
Abstract
Aims:
This study aimed to estimate the associations between preschool-level and individual- level socioeconomic deprivation and later mental disorders among children in a Swedish setting.
Methods:
The study used a longitudinal cohort study design including 2678 children, aged 3–5 years in Uppsala Municipality during 2017, with data on individual-level socioeconomic deprivation, and preschool-level socioeconomic deprivation. We followed the children for approximately five and a half years to assess later mental disorders, based on data from the Swedish National Patient Register. Frailty Cox regression models were used to analyse the data.
Results:
No associations were observed between preschool-level socioeconomic deprivation and subsequent mental disorders. In terms of individual-level deprivation, children whose parents had lower educational levels had a higher risk of receiving a diagnosis of any mental disorder (hazard ratio (HR: 1.40; 1.04–1.90)) and any attention deficit hyperactivity disorder or conduct disorder (HR: 1.87; 1.24–2.80) during follow-up than children whose parents had higher education levels.
Conclusions:
Keywords
Introduction
Child mental health problems represent a public health challenge. A study on school children across eight European countries showed that 22% had at least one self-reported mental disorder [1]. Internalising problems, including anxiety and depression, were reported by one in five children, while externalising problems, including aggression, hyperactivity and conduct problems, were reported by 1 in 12 children. It is widely known that children from socioeconomically disadvantaged families are at a greater risk of developing mental health problems compared to peers from more advantaged backgrounds [2].
The preschool years, typically ages three to five, represent a critical period in child development. During this time, foundational cognitive, emotional, social, and behavioural capacities are developing, and the experiences children have in these years can have long-term effects on their well-being and life trajectories [3]. Emotional and behavioural problems including anxiety, depressive symptoms, hyperactivity, aggression, and defiance are the most common mental health problems in children attending preschool [1, 4]. In many countries including Sweden, children spend a considerable time at preschool and preschool is available during a pivotal developmental stage. The Swedish preschool system serves children aged 1–5 years and is predominantly publicly financed through municipal tax revenues, with only modest parental fees covering a small percentage of total costs. Overall, preschool constitutes an important setting for the promotion of mental health and academic outcomes – particularly for children from socioeconomically disadvantaged backgrounds [5].
Socioeconomic deprivation can be assessed at different levels, such as school or individual levels. Deprivation at the school level refers to group-based indicators, such as housing conditions, average parental educational attainment, poverty prevalence, the proportion of foreign-born students and mean school performance. In contrast, individual-level deprivation includes individual indicators such as marital status, occupation, income level and parental education level. Research has demonstrated associations between school-level deprivation factors and children’s mental health problems [6, 7]. For instance, Horoz and colleagues [6] reported that enrolment in schools characterised by higher deprivation was associated with elevated behavioural and emotional problems among students. Moreover, a large UK-based study showed that school-level deprivation factors predicted mental health outcomes in pupils, but that such factors only accounted for a modest proportion of mental health variation [7]. Additionally, associations between individual-level socioeconomic deprivation and mental health outcomes in children have been observed with low and moderate parental education levels, financial problems, unemployment and single-parenthood as the most important factors [2, 7, 8].
Altogether, socioeconomic deprivation is correlated with mental health problems during childhood. However, the extent to which measures of socioeconomic deprivation at preschool and individual levels during children’s preschool years predict future mental health problems is unclear. Investigating the relationship between preschool- and individual-level socioeconomic deprivation and later mental health problems during childhood could inform implementation of targeted socioeconomic interventions during the preschool years as a strategy for mitigating the risk of subsequent mental health problems within this population.
Aims
The purpose of this study was to estimate the associations between preschool- and individual-level socioeconomic deprivation and later mental disorders among children in a Swedish setting.
Methods
Study design
This study utilised a longitudinal cohort design, using data from the Focus study [9]. The Focus study was established to examine the health of preschool-aged children and their parents, encompassing a cohort of children aged 3 to 5 years, with data collected between 2013 and 2017 in the Uppsala region of Sweden. For the purpose of this study, the cohort was prospectively followed from 2017 to 2022 using register data on mental disorders.
Participants and procedure
Parents of all children aged 3 to 5 years were recruited to the Focus study through child health centres (CHCs) prior to their child’s annual health check-up. CHC nurses included questionnaires with the invitation letters sent to parents at the child’s registered address prior to the scheduled visits, and parents returned the completed questionnaires at the time of the check-up. In addition to Swedish, the questionnaires were available in English, Arabic, Somali and Sorani, which are the most common languages in the immigrant community in Uppsala. The questionnaires comprised items assessing individual-level socioeconomic deprivation and the Strengths and Difficulties Questionnaire (SDQ) to evaluate the child’s emotional and behavioural problems [10]. Moreover, the Socioeconomic Structure Compensation Index (SSCI) from 2017, serving as a measure of preschool-level socioeconomic deprivation, was obtained from Uppsala Municipality and follow-up data on children’s mental disorders were extracted from the Swedish National Patient Register (SNPR). For the current study, these data were integrated with the Focus study data.
Across the four study years of the Focus study, more than 28,000 sets of questionnaires were distributed to parents in the Uppsala region and in total, 9496 unique children participated in the study [11]. The participation rate varied between 45% and 51% during the study years. The participants in the current study consisted of children recruited through CHCs located in Uppsala Municipality during the year 2017. We only included children with complete data on the variables of interest from at least one parent. In cases where data were available from both parents, data from one parent was selected at random for inclusion.
Among the 9496 participants, parents of 6957 children consented to registry data linkage. Of these, 2945 children were recruited from CHCs located in Uppsala Municipality during 2017. Of these, a total of 267 children were excluded. First, 157 children who attended preschools with no SSCI scores (see below) were excluded. The reasons for the missing SSCI scores for preschools were, first, that too few children were enrolled in these preschools – since scores are only calculated for institutions with a sufficient number of enrolled children to ensure statistical stability and comparability – and second, that the scores were not available in 2017 due to changes in the municipality’s reporting routines. In addition, 93 children with no data on individual-level socioeconomic deprivation or emotional and behavioural problems, and 17 children diagnosed with a mental disorder before inclusion in the Focus study were excluded. Consequently, the final analytical sample of this study comprised 2678 unique children.
Data sources
Preschool-level socioeconomic deprivation
The questionnaire used in the Focus study [9] included a question to determine which preschool each child attended, enabling the collection of the SSCI from 2017 as a measure of preschool-level socioeconomic deprivation. The SSCI serves as a tool for Uppsala Municipality to inform and direct the equitable allocation of funding to its preschools. This allocation is determined by two main components: a standard base amount, which provides equal funding for each child, and the Socioeconomic Structure Compensation (SSC), which takes into account the socioeconomic background of the children enrolled in each preschool. The primary purpose of the SSC is to facilitate a more equitable distribution of financial resources by addressing socioeconomic disparities across preschools.
Since 2010, Uppsala Municipality has employed various structural compensation models and the most recent revision of the SSCI occurred in 2016 [12]. The SSCI is calculated annually and is derived from statistical data provided by Statistics Sweden on the socioeconomic backgrounds of parents, including variables on housing conditions, country of birth, reliance on economic support, highest attained level of education, and the Human Development Index [13]. Each of these variables is assigned a weight based on how different socioeconomic factors correlate with children’s needs, such as more frequent interaction with adults, the benefits of participating in smaller group settings, developmental considerations, as well the demands that arise in the collaboration with parents. According to the SSCI, each preschool in Uppsala Municipality is assigned an individual score (range: 32–400, Mean = 96.2, SD = 50.4). Higher scores indicate greater levels of deprivation and result in increased financial compensation.
For enhancing interpretability and comparability across participant groups, SSCI scores were first categorised into three levels of socioeconomic deprivation. Low deprivation included scores below the 75th percentile (32–112), moderate deprivation corresponded to the 75th–89th percentiles (115–157), and high deprivation encompassed scores at or above the 90th percentile (⩾159) among all preschools in Uppsala Municipality. These thresholds, established in collaboration with Uppsala Municipality, were also applied in a previous study on a similar topic [14]. However, in the current study, the original preschool-level socioeconomic deprivation variable was further collapsed into two broader categories: low deprivation vs. moderate or high deprivation, to increase the sample size within the deprivation groups and to ensure sufficient power for meaningful statistical inference. The 2678 children in the study attended 207 preschools with enrolment per preschool ranging from 1 to 56 children. Among these preschools, 156 were classified as low-deprivation preschools, and 51 were classified as moderate/high deprivation preschools.
Individual-level socioeconomic deprivation
The following variables assessing individual-level socioeconomic deprivation were included and based on self-reported data from the Focus study: parental country of birth (dichotomised as Sweden vs. outside Sweden), parental marital status (dichotomised as married/cohabiting vs. single/living apart/other) and parental educational level (dichotomised as lower level, defined as not having completed primary school, having completed primary school, or upper secondary school, vs. higher level, defined as at least 3 years of college or university education). The variable measuring parental education level was dichotomised to create groups of comparable size, given that Uppsala Municipality has a large proportion of highly educated parents. As data from only one parent were used – either the sole respondent or randomly selected when responses were available from both – the analyses were adjusted for parental sex (female or male).
Child emotional and behavioural problems
Children’s emotional and behavioural problems were evaluated using the parent-report version of the SDQ [10]. This instrument comprises 25 items distributed across five subscales: emotional symptoms, conduct problems, peer-relationship problems, hyperactivity/inattention, and prosocial behaviour. A total difficulties score is derived by summing the scores of all subscales except prosocial behaviour. In the present study, Swedish age- and sex-specific cut-offs for the total difficulties score were applied to classify children as exhibiting emotional and behavioural problems [15]. The SDQ has consistently shown acceptable psychometric properties when used among children [16, 17].
Child mental disorders
Data on children’s mental disorders were obtained through linkage of their social security numbers with the SNPR, which comprises data on healthcare utilisation in inpatient and specialised outpatient facilities in Sweden with high validity [18]. Two outcomes were used: (1) any mental disorder, defined as at least one psychiatric diagnosis coded according to the International Classification of Diseases, 10th Revision (ICD-10), codes F00–F99; and (2) any diagnosis of attention deficit hyperactivity disorder (ADHD) or conduct disorder, defined as at least one psychiatric diagnosis corresponding to ICD-10 codes F90–F91. The rationale for using the first outcome was to apply a broad and inclusive definition of mental disorders, consistent with previous population-based register studies in Sweden [19, 20], and to capture the full spectrum of mental health conditions recorded in the SNPR. Specific diagnosis categories in this outcome included mood disorders (ICD-10 codes F30–F39), anxiety disorders (ICD-10 codes F40–F48), eating disorders (ICD-10 codes F50), and behavioural and emotional disorders (ICD-10 codes F90–F98). The inclusion of the latter outcome was motivated by prior findings indicating elevated prevalence rates of ADHD (5%–11%) among Swedish school-aged children in recent years [21].
Statistical analyses
Descriptive statistics, including frequencies, proportions, means, standard deviations and ranges, were used to describe the sample, while chi-square tests were used to compare groups. The associations between preschool- and individual-level socioeconomic deprivation and later mental disorders in the children were estimated using unadjusted and adjusted frailty Cox proportional hazards regression models, with time measured in days. Frailty models were used to account for clustering at the preschool level by incorporating random effects, thereby addressing unobserved heterogeneity and intra-cluster correlation, which enhances the accuracy of inference when survival times within clusters are correlated [22]. The observation period commenced on the date of the child’s inclusion in the Focus study in 2017 and concluded either at the date of the first mental disorder or on 31 December, 2022 for children with no mental disorders.
Prior to the Cox regression modelling, the proportional hazards assumption was tested using the Schönfeld residual tests, showing no violation of this assumption (p-values ranged from p = 0.06 to p = 0.96). Multicollinearity among independent variables was assessed using variance inflation factor (VIF) values, with VIF thresholds of ⩾10 indicating multicollinearity [23]. In this study, VIF values ranged from 1.01 to 1.04, suggesting no multicollinearity.
Unadjusted and adjusted frailty Cox regression models, with two different outcomes were computed: 1) any mental disorder and 2) any ADHD or conduct disorder during follow-up. The independent variables were 1) preschool-level socioeconomic deprivation (low deprivation vs. moderate or high deprivation); 2) individual-level socioeconomic deprivation factors, namely parental education level (lower vs. higher level), parental country of birth (Sweden vs. outside Sweden), and parental marital status (single/living apart/other vs. married/cohabiting); 3) children’s emotional and behavioural problems (identified problems vs. no identified problems); and 4) parental sex (female vs. male). All independent variables were assessed during the children’s preschool years and prior to the recorded dates of the mental disorders. In the adjusted models, all independent variables were entered simultaneously. Children’s mean follow-up times were 2018 and 2059 days respectively (approximately 5.5 years and 5.6 years). From the Cox regression models, we report crude hazard ratios (CHRs), adjusted hazard ratios (AHRs), and E-values for assessment of unmeasured confounding, along with 95% confidence intervals (CIs). In addition, we report frailty terms and estimated frailty variance. SPSS, version 30 and R-software, version 4.4.3 were used for all analyses.
Ethical considerations
Written informed consent was obtained from all parents or legal guardians of the participating children prior to their inclusion in the Focus study. The Focus study and the present study were granted ethical approval by the Regional Ethical Review Board in Uppsala/The Swedish Ethics Review Authority (ref nos. 2012/437 and 2022-06316-02), respectively.
Results
Participant characteristics
The majority of parents (n = 2678) were Swedish-born (84.6%), possessed a college or university degree (74.7%) and were married or cohabiting (95.7%) (Table I). According to the parental SDQ-ratings, 294 children (11.0%) had emotional and behavioural problems. During follow-up, 191 children (7.1%) received a diagnosis of at least one mental disorder, while 99 children (3.7%) were diagnosed with at least one ADHD or conduct disorder. Most children (80.0%, n = 2143) were enrolled in preschools categorised as low-deprivation preschools, whereas fewer children were enrolled in preschools classified as moderately or highly deprived (20%, n = 535).
Background variables and mental disorders during follow-up in the total sample, and children attending preschools with low or moderate/high levels of socioeconomic deprivation. Significant associations are highlighted in bold.
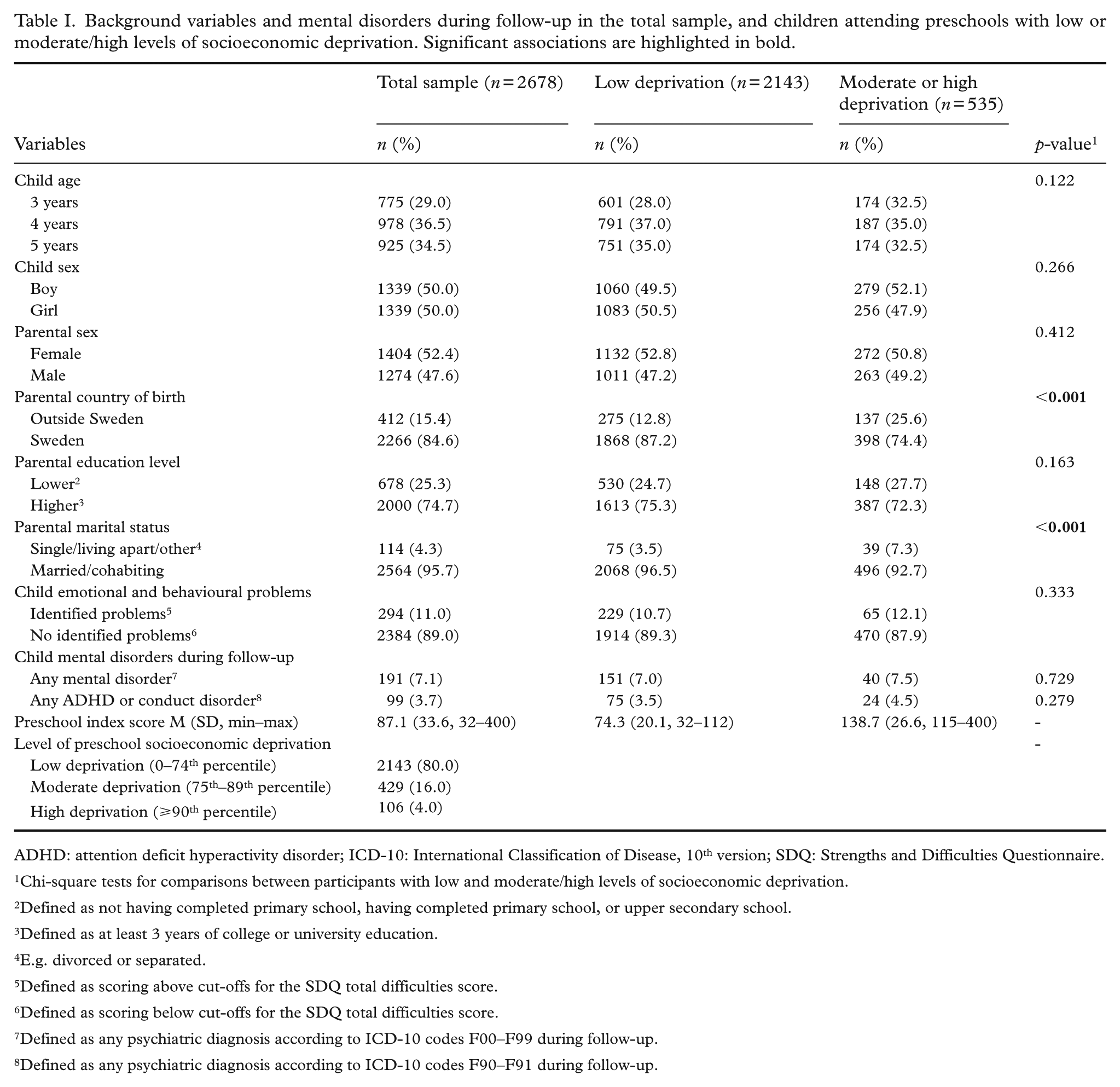
ADHD: attention deficit hyperactivity disorder; ICD-10: International Classification of Disease, 10th version; SDQ: Strengths and Difficulties Questionnaire.
Chi-square tests for comparisons between participants with low and moderate/high levels of socioeconomic deprivation.
Defined as not having completed primary school, having completed primary school, or upper secondary school.
Defined as at least 3 years of college or university education.
E.g. divorced or separated.
Defined as scoring above cut-offs for the SDQ total difficulties score.
Defined as scoring below cut-offs for the SDQ total difficulties score.
Defined as any psychiatric diagnosis according to ICD-10 codes F00–F99 during follow-up.
Defined as any psychiatric diagnosis according to ICD-10 codes F90–F91 during follow-up.
Moderately or highly deprived preschools had a higher proportion of children with parents born outside of Sweden (25.6%) compared to preschools with low levels of socioeconomic deprivation (12.8%; χ²(1) = 53.67, p < 0.001) (Table I). Additionally, the proportion of children with parents who were single, living apart, or had another marital status was greater in preschools with moderate or high deprivation (7.3%) than in low-deprivation preschools (3.5%; χ²(1) = 15.09, p < 0.001).
Preschool- and individual-level socioeconomic deprivation in relation to children’s mental disorders
The frailty Cox regression models (Table II) revealed no association between preschool-level socioeconomic deprivation and any subsequent mental disorder or any ADHD or conduct disorder in the children. However, children of parents with a lower education level had a higher risk of being diagnosed with a later mental disorder (AHR: 1.40; 95% CI: 1.04–1.90) and an ADHD or conduct disorder (AHR: 1.87, 95% CI: 1.24–2.80) than children of parents with a higher education level. Further, children with emotional and behavioural problems also had an increased risk of receiving a subsequent diagnosis of any mental disorder (AHR: 4.10; 95% CI: 3.02–5.58) and an ADHD or conduct disorder (AHR: 6.05; 95% CI: 4.04–9.07) relative to their counterparts without such problems. In the unadjusted model, children whose parents were single or living apart had an increased risk of being diagnosed with an ADHD or conduct disorder (CHR: 2.14; 95% CI: 1.08–4.23), but this association did not remain significant in the adjusted model. The frailty terms of the models were not significant (p = 0.91 and p = 0.92), suggesting that random effects at the preschool-level to account for clustering had no substantial effect on the hazards. The number of events related to any mental disorder and to ADHD or a conduct disorder per preschool, stratified by level of deprivation (low or moderate/high), is given in the supplemental materials (Supplementary Tables 1 and 2).
Frailty multiple Cox regression models with E-values for exploring the associations between preschool- and individual-level socioeconomic deprivation and children’s mental disorders (n = 2678). Significant associations are highlighted in bold.
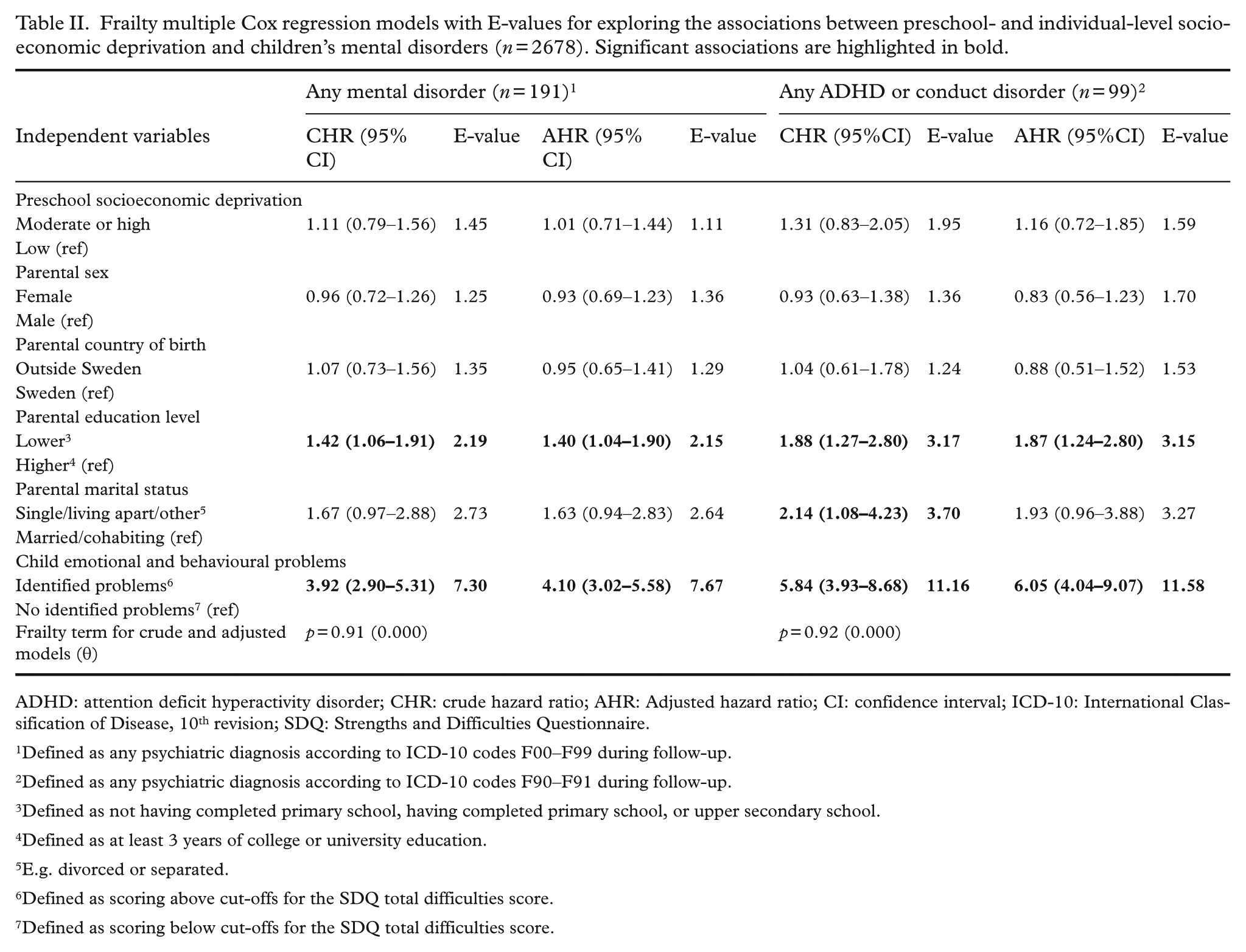
ADHD: attention deficit hyperactivity disorder; CHR: crude hazard ratio; AHR: Adjusted hazard ratio; CI: confidence interval; ICD-10: International Classification of Disease, 10th revision; SDQ: Strengths and Difficulties Questionnaire.
Defined as any psychiatric diagnosis according to ICD-10 codes F00–F99 during follow-up.
Defined as any psychiatric diagnosis according to ICD-10 codes F90–F91 during follow-up.
Defined as not having completed primary school, having completed primary school, or upper secondary school.
Defined as at least 3 years of college or university education.
E.g. divorced or separated.
Defined as scoring above cut-offs for the SDQ total difficulties score.
Defined as scoring below cut-offs for the SDQ total difficulties score.
Selection-bias analysis
Children in the current study (n = 2678) were compared with excluded children (n = 267) to explore whether the current study sample was representative of the larger Focus cohort of the year 2017. Among the included children, a larger proportion of children had parents with higher educational levels (74.7% vs. 53.1%) (χ2 (1) =38.99, p = 0.001, n with missing data: 92), and with married/cohabiting marital status (95.7% vs. 92.5%) than excluded children (χ2 (1) =3.97, p = 0.046, n with missing data: 93). Furthermore, among excluded children, a higher proportion were identified with emotional and behavioural problems (16.0%) compared to those included (11.0%) (χ²(1) = 4.30, p = 0.038, n with missing data: 86). Similarly, the proportion of children with a later mental disorder was greater among excluded children (10.5%) than among included children (7.1%) (χ²(1) = 3.97, p = 0.046).
Discussion
Our findings suggest no associations between preschool-level socioeconomic deprivation and subsequent mental disorders. However, individual-level socioeconomic deprivation, in terms of lower parental education level, and child emotional and behavioural problems increased the risk of such disorders.
The findings do not align with the previous research showing associations between school-level socioeconomic deprivation and children’s mental health outcomes. For instance, a previous Swedish study based on Focus data [14] found a correlation between preschool-level socioeconomic deprivation and peer-relationship problems in children at 3–5 years of age. Moreover, findings from other Swedish and international studies have demonstrated relations between school-level socioeconomic deprivation and both general mental health problems as well as specific emotional and behavioural problems among school-aged children [6, 7, 24].
However, a systematic review showed that associations between school-level socioeconomic deprivation and mental health outcomes among students were weak or non-significant [25]. It should be noted that, unlike the aforementioned studies, we included diagnosed mental disorders as outcomes. Thus, preschool-level socioeconomic deprivation did not predict severe mental health problems in the current study. An additional consideration relates to how preschool-level socioeconomic deprivation was operationalised. We employed the SSCI, a municipality-specific index designed to guide the allocation of compensatory resources. While this indicator has strong local policy relevance, its construction and scope differ from other deprivation measures commonly used in prior research, such as neighbourhood-level income, education levels, or unemployment rates [2, 6, 7, 25]. Such methodological differences in how deprivation was operationalised and measured may also have contributed to the non-alignment of our findings with those of previous studies.
Our finding showing that individual-level socioeconomic deprivation was related to subsequent child mental disorders aligns with findings from several studies [1, 2, 6, 8, 26]. For example, a systematic review found that individual-level socioeconomic factors, such as low parental educational attainment and limited household income, were associated with an increased prevalence of mental health problems among children [2]. Furthermore, Holstein and colleagues [8] demonstrated that low parental educational attainment at the time of childbirth was associated with an increased risk of diagnosed mental disorders in children from 11 months to 8 years. Similarly, Horoz and colleagues [6] found that children of parents with lower educational attainment exhibited greater problems in the emotional, behavioural and peer-relationship domains in the first grade, as well as an accelerated increase in behavioural problems from the first to the sixth grades. Our findings demonstrating relations between emotional and behavioural problems and subsequent mental disorders are consistent with previous research [27] and underscore the importance of routine screening for such difficulties during the preschool years.
Overall, single individual-level socioeconomic deprivation factors appear to be more important predictors of mental health outcomes in children than preschool-level socioeconomic deprivation factors. Consequently, prioritising interventions that address or mitigate the elevated mental health needs of children growing up with parents with lower socioeconomic status should be regarded as highly important. In Sweden, large proportions of children attend preschool (87%) and are enrolled in the child health services (99%) [28, 29], which makes these settings ideal for mental health interventions. Implementing interventions to support children facing individual socioeconomic disadvantages in these settings may reduce the risk of future mental health problems in this group.
Strengths and limitations
Strengths include the population-based sampling framework and longitudinal design, in which the children were followed for approximately five and a half years. Moreover, using the SDQ to assess children’s emotional and behavioural problems represents a methodological advantage, owing to the instrument’s psychometric properties as demonstrated in prior research [16, 17]. Furthermore, the reliance on SNPR data for identifying children’s mental disorders reduces the risk of self-report bias. Finally, by estimating the association between preschool- and individual-level socioeconomic deprivation factors and later mental disorders in children, this study contributes to addressing a gap in the existing literature.
However, several limitations must be acknowledged. The results were not adjusted for parenting style, children’s chronic conditions, or exposure to stressful or traumatic experiences, as data on these variables were unavailable or inadequate. Considering prior research demonstrating associations between these factors and mental disorders in children, the omission of such data is a limitation [24, 30-32]. A further limitation is that we did not have access to register-based socioeconomic data such as household income, nor other potentially important indicators of deprivation, such as parental mental health, substance use, or criminal behaviour. The absence of these data may restrict the precision with which we captured individual-level socioeconomic deprivation. Future studies should therefore aim to incorporate such data to provide a more comprehensive understanding of the interplay between socioeconomic deprivation and children’s mental health outcomes.
Further, all exposures including the socioeconomic deprivation parameters were measured only during the preschool period, reflecting a critical period approach, given that preschool years are a sensitive stage for child development. However, any changes in socioeconomic status across time not were not captured in our analysis, and thus our findings should be interpreted as reflecting the influence of socioeconomic deprivation during the preschool years, rather than across the full course of childhood. Future studies with repeated measures could therefore examine both critical and cumulative effects of socioeconomic deprivation in relation to mental health outcomes in children.
Moreover, the classification of preschools into deprivation categories may have been too broad to reflect smaller, more detailed contextual differences in their environments. As far as we are aware, the SSCI has not been psychometrically evaluated in prior research. Thus, using this index for assessment of socioeconomic deprivation at the preschool level could be considered a limitation. Moreover, the current study did not explore the compensatory mechanism of the SSCI per se, as no data were available on the amount each preschool received or how the amount was used. Thus, future research should explore such data in relation to mental disorders in young children to investigate the potential mitigating effects of the SSCI.
Most participating parents were highly educated and there was a higher occurrence of mental disorders among excluded children than children in the study. This may have contributed to underestimations of the actual prevalence of mental disorders in young children and the associations found in the study. In addition, the use of a complete case analysis may have introduced selection bias. Lastly, the SSCI provides a measure of preschool-level socioeconomic deprivation specific to Uppsala Municipality. Beyond this, other structural, organisational and policy-related factors vary between municipalities in Sweden, for example, differences in resource allocation, variations in preschool organisation, and local approaches to implementing compensatory measures. Altogether, these circumstances limit the generalizability of the present findings to other settings.
Conclusions
Preschool-level socioeconomic deprivation was not related to later mental disorders among children in a Swedish setting. However, individual-level socioeconomic deprivation, in terms of lower parental education level, increased the risk of such disorders. Children of socioeconomically disadvantaged families may be at risk of developing mental disorders. Swedish preschools and child health services could implement interventions targeting healthy development for this group.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948251406844 – Supplemental material for Preschool- and individual-level socioeconomic deprivation in relation to mental disorders among children in Sweden
Supplemental material, sj-docx-1-sjp-10.1177_14034948251406844 for Preschool- and individual-level socioeconomic deprivation in relation to mental disorders among children in Sweden by Sabine Lindén, Anton Dahlberg, Richard Ssegonja, Anna Fäldt and Natalie Durbeej in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-2-sjp-10.1177_14034948251406844 – Supplemental material for Preschool- and individual-level socioeconomic deprivation in relation to mental disorders among children in Sweden
Supplemental material, sj-docx-2-sjp-10.1177_14034948251406844 for Preschool- and individual-level socioeconomic deprivation in relation to mental disorders among children in Sweden by Sabine Lindén, Anton Dahlberg, Richard Ssegonja, Anna Fäldt and Natalie Durbeej in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank all participants of the study and nurses at the child health centres who facilitated the distribution of the questionnaires. We also wish to thank the research assistants in the Child Health and Parenting (CHAP) research group for their support during the data collection process.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Swedish Research Council for Health, Working Life and Welfare (Forte) (grant no. 2021-01046).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.