
Abstract
Aim:
Loneliness is an important public health concern, especially among young people experiencing multiple social transitions. Although research on loneliness and mental health is growing, few studies have focused on emerging adulthood, and most rely on cross-sectional designs. This study examines the association between loneliness and subsequent depression and anxiety, both as clinical diagnoses and as self-reported symptoms, among emerging adults.
Methods:
Data were obtained from Futura01, a Swedish national cohort study that tracks individuals born in 2001 and includes both survey data and linked register information. The study population included 3828 participants for the analysis of depression and anxiety diagnoses (based on International Classification of Diseases-10 codes in the Swedish National Patient Register), and 2747 participants for the analysis of self-reported depression and anxiety symptoms (based on the Patient Health Questionnaire-4). Logistic regression models were employed to analyse the associations.
Results:
Loneliness at age 18 was linked to both depression and anxiety diagnoses at ages 19–20 and self-reported depression and anxiety symptoms at age 21, even after the adjustment for sociodemographic characteristics and prior depression and anxiety diagnoses.
Conclusions:
Introduction
Loneliness is often described as a subjective distressing feeling that arises when individuals perceive their social relationships as lacking in either quantity or especially quality [1]. Loneliness indicates an unmet need for social connection and is increasingly recognised as a social determinant of health [2,3], affecting people of all sociodemographic backgrounds. It can have a detrimental impact on physical and mental health, quality of life and longevity, with mortality risks comparable with other well-established factors such as smoking, hypertension, obesity, physical inactivity and others [2,4]. Given the overall prevalence of loneliness and its adverse implications for health, it is acknowledged as a global public health concern [5].
Loneliness has been linked to various mental health problems, including depression and anxiety [6,7]. Prior research showed that the links between loneliness and mental health disorders may be especially pronounced compared with other medical conditions [8]. Furthermore, depression and anxiety, two of the most prevalent mental health problems, can create a self-perpetuating cycle with loneliness [9,10]. Loneliness can impact mental health through various mechanisms, including increased perceived stress, diminished capacity for self-regulation, lower self-esteem and poorer overall life satisfaction [7,11]. Furthermore, lonely individuals more often use negative coping strategies, experience negative self-talk and self-doubt, which can also be mechanisms leading to subsequent mental health problems [7,12]. Loneliness can contribute to cognitive biases related to social threats, resulting in a heightened state of alertness and negative thought patterns, such as an expectation of negative social interactions and a tendency to retain more negative social information [11].
While loneliness can be experienced at any stage of life, it is particularly prevalent among young people, in Sweden [13] and elsewhere [14]. In addition to experiencing higher rates of loneliness, emerging adults may be more profoundly affected by it than other age groups, often feeling heightened pain and distress [15]. Research has also emphasised the multifaceted nature of loneliness in this particular age group [9,10,12,15-17]. This life stage is marked by important social transitions which young people themselves view as determinants of loneliness [10]. Additionally, this developmental period is characterised by an increased desire for social connections, which can lead to loneliness when unmet [12]. Therefore, loneliness can be particularly impactful for emerging adults, as their need for social acceptance and belonging may intensify during this developmental stage. Social expectations for an emerging adult’s life also play an important role contributing to loneliness [17]. Additionally, the elevated prevalence of mental health problems among emerging adults has been highlighted, especially of anxiety and depression [18].
While there is a growing body of research on the relationship between loneliness and mental health problems, relatively few studies have specifically focused on the prospective association during emerging adulthood. Existing studies mostly rely on cross-sectional designs, underscoring the need for longitudinal research to better understand the long-term impact of loneliness in this population [19]. Moreover, longitudinal data enable the examination of temporal associations, which is crucial for understanding how loneliness contributes to mental health problems, given the potential bidirectional nature of their relationship.
This study aims to examine the prospective associations between loneliness and the subsequent likelihood of experiencing depression and anxiety, both in terms of clinical diagnoses as well as self-reported symptoms, among emerging adults. When examining the relationship between loneliness and subsequent mental health problems, it is crucial to consider pre-existing mental health conditions, as they may influence the experience of loneliness [9,10] and are also likely associated with later adverse mental health outcomes. In addition, sociodemographic characteristics that may be associated with both loneliness and mental health problems should be taken into consideration, e.g. gender, educational status, living arrangements, migration background and socioeconomic position in the family of origin [7,20-22].
Methods
Study design and material
The study uses data from Futura01, a Swedish cohort study of a nationwide sample of adolescents attending grade 9 in 2017, with the vast majority born in 2001 [23]. In 2017 (t1, at age 16), 500 schools across Sweden were randomly selected with a response rate of 69% at the school level [23]. Participating and non-participating schools did not differ significantly in terms of grade point average, the proportion of highly educated parents or the proportion of parents with a foreign background, indicating no systematic bias in school participation [23]. The baseline study (t1) was conducted in classrooms. Of the 6769 adolescents present at school on the day of the baseline study, 5722 (85%) agreed to participate and provided consent, and the final t1 sample comprised 5537 respondents (82%). The second and the third waves were performed in 2019 (t2, at age 18) and 2022 (t3, at age 21), respectively, primarily as online surveys. In the second wave (t2), 4141 of those responding at t1 agreed to participate (75%). The measure of loneliness was included for the first time in the second wave of data collection (t2). Therefore, only individuals who participated in the second wave were encompassed in the present study. Among them, only those with complete data on loneliness and the sociodemographic characteristics considered in this study were included (n = 3828). In the third wave (t3), 2956 of those who responded at both t1 and t2 agreed to participate [24]. Overall, in the follow-up surveys, dropout rates were slightly higher among males, individuals whose parents had less than tertiary education and those with two foreign-born parents [24,25]. Depression and anxiety symptoms were assessed for the first time in the third wave of data collection (t3). Consequently, the analysis of loneliness and self-reported depression and anxiety symptoms included only participants with complete data for this measure in the third wave (n = 2747). The self-report survey data have been linked to official registers, providing additional information on sociodemographic characteristics and depression and anxiety diagnoses. A flow chart of the data is displayed in Figure 1.
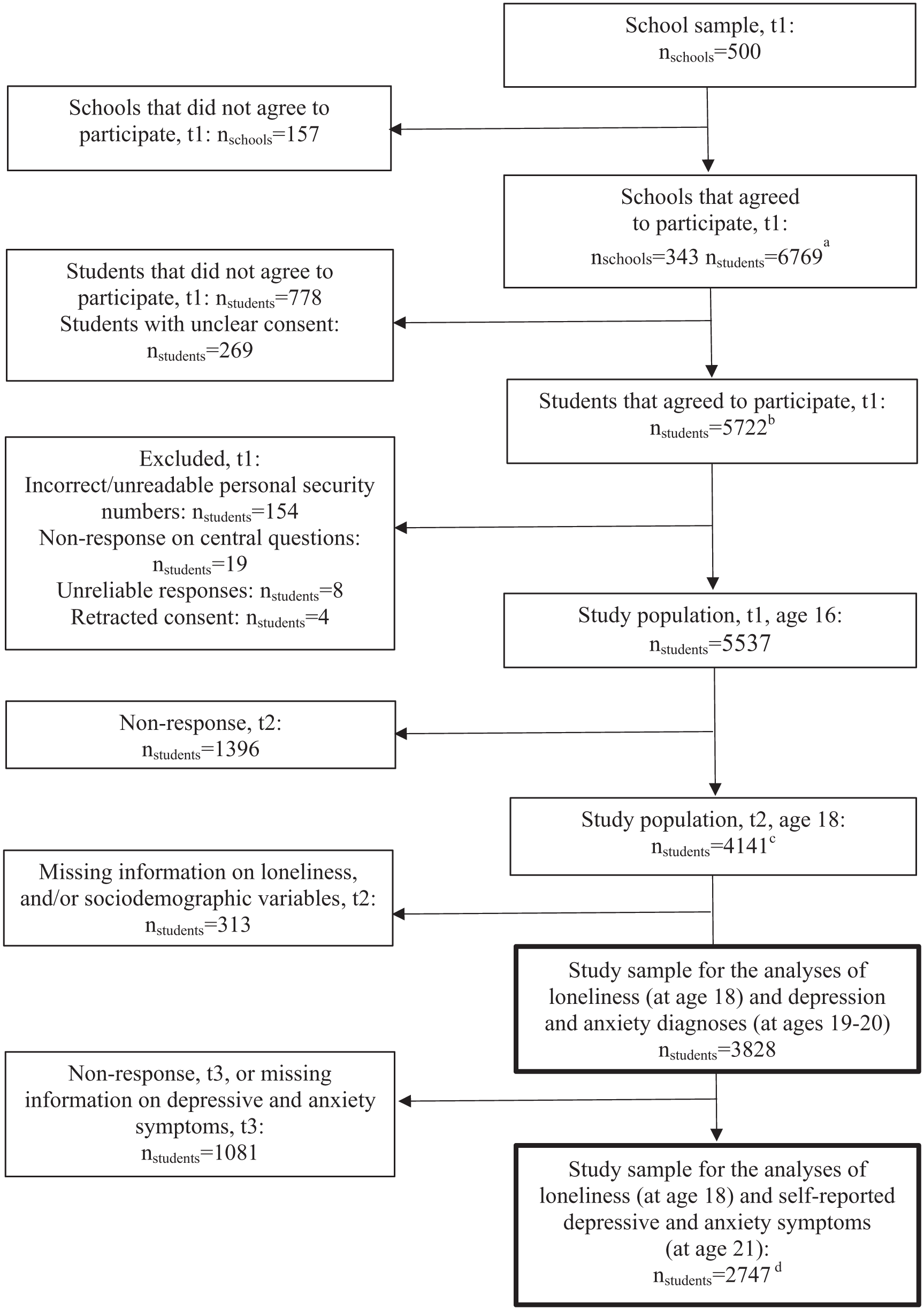
Flow chart of the data.
Exposure
Loneliness was measured in 2019 (at age 18) with a single item: ‘Are you bothered by loneliness?’ with the response categories (1) ‘Less often than once a month’, (2) ‘Several or one time a month’, (3) ‘One time a week’, (4) ‘Several times a week’ and (5) ‘Every day’. The responses were dichotomised, with answers from (1) to (3) coded as 0 (‘Low’) and answers from (4) to (5) were coded as 1 (‘High’) [e.g., 26,27]. While multi-item scales provide comprehensive assessments, single-item measures of loneliness have proven to be a valid and reliable alternative for use in population-based surveys. Prior research has demonstrated that single-item measures correlate well with established multi-item scales [28,29].
Outcomes
Depression and anxiety diagnoses were identified based on official register information from 2020 to 2021 (at ages 19–20). Information on specialised out-patient and in-patient care was drawn from the Swedish National Patient Register. Participants were categorised as having a depression and/or anxiety diagnosis if there was information on (one or more of) the following diagnoses based on International Classification of Diseases-10 codes: F32, F33, F34.1 (depression disorders), F40, F41, F42 and F43 (anxiety disorders).
Self-reported depression and anxiety symptoms were measured by the Patient Health Questionnaire-4 (PHQ-4) [30] in 2022 (at age 21). The PHQ-4 is a widely used, ultra-brief screening tool with well-established reliability and validity for measuring depression and anxiety in the general population [31]. The frequency of depression and anxiety symptoms over the last 2 weeks were assessed with two items each, resulting in a composite PHQ-4 score (α = 0.81) ranging 0–12, where 0–2 indicated ‘None’, 3–5 ‘Mild’, 6–8 ‘Moderate’ and 9–12 ‘Severe’ symptoms [30]. Using these cut-offs, a dichotomised variable was constructed, with 0 representing ‘None or mild symptoms’ and 1 indicating ‘Moderate or severe symptoms’.
Covariates
While information on sex was derived from the participants’ personal identification numbers, distinguishing between sex and gender is not feasible due to the nature of the data. Additionally, since biological factors (linked to sex) and social factors (linked to gender) often interact, we assume that the measure may capture aspects of both sex and gender. Given the assumption that the relationships between sex/gender and the variables of interest are primarily driven by social rather than biological factors, the term ‘gender’ is employed throughout the article.
Living arrangements were determined from self-reported information. In 2019 (at age 18) respondents were categorised into the following groups: ‘Lives with both parents’; ‘Shared residence’; ‘Lives with one parent’; ‘Lives in own accommodation (apart from parents)’; and ‘Other’.
Educational status was based on self-reported data. In 2019 (at age 18), respondents were categorised as either ‘In high school’ or ‘Other’. The latter category included those who were ‘Working’ (n = 33), ‘Unemployed’ (n = 33) or ‘On parental leave’ (n = 3).
Parental education was assessed using register information, reflecting the highest level of education achieved by the participants’ guardians in 2017, and was categorised into four levels: upper secondary school for 2 years or less, upper secondary school for at least 3 years, tertiary education for 2 years or less and tertiary education at least 3 years.
Parental country of birth was also derived from register information. A dichotomous variable was constructed to differentiate between participants with at least one parent born in Sweden and those with both parents born outside of Sweden.
Family disposable income per consumption unit was obtained from registry information from 2019. The combined disposable incomes of both parents were divided by the consumption weights of all household members, resulting in a final measure expressed in hundreds of Swedish crowns per year, categorised into quartiles [32].
To assess prior depression and anxiety, we used information on depression and anxiety diagnoses from the National Patient Register from 2017 to 2018 (ages 16–17). Since these measures capture only cases diagnosed in specialised care and do not account for the full range of depression and anxiety symptoms, we also performed additional analyses using psychosomatic complaints at age 16 as a proxy, given their correlation with later depression and anxiety symptoms [33]. Psychosomatic complaints were assessed through self-reports in the Futura01 study using the question: ‘During the past 6 months, how often have you had. . .’ and were defined as experiencing two or more of the following complaints more than once per week: stomach aches, headaches or sleep difficulties. These items have previously been applied to measure psychosomatic complaints among young people [24,33-35]. The timeline of the data collection and sources for information on loneliness and mental health problems is presented in the Supplemental Material, Table S1.
Analytical strategy
First, we examined descriptive statistics for loneliness, depression and anxiety and sociodemographic characteristics for all and stratified by gender. Since depression and anxiety in young adulthood tend to be gendered, with a higher prevalence among females [18], and findings on loneliness being mixed [19], gender differences were investigated using χ2 tests. Second, we conducted crosstabulations and χ2 tests to analyse how loneliness at age 18 varied by sociodemographic characteristics and prior depression and anxiety diagnoses, overall, and by gender. Third, we used logistic regression to examine the relationships between loneliness and subsequent depression and anxiety. Given the potential impact of loneliness on the onset and the prevalence of mental health problems, loneliness at age 18 was examined as the exposure. The outcomes included (a) depression and anxiety diagnoses at ages 19–20 and (b) self-reported depression and anxiety symptoms at age 21. Crude models, incorporating one variable at a time, were followed by Model(s) 1, adjusting for sociodemographic characteristics, and Model(s) 2, additionally adjusting for prior depression and anxiety diagnoses. Interaction terms between loneliness and all sociodemographic characteristics were tested using Stata’s factorial notation and evaluated with a Wald test. All statistical analyses were performed using Stata 17.0.
Results
Table I displays the descriptives for the analytical sample. About 14% of participants reported loneliness at age 18, with a higher prevalence in females. Furthermore, 4.5% and 6.0% of respondents had depression and anxiety diagnoses at ages 16–17 and 19–20, respectively, with more cases among females. At age 21, 22.3% of the participants reported depression and anxiety symptoms, with a higher prevalence among females. At age 18, the majority of participants were still in high school (98.2%). Around two-thirds lived with both parents (63.4%), and nearly half had a parent with at least 3 years of tertiary education (45.8%). A majority of the participants had at least one parent born in Sweden (84.3%). Descriptives for depression and anxiety diagnoses and self-reported depression and anxiety symptoms separately are displayed in Supplemental Table S2.
Distributions of loneliness, mental health problems and sociodemographic characteristics for all and by gender. Differences by gender assessed with χ2 tests (N = 3828).
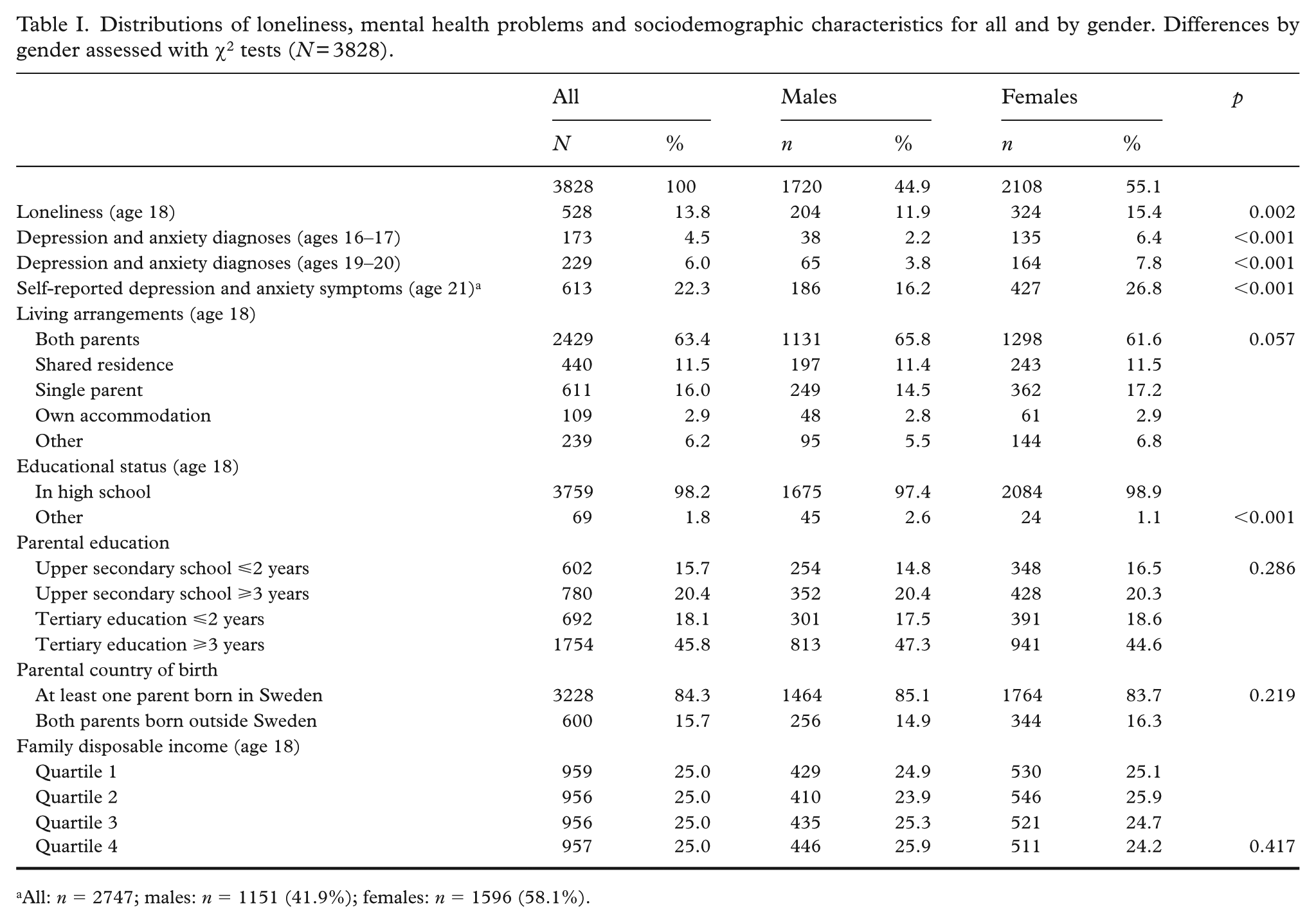
All: n = 2747; males: n = 1151 (41.9%); females: n = 1596 (58.1%).
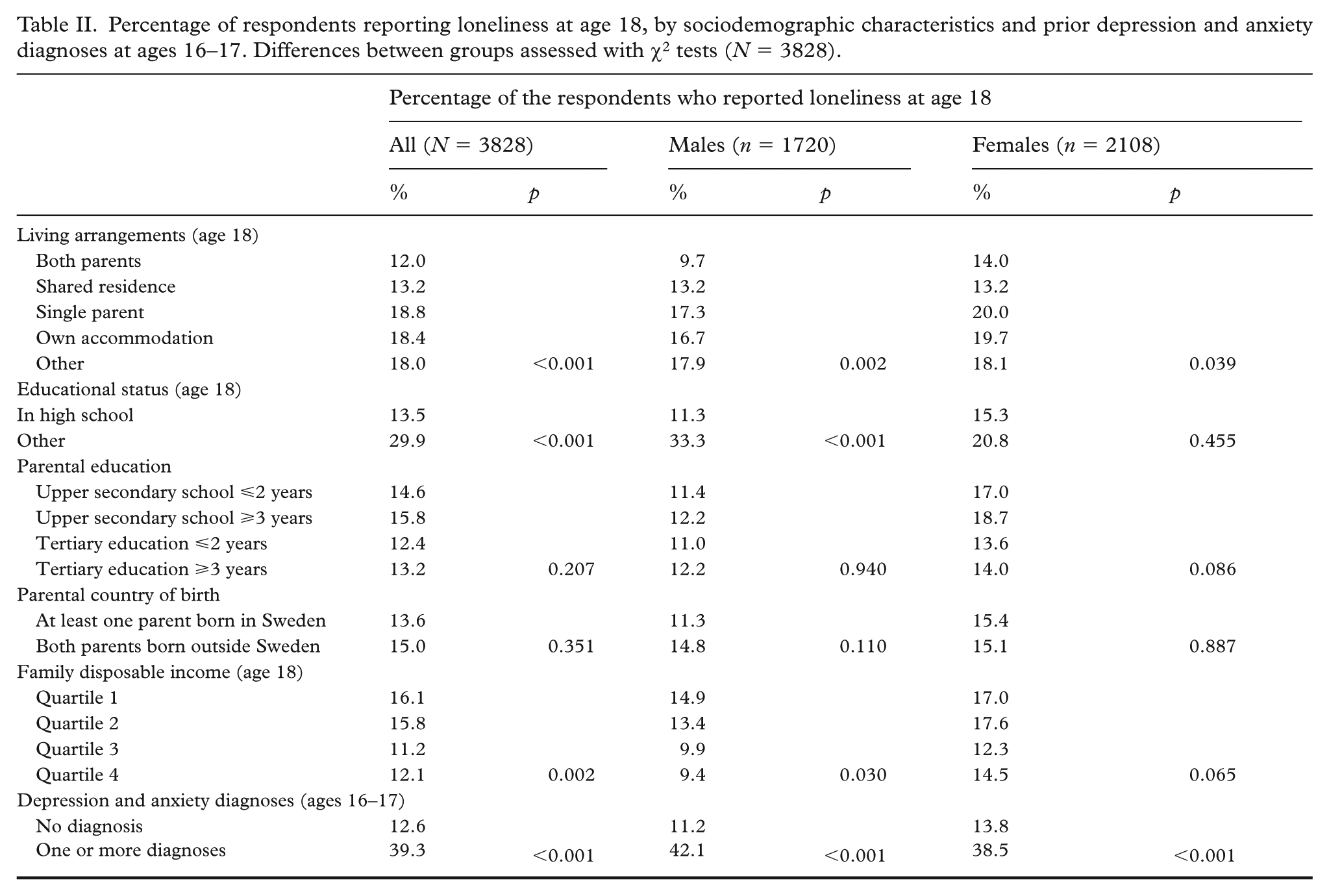
Table II displays loneliness at age 18 by sociodemographic characteristics, as well as prior depression and anxiety diagnoses, for the overall sample and separately for males and females. Loneliness was more prevalent among individuals living with a single parent, in own accommodation or in other living arrangements, compared with those living with both parents or in shared residence. Loneliness was also more common among those who did not attend high school. No statistically significant differences in loneliness were observed based on parental education or country of birth. However, loneliness was more common among participants from families with lower disposable income (quartiles 1 and 2) and among those with prior depression or anxiety diagnoses. These patterns were consistent in both males and females.
Percentage of respondents reporting loneliness at age 18, by sociodemographic characteristics and prior depression and anxiety diagnoses at ages 16–17. Differences between groups assessed with χ2 tests (N = 3828).
Results from logistic regression models analysing the associations between loneliness at age 18 and depression and anxiety diagnoses at ages 19–20 are presented in Table III. Loneliness was associated with depression and anxiety diagnoses in the crude model (odds ratio (OR) = 4.87; 95% confidence interval (CI): 3.64, 6.51) as well as in Model 1 (OR = 4.47; 95% CI: 3.33, 6.00) and Model 2 (OR = 3.48; 95% CI: 2.46, 4.91). The results of Model 2 further showed that, being female (OR = 1.64; 95% CI: 1.18, 2.28) and living with a single parent (OR = 1.64; 95% CI: 1.10, 2.44) was associated with a higher likelihood of receiving a depression or anxiety diagnosis. Having both parents born outside Sweden (OR = 0.30; 95% CI: 0.16, 0.58) and higher family income (OR = 0.58; 95% CI: 0.36, 0.91 and OR = 0.52; 95% CI: 0.32, 0.84 for quartiles 3 and 4, respectively) was linked to a lower likelihood of receiving a depression or anxiety diagnosis. Previous depression and anxiety diagnoses were associated with a higher likelihood of having these diagnoses at ages 19–20 (OR = 12.39; 95% CI: 8.48, 18.09). Additional adjustment for prior psychosomatic complaints (at age 16) was performed but did not change the overall pattern (data not presented). Interaction terms between sociodemographic characteristics and loneliness were tested but were not statistically significant.
Results from prospective analyses of depression and anxiety diagnoses at ages 19–20 by loneliness at age 18. Odds ratios (OR) and 95% confidence intervals (CI) from logistic regressions (N = 3828).
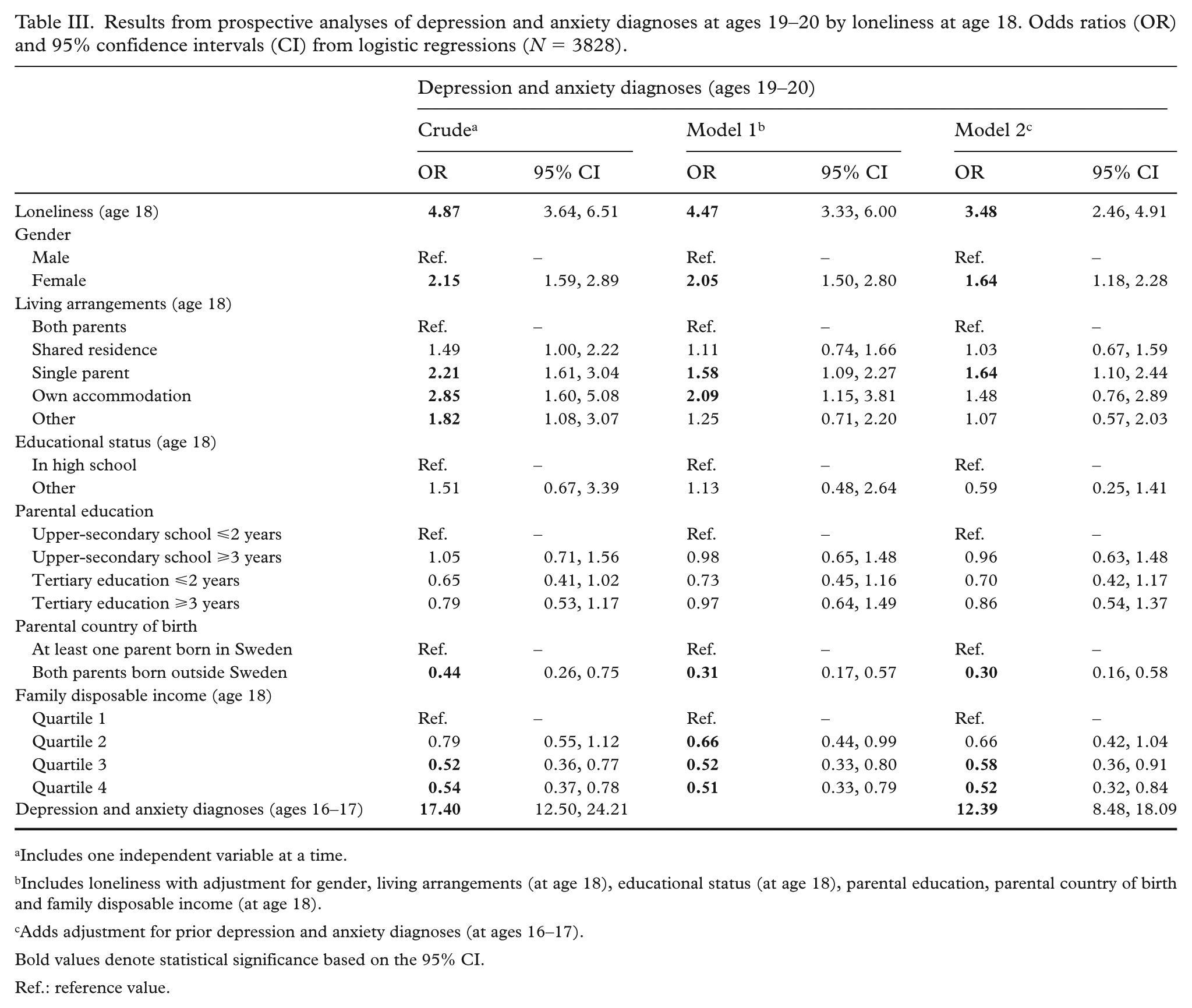
Includes one independent variable at a time.
Includes loneliness with adjustment for gender, living arrangements (at age 18), educational status (at age 18), parental education, parental country of birth and family disposable income (at age 18).
Adds adjustment for prior depression and anxiety diagnoses (at ages 16–17).
Bold values denote statistical significance based on the 95% CI.
Ref.: reference value.
Results from the analyses of the associations between loneliness at age 18 and self-reported depression and anxiety symptoms at age 21 are presented in Table IV. Loneliness was associated with depression and anxiety symptoms in the crude analysis (OR = 2.89; 95% CI: 2.31, 3.62), in Model 1 (OR = 2.72; 95% CI: 2.15, 3.43) and in Model 2 (OR = 2.48; 95% CI: 1.95, 3.14). Model 2 further showed that being female (OR = 1.78; 95% CI: 1.45, 2.19) and having both parents born outside Sweden (OR = 1.47; 95% CI: 1.12, 1.93) was associated with increased odds of reporting these symptoms, while having higher family disposable income (OR = 0.69; 95% CI: 0.51, 0.94 and OR = 0.68; 95% CI: 0.50, 0.93 for quartiles 3 and 4, respectively) was associated with reduced odds. Having depression and anxiety diagnoses at ages 16–17 was associated with a higher likelihood of reporting depression and anxiety symptoms at age 21 (OR = 3.10; 95% CI: 2.12, 4.54). Additional adjustment for prior psychosomatic complaints (at age 16) was performed but did not change the overall pattern (data not presented). Tests for interactions between sociodemographic characteristics and loneliness revealed no statistically significant results.
Results from prospective analyses of self-reported depression and anxiety symptoms at age 21 by loneliness at age 18. Odds ratios (OR) and 95% confidence intervals (CI) from logistic regressions (n = 2747).
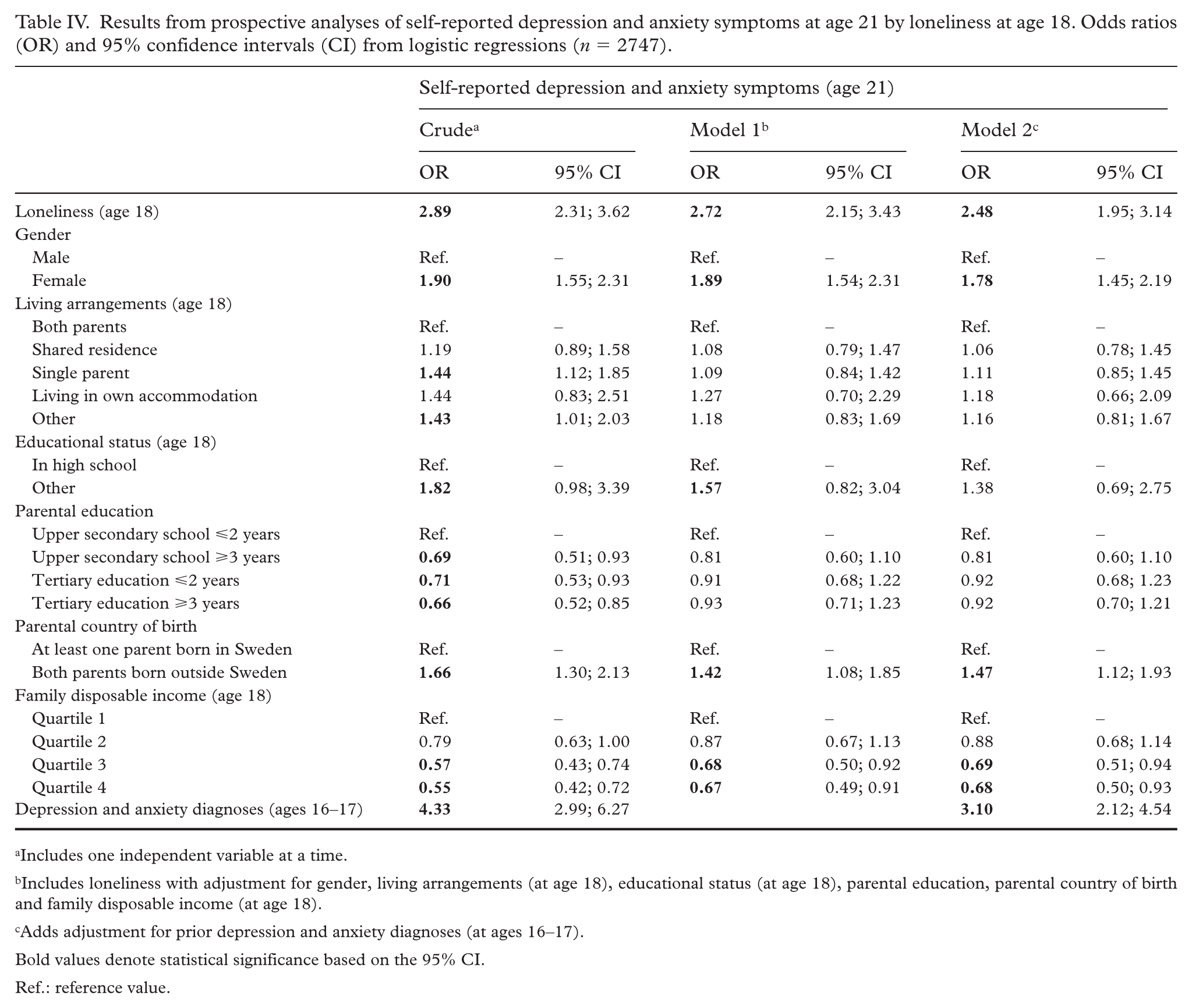
Includes one independent variable at a time.
Includes loneliness with adjustment for gender, living arrangements (at age 18), educational status (at age 18), parental education, parental country of birth and family disposable income (at age 18).
Adds adjustment for prior depression and anxiety diagnoses (at ages 16–17).
Bold values denote statistical significance based on the 95% CI.
Ref.: reference value.
Additional analyses limited to participants who did not have depression and anxiety diagnoses at ages 16–17 revealed consistent results with those presented in Tables III and IV (data not presented). Furthermore, when depression and anxiety – both in terms of diagnoses and symptoms – were examined separately for each condition, similar patterns emerged (data not presented).
Discussion
Loneliness at age 18 was positively associated with depression and anxiety diagnoses at ages 19–20, as well as with self-reported depression and anxiety symptoms at age 21, even after adjustment for sociodemographic characteristics and prior depression and anxiety diagnoses. Loneliness can adversely affect mental health through several interrelated mechanisms, including elevated perceived stress, diminished self-esteem, reduced self-regulation and maladaptive coping strategies [7,11]. Loneliness has been linked to cognitive biases related to social threat, characterised by heightened sensitivity to negative social stimuli and negative cognitive patterns [11,36]. Negative cognitive biases and coping strategies may further reduce opportunities for meaningful connection and contribute to more negative and less satisfying interpersonal interactions [36]. Over time, impaired social functioning can contribute to mental health problems, either leading to negative moods directly or by activating stress response systems involved in the development and persistence of mental health problems such as anxiety and depression.
The findings of the current study align with previous research demonstrating that loneliness is linked to depression and anxiety during this emerging adulthood – a life stage marked by multiple social transitions [6-7,37]. The instability and changes typical for this period may contribute to increased risk of loneliness, as acknowledged by emerging adults themselves [17]. A study using US data from the National Longitudinal Study of Adolescent Health (Add Health) demonstrated a prospective association between loneliness and diagnosed depression in emerging adults, even after accounting for prior depression symptoms [38]. However, this study did not explore other mental health problems. While Laustsen et al. [8] found a higher prevalence of pre-existing mental disorders among lonely individuals, their analysis included broad age ranges (16–65 and >65 years) and did not incorporate self-report data on mental disorders, which were based on hospital-based diagnoses and categorised broadly. To our knowledge, the present study is the first to investigate the longitudinal associations between loneliness and depression and anxiety in emerging adults, considering both self-reported symptoms and registered diagnoses, while adjusting for prior mental health problems.
Loneliness at age 18 was more common among those with previous depression and anxiety diagnoses. This supports previous research indicating that loneliness, being multifaceted and closely intertwined with mental health [10], has a reciprocal relationship with mental health issues [12]. Prior studies have demonstrated an association between mental health problems and subsequent loneliness among youth [7,10,16]. Potential mechanisms may include discrimination or stigma associated with mental health problems, or use of social isolation as a coping strategy to handle stress, which can lead to elevated loneliness [12]. Therefore, attempts to address loneliness should consider the interconnected nature of the relationship between loneliness and mental health.
While previous research on gender differences in loneliness has yielded mixed results, with a meta-analysis by Maes et al. [39] showing no clear pattern, our study indicated a slightly higher prevalence of loneliness at age 18 among females. A qualitative study on loneliness in young adults demonstrated that females tend to engage in social comparisons more often than males [40], which can be one of the potential explanations of this difference. Another factor that may contribute to gender differences in loneliness at this age is the higher prevalence of mental health problems among females [18], given the complex and interconnected relationship between loneliness and mental health [10,12]. Additionally, loneliness was more prevalent among individuals not attending school at age 18, supporting findings from prior research [7]. A study by Matthews et al. [7] demonstrated that loneliness in 18-year olds was distributed evenly across socioeconomic groups defined by household income, parental education and social class. Our study found no significant variation in loneliness based on parental education; however, loneliness was more common among individuals with lower family disposable income. Our study also showed that loneliness was more frequently reported by individuals not living with both parents or in shared residence, compared with those in such living arrangements. Although some sociodemographic differences were observed in both loneliness and mental health problems, the association between loneliness and mental health problems remained consistent across all sociodemographic groups. While Steen et al. [37] found that the link between loneliness and depression symptoms was stronger in young adult males than in females, we did not find evidence of any gender differences in the tested associations, aligning with the findings of Goosby et al. [38].
A major strength of this study was the use of a national cohort sample. The linkage between self-reported data and register information further reinforced the study. Firstly, register data provided reliable information on sociodemographic characteristics, while self-reports added valuable information not captured by the registers. Secondly, the use of both diagnoses and self-reported symptoms offered a more comprehensive understanding of how loneliness may impact depression and anxiety. Importantly, not all self-reported symptoms fulfil diagnostic criteria. Furthermore, among individuals whose conditions meet diagnostic criteria, not everyone receives a formal diagnosis – often referred to as ‘unmet care needs’ or ‘treatment gaps’ [41]. Additionally, self-reported symptoms were measured using a validated and well-established instrument. Self-report data also enabled capturing loneliness, which, being a subjective feeling, can be only measured with information or accounts provided by participants themselves. However, the data also had limitations. The potential underrepresentation of certain groups of students at baseline, along with attrition across study waves, may have compromised the generalisability of the findings. While no systematic differences were observed between participating and non-participating schools in terms of school-level sociodemographic characteristics or average academic performance [23], differences may still have existed between participating and non-participating individuals at baseline. Furthermore, attrition between the study waves was somewhat higher among males, individuals with parents who had less than tertiary education and those with two parents born abroad [24,25]. Importantly, however, the prevalence of high loneliness at t2 did not substantially differ between those who participated in t3 and those who did not (data not presented). It is also worth noting that since the information on psychiatric diagnoses was drawn from register data, there was no additional attrition in the corresponding analysis. Another limitation of this study was that the diagnoses recorded in the National Patient Register include specialised care only and do not include those from primary care. Furthermore, questions on depression and anxiety symptoms were included only in the third survey wave. Consequently, when adjusting for prior mental health problems in the analysis of depression and anxiety symptoms, register data on depression and anxiety diagnoses were used. Thus, it is likely that some participants with depression and anxiety symptoms, but without formal diagnoses, were not included in the adjustments. Additionally, self-report screening tools can hold a risk of overestimating the prevalence of symptoms when used to assess population-level prevalence [42]. Another limitation is that loneliness was assessed using a single item, which restricted the ability to explore its dimensionality. Future research could benefit from examining various dimensions of loneliness.
Conclusion
This study contributes to the growing body of evidence suggesting that loneliness can lead to mental health problems, specifically highlighting its association with depression and anxiety diagnoses, as well as related symptoms among emerging adults. Loneliness experienced during the life period marked by major social transitions, may contribute to subsequent depression and anxiety. Addressing loneliness among emerging adults, for instance, through education, job or living transition support activities, could help reduce mental health problems.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948251403064 – Supplemental material for Loneliness and subsequent depression and anxiety in emerging adults: Findings from a Swedish cohort study
Supplemental material, sj-docx-1-sjp-10.1177_14034948251403064 for Loneliness and subsequent depression and anxiety in emerging adults: Findings from a Swedish cohort study by Karina Grigorian, Viveca Östberg, Jonas Raninen and Sara Brolin Låftman in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The authors would like to thank all participants in Futura01.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported by the Swedish Research Council for Health, Working Life and Welfare (Forte) (grant nos. 2021-00537; 2022-01050) and Region Stockholm (grant no. RS 2021-0331).
Open access funding was provided by Stockholm University.
Ethical considerations
The study was approved by the Swedish Ethical Review Authority (ref. 2021-06504-01; 2022-02781-02; 2022-06502-02). Informed consent was obtained from all study participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.