
Abstract
Aims: Increasing self-reported mental health problems among adolescents in many countries, accompanied by worsening results in international studies of school achievement, raises questions about how school, learning and mental health interact. The purpose of the present study is to analyse the associations between mental health, early school achievement and subsequent school failure in the final year of compulsory schooling in Sweden. Methods: This study is based on a Swedish representative sample of 9020 children born in 2004, which was drawn in 2014 by Statistics Sweden. Three logistic regression models were analysed: regressing school failure in school year 9 on psychiatric diagnoses, grades in school year 6 and sociodemographic variables. Results: Psychiatric diagnoses and grades in school year 6 are strongly associated with school failure in school year 9. These two variables interact, and their combined effects on school failure is striking. Almost every second student with a psychiatric diagnosis and not achieving passing grades in all subjects in school year 6 fails in school year 9. The corresponding figure is 2% for students with no psychiatric diagnosis and passing grades in all subjects in school year 6.
Keywords
Background
A rising trend of self-reported mental health problems among adolescents in Sweden [1] is accompanied by worsening results in international studies of school achievement [2] and a moderate increase of the number of students who are not eligible for admission to upper secondary school. These parallel trends are monitored by surveys and administrative registers that do not permit causal explanations. Typically, there is a scarcity of single adolescent trend studies that bridge the gap between health and educational data analyses [3].
Failure to meet the criteria for admission to upper secondary school in Sweden after finishing the compulsory school (~15–16-year-old students) is captured by the concept of school failure. The concept has its roots far back in time [4], and its definition might vary across countries because of different school systems. Broadly, the concept can be defined as a discrepancy between a student’s behaviour and achievements, and the expectations of the school and other environments (e.g. parental) [5]. School dropout is a similar concept, which in a US context mainly refers to failure to complete high school [6]. School failure and school dropout do not only have negative impacts on the student’s educational career in the short-term, but are also likely to have negative long-term social and economic consequences [6,7]. This conclusion is supported by analyses of long-term psychosocial outcomes for 10 Swedish population cohorts born 1972–1981, which showed that school failure dramatically increased the risk for future psychosocial problems, drug use and criminality [8]. Negative impacts on later psychosocial problems of poor school performance were also found in a longitudinal register study among foster children in Sweden [9].
A number of proximal and distal factors at different levels are associated with school failure, but it has proven difficult to demonstrate causality [6]. Previous research has identified socioeconomic factors as major determinants of school outcomes, in addition to cognitive and non-cognitive ability [6,10] According to a UK study, cognitive ability and conscientiousness are stronger determinants of educational attainment than socioeconomic status [11]. Deficiencies in early academic achievement and engagement have also been shown to predict subsequent school failure [6].
Strong associations between mental health and school performance are reported in studies based on European and US data [10,12]. A systematic literature review on mental health and school performance conducted in 2010 detected several longitudinal international studies with high relevance and high quality [13]. None of these studies was Swedish, and since then only a few Swedish longitudinal population studies on this topic have been published. A recent Swedish study with data solely retrieved from health and educational registers demonstrated significant associations between psychiatric diagnoses and school grades and eligibility for upper secondary school [14]. Most of the diagnoses, in particular attention deficit hyperactivity disorder (ADHD), showed negative associations with educational achievements. Another study, based on self-reported mental health data and parental reports, found that mental health problems at ages 3 and 12 years were risk factors for poor academic achievement [15]. Similarly, a Danish register study showed that children with a mental disorder were significantly less likely than those without a mental disorder to pass the final examination at the end of compulsory school [16].
The association between school achievement and mental health is commonly described as bi-directional [17]. Weak school achievement might cause mental health problems in their own right, but mental illness might also cause school failure, which in turn might aggravate the mental health problems [13]. A systematic literature review indicates that externalising disorders have a stronger direct effect on early school dropout than internalising disorders, while highlighting increasing risks of internalising disorders in the wake of school dropouts [18].
Efforts have been made in different disciplines to examine and explain the associations between children’s mental health and future academic performance and success in life [19].
In order to deepen and qualify the understanding of the complex associations between mental health and school failure, there are empirical challenges to address including analyses of moderation, mediation and changes over time. The current paper responds primarily to the first of these challenges by considering potential interaction effects between mental health and other predictive factors in the analyses of school failure. Only a limited number of studies have examined potential non-uniformity of the association between mental health and school failure, for example, whether, and to what extent, the associations are moderated by sociodemographic or other key variables [20 –22].
A related issue that also concerns the strength of the association between mental health and school performance is whether, and to what extent, the association is stable or varies over time. A recent Norwegian study shows that the association between mental disorders and school performance has weakened over time, contrasting outcomes from studies conducted in the UK [3]. Another issue concerns the pathways from mental health problems to academic achievement, which have been suggested to operate through different mediators, representing different pathways: academic aptitude, school related disruptive behaviours, and educational expectations [19]. These different pathways relate to the distinction between cognitive and non-cognitive explanatory factors. Increasing attention is also paid to broader school expectations, which comprise potential risk and protective factors.
The present study addresses the complex associations between mental health and school performance by providing a lagged variable that measures school performance in school year 6 (~12–13-year-old students) in the analysis of mental health and school failure in year 9, the final year of compulsory schooling in Sweden (~15–16-year-old students). Upper secondary schooling in Sweden is optional and admission to the national programmes requires passing grades in the core subjects English, Swedish and mathematics, and some additional subjects [23].
Aims
The increase of self-reported mental health problems among adolescents in many countries, accompanied by reports in international studies of declining results in school achievement, raises questions about how school, learning and mental health interact.
Although poor early school achievement is known as a risk factor for subsequent school failure, studies on associations between mental health and school performance have rarely taken early school achievement into account. Combined and potential interactive effects of psychiatric diagnoses and early school achievement need to be examined analytically in order to disentangle potential risk factor patterns for later school failure in school year 9. Omitting such information might hamper our understanding of complex interrelationships between mental health and school achievement.
The purpose of the present study is therefore to analyse the associations between mental health, early school achievement and subsequent school failure in the final year of compulsory schooling in Sweden, with a special focus on combined and interactive effects on school failure of psychiatric diagnoses and grades in school year 6.
Methods
Sample
This study is based on a Swedish nationally representative sample of children, which was drawn in 2014 by Statistics Sweden when students were in school year 3. A two-stage sampling procedure was applied, drawing a stratified sample of schools from among which classes were then selected. The overwhelming majority of the students were born in 2004 (9437 of 9775; 96.5%). In the analyses reported in the present paper only students born in 2004 who 2020 finished the final year of compulsory schooling (n=9012) are included.
The 2004 birth cohort is one of 11 cohorts sampled for the purpose of the Evaluation Through Follow-up (ETF) study, including survey and test data in addition to register data. ETF is hosted by the Department of Education and Special Education at the University of Gothenburg. Only national register data are used in the current study, which is part of a project approved by the Swedish Ethical Review Authority (decision 2020-12-18, dnr 2020-04933).
Data
Data on psychiatric diagnoses were retrieved from the Swedish Patient Register, which contained data on diseases and treatments by doctors in specialised care in Sweden but not data from primary care. Among the students, 1513 were registered for any kind of psychiatric diagnosis at least once from 2004 to May 2020, that is, before the completion of the compulsory school in June 2020. Of these students, 1074 (71%) had their last registration for a diagnosis at special care at age 14–16 years.
The Patient Register is maintained by the Swedish National Board of Health and Welfare. Sociodemographic and educational data were retrieved from registers managed by Statistics Sweden.
The outcome measure of school failure
School failure is operationalised as not achieving passing grades in all of the three core subjects in school year 9, that is, English, mathematics and Swedish. Until a new curriculum was implemented in 2011, passing grades in these three subjects were the eligibility criteria for subsequent admission to upper secondary school. In addition to these three core subjects, the new curriculum requires pass grades in other subjects, specific to vocational and upper secondary programmes preparing for higher education. For the purpose of this study, we are defining school failure as not achieving pass grades in English, mathematics and Swedish in school year 9.
Definition of predictor variables
Psychiatric diagnoses
The psychiatric diagnoses included in the study are classified according to the International Classification of Diseases (ICD) version 10. All ICD variables are binary, coded yes/no and concern a main diagnosis at least once during 2004 to May 2020. The ICD codes for main diagnosis are specified in parentheses in the following. Any psychiatric diagnosis (F1–F9); depression (F32–F39); anxiety (F40–F48); neuropsychiatric diagnoses (F84 = pervasive developmental disorders) and (F90 = Attention-Deficit Hyperactivity Disorders). Other psychiatric diagnoses all diagnoses (F1–F9), excluding depression (F32–F39), anxiety (F40–F48) and neuropsychiatric diagnoses (F84, F90).
Across all ages (0–16 years) until December 2020, 89% of the students visiting specialised care had a registered psychiatric diagnosis (F1–F9). Among students aged 14–16 years, the corresponding figure was 96%.
School achievement school year 6
Swedish students who are enrolled in school year 6 study 16 subjects in total and are expected to complete (i.e. ‘pass’) all of these subjects. Year 6 students were classified into one of two groups: the first group was those students who successfully passed all 16 year 6 subjects (complete grades). The second group was those students who failed one or more of the 16 year 6 subjects (incomplete grades).
Sociodemographic variables
Student sex: male, female.
Parental education (the parent with the highest education): lower: no upper secondary school education or upper secondary school education from a vocational program; mid: education from a theoretical programme at upper secondary school or higher education less than two years; higher: two or more years of higher education.
National background: Swedish (child and at least one of the parents born in Sweden, or child born outside of Sweden and both parents born in Sweden.); foreign (child born in Sweden and both parents born outside of Sweden, or child and at least one parent born outside of Sweden).
Analysis
Three logistic regression models were analysed with school failure (defined above) as a common outcome variable. All three models included predictor variables on psychiatric diagnoses and grades in school year 6, as well as sociodemographic variables.
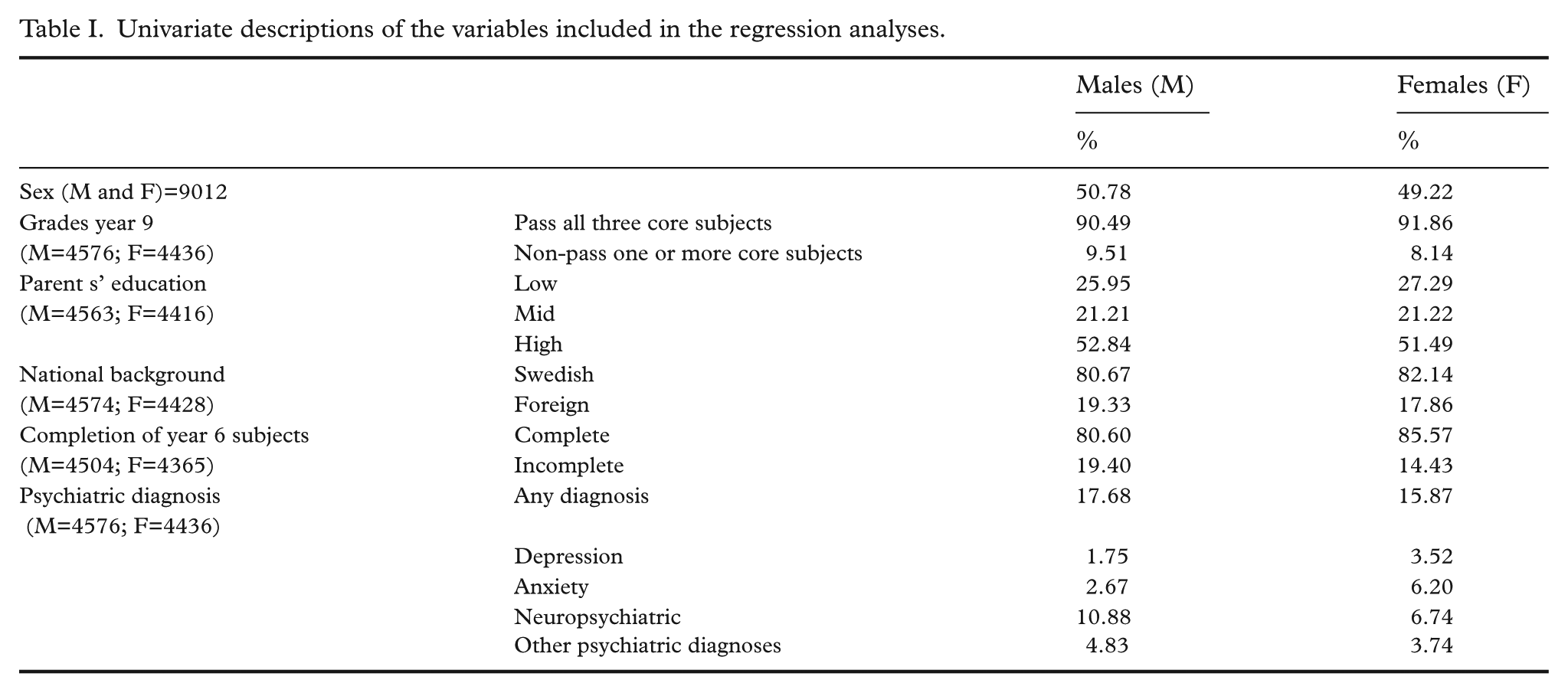
Crude descriptive statistics were calculated for all included variables and distributed by sex (Table I).
Univariate descriptions of the variables included in the regression analyses.
The regression models differed with respect to the measure of psychiatric diagnoses (overall or specific) and parametrisation of the variables (main/interaction effects). Models I and II only included main effects terms, that is, no interaction terms. In Model I a predictor variable containing all psychiatric ICD F-diagnoses (‘Any psychiatric diagnosis’) was included (Table II). In Model II (Table III) specific diagnoses were analysed: variables on depression, anxiety, neuropsychiatric diagnoses and ‘other diagnoses’ were entered simultaneously, in order to control for potential comorbidity between the individual psychiatric diagnoses. By inclusion of both main effect terms and interaction terms, Model III reflected the special focus of the study on the combined and interactive effects of psychiatric diagnoses and grades in school year 6. Because the LR-test (likelihood-ratio test) (see below) showed that grades in school year 6 also interacted with parental education, an additional interaction term was included in the model that was subjective to the analysis. In Model III the variable on ‘Any psychiatric diagnosis’) was used as a measure of psychiatric diagnoses (Table IV).
Odds ratios estimated in binary logistic regression analysis. School failure in school year 9 regressed on any psychiatric diagnosis, completion of subjects in year 6, sex, parents’ education and national background (N=8837). p-values and confidence intervals calculated based on robust standard errors.
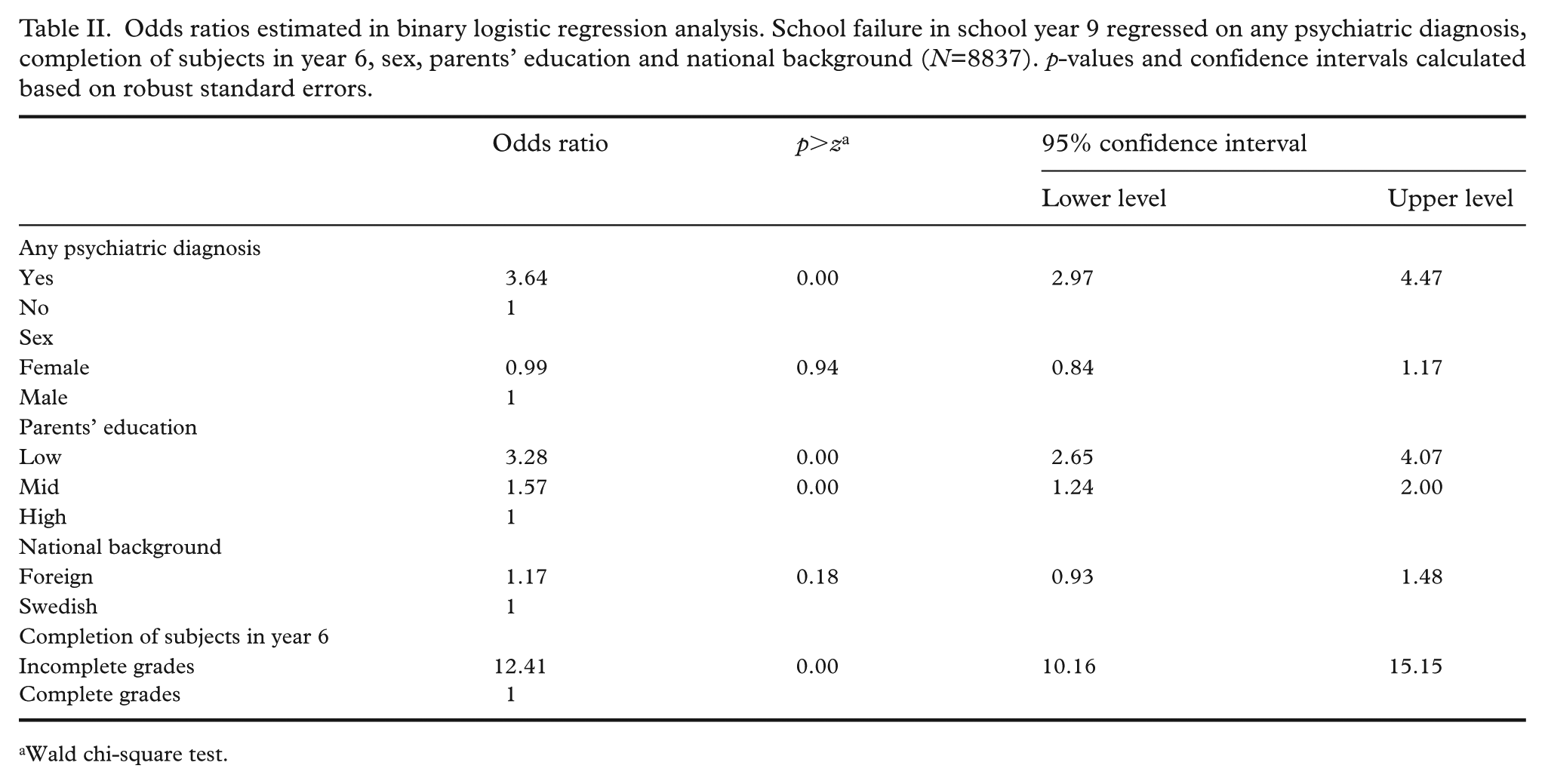
Wald chi-square test.
Odds ratios estimated in binary logistic regression analysis. School failure in school year 9 regressed on depression, anxiety, neuropsychiatric diagnoses, ‘other diagnoses’, completion of subjects in year 6, sex, parents’ education and national background (N=8837). p-values and confidence intervals calculated based on robust standard errors.
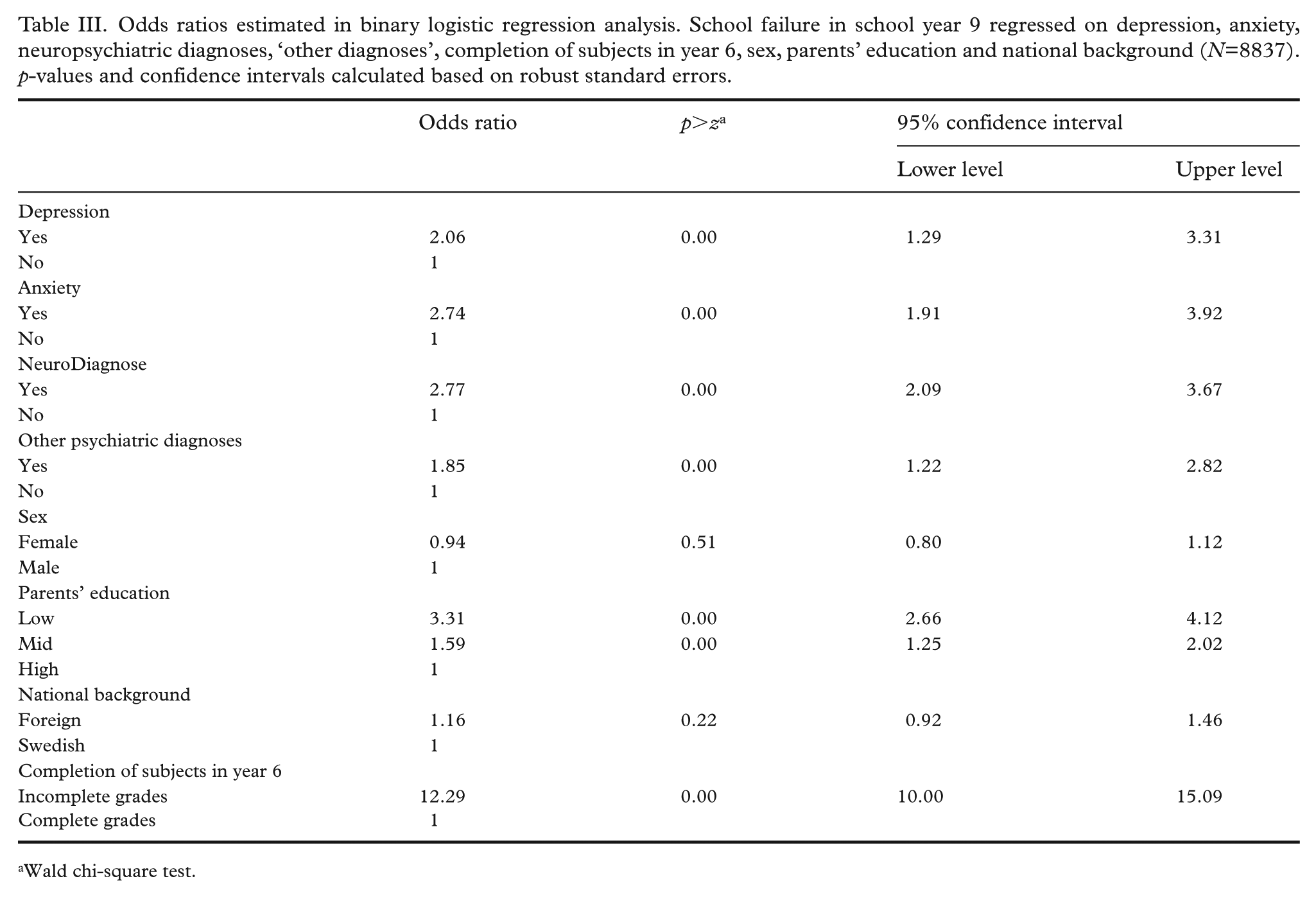
Wald chi-square test.
Log odds estimated in binary logistic regression analysis. School failure in school year 9 regressed on any psychiatric diagnoses, completion of subjects in year 6, sex, parents’ education and national background (N=8837). p-values and confidence intervals calculated based on robust standard errors.
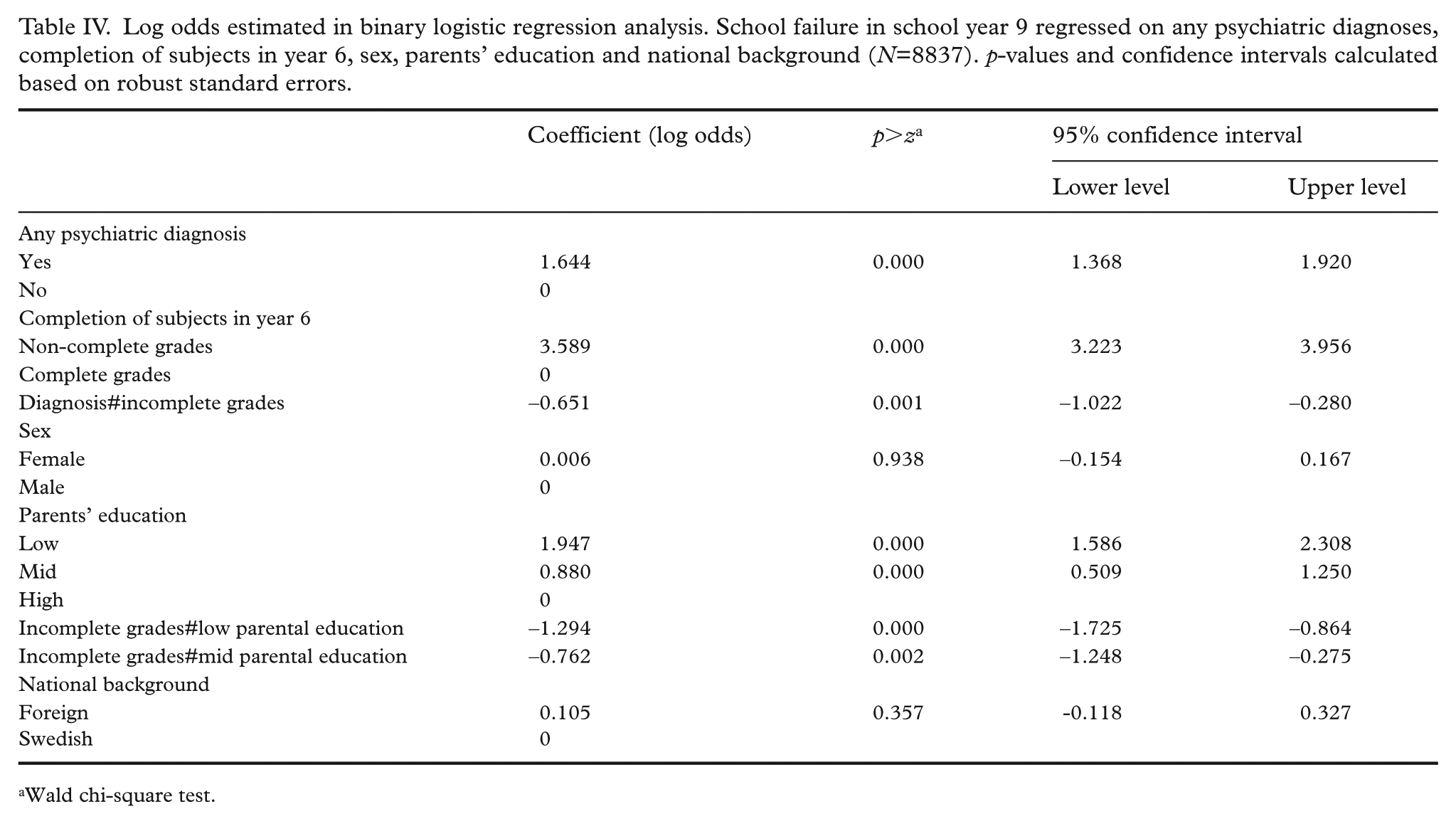
Wald chi-square test.
Robust standard errors were calculated, in order to take account of potential effects of school clustering when the sample was drawn. Tests for potential multicollinearity among the predictor variables were also applied. Values of around 1 or less for the Variance Inflating Factor were taken as evidence of absence of multicollinearity.
Potential statistical interactions between the variables ‘Any psychiatric diagnosis’ and ‘Grades in school year 6’, as well as the sociodemographic variables, were analysed with LR-tests, comparing the relative fit of the model including five main effect terms with models also including interaction terms. Sex did not show any interaction with the psychiatric variable. ‘Grades in school year 6’ was the only variable that showed interactions with the psychiatric variable. Based on these outcomes and to facilitate the analyses, a four-cell typology was constructed that captured combined and interactive effects of the variables ‘Any psychiatric diagnosis’ and ‘Grades in school year 6’. The log odds values for each of the four combinations of these two variables were estimated in Model III, controlling for the sociodemographic variables. As mentioned above, because ‘Grades in school year 6’ did also interact with parental education, an interaction term that captured this interaction was also included in the regression analysis, implying that Model III included two two-way interactions (Table IV). The log odds values pertaining to the four-cell typology were then converted through exponentiation into predictive probabilities, which were reported as predictive percentages (Table V).
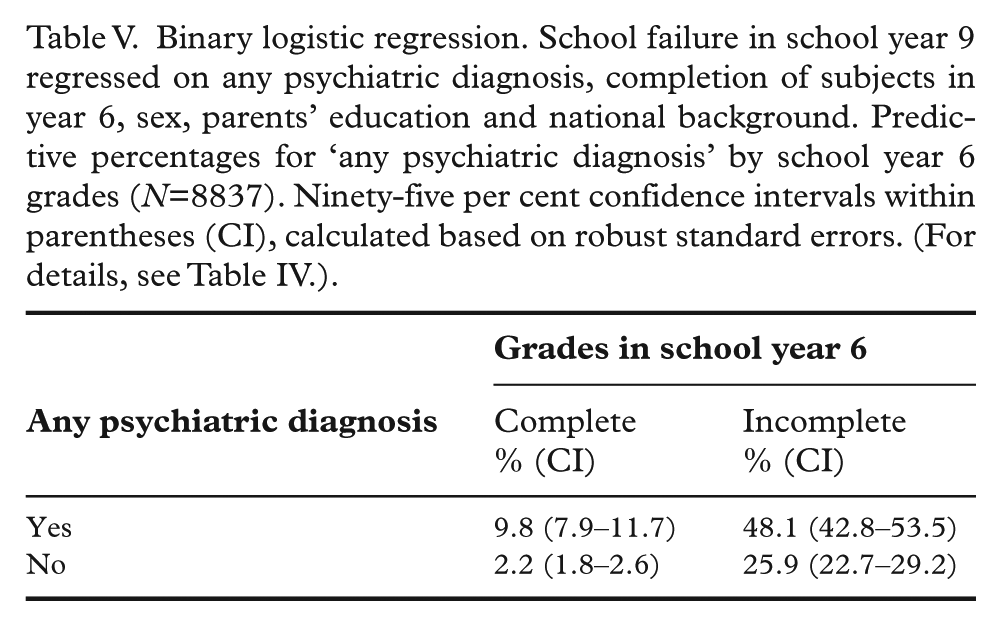
Binary logistic regression. School failure in school year 9 regressed on any psychiatric diagnosis, completion of subjects in year 6, sex, parents’ education and national background. Predictive percentages for ‘any psychiatric diagnosis’ by school year 6 grades (N=8837). Ninety-five per cent confidence intervals within parentheses (CI), calculated based on robust standard errors. (For details, see Table IV.).
Because data on the time point for the diagnoses were not available, variables on the age for the first and the last visit at specialised care respectively were used in a tentative regression analysis in order to capture a time (age) perspective (results not reported in a table).
Another tentative analysis examined the impacts of excluding the variable on grades in school year 6 from the regression analysis (results not reported in a table).
Statistical analyses were conducted with the STATA 18.0 software available in Statistic Sweden’s micro data portal [24].
Results
The proportion of students with incomplete grades was higher for boys than for girls, in both school years 9 and 6 (Table I). The sex differences were relatively small for the variables parental education and nationality. The proportion of students who had ever had any psychiatric diagnosis was slightly higher for boys than for girls. The proportions of depression and anxiety diagnoses were higher for girls than for boys while the opposite applied for neuropsychiatric diagnoses. More than half of the children had parents with higher education.
The logistic regression reported in Table II showed significant associations with school failure for ‘Any psychiatric diagnosis’. The odds for year 9 school failure was more than three times higher for students with any psychiatric diagnosis than for those without a diagnosis. Among the three sociodemographic variables, only parental education showed significant odds ratios: students with lower educated parents showed three times higher odds for year 9 school failure compared with students with higher educated parents. The odds ratio for grades in school year 6 was very high: students with incomplete grades in year 6 had 12 times higher odds for failure in school year 9 compared with students with complete grades in year 6. A tentative regression analysis focusing on students with their first and last visit to special care at age 14–16 years showed that this group (only including those with a psychiatric diagnosis) was 2.9 times more likely to fail in school year 9 compared with the group with no psychiatric diagnosis. The corresponding figure when comparing all students with and without any psychiatric diagnosis (i.e. not taking age into account) was 2.4. There were also significant associations with school failure for all specific psychiatric diagnoses reported in Table III, that is the odds for school failure was higher for students with a psychiatric diagnosis than for those without a diagnosis.
The logistic regression analysis estimating log odds values (Table IV) showed a significant interaction between any psychiatric diagnosis and grades in school year 6, which is reflected in Table V and interpreted in connection with that table.
Predictive percentages of school failure converted from log odds are reported within each of four cells that reflect the interactive effect between the dichotomous variables of any psychiatric diagnosis and completion of subjects in year 6 (Table V). Early school performance moderated the association between psychiatric diagnoses and later school failure, and vice versa. The differences in predictive percentages were large between the four combinations of the two interacting variables. Almost every second student with a psychiatric diagnosis and incomplete grades in school year 6 failed in school year 9. Compared with students with no psychiatric diagnosis and complete grades in school year 6, the likelihood for school failure in school year 9 was around 22 times as high for this subgroup. The results also showed that among students with complete grades in school year 6, the likelihood for school failure is 4.5 times higher for those with a psychiatric diagnosis compared with students without a psychiatric diagnosis.
Excluding year 6 grades in the regression models I and II increased the odds ratios for both low parental education and neuropsychiatric diagnoses, which indicated that these variables are likely to affect school performance in school year 9 both directly and indirectly by influencing grades in school year 6.
Discussion
The present study showed that psychiatric diagnoses, grades in school year 6 (completion of all subjects) and parental education were strongly associated with subsequent school failure in school year 9. This applied to the measure of ‘Any psychiatric diagnosis’ as well as specific diagnoses such as depression, anxiety and neuropsychiatric diagnoses. The most striking result was the combined and interactive effects of grades in school year 6 and ‘Any psychiatric diagnosis’ on school failure, even after adjustment for sociodemographic factors.
Only a few register studies have previously analysed associations between mental illness and school failure among adolescents in Sweden [14,25]. These studies have focused on school outcomes in school year 9 without specific consideration of school achievements in earlier years. The current study demonstrated that the combined and interactive effect of psychiatric diagnoses and early school achievement turns out to be decisive in disentangling the risk factor patterns for later school failure in school year 9. Among the sociodemographic factors, only the level of parental education showed a strong association with school failure, adjusting for all other predictor variables. The tentative analysis considering the age at last visit to specialised care indicated that the association of early school achievement and psychiatric diagnosis with subsequent school failure was stronger among students with a more recent visit to specialised care.
The results demonstrated that interdisciplinary approaches are necessary not only for identifying which factors matter for school achievement, but also for estimating the different magnitudes of these factors. The process to bridge the gap between educational and public health research has been relatively slow in Sweden, which appears in a literature review published by the Swedish National Agency for Education [26]. A State of the Science conference organised by the Royal Swedish Academy of Sciences marked a turning point in the Swedish context by highlighting the relationships between mental ill health and academic achievement [27].
Strengths of the study
Although low early school achievement is a known risk factor for subsequent school failure, there is a scarcity of research on the associations between mental health and school performance that take early school achievement into account. The current study responds to this gap by not just including a variable on early school achievement in the analyses, but also analysing associations based on the combined and interactive effects of early school performance and psychiatric diagnoses.
By demonstrating how early school achievement interacts with psychiatric diagnoses in relation to school failure at the end of compulsory schooling, this study adds to the small number of Swedish register studies on mental health and school failure. Considering grades in school year 6 in the analyses may also account for prior academic ability, and thereby reduce the potential risks of omitted variables.
Moreover, this study benefits from almost complete register data on sociodemographic factors, school performance and psychiatric diagnoses. Interaction effects were tested, and potential confounding variables and comorbidity were controlled for.
Study limitations
This study has limitations. The data on psychiatric conditions include only diagnoses set within special care, excluding mentally ill patients in community primary care. In the current sample, around one-fourth of the prescriptions of benzodiazepines, melatonin, antidepressants and ADHD medications until 2019 did not pertain to a diagnosis set in special care. This indicates that there might be a group of adolescents that meet diagnostic criteria but have not been registered. Whether this restriction of the register data on diagnoses affected the association between psychiatric conditions and educational outcomes is uncertain. There are studies reporting similar patterns of diagnoses in primary and specialist care, but there are few, if any, temporal studies that have examined the association between common psychiatric diagnoses set in primary care and educational outcomes.
The analyses were performed without consideration of the timing of the psychiatric diagnosis, nor the number of occasions that care was provided. Therefore, neither effects of exposure versus outcome nor effects of dose/exposure versus response could be estimated. It follows inevitably that causal conclusions cannot be made regarding the impact of mental health on school failure using the data available for this study. The results of the analyses of associations have been interpreted bearing these limitations in mind.
Conclusions
Psychiatric diagnoses and completion of subjects in school year 6 were strongly associated with school failure in school year 9. These two variables interacted and their combined effects on school failure are striking. This study demonstrated that early school performance moderated the association between psychiatric disorders and later school failure, and vice versa. Therefore, in order to properly estimate the magnitude of risk factors for failure in school year 9, the impact of the interaction between psychiatric diagnoses and grades in school year 6 on school failure needs to be accounted for. Broadly, the results present challenges for the educational and public health fields, which are reinforced by recent data showing an increase in adolescent mental health problems in many countries accompanied by poorer academic achievement.
In particular, the results of the current study underscore the importance of early identification of signs of school failure in order to provide opportunities to prevent mental health problems and to support school achievement. The school system should promote healthy and supportive learning environments for children from their first school years and onwards. Major efforts are required to support children’s academic performance, which is justified also from a mental health perspective. There is also a need for prevention measures and health promoting programmes that directly address the mental health problems among children and adolescents.
Footnotes
Acknowledgements
Professor Jan-Eric Gustafsson, Professor Francis Mitrou, Associate Professor Tamsin Newlove-Delgado and Professor Stephen R Zubrick provided valuable comments on earlier versions of the manuscript.
Author contribution
CH designed the study and conducted the analysis. DB contributed to the interpretation of the results. CH drafted the manuscript and DB critically revised it. Both CH and DB read and approved the final manuscript.
Availability of data
The project data are not publicly available and requests for data should be directed to Statistics Sweden.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Sten A Olsson Foundation for Research and Culture to the project ‘School, learning and mental health: Determinants, consequences and prevention of school failure’.
Ethics
The current study is solely based on register data and is conducted as a part of the project ‘School, learning and mental health: Determinants, consequences and prevention of school failure’, which was approved by the Swedish Ethical Review Authority (decision 2020-12-18, dnr 2020-04933).