
Abstract
Aims:
The potential health hazards associated with snus use are less studied compared with the health risks related to smoking. However, during the past decade there is growing evidence on increased risk for mortality, cardiovascular disease (CVD) and cancer following snus use. The aim of the present study was to examine the possible association between snus use at the age of 40 and 50 years, and the development of coronary heart disease (CHD), stroke, hypertension, or heart failure later in life in men with no history of smoking.
Methods:
Data from a population-based cohort with data from health examinations at 40 or 50 years of age, performed between 1990 and 1999 was used to identify non-smoking men that used snus or not. Crude and adjusted associations of snus use and first diagnosis of CHD, stroke, hypertension or heart failure and all-cause mortality were analysed for the age groups separately, using Cox proportional hazards regression models.
Results:
A total of 4222 non-smoking men were included, of which 458 (10.8%) used snus. The adjusted hazard ratios for a first diagnosis of hypertension were 1.64 (95% confidence interval (CI) 1.36–1.98), and 1.75 (95% CI 1.17–2.62) for heart failure, for 50-year-old, snus using men.
Conclusions:
Keywords
Background
Cardiovascular disease (CVD) remains the leading cause of premature death and disability-adjusted life years worldwide [1]. In recent years a wide range of commercial tobacco and recreational nicotine-containing products have become available globally, and their use has expanded rapidly. According to the global burden of disease study over 6 million disability-adjusted life years, and 258,000 lives can be attributed to smokeless tobacco-products [2]. One form of smokeless tobacco is Swedish snus (snuff), an oral moist tobacco product commonly used in Sweden and the other Nordic countries. The traditional Swedish snus is either used loose or in a portion-packed form (sachets). It is more common among men than women to use snus; 20% of all men and 6% of all women in Sweden reported using snus on a regular basis in a nationwide survey from 2022 [3]. Snus contains numerous potentially toxic ingredients such as tobacco-specific nitrosamines and nicotine. Nicotine has systemic haemodynamic effects, primarily mediated by activation of the sympathetic nervous system and therefore has an acute effect on both blood pressure and heart rate [4]. Additionally, the different tobacco-specific nitrosamines are important and potent carcinogens [4]. Traditional Swedish snus does not distribute the harmful combustion products, but the amount of nicotine is comparable to that in cigarettes, even though the nicotine content varies widely. The peak blood concentration of nicotine in snus users is similar to that observed in cigarette smokers. Nicotine is known to be highly addictive and can lead to the development of nicotine tolerance, and nicotine addiction can develop very quickly [4]. During the past decade several studies have demonstrated an increased association with hypertension and obesity [5], an increased risk for ischaemic heart disease, stroke and heart failure [6 –10], and an increased risk of fatal stroke [11] and fatal coronary heart disease (CHD) for men that use snus [12].
Despite recent studies on the negative health effects from snus use there is an ongoing debate in society about whether snus could be regarded as a harmless substitute for smoking. Therefore, there is a need for long-term follow-up studies, to explore the potential health hazards of snus use per se.
We hypothesised that the use of Swedish snus in midlife increases the risk of cardiovascular disease later in life. The aim of the present study was to examine the possible association between snus use at 40 and 50 years with cardiovascular disease development later in life, in men, with no history of smoking.
Methods
During 1990–1999 all inhabitants in Region Västmanland, Sweden were invited to a health screening the year they turned 40 or 50 years old.
The health screening aimed to identify risk factors for CVD to reduce CVD morbidity among 40 and 50-year-old inhabitants in Region Västmanland. It involved a clinical examination and a self-administered questionnaire with information on lifestyle habits such as smoking and snus use, previous history of CVD and diabetes mellitus, and socioeconomic factors. Data from the health examinations and questionnaires have been saved in a local database, the Westmannia Cardiovascular Riskfactor study (WICTORY) administered by the Centre for Clinical Research, Region Västmanland, and has been described in more detail in previous studies [13].
Snus use was reported as a single yes or no question. Smoking was reported by choosing one of the following alternatives: never smoked, previous smoker, current smoker 1–14 g/day, current smoker 15–24 g/day and current smoker more than 24 g/day, with 1 g corresponding to one cigarette. Education was self-reported as the number of years post-elementary school. In general, this implies 7 years in elementary school for participants born in the 1940s and 9 years for participants born in the 1950s due to a change in the Swedish school system. Physical activity was reported on a five-graded scale reaching from no regular physical activity to regular physical activity of 30 minutes or longer of at least moderate intensity every day.
Study population
Of the 56,977 individuals that were invited to the health screening, 34,269 (60.1%) completed the health examination during 1990–1999. A detailed overview of the selection procedure for the present study is presented in Figure 1. Reasons for exclusion were as follows: people who had moved from the county, missing records of snus use, incomplete date of health examination or death, female sex, current or former smoker. Finally, individuals who were deregistered from the Swedish Tax Agency Population Registration, who had deviant age or missing records for one or more of the covariates were excluded. A total of 4222 non-smoking men were included in the study, of which 458 (10.8%) were snus users (exposed group, 40 or 50-year-old men) and 3764 (89.2%) did not use snus or any other tobacco product (unexposed group, 40 or 50-year-old men).

Flow chart study population.
Follow-up started at the date of the index examination of an individual and ended in June 2022.
Data from the National Board of Health and Welfare (NBHW) were used for the years 1990–2007, this register only include data retrieved from hospitals. In addition, a local register, the Datalager för Uppföljning och Verksamhets Analys (DUVA) 2008–2022, was our main diagnosis register as it comprises data from both primary healthcare and hospitals in Region Västmanland. Information was searched for CHD (International Classification of Diseases, version 10 (ICD-10): I20–22, I24–25), stroke (ICD-10: I61–66, G45), hypertension (ICD-10: I10) and heart failure (ICD-10: I11.0, I50). As ICD-10-SE was implemented in 1997, a conversion of the diagnoses to ICD-9-SE was performed to be used for the earlier registers, see Supplemental Table I. Finally, the national register for death causes was used. Both primary and secondary diagnoses were searched for in all registers. Participants who were identified with the above-mentioned diagnosis at inclusion, based on data from NBHW with a lookback period to 1963, were excluded from the analysis, see Figure 1.
The Uppsala Regional Ethical Review Board approved the study by waiving informed consent (Dnr 2007/165, 2020-0930).
Statistical analysis
All continuous variables are presented as median (Q1, Q3). Categorical variables are presented as frequency and percentage. Smoking was dichotomised as never smoker versus current or former smoker. Members in the household were dichotomised to living alone versus more than one person in the household.
Crude and adjusted associations of snus use and first diagnosis of CHD, stroke, hypertension, heart failure and all-cause mortality were analysed for each age group separately, using Cox proportional hazards regression models. Adjusting variables were blood glucose, and total cholesterol for all cardiovascular outcomes, both being important factors in the development of CVD. In addition, mean arterial pressure was included in the multivariate analysis for all-cause mortality.
The proportional hazard assumption was assessed by visual inspection of the log[ -log(cumulative survival)] for each categorical variable, and by visual inspection of the Schoenfeld residuals versus time for continuous variables. Cumulative survival was estimated by the Kaplan–Meier estimator.
Kaplan-Meier survival analysis was used to assess the time to first CVD diagnosis and all-cause mortality.
A two-sided P value <0.05 was regarded as statistically significant. IBM SPSS Statistics, version 28 was used for all analyses.
Results
A total of 2143 (50.8%) men turned 40 years and 2079 (49.2 %) turned 50 years. Snus use was more common among 40-year-old men than 50-year-old men (13.6% and 8.0%, respectively). For further details, see Table I.
Baseline characteristics, non-smoking 40 and 50-year-old men.
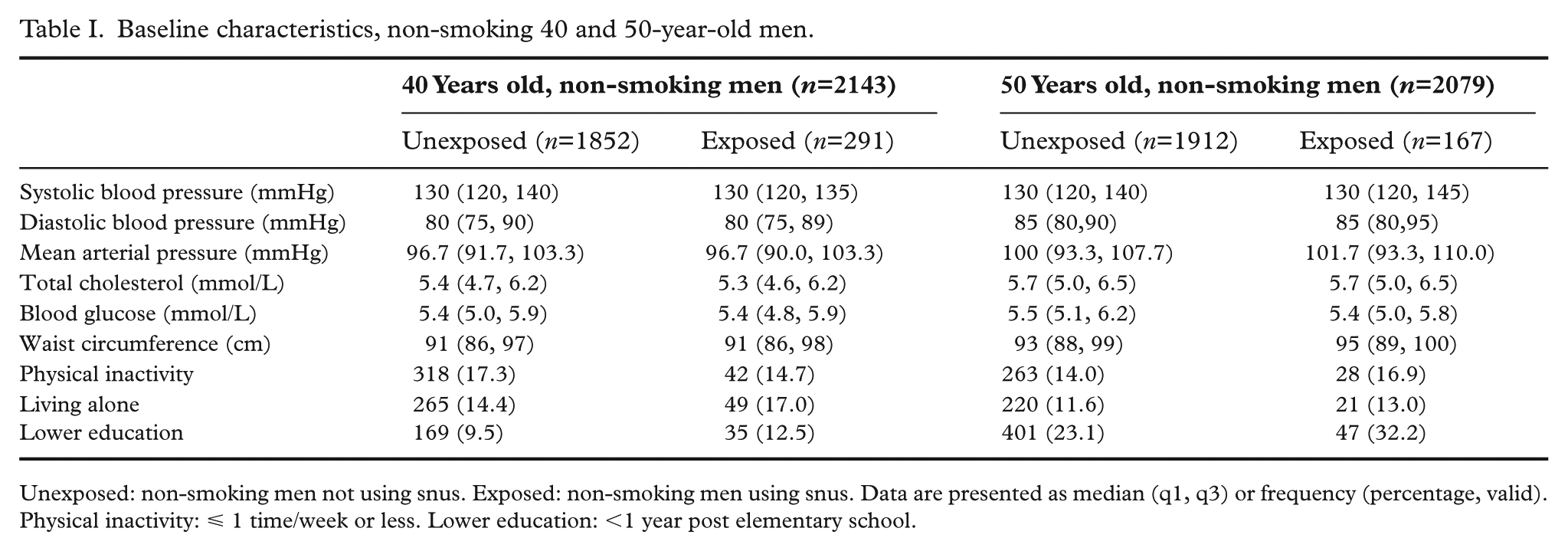
Unexposed: non-smoking men not using snus. Exposed: non-smoking men using snus. Data are presented as median (q1, q3) or frequency (percentage, valid). Physical inactivity: ⩽ 1 time/week or less. Lower education: <1 year post elementary school.
The median follow-up time for a diagnosis of hypertension was 19.2 (15.2, 22,2) years for the 50-year-old exposed group and 21.0 (17.5, 24.0) years for the 50-year-old unexposed group, corresponding to 3206 and 40,152 person-years at risk for the exposed group and unexposed group, respectively. There were 1153 (60.3%) men diagnosed with hypertension in the unexposed group and 121 (72.5%) men in the exposed group, corresponding to 29 men diagnosed with hypertension in the unexposed group and 38 men in the exposed group per 1000 person-years at risk. The corresponding figures for 40-year-old men were 22 men diagnosed with hypertension in the unexposed group and 24 men in the exposed group per 1000 person-years at risk. For heart failure the corresponding figures were 207 (10.8%) men diagnosed with heart failure (five events per 1000 person-years at risk) in the 50-year-old unexposed group and 27 (16.2%) men (eight events per 1000 person-years at risk) in the 50-year-old exposed group. The corresponding figures for 40-year-old group were two men diagnosed with heart failure in the unexposed group and three men in the exposed group per 1000 person-years at risk. See Supplemental Table II.
The results of the Cox regression (crude hazard ratio (HR)) indicated an increased risk for hypertension and heart failure for 50-year-old men, but not for 40-year-old men. For further details see Table II. After adjustment for total cholesterol and blood glucose the adjusted hazard ratio (aHR) for hypertension was 1.64 (95% confidence interval (CI) 1.36–1.98) for the 50-year-old exposed group. The aHR for heart failure was 1.75 (95% CI 1.17–2.62) for the 50-year-old exposed group. For CHD, stroke, and all-cause mortality the results were non-significant for both age groups.
Crude and adjusted HR for all-cause mortality and circulatory diseases; exposed group (snus use) versus unexposed group.

CI: confidence interval; HR: hazard ratio.
CHD (coronary heart disease): ICD-10: I20–22; I24–25. Stroke: ICD-10: I61–66; G45. Hypertension: ICD-I0: I10. Heart failure: ICD-10: I11.0. I50. All-cause mortality adjusted for mean arterial pressure, total cholesterol and blood glucose. CHD, stroke, hypertension and heart failure adjusted for total cholesterol and blood glucose.
To elaborate further on how snus use affects CVD morbidity, a Kaplan–Meier analysis was performed. See Figures 2 and 3.

Kaplan–Meier analysis on hypertension: exposed group (snus use) versus unexposed group.

Kaplan–Meier analysis on heart failure: exposed group (snus use) versus unexposed group.
Discussion
The main findings of this population-based study with a median of 27 years follow-up of non-smoking men were an increased risk for hypertension and heart failure for 50-year-old men that used snus. The results were insignificant for the association between snus use and the increased risk of CHD, stroke, and all-cause mortality for both age groups.
There is growing evidence for the association between snus use and CVD morbidity and mortality. A recent study of 169,103 never smoking, snus-using men demonstrated an increased risk for both all-cause mortality (aHR 1.28, 95% CI 1.20–1.35) and cardiovascular mortality (aHR 1.27, 95% CI 1.15–1.41) [6]. In our study there was a tendency towards an increased risk for all-cause mortality for the studied group of snus exposed men, although it was statistically insignificant. Another Swedish study of 1076 elderly never-smoking men investigated the possible association with heart failure and found an even higher risk for heart failure for snus users (HR 2.08, 95% CI 1.03–4.22) than in our material [7]. Even though there seems to be no evidence of a higher risk of myocardial infarction or stroke per se [14], as also demonstrated in our study, snus use or snus quitting after a major cardiovascular event is of importance. Patients who quit using snus after a myocardial infarction (MI) had half the risk of premature death compared with continuing snus users (aHR 0.51, 95% CI 0.29–0.91) according to a Swedish study of 2474 men, corresponding to the risk reduction for smokers after smoking cessation in the same study (aHR 0.54, 95% CI 0.42–0.69) [15]. Additionally, the risk of death following a stroke has been found to be increased among snus users compared with non-snus users (aHR 1.32, 95% CI 1.08–1.61) according to a study on 130,485 non-smoking men [11].
It is well known that nicotine has both acute and long-term effects on the cardiovascular system. Nicotine exerts its effects via stimulation of the nicotinic acetylcholine receptors and targets broad physiological effects, such as increased heart rate and blood pressure, increased blood viscosity and platelet aggregation [16]. Furthermore, the association between hypertension and the development of heart failure is well established, as hypertension causes structural and functional changes in the heart that can ultimately lead to heart failure and other important cardiovascular conditions [17,18]. Previous studies have shown that the risk of developing heart failure was two fold for hypertensive men of all ages [19,20] and three fold in hypertensive older subjects (>65 years) (odds ratio 3.08, 95% CI 2.88–3.31) [21]. Therefore, the result of our study is distressing, as the aHR for hypertension was 1.64 (1.36–1.98) for 50-year-old men, which might explain the increased risk for heart failure by over 70% in the same age group [17]. The present study could not demonstrate any significant associations between snus use and an increased risk for CHD or stroke. Although the pathway between hypertension and major cardiovascular events is also well established [18] the relatively few events in our material may have led to a lack of power in the Cox proportional hazard regression analysis.
Even more distressing is the fact that the so-called nicotine snus, or ‘white snus’, has reached the market in 2016 and that its use is rapidly increasing, especially among younger age groups. In 2023, one fifth of both men and women aged 17–29 years used nicotine snus daily [22]. Nicotine snus often has a higher nicotine content and is designed to maximise the nicotine uptake, hence increasing the risk of nicotine addiction. The effects on CVD morbidity and mortality are not possible to follow up at this point, but in the light of the increased risk of hypertension and heart failure demonstrated in our study, the long-term effects of nicotine snus need to be studied further.
Strengths and limitations
The strength of this population-based study is the long follow-up time of 27 years and the comparison with an unexposed group from the same population, which allows us to study time-dependent morbidity linked to the long-term use of snus. For many chronic diseases such as hypertension and heart failure, the impact from genetic conditions decreases with age, while the impact of lifestyle habits and environmental factors increases. The long follow-up period could partly mitigate the impact from the underlying genetic preconditions. Secondly, we were able to include only non-smoking men, which excludes the well-known detrimental effect of smoking and allows for an analysis of exclusive snus use. Thirdly, the health screening included information on important risk factors for CVD, such as blood pressure, blood glucose, and total cholesterol allowing adjustments for these covariates.
However, there are also some limitations that need to be addressed.
Swedish snus is a specially processed type of smokeless tobacco product and is restricted by Swedish law regarding nicotine and tobacco-specific nitrosamines content. Therefore, Swedish snus has fewer carcinogens than those typically found in smokeless tobacco products from the US and other parts of the world [2,23]. Given this difference, it is unclear whether the findings in our study can be generalised to other parts of the world where the adverse effects from the use of smokeless tobacco products are even higher. Secondly, excluding participants with pre-existing CVD at baseline can introduce selection bias. Many snus users start at a young age, leading to long-term exposure that may result in cardiovascular risks by age 40 or 50 years. Excluding those with CVD, including hypertension, might disproportionately exclude long-term users already experiencing cardiovascular issues, potentially underestimating the true risks of snus. Thirdly, the use of Kaplan–Meier curves and the Cox proportional hazard regression model may produce inflated results in the case of competing events. To check if this might have affected our conclusions, we reran the Cox regression analyses using the semi-parametric Fine and Gray model, which alleviates this inflation [24]. The results from the analyses showed that this was not the case. The relatively small number of exclusive snus users and few outcome events hamper the analysis and lead to low statistical power, as might be the case for CHD, stroke, and all-cause mortality. Although the results in our study can be supported by other larger cohort studies, the results need to be interpreted carefully. Fourthly, we do not know if the participants continued to use snus, quit using snus and/or started smoking, which might be an unknown confounding factor. On the other hand, it is unusual for non-smoking men above 40 years to start using tobacco of any kind.
Another limitation includes the restriction of the population to Swedish men. Even though this was necessary due to the small number of snus exposed women, this limits the generalisability of this study.
Conclusions
Snus use among non-smoking 50-year-old men was associated with an increased risk for hypertension and heart failure later in life, even after adjustment for known risk factors for CVD. However, the associations were insignificant for CHD, stroke and all-cause mortality. The findings demonstrate that snus use contributes to the burden of cardiovascular disease, highlighting the importance of public health initiatives aimed at reducing its use in the population.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948251405687 – Supplemental material for Swedish snus use in non-smoking middle-aged men and risk of cardiovascular disease: a population-based cohort study with 27-year follow-up
Supplemental material, sj-pdf-1-sjp-10.1177_14034948251405687 for Swedish snus use in non-smoking middle-aged men and risk of cardiovascular disease: a population-based cohort study with 27-year follow-up by Lena M Loennberg, Abbas Chabok, John Ohrvik, Mattias Rehn, Jerzy Leppert and Mattias Damberg in Scandinavian Journal of Public Health
Supplemental Material
sj-pdf-2-sjp-10.1177_14034948251405687 – Supplemental material for Swedish snus use in non-smoking middle-aged men and risk of cardiovascular disease: a population-based cohort study with 27-year follow-up
Supplemental material, sj-pdf-2-sjp-10.1177_14034948251405687 for Swedish snus use in non-smoking middle-aged men and risk of cardiovascular disease: a population-based cohort study with 27-year follow-up by Lena M Loennberg, Abbas Chabok, John Ohrvik, Mattias Rehn, Jerzy Leppert and Mattias Damberg in Scandinavian Journal of Public Health
Footnotes
Data availability statement
Data are available on reasonable request. Qualified researchers may request access to patient-level data and related study documents and dataset specifications. Patient-level data will be anonymised, and study documents will be redacted to protect the privacy of trial participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The health examination and data collection were supported by the Regional Council of Västmanland and the Regional Research Council of Uppsala-Örebro, Sweden (RFR 73931).
Ethical considerations
This study involves human participants and was approved by the Uppsala Regional Ethical Review Board by waiving informed consent (Dnr 2007/165, 2020-0930).
Consent to participate
According to Swedish ethical standards in 1988–89 the invitation to participate in the health screening included written information that data, including test results, should be filed and used for future scientific studies. The information was repeated verbally by the attending nurse to those who chose to participate in the health screening. An application was filed to the Regional Board of Ethics, Uppsala in 2007 to ensure that future studies should be in line with more recent ethical standards. The Uppsala Regional Ethical Review Board approved the study by waiving informed consent (Dnr 2007/165, 2020-0930).
Consent for publication
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.