer in Scandinavian Journal of Public Health
Footnotes
Author contributions
KH: Investigation, Formal Analysis, Visualization, Writing – Original Draft
RA: Funding acquisition, Writing – Review & Editing
AJS: Funding acquisition, Writing – Review & Editing
HEM: Conceptualization, Methodology, Funding acquisition, Project administration, Data Curation, Investigation, Formal Analysis, Visualization, Writing – Review & Editing.
Availability of data and materials
The corresponding author K.H. may be contacted for details concerning the data and materials. The registry data that support the findings of this study are available upon application to the respective data owners, but restrictions apply to the availability of these data, which were used under approval for the purpose of the current research project, and so are not publicly available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study has been funded by a grant from the Research Council of Norway (grant number 296587).
Disclaimer
Data from the Norwegian Patient Registry have been used in this publication. The interpretation and reporting of these data are the sole responsibility of the authors, and no endorsement by the Norwegian Patient Registry is intended nor should be inferred.
Ethics approval
The study and the data linkages have been approved by the Regional Committee for Medical and Health Research Ethics (REC South East A, ref 32612). The data were handled in accordance with the General Data Protection Regulation, and a Data Protection Impact Assessment has been conducted in consultation with the Data Protection Officer.
Supplemental material
Supplemental material for this article is available online.