
Abstract
Aims:
The Health in All Policies (HiAP) approach is based on the understanding that much of health and health equity is constructed in society outside the health sector, and that health and health equity are also crucial for achieving many other societal goals. To strengthen the implementation of HiAP in the European Union, we will study the current systems and practices for inclusion of health and health equity perspectives in policies across sectors. We will also examine the opportunities for health in various sectoral policies and the challenges in evidence-informed policymaking, including those posed by commercial actors. This work is done as part of the Joint Action on the Prevention of Cancer and other Non-communicable Diseases (JA PreventNCD).
Methods:
We will collect scientific literature, policy documents, grey literature, utilise databases, conduct interviews and organise workshops. For analysis, we will use content, policy and stakeholder analyses, as well as quantitative methods. We will compare results between countries. Results: The final outputs include research articles, policy briefs, reports, toolboxes, policy dialogues and capacity-building activities.
Conclusions:
This work aims to strengthen the inclusion of health and health equity perspectives in policymaking by assessing the current landscape, developing tools, providing actionable recommendations and engaging in policy dialogues with decision-makers.
Keywords
Background
A significant portion of health is constructed in society outside the health sector [1]. The Health in All Policies (HiAP) approach seeks to ensure that health implications are considered in policymaking across sectors and appropriate levels of governance.
This article describes the planned work on HiAP as part of the Joint Action on the Prevention of Cancer and other non-communicable diseases (JA PreventNCD), which runs from 2024 to 2027. The aim of the JA PreventNCD project is to support strategies, policies and practices that reduce the burden of NCDs and reduce inequities in NCDs [2].
In this paper we will describe the major concepts for intersectoral health policies, then provide background on the issues to be studied and outline our major aims. We will describe the methods used and discuss the limitations, challenges and potential significance of the anticipated results. This paper only provides a brief overview of the methods we will use: detailed descriptions of data selection, participant identification and recruitment and methods used for analysis will be provided in subsequent papers that address specific aspects of the project.
Evolution of intersectoral work on health and health equity
Over time, efforts to work with various societal sectors and their policies with the potential to contribute to and benefit from health and health equity have expressed their role through various evolving concepts, such as intersectoral action for health (Alma-Ata Declaration, 1978) [3], healthy public policies (Ottawa Charter, 1986) [4] and HiAP [5,6].
The HiAP concept (see Box 1) was initially developed to protect health in the context of the European Union (EU) [7]. While organising and financing health services are mainly the competence of member states, EU-level policies contribute to regulating the quality, availability and marketing practices of many health determinants and risk factors, such as food, tobacco and alcohol. The EU’s internal market seeks to guarantee free movement of goods, services, people and capital, which has implications for health-related products, determinants of health and the context in which health services can be organised and financed in the member states.
Definition of Health in All Policies [8].
The need for protecting human health in EU policies became especially clear and urgent when many member states were affected by bovine spongiform encephalopathy (mad cow disease) in the 1980–90s [9]. The legal basis for health policy measures was first expressed in the Maastricht Treaty in 1992, strengthened in the Amsterdam Treaty in 1997 and consolidated as part of the Lisbon Treaty Article 168 (Box 2) in 2007 [10].
Article 168 of the Lisbon Treaty (16).
The HiAP concept was first introduced in 2006 when it was the main health theme of the Finnish EU presidency [7]. In 2013, the World Health Organization’s (WHO) 8th Global Conference on Health Promotion in Helsinki focused on HiAP [11].
The need for applying the HiAP approach arises from three basic policy situations (Figure 1) [11 –13]:
(1) To solve complex health and health equity problems together with other sectors, such as meeting the intersectoral challenges of mental health.
(2) To promote the contribution of health, health equity and health systems for important societal aims, such as those pursued under work on wellbeing economy (WBE). The WBE is a concept proposing that a paradigmatic shift towards wellbeing and economic and ecological sustainability should be taken.
(3) To integrate health, health equity and health systems perspective into non-health sectors’ policies, such as policies on agriculture and urban planning.
The United Nations Sustainable Development Goals (SDGs) [14] link health to other key areas such as poverty, education and environment recognising that good health, health equity and the availability of equitable, high-quality health systems are cornerstones for many societal goals, such as the ability to learn and work, and vice versa [1,15]. The WHO has recommended key intersectoral policy interventions to tackle the most important risk factors for NCDs, also called ‘best buys’ and ‘quick buys’ [16,17]. They represent evidence-based intersectoral actions regarding tobacco, alcohol, nutrition and physical activity.
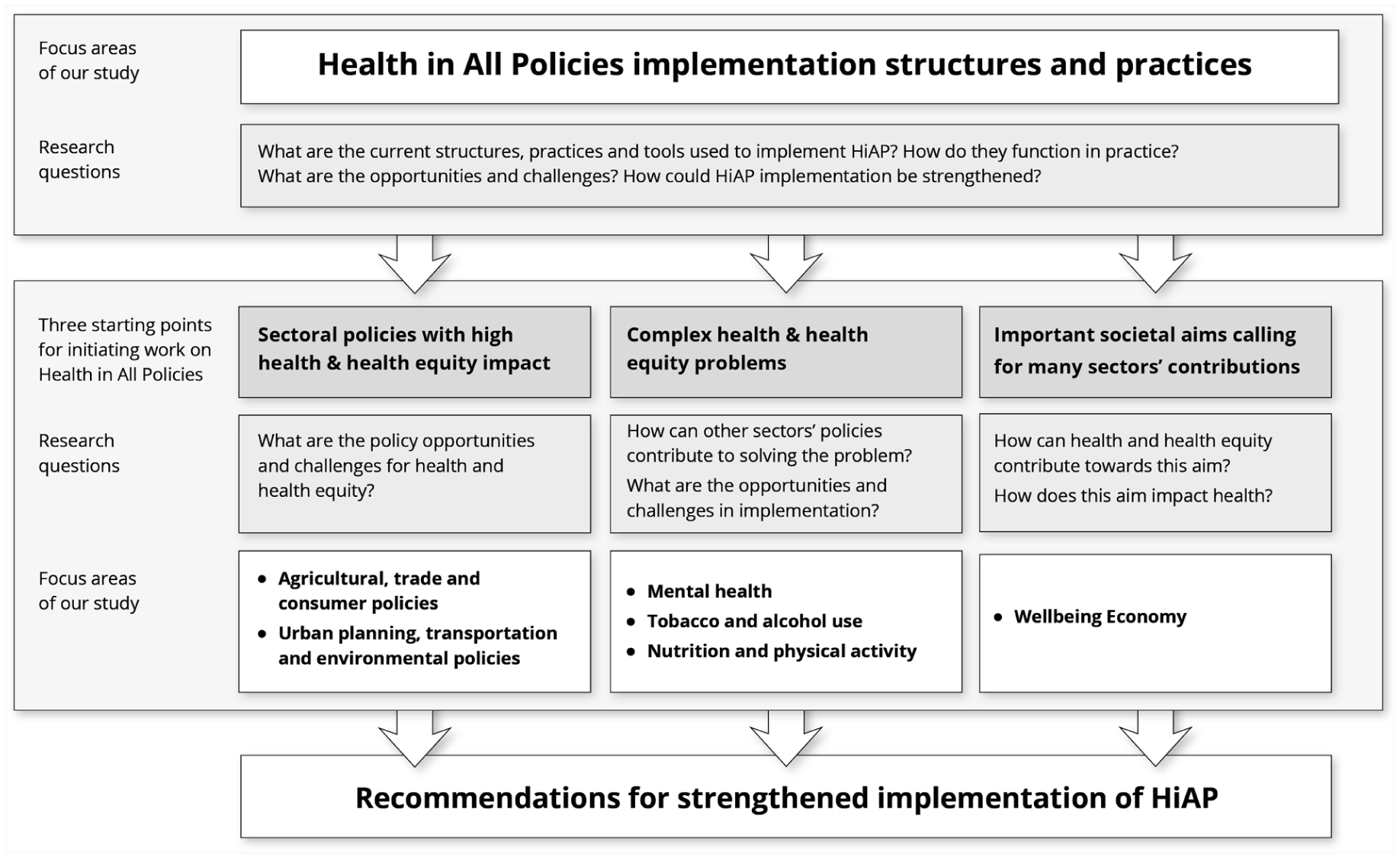
The framework, study areas and main research questions of our work.
The commercial determinants of health are private-sector activities that affect people’s health, directly or indirectly, positively or negatively [18]. Corporate political activity involves the strategies and practices of commercial actors to prevent, shape, circumvent or undermine public policies, and influence public opinion in ways that favour corporate interests [19].
Rationale for our work: previous research
This work is being carried out as part of the JA PreventNCD project, co-funded by the EU and the participating countries or their institutions from 2024 to 2027. Joint Actions (JAs) are collaborative projects involving multiple EU and associated countries, which aim to address key EU health policy priorities, for example, by sharing, testing and refining successful tools, methods and approaches [20]. Therefore, they are not purely research endeavours but also aim for shared learning and practical implementation. The EU’s call for proposal for this JA-guided our work in terms of the major determinants of NCDs selected, such as food systems and nutrition, physical activity, tobacco and nicotine products, alcohol, sleep and climate change.
With the overall aim of strengthening the inclusion of health and health equity in policymaking, our study examines structures, practices and tools for HiAP implementation, as well as some specific health issues, sectoral policies and societal goals (Figure 1). The emphasis is on the current functioning, opportunities and challenges and recommendations for improvement in intersectoral work. In this paper we provide a brief review of the areas on which we are focusing our work.
HiAP implementation involves considering health, health equity and health system perspectives in decision making and implementation across sectors in various ways. Previous research on HiAP has analysed the legal basis, structures and tools of the approach [21 –24] and developed models for HiAP implementation [13,25,26]. Implementing intersectoral health policies has proven challenging, partly due to the complexity of devising effective policies [27]. Furthermore, HiAP implementation occurs in diverse cultural, political and economic contexts, dealing with a variety of policy sectors. Consequently, there is no universal model for HiAP implementation, and governments must continually adapt their strategies, structures and tactics [17,21,22,28,29].
Structural health policy measures include fiscal measures [30,31], regulatory measures and other interventions [32,33]. For example, reducing or eliminating significant risk factors, such as tobacco and alcohol use, requires regulation, taxation and other intersectoral policies that affect price, availability, product characteristics and information provision [34 –36]. Although evidence-based policies have been identified in areas such as tobacco, alcohol and nutrition, these policies are not always implemented [37 –39].
In addition to intersectoral working methods, one of the major tools for HiAP implementation has been prospective impact assessments of proposed policies, such as prospective sectoral-specific assessments [40 –43], health impact assessments and integrated assessments. Previous studies have indicated that health and health equity impacts are often assessed narrowly or otherwise poorly in assessments not specifically focused on health [44 –49].
The WBE is an evolving concept that aims to create a strategic shift toward a society where human and ecological wellbeing are prioritised over purely material growth. In 2019, the Organisation for Economic Co-operation and Development published a working paper on the economy of wellbeing [50], and the Council of the EU issued conclusions on the same topic during the Finnish EU presidency [51]. The concepts of the economy of wellbeing and the WBE are often used interchangeably to reflect a shared call to reorient the overarching aims of policymaking, from a narrow focus on economic growth to the pursuit of sustainable wellbeing for people and planet, alongside economic considerations. The concept’s definition, content and implementation strategies are still under development [50,52,53]. The main tools identified for implementing the WBE include developing indicators that capture the various dimensions of wellbeing [54 –56], cost–benefit analyses of interventions, wellbeing budgeting [57], and some wider national frameworks [58].
Poor mental health represents a complex health problem, mental health symptoms being very common among European citizens, affecting not only mental wellbeing (i.e. the individual’s subjective experience or emotional state [59]), but also overall health and the achievement of other personal and societal goals. The most important factors for achieving good mental wellbeing are intersectoral [60]. Good mental health and wellbeing are important for the achievement of many sectoral goals beyond those of the health sector. Mental health stigma refers to the negative attitudes, beliefs, and stereotypes people may hold towards those who experience mental health conditions [61]. Sleep is another neglected public health issue that requires intersectoral action [62].
Intersectoral collaboration is easier when mutual benefits can be identified and win–win solutions are possible, but the aims may also conflict. The WHO has estimated that commercial determinants such as tobacco, alcohol, processed food and beverages (i.e. those that contribute to a diet high in processed meat, sodium, sugar-sweetened beverages and trans fatty acids), fossil fuels and commercial practices (such as exposure to occupation-related carcinogens), account for almost a quarter of all deaths in the WHO European region [18]. Furthermore, The Global Burden of Disease study has estimated that approximately a third of deaths worldwide are attributable to risk factors related to commercial determinants such as alcohol, drug and tobacco use and unhealthy diets [63].
To study the opportunities and challenges that sectoral policies present for health and health equity, we have chosen to focus on major policies affecting nutrition and physical activity. Eating habits are complex and influenced by factors such as availability, price and marketing, all of which are shaped by multiple policies, including those relating to agriculture, trade and consumer affairs. Most of these policies, which are crucial for nutrition, have other goals too. For example, agricultural policies are designed to achieve goals such as food, feed, and alcohol production, rural development, market stability and food affordability (see also Gillespie et al. [37] and Hawkes [64]). Previous EU-level analyses have found that ‘diets have been a major casualty of incoherent policies’ and have identified the need for greater coherence between policy sectors [65]. Similarly, a number of policies [66,67], including on urban planning, transport, forestry and the environment, influence opportunities for physical activity [40,41,68] though their primary objectives are not health related.
In terms of nutrition and healthy food environments, a Healthy Food Environment Policy Index (Food-EPI) has been established and studied in 11 countries [69,70]. On physical activity, The Global Action Plan on Physical Activity, the Council recommendation (2013/C354/01) on health-enhancing physical activity and Physical Activity Environment Policy Index (PA-EPI) has been established [71]. Nutrition policy environments have been compared across countries [72], while the only European country to have applied PA-EPI is Ireland [73].
Aims
The main aim of our work is to strengthen the inclusion of health and health equity into policymaking across sectors.
The overarching aims are:
(1) to explore the functioning of current structures, processes and tools for the inclusion of health and health equity in policies across sectors;
(2) to identify opportunities and challenges in including of health and health equity considerations;
(3) to assess and develop monitoring and evaluating policy implementation;
(4) to make recommendations for strengthened inclusion of health and health equity perspectives in policies across sectors.
Methods
Planning was initiated by inviting representatives of all countries eligible for JA funding to contribute suggestions and feedback on the proposed work. Once the overall framework had been established, participating countries were asked to sign up for specific activities in which they wished to participate and to nominate their participating institution and representatives. Participants in our work on HiAP include researchers, policy planners and implementers from 16 countries, with 37 partner organisations involved. Detailed work plans for the tasks were developed with the task leaders. In our work package within the JA, six tasks (Figure 1 and Table I) contribute to the four overreaching aims of our work. For the timeline of the major outputs, see Figure 2.
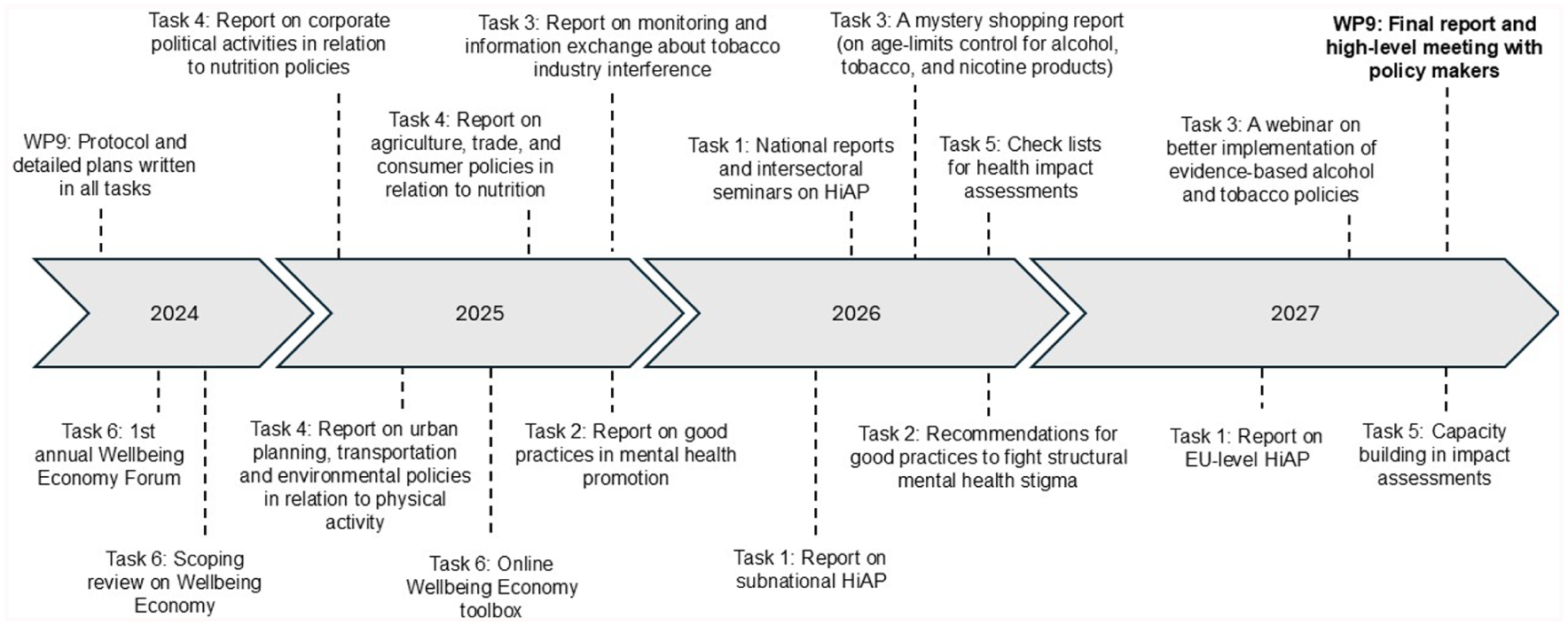
Timeline of major activities in JA PreventNCD ‘Health in All Policies’.
Overview of the objectives, methodology and countries involved in the study.
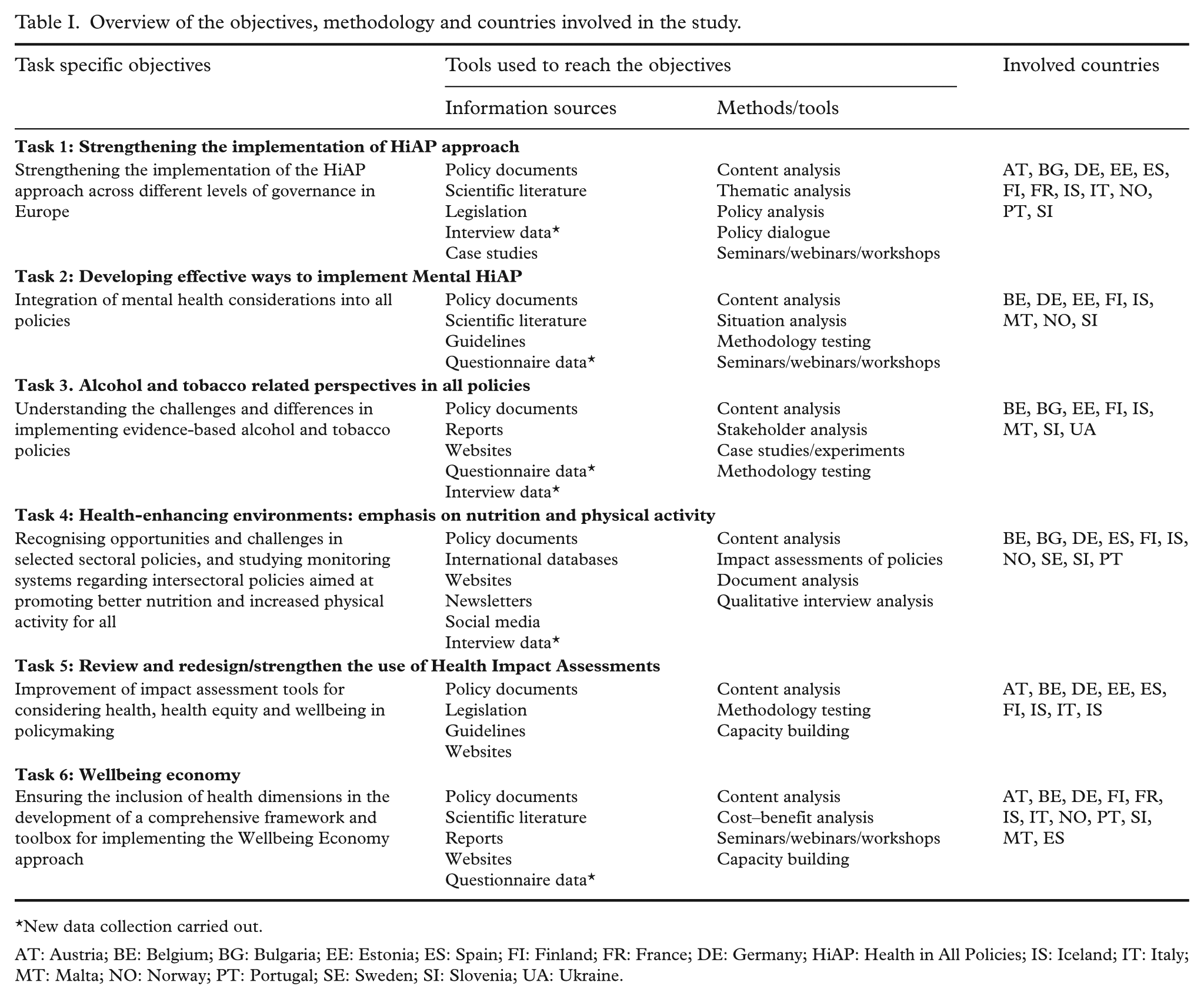
New data collection carried out.
AT: Austria; BE: Belgium; BG: Bulgaria; EE: Estonia; ES: Spain; FI: Finland; FR: France; DE: Germany; HiAP: Health in All Policies; IS: Iceland; IT: Italy; MT: Malta; NO: Norway; PT: Portugal; SE: Sweden; SI: Slovenia; UA: Ukraine.
Aim (1) To explore the functioning of the current structures, processes and tools for the inclusion of health and health equity in policies across sectors
A scoping review will be conducted to study EU-level HiAP implementation, analysing major policy documents and conducting interviews with policymakers, experts and EU-level public health non-government-organisation representatives. At the national level, we will examine the structures, practices, processes and various tools integrating health and health equity into policymaking. To do this, policy documents will be analysed, and thematic interviews will be conducted with policymakers and experts in nine countries [74 –77]. The current functioning of HiAP implementation, as well as administrative and political challenges, will be explored. National reports will be written and discussed in national intersectoral seminars. We will also analyse data from WHO Healthy Cities network and conduct case studies on subnational HiAP implementation in six countries. The results from different countries and subnational-level case studies will be compared, and good and innovative practices will be identified (task 1 in Table I).
Prospective integrated impact assessments will be reviewed for their health and health equity aspects. Based on this review, a checklist for assessing health and health equity in impact assessments will be developed and piloted in specific policy proposals or projects in the participating countries. A toolbox for impact assessments will be developed, and capacity-building activities will be conducted (task 5 in Table I). We will also develop and evaluate a tool for assessing mental health promotion policy interventions (task 2).
The foundations of the WBE concept will be clarified through a scoping review. Implementation strategies will be examined through case studies in two participating countries, and via a survey in nine countries. The inclusion of health and health equity will be a key focus of this work (task 6, Table I).
The use of cost–benefit analyses for selected wellbeing interventions will be explored. These interventions will be selected in collaboration with relevant experts, including partners from the Wellbeing Economy Alliance, which brings together organisations, alliances, movements and individuals working towards a WBE. The process will also be informed by established resources such as the WHO’s ‘best buys’ for the prevention and control of NCDs [78]. The criteria for selecting best practices will include policy relevance, institutional integration, evidence of impact, transferability and feasibility in practice.
Emerging and existing wellbeing policies for WBE implementation will be identified through a review of the literature and a validated survey distributed to representatives of participating countries and other stakeholders. An online toolbox will be developed, containing tools that have been identified, assessed and, in some cases, developed within our work (task 6).
Aim (2) To identify opportunities and challenges in including health and health equity considerations
Taking stock of previous EU work on intersectoral mental health, we will design a survey to further explore how mental health promotion is incorporated into various sectoral policies. The aim is to identify good practices, opportunities and challenges in systematically including mental health. Building on the European Commission (EC)’s support package on stigma and the WHO toolkit on stigma [79], we will conduct a survey to analyse structural mental health stigma and seek to identify best practices in avoiding it (task 2).
To provide recommendations for intersectoral action on improving sleep, we will collect information on sleep data and existing intersectoral strategies to improve sleep from seven countries. We will then identify relevant sectors and stakeholders, recommended actions, cross-cutting sectoral interests and co-operation between actors for these strategies and formulate recommendations for action (task 2).
In focusing on nutrition and physical activity, we will study how they are or can be impacted within selected sectoral policies, such as agricultural, trade, urban planning, active transportation and environmental policies. Using literature reviews and online databases, we will explore the implications of the Common Agricultural Policy, as well as trade and consumer policies on food, tobacco and alcohol production at the EU level. For national policies affecting nutrition, we will focus on the food environment, and analyse laws, regulations, guidelines and programmes linked to agricultural, trade, consumer and possibly environmental policies (task 4).
Regarding physical activity, the Global Action Plan on Physical Activity, the Council recommendation (2013/C354/01) on health-enhancing physical activity and PA-EPI will provide a framework that will be used to examine the role played by urban planning and transport policies on physical activity [66,67,80]. The role of climate change for public health policies is also examined, with Germany as a case study (task 4).
We will explore the obstacles and enablers for developing and implementing evidence-based policies on alcohol, tobacco and nicotine by conducting stakeholder analyses and interviews with key actors (tasks 3 and 4). We will also examine tobacco and nicotine industry interference by reviewing open data sources (task 3).
The corporate political activities of relevant food industry actors will be explored by analysing public national-level documents of national umbrella organisations and other major food industry actors. This will enable us to identify the frameworks, strategies, practices and mechanisms used to prevent, weaken or delay the design and implementation of public health nutrition policies. We will then conduct in-depth interviews with stakeholders (e.g. politicians, policymakers and civil society organisations), which will be analysed qualitatively using existing frameworks to categorise the identified practices (task 4 in Table I).
Aim (3) To assess and develop monitoring and evaluating policy implementation
We will examine policy documents from various international organisations, such as the United Nations agencies and the EU, to identify existing process indicators for tracking and monitoring intersectoral policies on good environments for nutrition and physical activity. A thematic qualitative analysis will then be conducted to identify the usage and relevance of the identified indicators, as well as any gaps in them (task 4 in Table I).
Building on earlier work with the Food-EPI [69], we will review the implementation status of policies aimed at creating healthy food environments in selected countries, while also exploring their linkages with environmental sustainability. A methodology and template will be developed for data collection across the countries involved in this task (task 4).
The objective 2 of the Global Action Plan on Physical Activity 2018–2030, the Council Recommendation (2013/C 354/01) health-enhancing physical activity and the PA-EPI, will be studied as a basis for a framework. A template for reviewing the implementation of the international recommendations in comprehensive intersectoral national plans on physical activity in at least three countries will be designed (task 4 in Table I).
Finally, we will survey the experiences and perceptions of the supervisory authorities in five countries on the strategies used by private off-premises outlets to maximise alcohol, tobacco and nicotine sales. Furthermore, to assess age-verification practices, we will map current mystery shopping practices in Europe and test selected mystery shopping practices in selected European countries (task 3).
Aim (4) To make recommendations for strengthened inclusion of health and health equity perspectives in policies across sectors
The results of this work will be formulated into suggestions and recommendations for policymakers. Policy dialogues in the form of seminars and co-creation workshops will be organised. Presentations in policymakers’ forums, scientific conferences and seminars will provide opportunities to engage with policymakers at the various levels of governance. The draft results from the national-level HiAP analyses will be discussed in national intersectoral seminars in nine countries. An annual international WBE Forum has been established, providing further opportunities for presentations and dialogue. The tools being developed for assessing health and health equity impacts, cost–benefit analysis of interventions that promote good health and wellbeing, as well as wellbeing budgeting guidelines, will be made available on open websites and promoted for use, alongside capacity-building efforts to support their use. A final report will summarise the various aspects of this work, and the results and recommendations will be discussed in an international meeting for policymakers.
Discussion
Joint Actions are a means of sharing knowledge, experiences and learning across countries in Europe. They aim to engage policymakers by valuing tacit knowledge and practical understanding alongside academic research and practice to discuss and compare experiences in various countries. Our work will provide ‘real-world evidence’ and insights into improving the inclusion of health and health equity perspectives in policymaking across sectors at the various levels of governance in the EU, its member states and associated countries. Our focus is on understanding the dynamics, opportunities and obstacles in integrating health and health equity in policymaking, learning from each other’s experiences and making recommendations for improved performance.
Due to the funding rules of JAs (specifically, who is eligible for funding, the requirement for resource allocations to go through the competent authorities designated by the Ministry of Health in each country and the rule that any funded organisation must have a legal link to the competent authority), participation from sectors beyond health is somewhat complicated. In our work, most of the participants are mainly linked to the health sector, although some participants work in others, such as social affairs, agriculture, forestry and economics. The scarcity of professionals from outside the health sector limits our work around improving our understanding of the aims, objectives and strategies, as well as working methods of sectors beyond those of health. Another limitation is that we focus mainly on ways in which health and health equity could benefit from intersectoral work, and to a much more limited extent on how improved health and health equity can support the goals and policies of other sectors [81].
The HiAP and WBE approaches have the potential to be mutually beneficial. The HiAP concept has evolved from decades of history of experience on various concepts on intersectoral health policymaking. HiAP aims at evidence-informed policymaking by assessing impacts on health, health equity and health systems and emphasising intersectoral dialogue and negotiations, that is, it is rooted in administrative practices to enhance health and health equity in policymaking. WBE aims for a wider paradigm shift in the aims of societal policies, and with indicators monitoring that shift in political priorities and their implementation in practice. While HiAP has often remained largely within the health sector, WBE concept development has had major contributions from social scientists and economists with underpinnings from welfare state discussions, but stronger attention to ecological and economic sustainability and on developing socioeconomic indicators and wellbeing budgeting. Our work on the WBE concept and tools emphasises ensuring that the potentials and needs of health, health equity and health systems are properly included in the concept, its tools and implementation strategies.
While wellbeing and health have strong mandates at national and subnational levels, Article 168 of the Lisbon Treaty provides a strong mandate also for HiAP at the EU level and the Treaty on European Union Article 3 for WBE [82], and the Social Pillar gives support both for HiAP and WBE [83]. Our work aims to examine how this strong mandate could be made more explicit and stronger in the practices of the EU, as well as its member states. Further work is needed to establish synergies between the concepts, their strategies, policy entry points and tools.
Conclusion
This work seeks to strengthen the inclusion of health and health equity perspectives in policymaking across sectors by assessing the current landscape, analysing opportunities and challenges in current systems and practices, providing actionable recommendations, engaging in policy dialogues with decision-makers and providing capacity building.
Footnotes
Acknowledgements
We extend our sincere thanks to the editors and reviewers for their constructive and thoughtful comments, which significantly improved the quality and clarity of this article. We are also grateful to all participants of the HiAP work package, as well as to the entire JA PreventNCD team, for their work and support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This document forms part of a project that has received funding from the EU4Health programme under grant agreement no. 101128032. The information reflects the authors’ views only, and the European Commission is not responsible for any use that may be made of the information it contains.
Ethical considerations
All scientific research activities in this work package adhere to the ethical guidelines and principles to ensure participants’ rights and follow overarching ethical principles set out for the EU-funded research. The task leader of each research activity is responsible for carrying out the ethical pre-review at their institutional review board. In addition, the JA PreventNCD Ethics Board has an advisory role and reviews all the proposals. Furthermore, each partner must obtain the required ethical approvals from the relevant ethics committee (institutional, regional, national) if necessary.