
Abstract
Aims:
Using a longitudinal approach, the aim of this study was to examine whether baseline engagement in arts and culture was associated with a decline from ‘Good’ to ‘Poor’ health at follow-up.
Methods:
Self-rated health (SRH) and engagement in six cultural activities among randomly selected Danish adults (⩾15 years) were assessed using data from the Danish Health and Wellbeing Survey in 2019. One year later, all individuals were invited to complete a follow-up survey questionnaire. SRH was dichotomised into ‘Good’ (very good/good) and ‘Poor’ (fair/bad/very bad). The cultural participation index (CPI) was used to measure engagement in arts and culture activities. Each activity was scored from 0 (never) to 4 (at least once a week). The total score across all activities could reach a maximum of 24. Adjusted logistic regression models assessed associations between cultural participation and poor health at 1-year follow-up.
Results:
The present study included 3286 individuals who perceived their health as good at baseline who completed both survey waves; 11.2% reported poor health at follow-up. Individuals who attended concerts and musical events at least once every 3 months were less likely to report poor health at follow-up (adjusted odds ratio (OR): 0.50, 95% confidence interval (CI): 0.35–0.71) than individuals who never attend concerts and musical events. Furthermore, a 1-point-higher CPI score was associated with a 0.96 (95% CI: 0.93–0.99) lower (adjusted) OR of reporting poor health at follow-up.
Conclusions :
This follow-up study extends our understanding of the positive health outcomes from engagement in arts and culture activities.
Introduction
Global health challenges are multifaceted, necessitating innovative approaches to health promotion and disease prevention [1–4]. Increasingly, engagement in arts and cultural activities has been recognised as a significant contributor to health and wellbeing across various populations [5–9]. Previous research has consistently demonstrated that participation in arts and culture activities is associated with a range of positive health outcomes, including enhanced mental health, reduced stress, and improved social cohesion [8,10,11].
For instance, a study by Davies et al. [12] found that individuals who regularly attended arts and cultural events such as concerts and art exhibitions reported significantly lower levels of anxiety and depression. Similarly, Løkken et al. [7] observed arts and culture engagement to be associated with lower all-cause mortality as well as fewer general practitioner visits, especially among men. Significantly, Santini et al. [6] found that those who attended concerts, the theatre, museums or the cinema at least once per quarter had 57% lower odds of developing depression over the following year compared to those who never engaged. Our previous study involving over 6600 Danish adults found that every 1-point increase in arts and cultural participation (e.g. concerts, exhibitions, library visits) was associated with a 10% higher likelihood of reporting good self-rated health (SRH) after adjusting for relevant covariates [13]. Individuals who frequently engaged in such arts and cultural activities – such as visiting libraries, attending concerts, participating in choirs or orchestras, and attending theatre or art exhibitions – were more likely to report good health. While these 2023 findings indicated promising outcomes regarding the role of arts and culture engagement in promoting individual and social health and wellbeing, the long-term effects on SRH remain uncertain.
Observing the health and wellbeing benefits associated with participation in arts and culture activities can inform the development of targeted health promotion and disease prevention strategies, particularly through intersectoral collaborations. However, although these cross-sectional findings highlight the positive associations between arts engagement and SRH, they also raise important questions about the sustainability and broader impact of such effects over time, as noted in other studies [7,14].
The aim of the present study was to examine whether baseline engagement in arts and culture was associated with a decline from ‘Good’ to ‘Poor’ health at follow-up 1 year later.
Methods
Study design and setting
The study’s data were derived from the Danish Health and Wellbeing Survey in 2019, and a follow-up survey carried out 1 year later. The baseline survey in 2019 was conducted as part of the third wave of the European Health Interview Survey. The primary objective of the survey in 2019 was to provide information on health status, health determinants and healthcare utilisation of the Danish population. In all, 14,000 Danish residents aged 15 years or older (no upper age limit) were randomly selected from the Danish Civil Registration System [14].
An invitation letter was sent to all selected individuals (N = 14,000) in 2019. Individuals registered to use Digital Post (a secure digital mail service) received the letter through this system. The letter outlined the purpose, content and importance of the survey. Furthermore, the letter included instructions on how to complete the online questionnaire. In 2019, a small segment of the population (8.3%) had deregistered Digital Post. These individuals were sent an invitation letter, a paper questionnaire, and a prepaid return envelope by regular postal mail. The letter to this group also included instructions on how to complete the online questionnaire. Data were collected between September and December 2019.
All individuals who were still alive and resident in Denmark by mid-August 2020 were invited to participate in a follow-up questionnaire survey on the public health consequences of the COVID-19 pandemic. Hence, 13,474 individuals were invited to the follow-up survey. Overall, the same methodology as in the 2019 wave was applied. In Denmark, individuals holding permanent residency are assigned a personal identification number [15]. This unique identifier facilitated the linkage of baseline and follow-up survey data at the individual level. Follow-up data were collected between September and November 2020.The study design and methodology of the Danish Health and Wellbeing Survey in 2019 along with the follow-up survey in 2020 have been extensively described elsewhere [15].
Measures
All respondents in 2019 were queried about their typical frequency of engagement in each of the following arts and cultural activities: concerts or musical events (including festivals); participation in a choir, band, or orchestra; theatre show or other performing arts; cinema; art museum or exhibition; library. The available response categories for all activities were ‘at least once a week’, ‘at least once a month’, ‘at least once every three months’, ‘at least once a year’, and ‘never’. In a recent study that also used data from the Danish Health and Wellbeing Survey in 2019 a cultural participation index (CPI) was generated (see Jensen et al. [13]). For each activity, the response categories were allocated the following scores: ‘at least once a week’ (score = 4), ‘at least once a month’ (score = 3), ‘at least once every three months' (score = 2), ‘at least once a year’ (score = 1), and ‘never’ (score = 0). The scores from all activities were added up, with a maximum possible score of 24. It should be noted that the question on engagement in arts and cultural activities was not asked in the follow-up survey since cultural venues and events in Denmark were closed for a long period of time in 2020.
We collected information on SRH in both 2019 and 2020 from the following question: ‘How is your health in general? Is it. . .’ with the following five response categories: ‘very good’, ‘good’, ‘fair’, ‘bad’ and ‘very bad’ [16]. The response categories were collapsed into a dichotomous response: ‘Good health’ (very good or good) and ‘Poor health’ (fair, bad or very bad).
To maintain methodological consistency and ensure comparability, the potential confounders selected mirrored those used in our previous cross-sectional study [13]. Thus, data regarding sex, age, marital status, country of birth and municipality of residence were derived from the Danish Civil Registration System [15]. We utilised Eurostat’s classification of degree of urbanisation (DEGURBA) to categorise municipalities into three types of areas: ‘cities’, ‘towns and suburbs’ and ‘rural areas’ [17].
The individuals were categorised into three broad groups relating to country of birth based on Statistics Denmark’s definition of Western countries: ‘Denmark’, ‘other Western countries’, and ‘non-Western countries’. The following countries were regarded as Western countries: the 27 European Union Member States, the UK, Andorra, Iceland, Liechtenstein, Monaco, Norway, San Marino, Switzerland, the Vatican City State, Australia, New Zealand, Canada and the USA. Countries outside the Western category were defined as non-Western countries. The highest completed level of education served as a proxy for socio-economic status in the present study. Data regarding individuals’ highest completed education level relied on self-reported information and were categorised into three groups: ‘basic school’, ‘upper secondary or vocational education’, and ‘higher education’.
Statistical analysis
We examined whether a transition from the ‘Good health’ category at baseline to the ‘Poor health’ category at follow-up was related to the frequency of engagement in arts and culture activities at baseline. We report descriptive statistics using percentages and means with standard deviations (SDs). Logistic regression models were used to examine the associations between participation frequency in various cultural activities and the CPI score, respectively, and reporting poor health at 1-year follow-up. First, an unadjusted model was used to examine the associations. In the second model, the associations were adjusted for sex and age. The last model was further adjusted for marital status, highest completed education level, country of birth, and degree of urbanisation. The latter models were restricted to individuals who were likely to have completed their education (i.e. individuals aged ⩾25 years, n = 3031). The CPI score was both treated as a continuous variable and grouped to simplify the interpretation of the results into four groups: ‘0’, ‘1–4’, ‘5–8’ and ‘⩾9’. We used the category ‘5–8’ as the reference group because it was the largest group in our sample. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for all logistic regression models. Additionally, we examined whether the association between participation in cultural activities and poor SRH health at follow-up differed by sex, by including interaction terms in the logistic regression models. No statistically significant interactions were revealed and, thus, the results are not presented separately for men and women. SAS version 9.4 was utilised for performing statistical analyses [18].
Results
In all, 6629 individuals (47%) completed the questionnaire in 2019, of which 5000 also completed the questionnaire in 2020. Thus, the follow-up response proportion was 75%. The baseline population was restricted to the 3510 individuals who rated their health as good at baseline. Of these, 3286 individuals also completed the question on SRH at follow-up (see the flowchart in Figure 1).
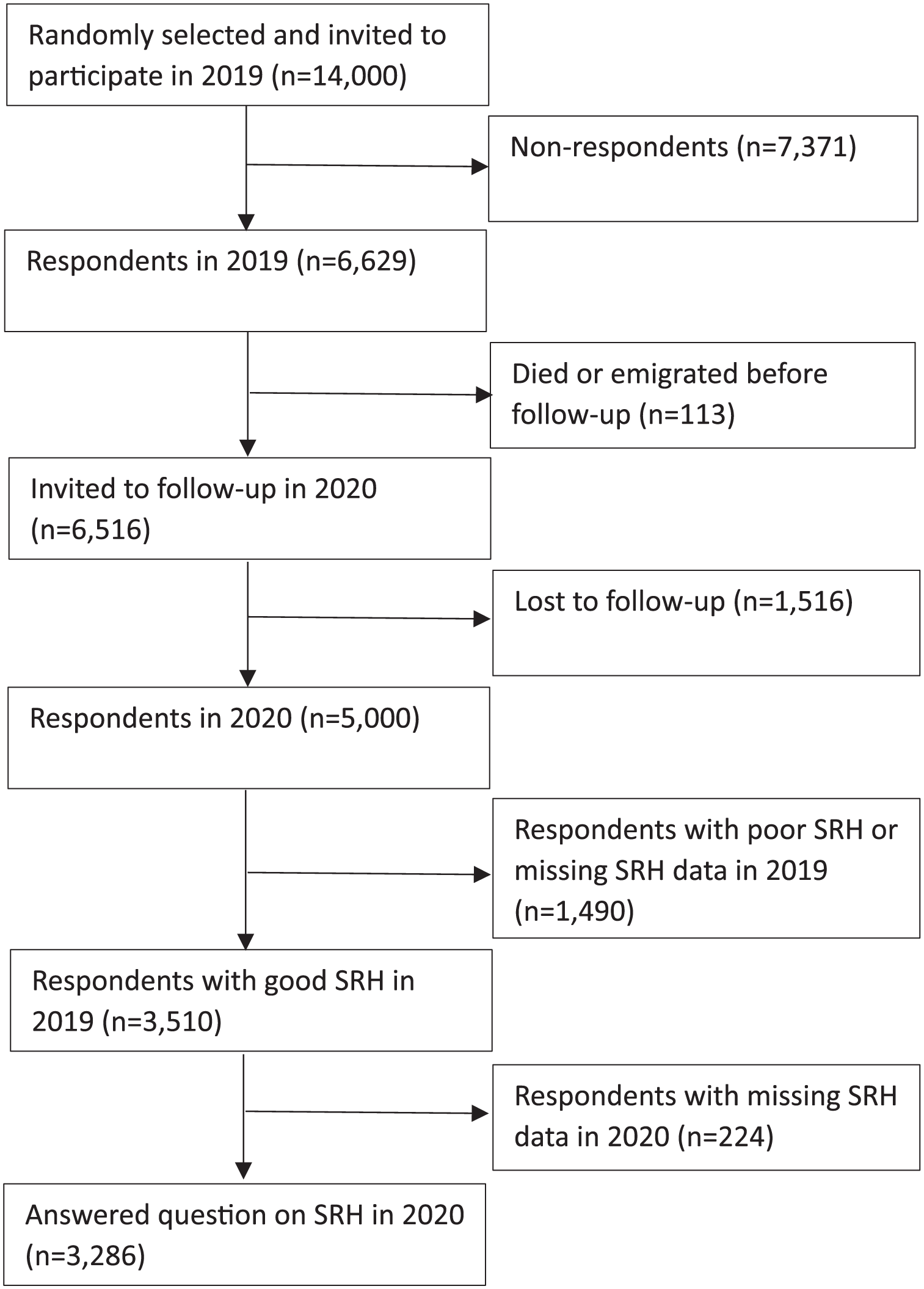
Flowchart of respondents included in the follow-up study in 2020.
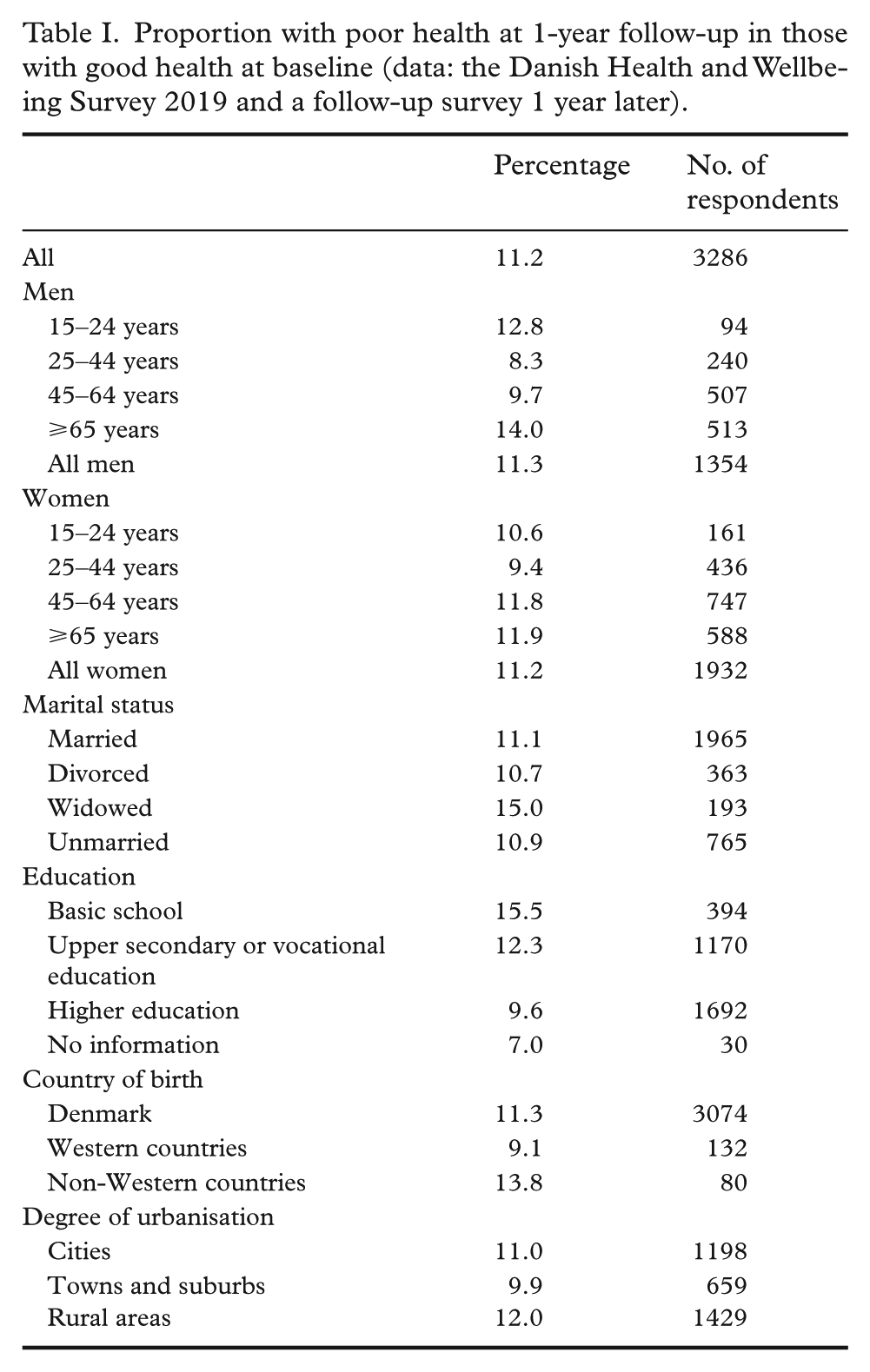
Table I shows that 11.2% of the 3286 individuals who rated their health as good at baseline rated their health as poor at follow-up 1 year later. An equal proportion of men (11.3%) and women (11.2%) rated their health as poor at follow-up.
Proportion with poor health at 1-year follow-up in those with good health at baseline (data: the Danish Health and Wellbeing Survey 2019 and a follow-up survey 1 year later).
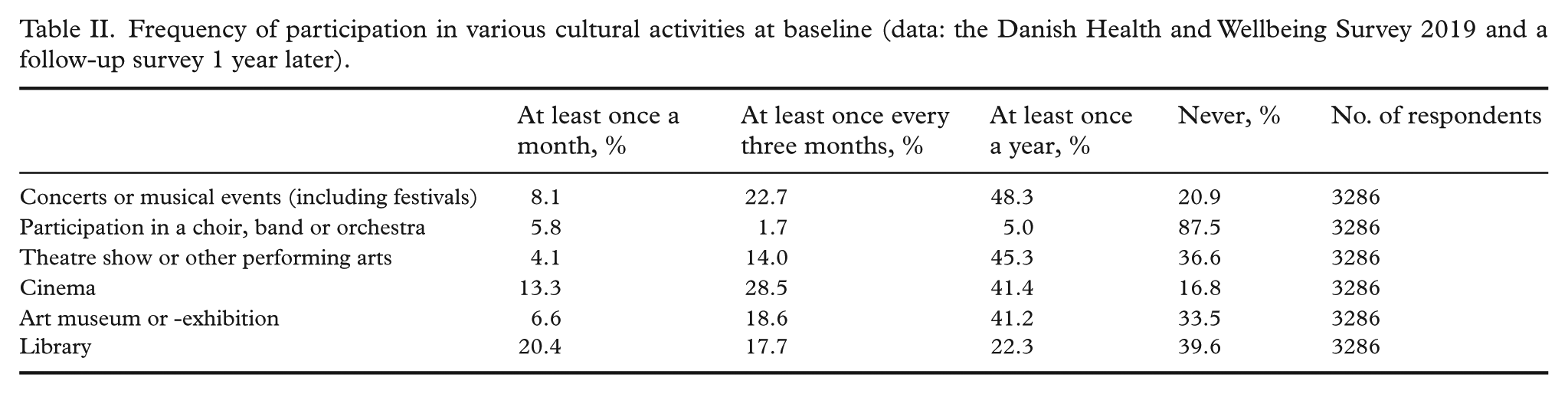
The frequencies of participation in various cultural activities at baseline among respondents who answered the question on SRH in both 2019 and 2020 are shown in Table II. For all categories, the two highest response categories were combined into a single category due to the limited number of ‘at least once a week’ responses. The most frequently attended activities, at least once a month, were visiting a library (20.4%) and going to the cinema (13.3%).
Frequency of participation in various cultural activities at baseline (data: the Danish Health and Wellbeing Survey 2019 and a follow-up survey 1 year later).
Both the unadjusted and adjusted logistic regression models revealed that a higher frequency of attending concerts and musical events, and theatre shows or other performing arts, respectively, were associated with better SRH at 1-year follow-up (Table III). For example, individuals who attended concerts and musical events at least once every 3 months were less likely to report poor health at follow-up (OR: 0.50, 95% CI: 0.35–0.71) than individuals who never attend concerts and musical events (fully adjusted model). The corresponding OR for those attending concerts and musical events at least once a year was 0.60 (95% CI: 0.46–0.79). The OR for those attending concerts and musical events at least once a month was 0.74 but with a broad CI (95% CI: 0.48–1.16).
Prevalence and odds ratios (95% confidence intervals) of reporting poor health at 1-year follow-up (data: the Danish Health and Wellbeing Survey 2019 and a follow-up survey 1 year later).
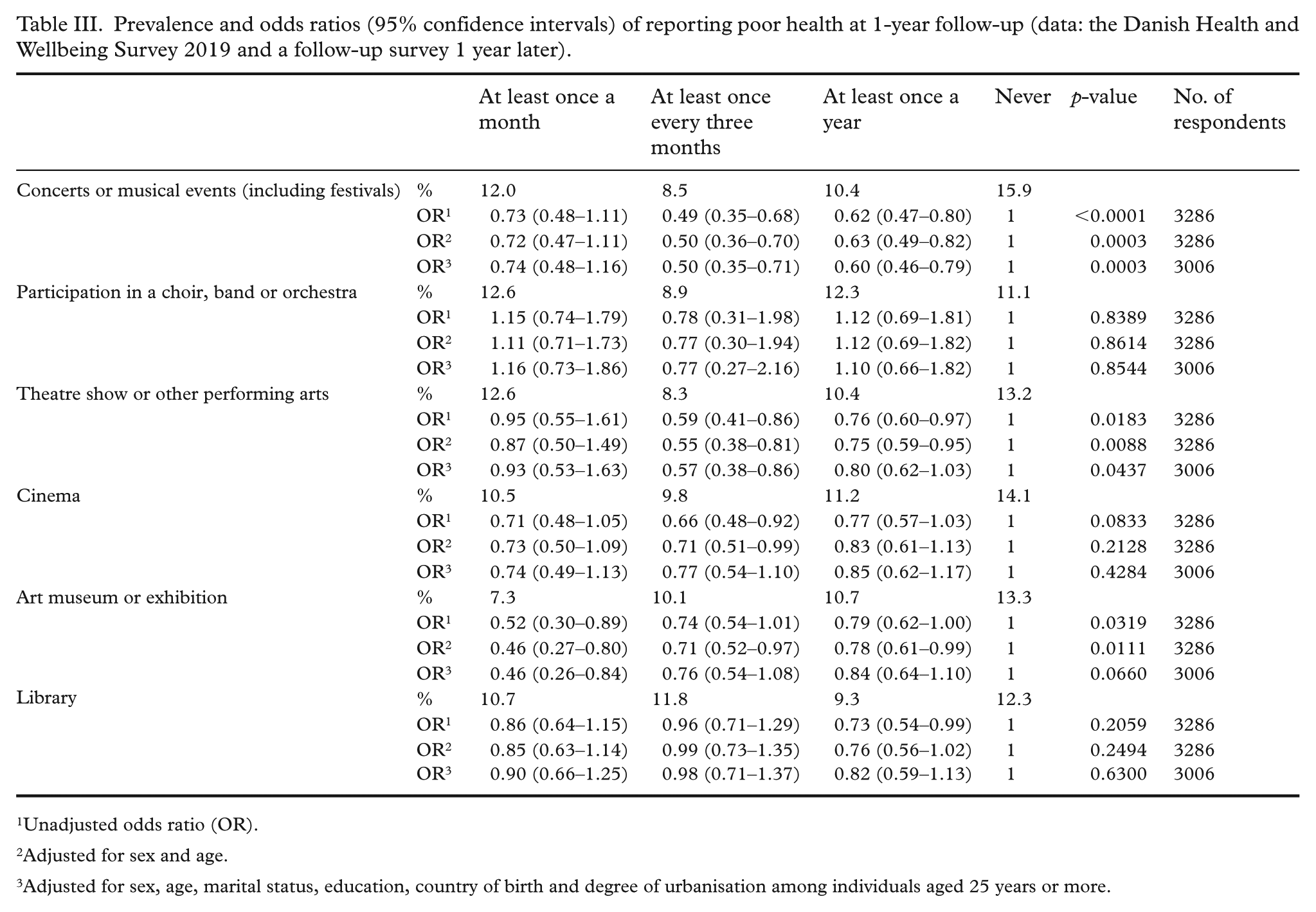
Unadjusted odds ratio (OR).
Adjusted for sex and age.
Adjusted for sex, age, marital status, education, country of birth and degree of urbanisation among individuals aged 25 years or more.
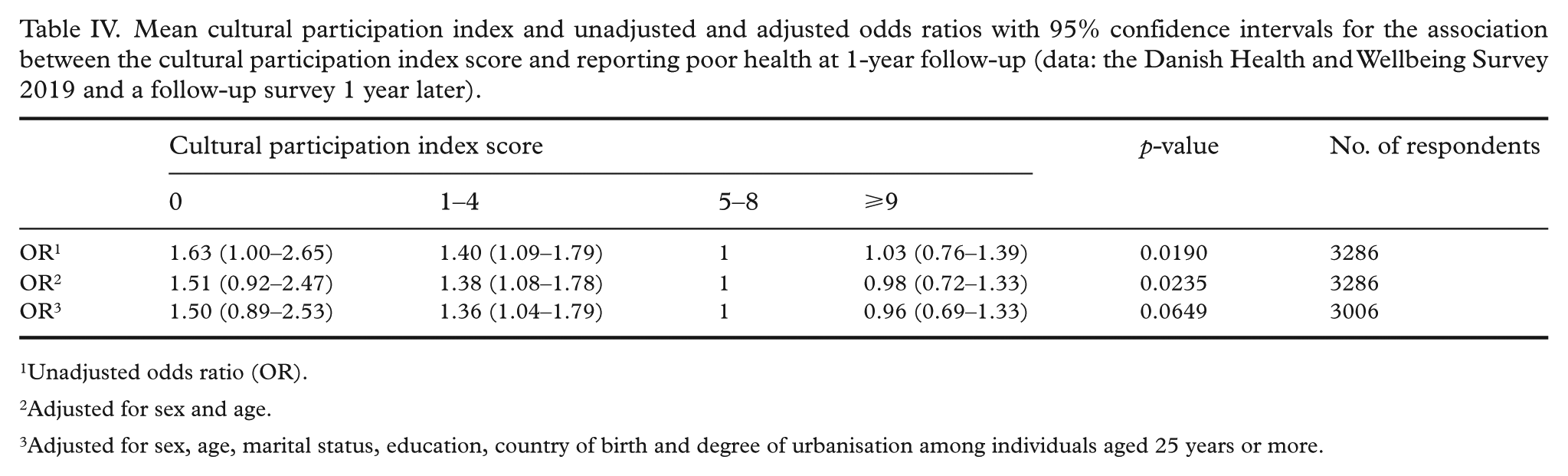
The overall mean CPI score at baseline was 5.9 (SD: 3.6). In the unadjusted logistic regression model, a 1-point higher CPI score was associated with a 4% lower OR of reporting poor health at 1-year follow-up (OR: 0.96, 95% CI: 0.93–0.99; data not shown). The fully adjusted model did not alter the OR (OR: 0.96, 95% CI: 0.93–0.99). In Table IV, the CPI score is presented according to the four defined levels.
Mean cultural participation index and unadjusted and adjusted odds ratios with 95% confidence intervals for the association between the cultural participation index score and reporting poor health at 1-year follow-up (data: the Danish Health and Wellbeing Survey 2019 and a follow-up survey 1 year later).
Unadjusted odds ratio (OR).
Adjusted for sex and age.
Adjusted for sex, age, marital status, education, country of birth and degree of urbanisation among individuals aged 25 years or more.
The unadjusted logistic regression model also revealed that the grouped score was associated with poor SRH at 1-year follow-up (p = 0.02). The fully adjusted model did not reach statistical significance (p = 0.06). However, it indicated an inverse dose-response relationship between the CPI score and reporting poor health at follow-up. Hence, individuals who never participated in arts and culture activities (score = 0) had 1.50 (95% CI: 0.89–2.53) times higher odds of reporting poor health at follow-up compared to individuals with a score of 5–8. Individuals with a score of 9 or higher had 0.96 (95% CI: 0.69–1.33) times lower odds of reporting poor health at follow-up compared to individuals with a score of 5–8.
Discussion
The current follow-up study addresses SRH 1 year later, providing valuable insights showing that the observations from the 2019 study were still significant in 2020, which strengthens the data by reducing the impact of recall error or bias.
A single-item question on SRH is the most widely utilised measure of health in population-based surveys. The specific phrasing and response categories of SRH questions may take different forms. While the levels and distributions of the questions are not directly comparable, they provide parallel assessments of the same phenomenon and generally yield consistent results [19]. Assessing SRH using s single-item question has several advantages. It is simple and clear, making it easy for respondents to comprehend and respond to. Furthermore, it captures both mental and physical components of health and it is a strong predictor of morbidity and mortality [20–22].
Baseline data were collected in the last months of 2019 just before the COVID-19 pandemic hit Europe and Denmark, while follow-up data were collected 1 year later. Denmark instated a lockdown in March 2020 to reduce the spread of COVID-19. The Danish lockdown restrictions included limits on public gatherings, travel restrictions, and the closure of schools, shops, workplaces, and cultural institutions open to the public. Starting in April 2020, some areas began to reopen gradually, with more significant easing in May and June. From June to August 2020, only minor restrictions remained, although the general recommendation to work from home persisted. By August 2020, a rise in COVID-19 cases led to the mandatory use of face masks in public indoor spaces. In September and October 2020, travel restrictions and limits on social interactions were reintroduced. The COVID-19 pandemic introduced many radical changes in our daily lives (including the lockdown of cultural venues and events) and the findings of the present study should be interpreted in light of the aforementioned conditions. In this context, it is worth mentioning that a recent study showed that there is no evidence suggesting that digital cultural participating replaced physical participation during the lockdown periods in Denmark [23].
Beyond the COVID-19 pandemic, other studies using longitudinal data, including those by Lindström et al. [24] and Løkken et al. [7], have identified associations between arts and culture engagement and improved SRH scores among populations. Since SRH also has been shown to serve as a predictor of morbidity and mortality [21] it may be useful to investigate such associations further. Building on these findings, the present study emphasises arts engagement – defined here as participation in concerts, musical events (including festivals), choirs, bands or orchestras; theatre performances or other performing arts; cinema; art museums or exhibitions; and libraries – as a behaviour that positively supports SRH. Population cohort surveys have shown that arts and culture engagement reduces mortality, depression, stress, and enhances wellbeing [6,7,11,25]. Moreover, social medicine perspectives provide an analytical framework: arts can act as a social determinant that becomes internally embodied, can operate across biopsychosocial systems, and can enrich meaningfulness for individuals and community cohesion. While not a substitute for clinical care, involvement in the arts has been associated with improved health and wellbeing benefits, particularly when integrated into broader health and community strategies such as social prescribing [25]. In addition, social determinants of health, as recognised by the World Health Organization, emphasise that health is shaped not only by biology or behaviour, but also by the social, economic and environmental contexts in which people live, including conditions such as income, education and social inclusion [26]. Here arts and culture engagement can be seen as a positive health behaviour [27] within the broader context of healthy lifestyle promotion with longitudinal benefits.
Strengths and limitations
We acknowledge that our study has some limitations. Even though the response proportion was quite satisfactory, estimates may be subject to non-response bias. However, a low response proportion is not necessarily directly associated with non-response bias and there is no reason to believe that respondents and non-respondents are different in ways that matter for the conclusions drawn in this study. Furthermore, as previously described, follow-up data were collected shortly after the lockdown restrictions were lifted, but at a time when new restrictions were reintroduced (i.e. the early stage of the second wave of COVID-19). The COVID-19 pandemic and the associated restrictions had a considerable impact on the daily life of all Danes, but some groups in society were more affected than others [28]. For example, it seems obvious to assume that the temporary closing of cultural venues and events had a greater negative impact on individuals who, at baseline, were more engaged in arts and culture activities, compared to individuals who were less engaged in such activities. This is not necessarily a limitation of this study, but the results should be interpreted bearing this in mind. Moreover, as in all observational studies, the possibility of residual confounding cannot be ruled out. In addition, despite the rather large sample size, we did not examine additional potential interactions, as the statistical power probably would have been insufficient to examine such associations. Lastly, it is difficult to interpret the practical significance of the present study in a public health perspective. Unlike clinical measures, SRH is a subjective indicator of health status, making it difficult to quantify public health significance. This indicator also lacks standardised benchmarks that link small shifts to tangible health outcomes, and public health decisions often rely on quantifiable outcomes such as reduced disease incidence or healthcare costs. Nevertheless, SRH remains an important indicator because it predicts morbidity and mortality, suggesting that even modest improvements could have implications at the population level. To advance this area, future research should aim to establish these links by integrating objective health measures and conducting cost–benefit analyses to evaluate the potential public health impact of promoting arts and culture engagement for health.
The present study also has several strengths. Primarily, the design used made it possible to examine the longitudinal association between engagement in arts and culture activities and SRH. Another strength is the large study population of Danish adults. Longitudinal data collection minimises recall bias by capturing information at multiple time points, thereby reducing reliance on participants’ memory; this enhances data accuracy and reliability by tracking changes over time and observing trends in a systematic manner.
Conclusion
The findings suggest that individuals who regularly attend concerts and musical events experience better SRH outcomes over time compared to those who never attend such events. Specifically, concert attendance at least once every 3 months is associated with a significantly lower likelihood of reporting poor health at follow-up. Additionally, a higher CPI score is linked to reduced odds of reporting poor health, indicating that broader engagement in arts and culture activities may contribute to overall wellbeing. These findings underscore the potential benefits of arts and cultural participation for health and wellbeing, particularly in supporting the maintenance of positive SRH.
Supplemental Material
sj-xlsx-1-sjp-10.1177_14034948251399932 – Supplemental material for Arts and culture engagement for health: a Danish population-based follow-up study
Supplemental material, sj-xlsx-1-sjp-10.1177_14034948251399932 for Arts and culture engagement for health: a Danish population-based follow-up study by Anita Jensen, Lau Caspar Thygesen, Anna Paldam Folker, Martin Lindström and Ola Ekholm in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
According to Danish legislation, register-based and questionnaire studies are exempt from requiring approval by biomedical research ethics committees. This survey received approval from the Research & Innovation Organization (RIO) at the University of Southern Denmark (SDU). RIO is responsible for reviewing and approving all scientific and statistical research projects at SDU in accordance with the Danish Data Protection Regulation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.