
Abstract
Aims:
This systematic review and meta-analysis aimed to identify sociodemographic, lifestyle, and occupational risk factors for disability retirement among middle-aged workers.
Methods:
Searches were conducted in PubMed, Web of Science, PsychInfo, Scopus, and Google Scholar from their inception until February 2025. Observational longitudinal studies involving workers aged 40–64 years were included. Two reviewers independently assessed the methodological quality of the studies. A random-effects meta-analysis was performed, with heterogeneity and publication bias evaluated.
Results:
From 13,899 reports, 71 reports from 39 longitudinal studies (N=7,309,799 participants) were included. The meta-analysis found that older workers, women, those with 12 years or less education, and workers in intermediate or low occupational class are at increased risk of all-cause disability retirement. Other high-risk groups include past (hazard ratio (HR) 1.08, 95% confidence interval (CI) 1.01–1.15) and current (HR 1.29, 95% CI 1.17–1.41) smokers, individuals who are underweight (HR 1.49, 95% CI 1.00–2.23) or obese (HR 1.54, 95% CI 1.31–1.81), individuals lacking physical activity (HR 1.46, 95% CI 1.04–2.06), and those who consume excessive amounts of alcoholic drinks (HR 1.43, 95% CI 1.18–1.73). Additionally, high workload (HR 1.38, 95% CI 1.23–1.56) and low job control (HR 1.47, 95% CI 1.32–1.63) also contribute to the increased risk.
Conclusions:
Introduction
The demographic shift in Europe, characterised by a growing proportion of the aging population and decreasing fertility rates, has led to significant changes in national retirement schemes and a gradual increase in the retirement age [1 –3]. As a result, the need to extend working life means that mid-career and older employees are increasingly representing the workforce. It is estimated that in Organisation for Economic Co-operation and Development (OECD) countries, one in six employees will be over the age of 65 years by 2050 [1,2]. Simultaneously, a considerable number of workers retire early, driven by factors such as health problems, poor work conditions, the availability of early retirement schemes, and economic conditions [4 –6].
Earlier meta-analyses of workers aged 18 years and above have demonstrated that several factors significantly increase the risk of all-cause disability retirement [7 –11]. These factors include past and current smoking, being underweight, overweight, or obese, as well as having suboptimal self-rated general health [7 –9]. Additionally, mental health conditions, and physical conditions such as chronic disease, musculoskeletal disorders and respiratory diseases also contribute to this increased risk [10,11]. In addition to lifestyle risk factors and health conditions, occupational risk factors play a crucial role in the likelihood of disability retirement. A meta-analytical review of workers aged 18 years and above identified a significant association between low job control and all-cause disability retirement. However, this review did not find a significant increase in risk among workers exposed to high job demands, job strain, low social support and shift work [12].
Despite extensive research on lifestyle factors, occupational risk factors, and health conditions, there remains a gap in understanding how sociodemographic factors contribute to disability retirement. To date, no meta-analysis has been conducted to explore the impact of sociodemographic factors such as age, gender, marital status, education level, occupational class, income, and immigration status on the risk of disability retirement. Addressing this gap could provide a more comprehensive understanding of the multifaceted nature of disability retirement and inform targeted interventions to support at-risk populations.
Although several risk factors contributing to disability retirement among workers aged 18 years and older have been identified, the specific causes of disability retirement among middle-aged and older workers are not well known. The aim of this study was to conduct a systematic review of the literature exploring the associations of sociodemographic factors, lifestyle habits, and occupational factors with the incidence of disability retirement in individuals of middle age. Furthermore, the study aimed to estimate the magnitudes of these associations through meta-analysis.
Methods
Search strategy
Our review protocol and meta-analysis were guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [13]. We conducted a comprehensive search of PubMed, Web of Science, PsychInfo, and Scopus databases from their inception until February 2025, using a mix of MeSH terms and text words as published in our earlier reports (Supplemental Table I) [6,14]. Using the PI(E)COTS framework [15], we focused on the ‘P’ (population) to narrow our search to middle-aged workers and the ‘O’ (outcome) to develop a comprehensive sensitive search string. We did not incorporate ‘I(E)’ (intervention/exposure), ‘C’ (control/comparison group), or ‘S’ (setting) in our search criteria. We applied a filter for ‘T’ (types of studies) to exclude clinical trials and reviews. We also searched Google Scholar and screened reference lists of seven systematic reviews and meta-analyses on this topic [7 –12,16].
Inclusion and exclusion criteria
This review included longitudinal studies targeting middle-aged employees aged 45 to 64 years. Given that many studies focused on individuals aged 40 years and above, our inclusion criteria were broadened to include workers aged 40 to 64 years. These studies investigated risk factors for early old-age retirement, disability retirement, or unemployment. Results for unemployment and early old-age retirement were published in other reports [6,14]; this report focuses on the effects of sociodemographic factors, lifestyle habits, and occupational factors on disability retirement. One reviewer (RS) screened and extracted the data.
We excluded research involving clinical subjects, individuals solely on sick leave, or already retired. Studies that combined various forms of labour market departures into a single outcome, such as merging disability retirement with sickness absence, conflating disability retirement with unemployment, or combining disability retirement with early old-age retirement were also excluded.
Quality assessment
The methodological quality of the studies was evaluated independently by two reviewers (RS, and EH or JP), employing criteria modified from the Effective Public Health Practice Project tool (Supplemental Table II) [17]. The evaluation focused on five potential biases: selection, performance, detection, attrition, and confounding, as detailed in our earlier reports [6,14]. Any discrepancies between the reviewers were settled through discussion, and when required, a third reviewer was consulted to reach a consensus.
Statistical analysis
Two studies compared the risk of disability retirement for men with that for women [18,19]. To combine these with others comparing women with men, we inverted the men’s hazard ratio (HR) to derive the HR for women and used the standard error of the men’s estimate to calculate the 95% confidence interval (CI). One study [20] reported an estimate for a 5-year increase in age; we divided the natural logarithm of the estimate by 5 to obtain a 1-year estimate. To examine the effect of education on disability retirement, we recalculated the adjusted HRs by comparing workers with 12 or fewer years of education with those with more than 12 years [18 –28]. For occupational class comparisons, we calculated risk ratios for one study [29] and recalculated adjusted HRs for another [27].
One study compared married with unmarried workers [30]. To combine this with others comparing unmarried with married, we inverted the HR for married workers to derive the HR for unmarried and used the standard error of the married estimate to calculate the 95% CI. Another study compared Swedish-born to foreign-born workers [20]. To combine this with others [23,24] comparing foreign-born with Swedish-born, we inverted the estimate for Swedish-born to derive the estimate for foreign-born and used the standard error of the Swedish-born estimate to calculate the 95% CI. Another study compared foreign-born workers with those born in Sweden to Swedish-born or foreign-born parents [24]. We recalculated the HR for this comparison. Another study compared low and moderate job demands with high job demands [31]. We inverted the estimate for low job demands to calculate the HR for high job demands, using the standard error of low job demands estimate to calculate the 95% CI for high job demands. Additionally, we divided the HR for moderate job demands by the HR for low job demands to obtain the HR for moderate job demands.
To compare alcohol abstainers and high alcohol consumers with light alcohol consumers, we recalculated the adjusted HR for one study [32]. Two studies compared low leisure-time physical activity with high physical activity [33,34]; we recalculated their HRs and compared low physical activity with moderate or high physical activity. One study compared moderate and low work ability with excellent work ability [35]; we recalculated the HRs for moderate and low work ability to align with two other studies [36,37] comparing low and moderate work ability with good or excellent work ability.
Some studies used logistic regression to examine risk factors for disability retirement. We converted odds ratios (ORs) and their 95% CIs to risk ratios (RRs) for two studies [38,39] in which more than 5.5% of the participants received disability retirement during follow-up [40]. We used a fixed-effect meta-analysis to integrate subgroups within a single study and a restricted maximum likelihood (REML) random-effects meta-analysis to synthesise findings from various studies. Meta-regression was conducted to explore heterogeneity and identify potential sources of variability in effect sizes across studies. This approach helps to clarify whether study-level characteristics such as sample size and study quality contribute to differences in observed outcome. A funnel plot examined publication bias, and Egger’s regression test assessed funnel plot asymmetry. The trim-and-fill method imputed potentially missing studies due to publication bias. Stata version 18 was used for the meta-analyses.
Results
A total of 12,899 reports were gathered from PubMed, Web of Science, PsychInfo, and Scopus (Figure 1). The first reviewer screened titles and abstracts, including the first 1000 results from Google Scholar, bringing the total to 13,899. Subsequently, 964 full-text articles were thoroughly reviewed to assess relevance, focusing on participant age, which was not reported in the abstracts. Of these, 803 were excluded for not addressing disability retirement, and 90 were excluded for various reasons. Specifically, 40 studies were excluded as they examined the link between sleep problems and health conditions with disability retirement. Ten studies were excluded as they combined disability retirement with sickness absence, two with long-term sickness absence and unemployment, and seven with unemployment and other reasons for not working. Additionally, five studies combined disability retirement with early old-age retirement and old-age retirement, three with early old-age retirement and unemployment, nine with early old-age retirement, and one study with the ‘not in labor force’ route. Furthermore, seven studies focused on early retirement intentions, three were case–control studies, one study measured age at the end of follow-up, and two reports from studies included in the review did not provide confidence intervals for adjusted estimates. The references can be found in the supplemental materials.
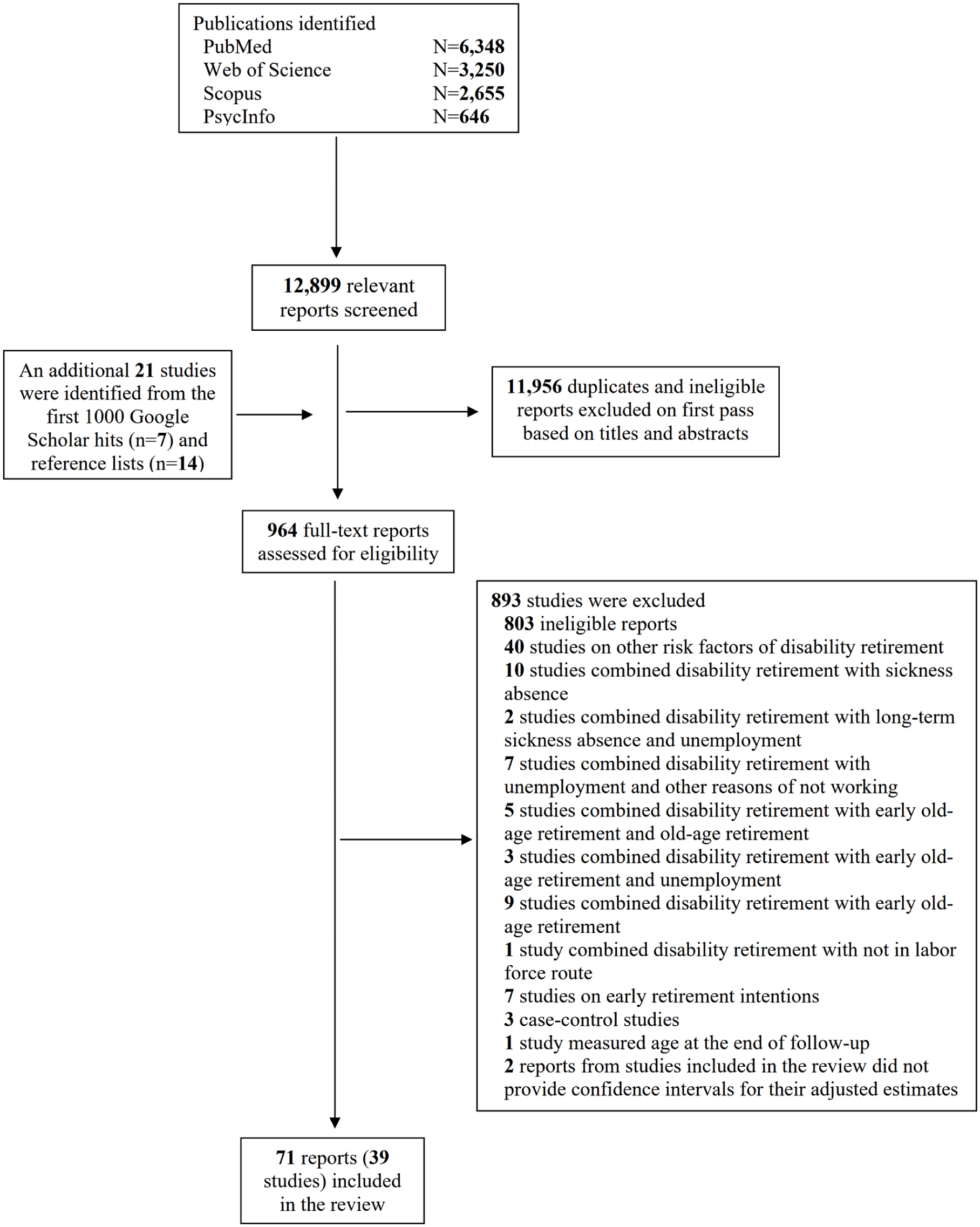
PRISMA flow diagram of the studies selection.
Ultimately, this review included 71 reports from 39 longitudinal studies, encompassing 7,309,799 participants. The number of participants ranged from 850 to 2,281,599 individuals (Supplemental Table III). The 39 studies were distributed as follows: 12 from Sweden (23 reports), five from Finland (17 reports), six from Denmark (nine reports), four from The Netherlands, six from Norway (10 reports), and one each from France, Germany, South Korea (three reports), the United States, and Switzerland. Additionally, one study included participants from 11 different European countries: Austria, Belgium, Denmark, France, Germany, Greece, Italy, Spain, Sweden, Switzerland, and The Netherlands.
Methodological quality of the studies
Sixteen reports were deemed to have a low risk of selection bias, 41 reports were considered to have a moderate risk, and 14 were identified as high risk (Supplemental Figure 1). For performance bias, 12 reports were rated as low risk, and 59 reports were considered moderate risk (Supplemental Figures 1 and 2). In terms of detection bias, 59 studies were assessed as having a low risk, and 12 as moderate risk. Regarding confounding, 14 reports were evaluated as low risk of bias, having accounted for the most confounding factors. Forty-seven reports were rated as having a moderate risk of bias, as they only adjusted for some confounders in their observed associations. Additionally, 10 reports were considered to have a high risk of bias. Concerning attrition bias, 49 reports were rated as low risk, 21 moderate risk, and one report was considered to have a high risk.
Risk factors for all-cause disability retirement
Sociodemographic factors
Older workers face a higher risk of all-cause disability retirement, with each additional year of age increasing the risk (HR 1.07, 95% CI 1.03–1.12, Table I and Supplemental Figure 3). Women are also at a higher risk compared with men (HR 1.28, 95% CI 1.01–1.62, Supplemental Figure 4). Unmarried, separated, or widowed workers (HR 1.13, 95% CI 1.02–1.24, Supplemental Figure 5), workers with 12 years or less of education (HR 1.37, 95% CI 1.16–1.62, Supplemental Figure 6), and those in intermediate (HR 1.43, 95% CI 1.18–1.74, Supplemental Figure 7) or low (HR 2.06, 95% CI 1.59–2.66, Supplemental Figure 7) occupational classes are at elevated risk. Immigrants are not at increased risk (HR 1.27, 95% CI 0.87–1.87, Supplemental Figure 8).
Risk factors of all-cause disability retirement.
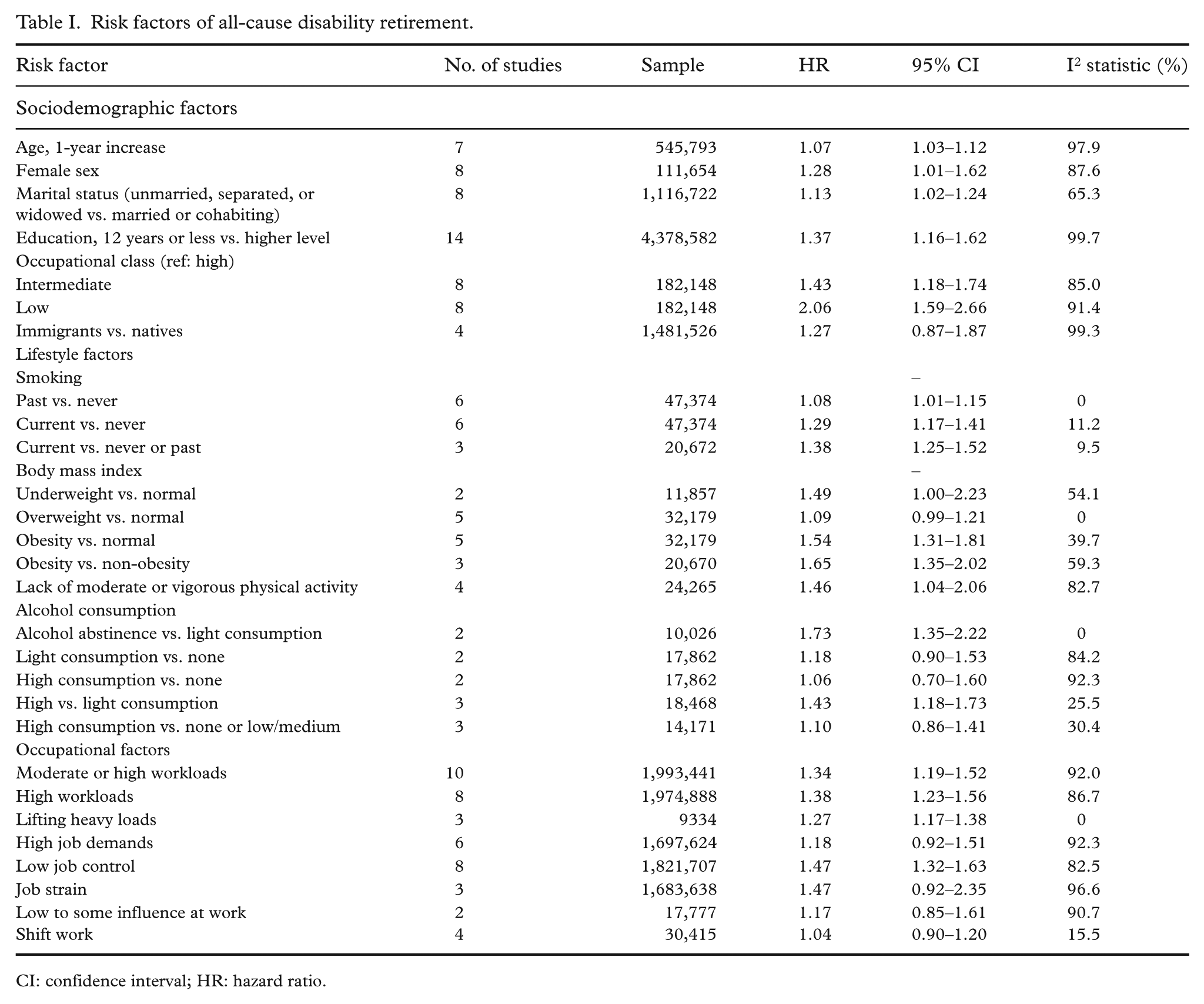
CI: confidence interval; HR: hazard ratio.
Lifestyle factors
Current smokers are at an increased risk (HR 1.29, 95% CI 1.17–1.41, Supplemental Figure 9), as are underweight (HR 1.49, 95% CI 1.00–2.23, Supplemental Figure 10) and obese (HR 1.54, 95% CI 1.31–1.81, Supplemental Figure 10 and 11) workers. Past smokers also face a slightly higher risk (HR 1.08, 95% CI 1.01–1.15, Supplemental Figure 9), but overweight workers do not (Supplemental Figure 10). Workers who lack moderate or vigorous physical activity are at increased risk (HR 1.46, 95% CI 1.04–2.06, Supplemental Figure 14). Both alcohol abstainers (HR 1.73, 95% CI 1.35–2.22) and excessive alcohol consumers (HR 1.43, 95% CI 1.18–1.73) have higher risks compared with light alcohol consumers (Supplemental Figure 15).
Occupational factors
Workers exposed to moderate or high workloads (HR 1.34, 95% CI 1.19–1.52, Supplemental Figure 16), high workloads (HR 1.38, 95% CI 1.23–1.56, Supplemental Figure 17), heavy lifting (HR 1.27, 95% CI 1.17–1.38, Supplemental Figure 18), and low job control (HR 1.47, 95% CI 1.32–1.63, Supplemental Figure 19) are at an increased risk of all-cause disability retirement. However, workers exposed to high job demands (Supplemental Figure 20), job strain (Supplemental Figure 21), low to some influence at work (Supplemental Figure 22), or those working shifts (Supplemental Figure 23) do not appear to have an increased risk.
Risk factors for cause-specific disability retirement
A limited number of studies have examined the risk factors for cause-specific disability retirement (Table II). The findings indicate several factors associated with an increased risk of disability retirement due to musculoskeletal disorders, including obesity (HR 1.65, 95% CI 1.30–2.08, Supplemental Figure 12), moderate or high workload (HR 1.91, 95% CI 1.44–2.55, Supplemental Figure 16), and low job control (HR 1.36, 95% CI 1.21–1.51, Supplemental Figure 19). Conversely, being overweight (Supplemental Figure 12), lacking moderate or vigorous leisure-time physical activity (Supplemental Figure 14), and experiencing high job demands (Supplemental Figure 20) did not increase the risk.
Risk factors of disability retirement due to musculoskeletal and mental disorders.
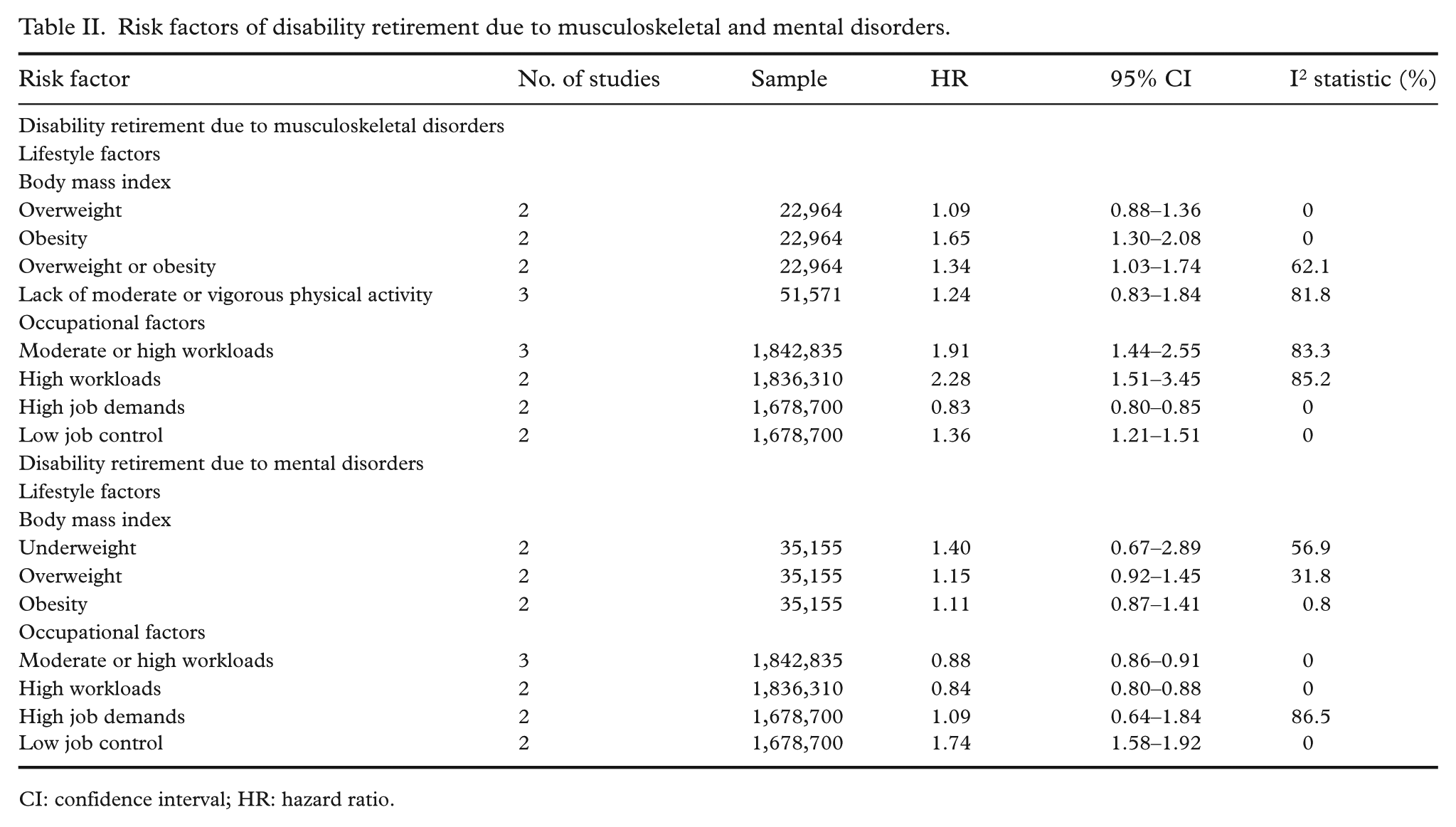
CI: confidence interval; HR: hazard ratio.
For disability retirement due to mental disorders, the associated risk factors include low job control (HR 1.74, 95% CI 1.58–1.92, Supplemental Figure 19). In contrast, moderate to high workload (Supplemental Figures 16 and 17) was associated with a lower risk of disability retirement. Additionally, body mass index (Supplemental Figure 13) and high job demands (Supplemental Figure 20) were not significant risk factors.
Moderate to high workload was also associated with disability retirement due to cardiovascular disease (HR 1.22, 95% CI 1.15–1.28, Supplemental Figure 16).
Assessment of heterogeneity
Meta-regression analysis showed that differences in effect sizes for age, sex, and education were independent of sample sizes and study quality. Confounding factors influenced the effect of occupational class on all-cause disability retirement. For intermediate occupational class, the pooled HR was 1.21 (95% CI 0.96–1.53) in low-risk confounding studies and 1.73 (95% CI 1.46–2.06) in moderate/high-risk studies. For low occupational class, the pooled HR was 1.68 (95% CI 1.18–2.38) in low-risk confounding studies and 2.64 (95% CI 2.38–2.92) in moderate/high-risk studies. Additionally, the pooled HR for low occupational class was 2.56 (95% CI 2.43–2.70) in low attrition bias studies and 1.60 (95% CI 0.97–2.64) in moderate attrition bias studies.
Heterogeneity was largely explained for the effect of high physical workloads on all-cause disability. The pooled HR was 1.24 (95% CI 1.10–1.39, I²=0%) in four studies with low confounding risk, 1.34 (95% CI 1.12–1.61, I²=30.6%) in two studies with moderate risk, and 1.62 (95% CI 1.42–1.84, I²=25.6%) in two studies with high risk. For moderate or high physical workloads, selection bias and confounding influenced the effect size. The pooled HR was 1.28 (95% CI 1.05–1.57) in four studies with low selection bias and 1.41 (95% CI 1.21–1.66) in six studies with moderate bias. The pooled HR was 1.24 (95% CI 1.05–1.45) in five studies with low confounding risk and 1.45 (95% CI 1.24–1.69) in five studies with moderate/high risk. Heterogeneity in effect sizes for low job control was explained by confounder adjustment and sample sizes. The pooled HR was 1.44 (95% CI 1.36–1.53, I²=10.4%) after excluding two studies with unadjusted estimates. It was 1.33 (95% CI 1.16–1.52, I²=0%) in three smaller studies and 1.47 (95% CI 1.40–1.54, I²=3.4%) in three larger studies.
Assessment of publication bias
No publication bias was found for age, sex, education, physical workloads, and job control with all-cause disability retirement. The trim-and-fill method did not impute any missing studies, except for low job control, in which one significant study was added. However, publication bias was evident for marital status, low occupational class, and smoking. For marital status, three missing studies were imputed (Supplemental Figure 24), and the excess risk disappeared after adjustment for publication bias (HR 1.07, 95% CI 0.97–1.18). For low occupational class, the P value for Egger’s test was 0.035, and the trim-and-fill method imputed one missing study (Supplemental Figure 25). The pooled HR reduced from 2.06 (95% CI 1.59–2.66) to 1.93 (95% CI 1.48–2.51). No bias was found for intermediate occupational class. A funnel plot of nine studies on the link between smoking and all-cause disability retirement was asymmetrical, but Egger’s test was non-significant (P=0.12). The trim-and-fill method imputed two missing studies (Supplemental Figure 26), reducing the pooled HR from 1.33 to 1.31.
Discussion
This study identified various modifiable and non-modifiable risk factors for disability retirement among middle-aged individuals. Key non-modifiable sociodemographic factors include age, sex, education, occupational class, and immigrant status, highlighting vulnerabilities in certain demographic groups. Modifiable lifestyle and occupational risk factors include smoking, physical inactivity, underweight, excess body mass, excessive alcohol consumption, high workloads, low job control, and impaired work ability. Addressing these modifiable factors through proactive interventions can reduce disability retirement risks and promote longer, healthier working lives.
Women are more likely than men to receive disability retirement [30,41]. One study found that self-rated general health, mental distress, occupation, working conditions, and income fully explain this gender difference [41]. However, another study found that while self-rated physical and mental health account for some of the disparity, family factors, occupational class and weekly working hours do not [30]. For highly educated individuals, the gender disparity is fully explained by self-rated physical and mental health, family factors, occupational class and weekly working hours, but for those with medium or low education, the gender gap remains unexplained [30].
The connection between education, occupational class, and disability retirement is partly mediated by occupational risks and health conditions. Workers with lower education levels are more likely to face occupational risks [42] and chronic illnesses [43], increasing their likelihood of disability benefits. Alcohol-related conditions explained 4% to 10% of the link between education level and disability retirement, while common mental disorders accounted for only 0% to 4% of the association [44]. The link between occupational class and all-cause disability retirement is partly due to low job control and physically demanding work, especially among manual workers [45]. The relationship between education and all-cause disability retirement is mediated by 8–20% due to high physical workload and by 11–18% due to low job control [42].
Our study identified several lifestyle risk factors – such as smoking, underweight, obesity, excessive alcohol consumption, and physical inactivity – that significantly increase the risk of disability retirement. Interestingly, alcohol abstainers also have an elevated risk, likely because individuals with health conditions often abstain from alcohol years before applying for disability retirement. To mitigate these risks, programmes promoting smoking cessation, weight management, reduced alcohol consumption, and regular physical activity can be highly effective. These initiatives not only improve overall health but also support longer, healthier working lives. For instance, previous randomised controlled trials have demonstrated the effectiveness of physical activity [46,47], and self-management programmes [48] in enhancing the work ability of older workers. Impaired work ability is a significant risk factor for disability retirement [36]. Therefore, developing and implementing workplace interventions is crucial for prolonging work life participation. Additionally, there is moderate evidence that active workplace health promotion for older workers can reduce waist circumference, body mass index and other components of the metabolic syndrome [49].
This review shows that high physical workloads and low job control significantly increase the risk of disability retirement. This aligns with previous studies indicating that a supportive psychosocial work environment can extend employment beyond retirement age, while physically demanding jobs tend to reduce it [50,51]. Improving the physical working environment and enhancing job control can help mitigate these risks and support longer working lives. However, evidence on the favourable effects of high job control is inconsistent. One study found that two components of job control – decision authority and skill discretion – show inconsistent associations with early retirement and opposite associations with mortality [52]. High skill discretion was linked to a lower risk of early retirement, while decision authority showed no association [52]. For mortality, high skill discretion was associated with a lower risk, whereas high decision authority was linked to a higher risk [52]. Another study found that high skill discretion and high decision authority were associated with a lower risk of all-cause mortality among white-collar women [53], but high decision authority increased mortality risk among blue-collar women [53]. No associations were found among men [53]. To address these complexities, tailored interventions considering the specific needs of different occupational groups are essential. Enhancing decision making autonomy and providing opportunities for skill development can benefit workers in high-stress environments. Conversely, reducing physical strain and improving ergonomic conditions are critical for those in physically demanding jobs. Overall, a balanced approach that improves both the physical and psychosocial aspects of the work environment can support longer, healthier working lives. By addressing the diverse needs of the workforce, more effective strategies can be developed to reduce the risk of disability retirement and promote sustained employment.
Limitations
Numerous studies have identified various risk factors for disability retirement. However, in each report, the authors have adjusted the observed associations for only a limited number of confounding factors, potentially leading to an overestimation of these associations. They did not control for the majority of risk factors that their study identified. The correlations between the identified risk factors were not high enough to justify excluding many risk factors from multivariable models, resulting in significant residual confounding. Additionally, some of these studies have employed logistic regression to identify risk factors for time-to-event data related to disability retirement, despite logistic regression’s inability to account for the timing of events [54]. This methodological choice can lead to inaccurate conclusions about the risk factors. Furthermore, many studies have conducted stratified analyses to explore interactions between risk factors. Most of these studies found only additive effects. However, the authors did not report the estimates for main effects in the absence of joint effects for each risk factor, which are necessary for meta-analysis. To address these issues, future research should aim to control for a comprehensive set of confounding factors to provide more accurate estimates of the associations between risk factors and disability retirement. Additionally, employing appropriate statistical methods, such as Cox proportional hazards models, which account for the timing of events, would yield more reliable results. Reporting results both in the absence and presence of joint effects would also enhance the understanding of how different risk factors interact to influence disability retirement.
Conclusions
This comprehensive meta-analysis highlights various modifiable and non-modifiable risk factors that significantly increase the risk of disability retirement among middle-aged individuals. To prolong the working careers of aging workers, targeted interventions and programmes are essential. These should focus on fostering a supportive work environment by managing high workloads and enhancing job control, and promoting healthy lifestyle choices, including regular physical activity, balanced nutrition, smoking cessation, and responsible alcohol consumption. Addressing these modifiable risk factors can reduce the incidence of disability retirement, benefitting individual workers and contributing to overall workforce productivity and economic stability.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948251398695 – Supplemental material for A meta-analysis of risk factors for disability retirement in middle-aged workers
Supplemental material, sj-pdf-1-sjp-10.1177_14034948251398695 for A meta-analysis of risk factors for disability retirement in middle-aged workers by Rahman Shiri, Eija Haukka, Mikko Härmä and Joonas Poutanen in Scandinavian Journal of Public Health
Footnotes
Author contributions
Conceptualisation, RS, MH, EH, and JP; funding acquisition, RS, MH, EH, and JP; screening and data extraction, R.S.; quality assessment, RS, JP, and EH; analysis and interpretation of results, R.S.; writing – original draft preparation, RS; writing – review and editing, RS, MH, EH, and JP; project administration, RS; and guarantor, RS. All authors have read and approved the final version of the manuscript.
Availability of data and material
The data are included in the supplemental file.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Finnish Work Environment Fund (grant no. 230363).
Ethics approval
Ethics approval is not required for conducting a systematic review that includes only aggregated data from previously published studies.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.