
Abstract
Aim:
Need-based access to health care and social welfare services is an element of health promotion, and it endorses equity and the principles of universalism in society. To explore access to services, this study analyses unmet need for services, barriers that impede access and whether individual characteristics are associated with service access. The study period coincided with the COVID-19-pandemic and health and social services reform in Finland.
Method:
The prevalence of subjective unmet need was used as an indicator of service access. Inconvenient opening hours, a difficult journey to the service unit and high user fees were barriers to receiving services. A nationally representative FinSote survey 2018 and 2020 was used in the analyses. Data were examined with multivariate logistic regression models using SPSS.
Results:
A high prevalence of unmet need for health care and especially for social welfare services was observed. The prevalence of unmet need increased from 2018 to 2020, but in health care only, and access to social welfare services deteriorated. In particular, women, younger people, those who need income support and those with poor health or quality of life forgo care.
Conclusions:
Keywords
Introduction
In the Nordic health and social welfare service model, universalism is a guiding principle for care policies and service provision [1,2]. In this study, the principle of universalism involves equal access to care for equal need, regardless of the socio-demographic characteristics of individuals, area of residence or other factors limiting the use of services. Equal access, in practice, invalidates system- and individual-based barriers to care, and requires the service system to overcome obstacles in seeking services, such as long waiting lists or poor availability of services and lack of economic resources [3]. Equal access is seen as a value as it strengthens equity in health and narrows existing social inequalities in health, leading to a fairer and more inclusive society [4].
Health inequalities are unfair and avoidable differences in health between groups of people, and, despite the aims of health equity and universal care, disparities still exist in Europe [5-7]. Unmet need for services (the difference between services deemed necessary to maintain health and wellbeing and the services received) represents a measure of access to services. Self-assessed unmet need is an indicator of service availability and access [8,9]. It is argued that the concept provides a more reliable estimation of service access in relation to the person’s need compared, for example, with the use of services or a professional’s assessment of a client’s service need. While little is known from the field of social welfare services, research focused on health care has identified some groups with increased likelihood of reporting unmet or forgone need. These include women and younger people [5,10,11], people in poor health [5,11-13] and people with low incomes or with financial distress [5,12-14]. The relationship between education and unmet need has not been systematic [5,10,12]. Barriers to services might relate to structural supply factors (such as long waiting times, distance to care, high user fees), and demand factors, i.e. individual characteristics [15-18]. Unmet need is expected to be especially linked to rural areas due to the reasons above, especially due to spatial limitations and socio-cultural factors [15-17].
Finnish health care and social welfare system
Since the beginning of 2023, 21 wellbeing service counties and the City of Helsinki have been responsible for organizing health care and social welfare services in Finland. The Finnish health-care system consists of three channels: The public service system offers a comprehensive range of services for all residents but has long waiting times and access control. In occupational health care, services are provided by employers for their employees. No user fees are charged. Private health care offers quick access and is an opportunity for those willing and able to pay relatively high user fees. Partial reimbursement is available from the Social Insurance Institution of Finland (KELA). There are regional differences in the provision of private health services. Some private health insurances are used too. Public social services are provided based on special legislation. They are needs assessed by social care authorities. There is some variation between wellbeing services counties in the evaluation criteria and its application, but uniform practices are reinforced by national guidelines. Health care and social welfare services are funded mainly by taxation and involve moderate or no user fees. User fees are regulated through legislation but households’ catastrophic health spending in Finland is relatively high compared with other Nordic countries [19]. For more information on the Finnish health and social welfare service system, see [20,21].
The Finnish service system encountered challenges in the late 2010s. Health and social services reform has been complicated and its implementation has failed several times. It was finally introduced in 2023. The pressure to save in public finances has been very present in the reform preparation. The service-producing environment was shaken by the COVID-19-pandemic: In March 2020 a state of emergency was declared. The range of health and social welfare services narrowed, some closed, and services were altered to emphasize remote access. COVID-19 measures delayed access to services and had negative impacts especially on the most vulnerable groups in society [22-24].
Study questions
During the study period, exceptionally significant changes took place in the service production environment in Finland (the ongoing reform, austerity measures taken in public spending, the COVID-19-pandemic). All of them may have had an impact on service access. It is important to monitor how the universal system achieves its goals when service delivery is under stress. The universal service system should perform well in times of crisis also, offering support to all population groups. The study questions are: (a) What is the prevalence of unmet need for health care and social welfare services in the Finnish population in 2018 and 2020? (b) What is the prevalence of service access barriers? (c) How are socio-demographic characteristics associated with service access? The information is important for health and social care planning and policies aimed at health equity. It is worth noting that the client structure is different in health and social welfare services. The need for health services covers the entire population in Finland, whereas the need for social welfare services is more limited and primarily concerns specific sub-groups or specific stages of life.
Data and methods
The data are from a cross-sectional, sample-based national survey on health, wellbeing and services (FinSote). The nationally representative sample of the FinSote survey consists of the population permanently residing in Finland and aged 20 or over. The sampling method is stratified random. Response loss is corrected using weighting factors which are calculated from the information available for the whole sample: age, gender, marital status, educational attainment, language and urbanity of residence area [25]. The sample included 60,000 people in 2018 and 61,600 in 2020. The number of respondents was 26,422 and 28,199, and the response rate was 45% and 46%, respectively.
Data were collected using a paper questionnaire mailed to respondents; answering the questionnaire online was also possible. Questionnaires were available in Finnish, Swedish, Russian and English. Data were collected between September 2017 and April 2018, and between September 2020 and February 2021. Hereinafter, 2018 and 2020 are used to indicate the time points according to the year in which most of the responses were received. For more information on data collection, see the work of Parikka et al. and Pentala-Nikulainen et al. [26,27]. It should be noted that data collection in 2020 occurred just after the first wave of the COVID-19-pandemic. At that time, some measures were still in effect, and services were in a recovery phase.
Dependent variables
Unmet need for health care was measured by asking: ‘Do you feel you received enough of the following health services in the previous 12 months?’ The services were: (1) doctor’s appointment services; (2) nurse’s appointment services; and (3) dentist services. The answer options were: (1) I didn’t need it; (2) I needed it, but the service wasn’t received; (3) I received it but the service wasn’t sufficient; and (4) I received it and the service was sufficient. A dichotomous variable was computed by combining options 2 and 3 for unmet need and option 4 for met need. When interpreting the results and making comparisons with other studies (e.g. European Union Statistics on Income and Living Conditions), it should be noted that people without a need for the service were excluded from the analysis. The proportion of respondents who indicated they did not need doctor’s appointment services was 25%, nurse’s appointment services 35% and dentist services 41%.
Unmet need for social welfare services was measured by asking: ‘Do you feel you have been adequately provided with the following social welfare services in the past 12 months?’ The services were: (1) treatment and care services provided at home (e.g. home care for the elderly, meal delivery and other support services, rehabilitation services, home alteration work); (2) services for disabled people (e.g. transportation, personal assistance, apartment alteration work); (3) social worker guidance or counselling services; and (4) services for families with children (e.g. child welfare services, parenting and family counselling, home services). The answer options and variable formatting were the same as for health care. The proportion of respondents who indicated they did not need treatment and care services was 93%, services for disabled people 99%, social worker guidance 93% and services for families with children 90%.
Access barriers were measured by asking: ‘Have the following factors interfered with you receiving health care/social welfare services in the past 12 months?’ (1) Opening hours were difficult; (2) the service unit was hard to reach; and (3) high fees made it difficult to receive treatment. The answer options were: (1) always; (2) most of the time; (3) sometimes; and (4) never. Concerning barriers, the analysis was limited to those who had used health or social welfare services. A dichotomous variable was computed by combining options 1–3 for access barriers and option 4 for no access barriers. To describe the prevalence of unmet need, age-standardized gender percentages were calculated for the years 2018 and 2020. Age was standardized by modelling, and p values describing significance were calculated for differences between years using the Wald test.
Independent variables
Disparities in the prevalence of unmet need and access barriers by respondent background were examined in the 2020 data only. The background factors were age, gender, native language, education, labour market status, whether the respondent has had a need for income support, urbanity of residence area and need for services: perceived health in models for health services and quality of life/EUROHIS-8 quality-of-life instrument [28] in models for social welfare services. Variable formatting is described in the Appendix.
The role of independent variables on unmet need and access barriers was examined with logistic multivariate regression models, where unmet need and availability variables were each in turn explanatory variables, and where all independent variables were simultaneously standardized as explanatory variables.
p value (0.05 or lower) and confidence intervals were used to identify statistically significant differences. Analyses were conducted using IBM SPSS Statistics version 27.
Results
The characteristics of the FinSote-2020 study participants are presented in Table I.
Respondents according to their socio-demographic characteristics, FinSote 2020 survey (n = 28,199). As the survey is nationally representative, the weighted proportions presented in the table resemble those in the FinSote 2018 survey data.
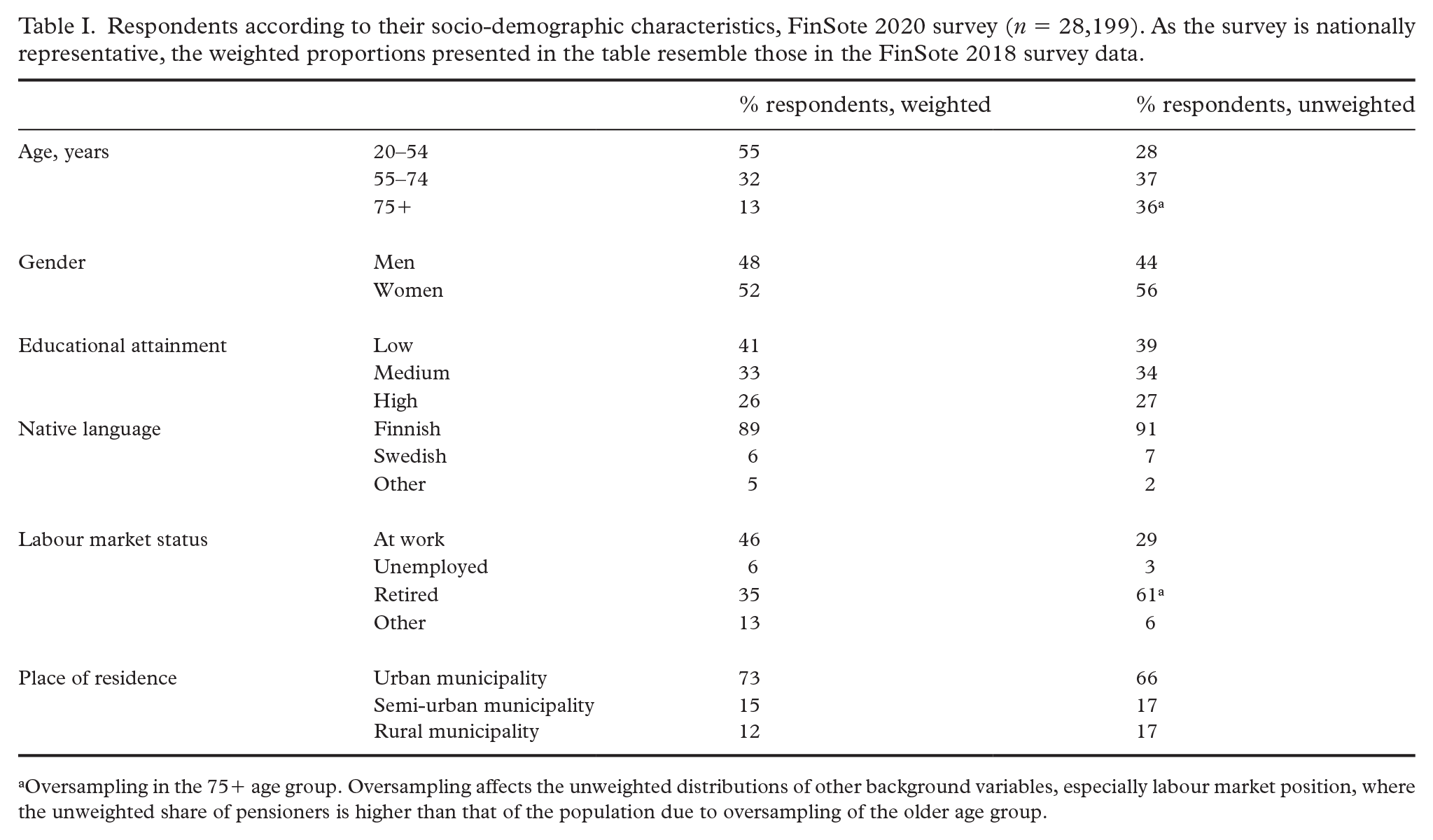
Oversampling in the 75+ age group. Oversampling affects the unweighted distributions of other background variables, especially labour market position, where the unweighted share of pensioners is higher than that of the population due to oversampling of the older age group.
Unmet need for health services was reported more often in 2020 than in 2018. For doctor’s appointment services it was 16% in 2018 and 20% in 2020, and for nurse’s appointment services it was 11% in 2018 and 14% in 2020. For dentist services it was 19% and 24%, respectively (Figure 1).

Percentages of unmet need for health-care services in Finland, FinSote survey 2018 and 2020. Number of respondents is 14,761–21,299 (unweighted).
Younger participants reported unmet need more often than those over 55 (Table II in the Appendix). Women experienced unmet need for doctor’s services more often than men. Native speakers of Swedish or another language experienced unmet need more often than Finnish speakers. Unemployed and retired people reported more often unmet need for doctor’s and nurse’s services than working people. People who have needed income support and those with poor perceived health reported unmet need for health services more often. Finally, those living in urban municipalities reported unmet need more often than those living in rural municipalities, and they also reported unmet need for dentist services more often than those living in semi-urban municipalities for dentist services.
Unmet need for social welfare services was reported in 2020 as often as in 2018. It was almost 40% for home care and more than 40% for services for disabled people (Figure 2). Unmet need for social worker guidance or counselling services was close to 50%, and for services for families with children over 30%.

Percentages of unmet need for social welfare services in Finland, FinSote survey 2018 and 2020. Number of respondents is 590–1590 (unweighted).
Respondents aged 55–74 reported unmet need for care services provided at home more often than people over 75 (Table III in the Appendix). Those with a high educational attainment felt that they did not get services for disabled people more often than those with a low attainment. People in need of income support reported unmet need for home care services, services for disabled people and social worker guidance services more often than those not needing income support. Perceived poor quality of life was related to a higher prevalence of unmet need for social welfare services.
Barriers to receiving health services were less severe in 2020 than in 2018 (Figure 3). While in 2018, one-third of health-care service users reported problems with opening hours; in 2020 the corresponding proportion was 28. The service unit being hard to reach was estimated to hinder access by 28% in 2018 and 25% in 2020. In both 2018 and 2020, around one in five reported that high user fees interfered with access to services.
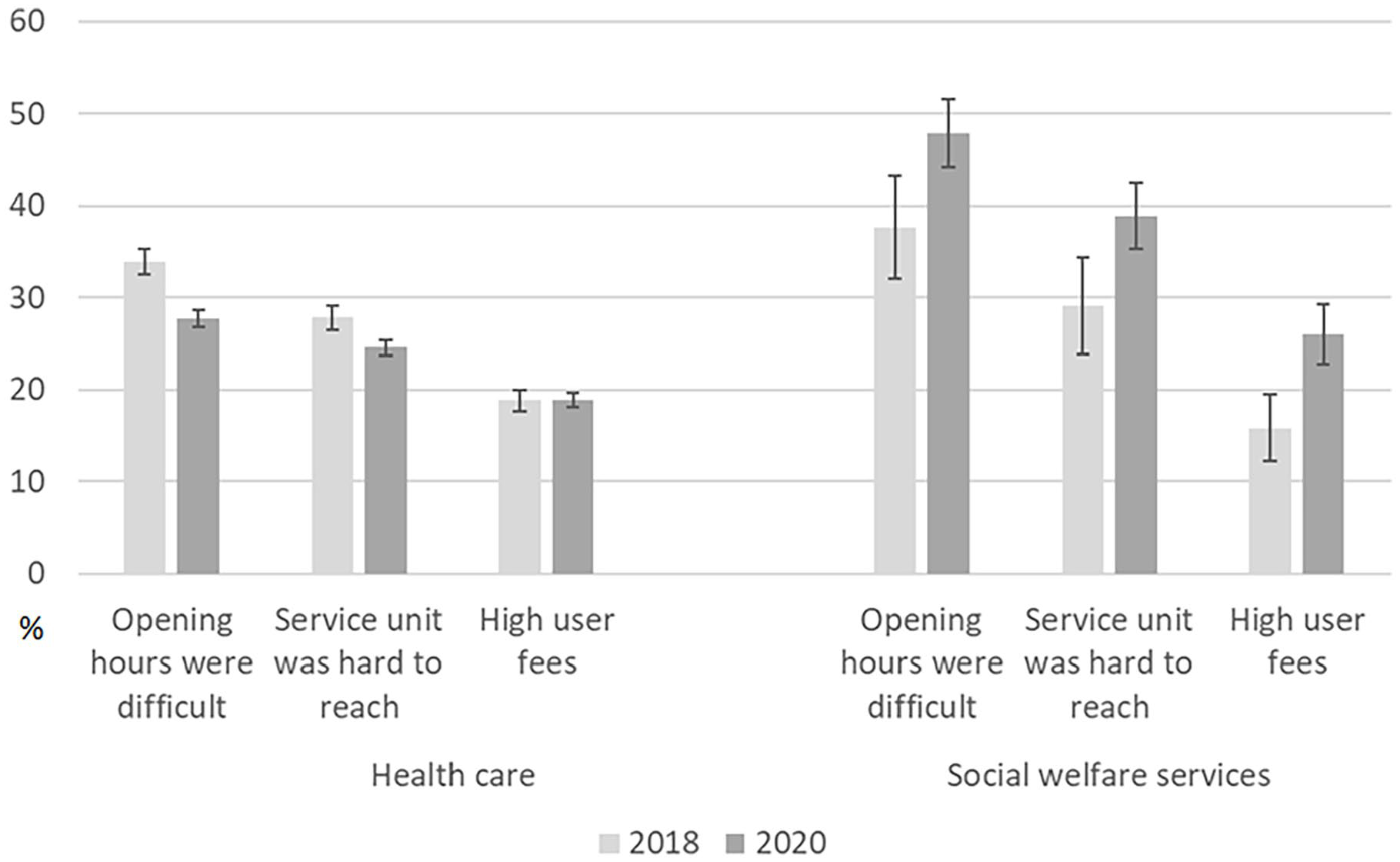
Prevalence of barriers to receiving health care and social welfare services in Finland, FinSote survey 2018 and 2020. Number of respondents is 1273–18,146 and 1426–20,483 respectively (unweighted).
Those under 55 reported problems with opening hours more often than those aged 55–74, and problems with high user fees more often than the oldest age group (Table IV in the Appendix). Women experienced barriers to receiving health services more often than men. Those with low educational attainment, the unemployed and pensioners reported problems related to high user fees more often than their comparison groups. Those who have needed income support and those with poor perceived health reported all problems with health services more often than others. Those living in semi-urban and rural municipalities reported problems with opening hours and that the service unit was hard to reach more often than urban dwellers.
Problems receiving social welfare services were more commonly reported in 2020 than in 2018 (Figure 3). In 2018, 38% of users of social welfare services reported problems with opening hours, 29% stated that service unit care was difficult to access, and 16% had problems with high user fees. In 2020, the corresponding proportions were 10 percentage points higher.
People over 75 reported access problems more often than those under 55. Those aged 55–74 reported problems caused by user fees more commonly than those under 55 (Table V in the Appendix). People who have needed income support and those who felt their quality of life to be poor reported nearly all access problems more often than others.
Discussion
The results indicate that a considerable proportion of the Finnish population faces unmet need for essential services, referring to the weakness of the service system (which aims to be universal) regarding overcoming barriers to access. Perceived unmet need increased in health care from 2018 to 2020. One plausible reason is the COVID-19 measures, which negatively affected access to services [22,23]. Another possible explanation could be the health and social services reform. The last proposal failed in 2019 and the delay of the reform may have suspended the development of services, leading to access problems. No change in unmet need was detected regarding social welfare services. This is somewhat surprising because the supply of social welfare services was significantly reduced due to the pandemic, and COVID-19 measures particularly affected the lives of the most vulnerable in society (presumably the clients of social welfare services) [23]. Behind this could be that relatives and third-sector actors replaced discontinued formal care and took over responsibility for taking care of everyday needs, especially for the elderly [29,30].
In keeping with previous research, perceived unmet need was associated with socio-demographic characteristics in contrast to health promotion and equity. Women and young people were more susceptible to unmet need compared with older people, the unemployed, those with economic difficulties and those with poor perceived health/quality of life. The explanation may be that these groups have more care needs than others and greater use of services makes people aware of shortcomings in receiving them [31]. Furthermore, navigating the service system (finding a suitable service, booking an appointment, long waiting lists) can be a complicated task, especially for those with scarce resources. The cost of care may have an effect too: High user fees and travel costs could make it difficult for economically weaker groups to obtain the care they need [8,19,32]. A special challenge in Finnish health care is inequality in access to primary care. The working population largely receives primary care through occupational health care, with easy access and no user fees; private services are an option for those who can afford it and are willing to pay user fees. The unemployed, students and older people are dependent on public primary care, where waiting times are long and user fees common. It seems that the Finnish system lacks true universalism where all population groups have equal access to care services.
Among those who used health services, barriers were less severe in 2020 than in 2018. This may be partly explained by the increased supply of e-services. Digitalization has progressed in Finland, especially in health care, and the COVID-19-pandemic accelerated the development and the use of e-services. However, not everyone benefits from digitalization, and particularly vulnerable groups are at risk of digital exclusion [33]. In contrast to health care, barriers to receiving social welfare services were more evident in 2020 than in 2018. Among users of social welfare services, the worse off, in particular, seem to have access problems, indicating a risk that health inequalities will continue to grow. Better access to health care has been emphasized in the reform of services, and the role of social care in the implementation of the reform has been sidelined; COVID-19 measures probably made the situation even worse. It seems social services did not perform adequately in supporting vulnerable groups in society during the pandemic. The results here show problems regarding receiving social welfare services are substantial, and resources must be allocated urgently to facilitate access and thus improve health promotion and ensure equity goals.
Accessibility-related barriers to reaching health services were more common among rural and semi-urban residents than among urban residents, as expected [16]. In Finland, the long, ongoing trend towards service centralization has increased distances to service units, which has been compensated by e-services and ‘on the wheels’ services. However, internet use in general, and satisfaction with the function of communication connections, is lower in sparsely populated areas [34], which reduces the full use of e-services. Despite this, residents of rural municipalities did not report higher level of unmet need. Accessibility problems are experienced, but it seems that rural residents accept restrictions related to their place of residence and have adapted to problems. In fact, a higher level of unmet need was linked to urban municipalities. The COVID-19-pandemic might be part of the explanation: the pandemic affected densely populated areas more. In Finland, minimization and management of service debt has been at least partially less successful in large cities than in smaller and medium-sized cities and organizations [33].
Finally, Swedish speakers and those who were not native speakers of Finnish or Swedish experienced greater unmet need for health services. It is known that immigrants are less satisfied with health care and find it less accessible than non-migrants. This disparity might be attributable to cultural and communication issues [35]. Swedish speakers typically also speak Finnish. Despite bilingualism, it is possible that care in Finnish hampers communication with health-care providers and does not fully meet the service need [36].
Limitations
The results should be interpreted keeping the concept of unmet-need subjectivity in mind; it is not an objective measure. Also, barriers were studied at a general level only, not focused on one service type, and only among those who have used the service. The inability to include background variables in the 2018 survey analyses can be viewed as a limitation, since potential time-related changes in social inequalities regarding access to services could not be explored. Here, a relatively large sample size enables to focus on social welfare services despite the small share of service users in the population. A part of those services is targeted at the most vulnerable people in society. This group is presumably under-represented in the survey. It is possible that non-respondents have different experiences and probably more difficulties than average regarding accessing services. Some language groups were left out of the study because only four language versions of the questionnaire were available: Finnish, Swedish, English and Russian (93% of the Finnish population speak one of these languages as their native language [37]).
Conclusions
A considerable share of the Finnish population faces unmet need and barriers to accessing health and social welfare services despite the principles of universalism, health equity and health promotion. The high rate of unmet need for social welfare services, as well as considerable problems regarding access to them, are of particular concern. COVID-19 measures presumably increased unmet need during the study period, indicating that the service system partly failed regarding its performance at the time of the crisis. Policies and service development must continue to facilitate access to essential services and reduce socio-demographic inequities, particularly addressing groups vulnerable to forgone care. We also suggest that needs-based access to essential services should be discussed more often in the context of universalism and equal opportunities for all.
Footnotes
Appendix
Acknowledgements
The authors would like to thank statistician Jonna Ikonen for helping with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FORTE (grant number: 2022-01357) and the Swedish Research Council for Sport Science (grant number: 2020/3, P2021-0065).
Ethics approval
The FinSote study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the Coordinating Ethics Committee of the Finnish Institute for Health and Welfare in 2017 (approval number THL/637/6.02.01/2017).