
Abstract
Background:
Adolescence is a life phase in which future life opportunities and patterns of adult health are established. There is growing concern about excessive screen use among adolescents. Health literacy is associated with various health behaviours, but the association with screen use is scarcely studied. The aim of this study was to investigate associations between health literacy and diverse types of screen use among students and to identify possible gender differences.
Methods:
Cross-sectional data was collected from a self-report survey distributed to 1425 (68.5% of those invited) 13-year-old students across 48 schools from 19 municipalities in Norway. Associations between self-reported health literacy (gathered using the Health Literacy in School Aged Children scale) and time spent on gaming, social media, TV, and total screen use were studied using linear mixed effect models.
Results:
Overall, a statistically significant association between health literacy and screen use was identified: an increase in health literacy tends to be associated with a decrease in screen time. This association was stronger for girls than boys and varied with different screen activities. The health literacy mean score was statistically significantly higher for boys (30.43) than girls (29.81), but the difference was small. About 25% of the students spend seven hours or more on screens on weekdays outside school hours. Girls are more likely to use social media and boys are more occupied with gaming.
Conclusions:
Introduction
Adolescence is a sensitive and crucial life phase that lays the foundation for future opportunities and establishes patterns of adult health [1]. This period offers a crucial opportunity to implement prevention and intervention strategies that promote healthy growth, development, and well-being. The World Health Organization (WHO) recognizes health literacy as a modifiable resource for personal well-being and overall growth, and a key indicator of health, emphasizing the enhancement of health literacy as global priority [2]. Measures and definitions of health literacy vary [3]. The Organisation for Economic Co-operation and Development (OECD) defines health literacy as ‘an individual’s knowledge, motivation and skills to access, understand, evaluate and apply health information’ [4].
One commonly used instrument for assessing health literacy among adolescents (10–18 years) is the Health Literacy in School Aged Children (HLSAC) scale [3]. A study using HLSAC scores from 10 European countries found that 13.3% of the participants scored low, 67.2% scored moderate, and 19.5% scored high on measures of health literacy [5]. However, studies reporting scores by gender are inconclusive concerning differences [5, 6]. While some studies have found that boys report lower levels of health literacy than girls [6], other, more recent studies have found no gender differences [5].
Research indicates that increased health literacy in adolescence is associated with health-promoting behaviours like higher levels of physical activity and healthy diet [3]. In contrast, lower levels of health literacy are associated with unhealthy behaviours like smoking and alcohol use [3]. Also, in studies examining the associations between health literacy and various health behaviours, the findings are inconsistent when it comes to gender differences, with most studies revealing no significant variation between genders [3, 7]. Additionally, sosioeconomic status (SES) has been potively linked to adolescents’ health literacy [8]: the higher SES the higher health literacy.
In light of these findings, OECD members highlight the importance of developing health care services that support and enhance health literacy among the population [9]. In Norway, the School Health Service is legally mandated to carry out health promotion and preventive work for all students, regardless of background and social status, with the aim of reducing health disparities and promoting equity. This mandate is outlined in the National Guideline for the School Health Services [10], which strongly recommends promoting health literacy and positive health behaviours. The guidelines include a recommendation to limit screen time among adolescents. Excessive screen use is a primary concern for parents in Western countries regarding their children’s lifestyle and health behaviour, ahead of nutrition, bullying, and physical inactivity [11]. A substantial body of evidence indicates that increased screen time is associated with various health risks for children and adolescents, with the strongest evidence supporting links to obesity, unhealthy diet, depressive symptoms, and lower quality of life [12]. Nevertheless, screen use is multifaceted, influenced not only by the duration of use and type of device but also by the content and the environment in which the exposure takes place [11]. Moderate levels of screen time, on the other hand, are associated with positive psychosocial functioning and can have positive educational effects [11, 12].
Prior studies indicate a small gender difference among adolescents in terms of total screen use [13]. Although the content of their screen activities varies, girls dedicate more time to smartphones, social media, texting, and general computer use, while boys allocate more time to gaming. Social comparison, image concerns, and self-harm contagion tend to be more prevalent on social media than on gaming platforms [14, 15]. This may partly explain why previous research has found that the association between extensive digital media consumption and diminished psychological well-being is more pronounced among teenage girls compared to boys [16]. In line with these concerns, the WHO recommends limiting screen use [17], with more than two hours a day considered excessive screen time for school-aged children. Despite this, 46.4% of 6–14-year-olds spend more than two hours per day on screen activities [18]. In Norway, 74% of 13–18-year-olds report spending more than three hours daily in front of a screen outside of school hours, while 28% report more than six hours of screen time [14]. Furthermore, screen use is associated with socioeconomic inequalities in adolescents.
To our knowledge, there is a scarcity of studies focusing on the associations between health literacy and various types of screen use. The one Finnish HBSAC-study from 2021 we have identified focuses on social media [19]. Results from this study indicate that a higher level of health literacy is associated with a lower risk of problematic social media use. More knowledge of the associations between health literacy and time spent on various types of screens may provide insight on how adolescents manage various types of screen activities. This knowledge may be important in preventing the potential risks that follow various types of screen use.
Based on findings from previous studies, we hypothesized that higher levels of health literacy would be associated with lower screen time, with patterns varying by type of screen use and by gender. The overall aim of the present study was therefore to investigate associations between health literacy and different types of screen use among 13-year-old students, stratified by gender.
Methods
Study design and population
This cross-sectional study uses baseline data from a study among 13-year-old students (GuideMe) [20]. A total of 48 lower secondary schools located in urban and rural areas of the southeastern and middle parts of Norway participated in the study. Both large and small schools were represented, with a mean school size of 314 students (SD=189 students). Two waves of 13-year-old students were recruited: 2022/2023 (wave 1) and 2023/2024 (wave 2), and participated during one school year. The students completed an electronic survey in the classroom at the beginning of the semester. The baseline survey was answered by 1425 students, 68.5% of those invited, of whom 50.3% were girls and 49.7% boys (Figure 1). The exclusion criteria were intellectual disability or language problems, defined as not being able to complete the questionnaire. More details about the recruitment procedure can be found in the GuideMe protocol [20].
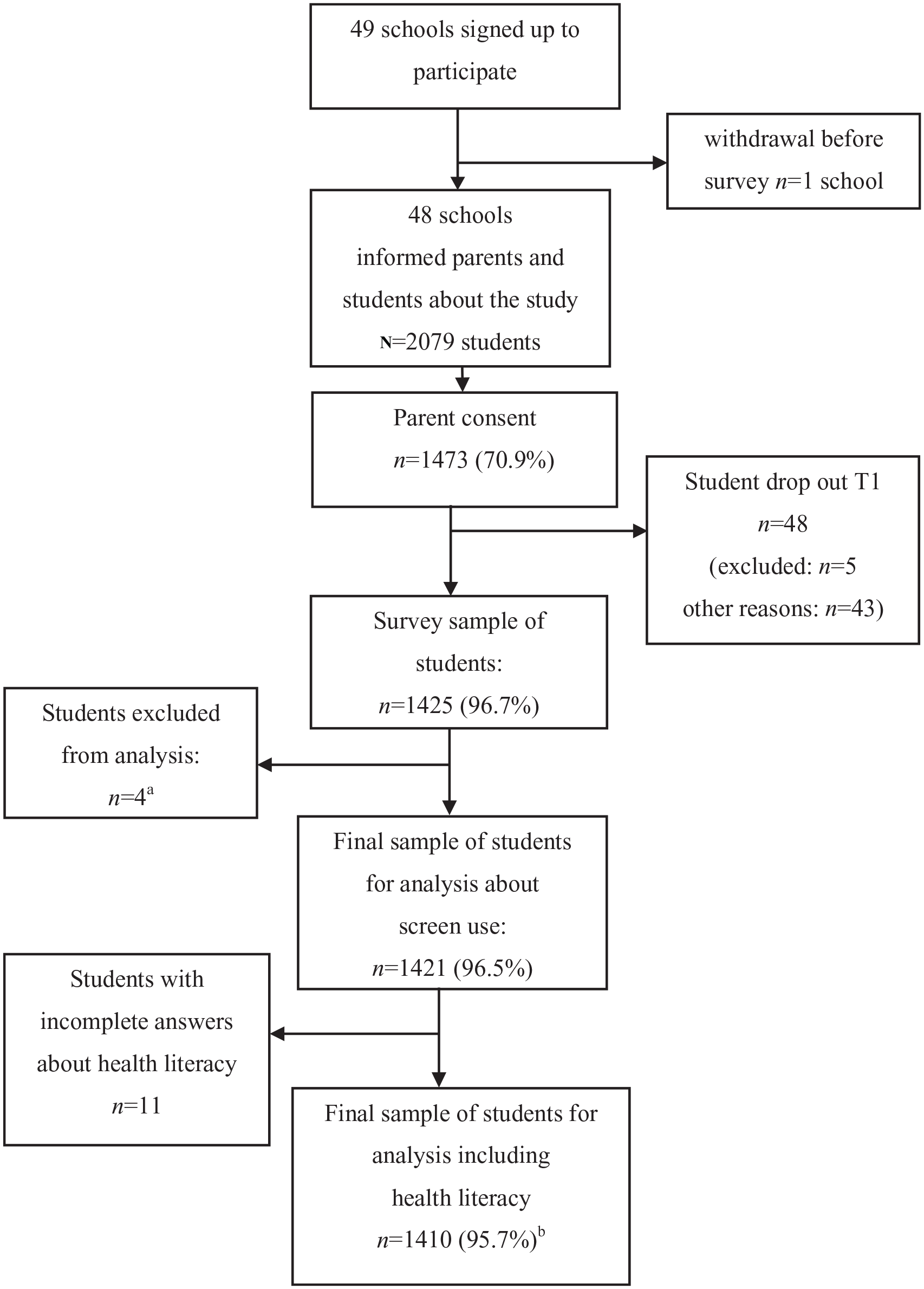
CONSORT flowchart of participating 13-year-old adolescents in Norway, school years 2022/2023 (wave 1) and 2023/2024 (wave 2).
Measures
Health literacy
Health literacy (HL) was measured using the self-report instrument Healh Literacy for School-Aged Children scale (HLSAC) [20]. HLSAC is a 10-item scale and includes five core components. During the development of the HLSAC instrument, health literacy was expanded from a definition to a measurable learning outcome with five components: theoretical knowledge, practical knowledge, critical thinking, self-awareness, and citizenship. Two items tap into each component. All 10 items followed the format ‘I am confident that [. . .]’ and were assessed using a four-point Likert scale. (1=not at all true, 2=barely true, 3=somewhat true, 4=absolutely true). The instrument is constructed as a one-factor model. The HLSAC sum score ranges from 10 to 40. The instrument has been validated in several European countries and shows high internal consistency (ɑ = 0.79–0.90) [21]. Results from the current study indicated that the internal consistency of the HLSAC instrument was excellent (ɑ=0.90). The Norwegian version has been translated and re-translated from English to Norwegian by professional translators. In line with previous studies [5], the health literacy sum score was classified into three categories representing low HL (10–25), moderate HL (26–35), and high HL (36–40) to be able to compare health literacy score levels with previous research [5].
Screen use
Both total screen time and diverse types of screen use during weekdays were assessed through self-report. Types of screen use were measured by three questions covering gaming on different devices (gaming) (1); social media, surfing/chatting (social media) (2); and TV or other screen-based entertainment (TV) (3). The response categories were 0, < ½, ½–1, 2–3, 4–6, and ⩾7 hours per weekday. The total screen time question, taking device multitasking into account, had the following response categories: < ½, ½–1, 2–3, 4–6, 7–9, 9–11, and ⩾ 12 hours per weekday. The questions were inspired by the Young-HUNT study, a longitudinal population study including 13-year-old students from the central part of Norway [22].
Socioeconomic status
Socioeconomic status is considered as a confounder and was determined by asking about the family’s perceived economic situation: ‘How economically well-off do you think your family is compared to most others?’ The response categories were worse off (1), about the same (2), and better off (3). This variable is used as a proxy for socioeconomic status in the Norwegian Young-HUNT study [22].
Statistical analysis
The normal distribution of the variables was evaluated by visually inspecting their histograms as part of the preliminary data analysis. Health literacy was studied using descriptive analysis, including mean and standard deviation (SD), and gender differences were examined using t-tests. The different categories of health literacy (low, moderate, and high) were analysed using chi square tests by gender. Screen use and family’s perceived economic situation were measured using frequencies and percentages, and gender differences were assessed using chi square tests.
Since the study had a cluster design, the students from the same school might not be independent with respect to the outcome variables [23, 24]. Although it is suggested that possible clustering effects may be negligible when intra-class correlation coefficients (ICCs) are below .05, it is also acknowledged that even small ICCs can lead to substantial bias when cluster sizes are large (e.g., greater than 30) [24]. The ICCs were <.05. Linear mixed effect models stratified by gender were applied to examine the associations between health literacy (assessed by the total sum score 10–40) and screen use variables. Gender differences in these associations were assessed using unstratified models that included an interaction term between health literacy and gender. All models were adjusted for family economy. The ordinal response categories for total screen time and types of screen use were transformed for the linear mixed effect model analyses. This transformation was done in line with previous research [25] by estimating the halfway point between the boundaries (e.g. 4–6 hours=5 hours). As the highest categories (>12 hours and >7 hours) had no upper bound, it was assumed that they had the same range as the preceding category and were given the values 14 and 9 hours respectively.
The significance level was set to p<0.05. Descriptive statistics were analysed using IBM SPSS Statistics version 27. Linear mixed effect models were estimated using the R package nlme.
Ethics
The study was performed in line with the Norwegian ethical guidelines for research [26]. The data protection is evaluated by the Norwegian Agency for Shared Services in Education and Research (Sikt, ref id. 694124). This registration ensures compliance with national requirements for data protection, information security, and ethical standards. By using Sikt, the research follows guidelines for digital infrastructure that ensure accessibility, quality, and traceability in the research process.
Informed consent from parents was required due to the students’ age. Active parental consent was obtained digitally from at least one parent. Parental consent was obtained digitally, while students provided consent by responding to the questionnaire. Standardized and customized information was given to both students and parents (written, oral, and in an animated movie) stating that participation was voluntary and that participants could withdraw from the study at any time without stating a reason.
Results
Health literacy
Boys reported higher health literacy than girls (p=0.026), with a mean (SD) score of 30.43 (5.19) vs. 29.81 (5.14). When categorizing the scores into low, medium, and high, there were no longer statistically significant gender differences (p=0.511) (see Table I).
Descriptive statistics of health literacy and family’s perceived economic situation of 13-year-old adolescents in Norway by gender, school year 2022/2023 (wave 1) and 2023/2024 (wave 2).
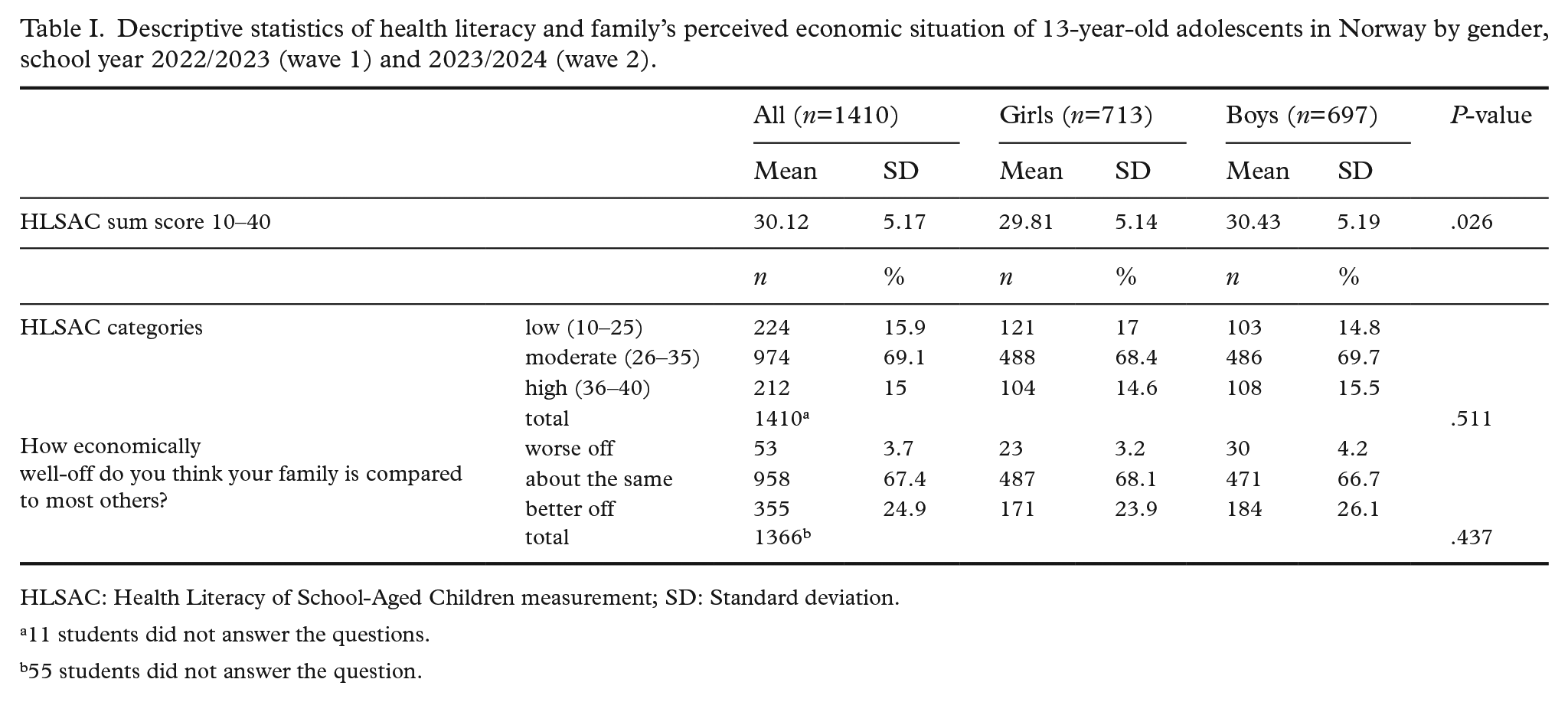
HLSAC: Health Literacy of School-Aged Children measurement; SD: Standard deviation.
11 students did not answer the questions.
55 students did not answer the question.
Screen use
There were no statistically significant gender differences in self-reported total screen time or TV use. Most girls (97.2%) and boys (95.8%) exceeded the World Health Organization’s recommendation of a maximum of two hours of screen time per day. Additionally, 24.4% of the girls and 25.9% of the boys reported using screens for seven hours or more per weekday (Figure 2).
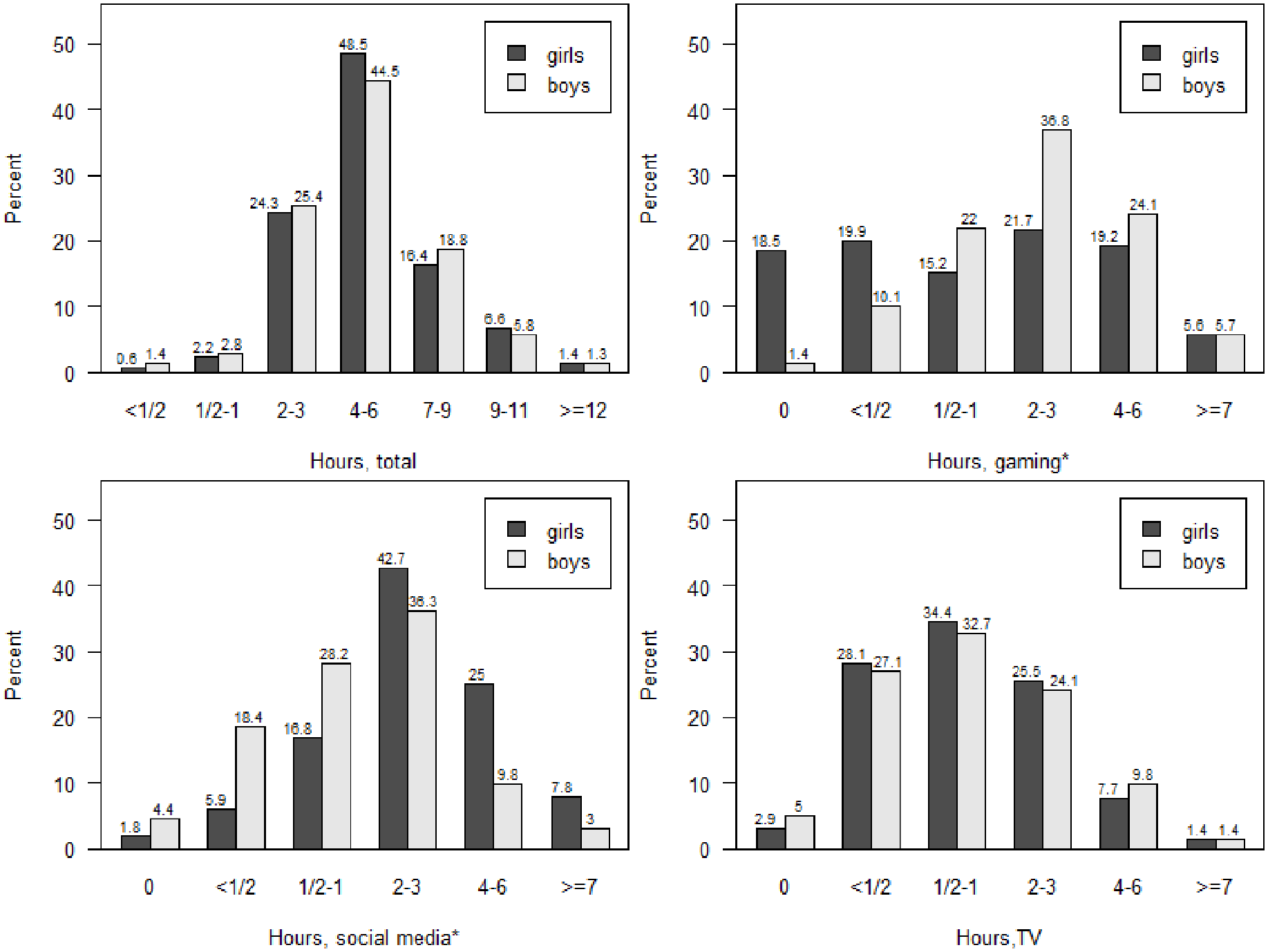
Total screen use and screen time per weekday on different devices for 13-year-old adolescents in Norway, school year 2022/2023 (wave 1) and 2023/2024 (wave 2).
Time spent on gaming and on social media differed according to gender (both p<0.001). Among boys, 66.6% reported spending over two hours gaming per weekday, while the corresponding figure for girls was 46.5% (p<0.001). Girls reported spending more time on social media; 75.5% reported using two hours or more per weekday, compared to 49.1% of the boys (p<0.001) (Figure 2).
The association between health literacy and screen use
In the stratified linear mixed effect models, adjusted for perceived economic status, there were statistically significant relationships between health literacy and all measures of screen use per weekday for girls (Coeff= –.100 – Coeff= –.036, p<.001–p=.002). For details see Table II. For boys, there were statistically significant relationships between health literacy and total screen time per weekday (Coeff= –.036, p < 0.001) and between health literacy and gaming (Coeff= –.044, p<001). The association differed significantly between the genders for all measures, with a stronger association among girls (interaction p =.005–.238), see Table II. Crude and adjusted stratified linear mixed models showed insignificant differences. Crude models are presented in the supplemental material.
Associations between screen time variables per weekday and health literacy of 13-year-old adolescents in Norway, school year 2022/2023 (wave 1) and 2023/2024 (wave 2), adjusted for perceived family economy: linear mixed effect models, including interaction between health literacy and gender (gender difference).
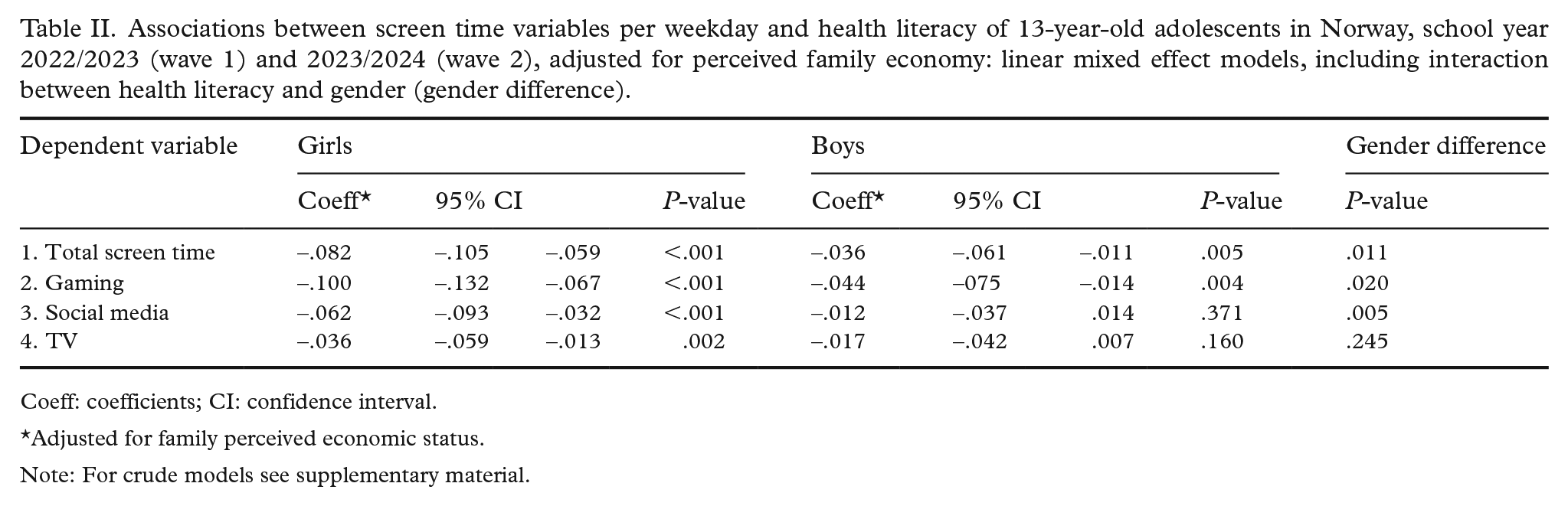
Coeff: coefficients; CI: confidence interval.
Adjusted for family perceived economic status.
Note: For crude models see supplementary material.
The coefficients suggest that total screen time decreases by an average of five minutes for each point increase in the health literacy sum score for girls (–.082×60 ≈ –5) and 2.2 minutes for boys (–.036×60 = −2.2) (see Table II).
Discussion
In the present study, a statistically significant association was identified between health literacy and all types of screen use for girls, and total screen time and gaming for boys. The association was significantly stronger for girls than for boys across all measures. The health literacy mean score was higher for boys than for girls, but the difference was small. In addition, about 25% of both girls and boys reported spending more than seven hours per weekday on screens outside of school hours.
Health literacy among 13-year-old students
Our findings concerning gender differences in health literacy are consistent with previous research, indicating that the differences are small across most countries [5]. Concerning the overall level of health literacy, the participating 13-year-old students in the present study had a slightly lower mean health literacy score (30.12) compared to the European cross-national survey’s findings that focused on 15-year-olds (30.78) [5]. Also, the proportion of students with low health literacy (16%) was higher in the present study than in the European study (13.3%). Nevertheless, prior research suggests that a two-year age difference can significantly influence health literacy levels, with an average increase of 0.47 [5]. Thus, it is reasonable to infer that the 13-year-old students in this Norwegian study have a health literacy score close to the European average.
Health literacy has emerged as a significant independent factor contributing to health disparities [7], and enhancing health literacy among adolescents is a global priority [2]. Previous research shows that students with higher health literacy scores tend to exhibit healthier behaviour than students with lower scores [3]. In the realm of public health, the School Health Service has a mandate to promote health literacy and to reduce disparities in health. The service can play a role in measuring, monitoring, and enhancing health literacy within the school environment in line with the WHO’s health literacy implementation plan for Europe [2]. Assessing students’ health literacy regularly within the School Health Service could serve as an effective way to monitor how well actions are targeted toward improving health literacy. There is some evidence from school nursing in Germany (2020) that the School Health Service has the potential to improve students’ health literacy [27].
Screen use among 13-year-old students
The results of the current study provide updated information about how much time female and male adolescents report spending on screens. This information can help raise awareness of screen use as a crucial health behaviour topic for public services, such as school health services and schools, to address. Consistent with previous research [18], this study showed that only a small percentage of both girls (2.8%) and boys (4.2%) adhere to the screen time guidelines recommended by the WHO [17]. Additionally, a substantial portion of girls (24.4%) and boys (25.9%) reported spending seven hours or more on screens outside of school on weekdays. In line with earlier studies [15, 16], the study identified that girls spent more time on social media while boys were more engaged in gaming. The results underscore a need for effective actions to decrease screen time among adolescents, and knowledge about how differences in preferences in screen use is important when planning strategies to decrease screen time that are tailored to the participants. Reducing sedentary behaviour has long been a global priority and the primary rationale for recommending limits on screen time. However, researchers have increasingly turned their attention to the psychological effects of screen use, highlighting the need to consider not only the quantity but also the type and context of screen engagement [11, 12]. Extensive digital media consumption, particularly among teenagers and especially girls, has been linked to decreased psychological well-being [15].
While there is broad consensus on the importance of addressing excessive screen use, research on effective interventions remains limited. To develop impactful strategies, further exploration is needed into how health-promoting actions can both reduce screen time among adolescents and influence the ways screens are used. Additionally, understanding the complex relationships between screen use and various health outcomes – such as physical health, cognitive abilities, and emotional well-being – is crucial [11]. Schools can serve as an arena where adolescents can practise and discuss how they engage with screens. Themes such as source criticism and digital communication should be included, together with discussions about the physical and psychological consequenses of excessive screen use.
Effective approaches to encourage positive behavioural change that could help reduce overuse of screen media should be examined. Preliminary studies suggest that boosting attitude and self-efficacy among adolescents could serve as an effective strategy to reduce screen time [28]. A systematic review of self-control interventions to reduce media multitasking [29] concludes that there is a general lack of confidence in the results due to limited sample sizes, brief study durations, and unclear study contexts.
Associations between health literacy and screen use
We identified that a high level of health literacy tended to be associated with a small decrease in total screen time and gaming for both girls and boys. Yet, the association between health literacy and screen use was somewhat stronger among girls than boys. Further research is needed to understand the underlying mechanisms behind these differences before implementing tailored strategies.
Health promotion and prevention are complex tasks that require collaboration on an individual and general level involving parents, schools, school health services, and other instances in the municipality. Our findings suggest that increasing health literacy among students might contribute to decreasing screen time. Studies also find that health literacy is associated with other health behaviours like physical activity and sleep, which are also linked to screen use [5]. One suggestion is that the core components of HLSAC (theoretical knowledge, practical knowledge, critical thinking, self-awareness, and citizenship) [29] can be used to address several health behaviours, such as screen time, physical activity, and sleep, at both the individual and general level. To foster healthy screen use, adolescents and their caregivers need to have theoretical and practical knowledge based on recently collected data about screen habits among adolescents and insights about the physical and psychological impacts of screens. Such information provides valuable knowledge for adressing actions together.
Furthermore, research on enhancing self-awareness [29] has shown positive outcomes for addressing students’ perspectives towards digital screen usage, fostering critical thinking. The observed gender difference in type of screen use might be important to consider when addressing attitudes towards screen use, since girls tend to be more active on social media while boys are more occupied with gaming. Still, it is important to look at the statistics and research in detail and not stereotype when discussing screen use. This is supported by a recent study using the Social Media Disorder Scale, which found no gender differences in problematic social media use [19].
Strengths and limitations
A major strength of this study is the relatively large sample size (1425), which enhances the reliability and generalizability of the findings. However, the cross-sectional design used in this study is limited in its ability to establish causation, providing only a snapshot of associations at a single point in time, and cannot establish causal relationships. In this study, we found that improving health literacy may lead to a reduction in screen time. Conversely, decreased screen time may also enhance health literacy, as adolescents who spend less time on screens might be more influenced by other sources that positively affect health literacy. For more robust generalizations, especially when it comes to causal relationships, longitudinal studies or experimental designs would be more reliable.
Self-reported measures of health literacy and screen habits are subject to biases such as recall bias, social desirability bias, and potential misconceptions [30]. The health literacy questionnaire requires accurate understanding, which could lead to misinterpretation among students. However, our analysis demonstrated high internal consistency and confirmed a one-factor model for the instrument (HLSAC), suggesting good reliability. Detailed questions on screen time were asked to encourage accurate reporting of daily routines, but social desirability bias may have led some students to underreport their screen use.This underreporting could potentially strengthen observed associations between health literacy and screen time, as students with higher health literacy may downplay their screen use to align with perceived social norms.
Another limitation was that unmeasured factors that may also influence adolescent screen use, such as parental screen habits, peer influence, and school policies, were not controlled for in this study. While perceived family economic status was included in the linear mixed effect models, the inclusion of additional socioeconomic variables could have further strengthened the study’s robustness.
Despite these limitations, the study provides a valuable foundation for generating further hypotheses and deeper exploration of this important topic.
Conclusions
The present study contributes to the literature by adding screen use to the long list of health behaviours that are associated with health literacy level, together with physical activity, diet, sleep habits, smoking, alcohol and drug use, and other important health parameters. More research is needed to study how health-promoting actions could serve as effective strategies to enhance health literacy and reduce screen time among adolescents, and influence how screens are used.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948251358570 – Supplemental material for Health literacy and screen use among 13-year-old students in Norway – A cross-sectional study
Supplemental material, sj-docx-1-sjp-10.1177_14034948251358570 for Health literacy and screen use among 13-year-old students in Norway – A cross-sectional study by Kristin Sofie Waldum-Grevbo, Solveig Holen and Åse Sagatun in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank all participating adolescents and their parents, as well as collaborating public health nurses and schools, for contributing to the study. We are grateful to the Norwegian Research Council for funding.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by the Norwegian Research Council (grant number 320097).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.