
Abstract
Aim:
This study aimed to investigate awareness of having hypertension, diabetes and dyslipidaemia and their associated factors among US adults.
Methods:
Data from the National Health and Nutrition Examination Survey, including 21,399 adults aged ⩾20 years (pregnant women excluded) collected between 2011 and 2018, were used. Blood pressure was measured using a Baumanometer calibrated mercury true gravity wall model sphygmomanometer. Serum total cholesterol levels were measured using enzymatic assays. The percentage of haemoglobin A1C (HbA1c), which reflects long-term blood glucose levels, was measured and used to identify diabetes. Participants self-reported whether they were told by a doctor that they have hypertension, dyslipidaemia and diabetes. Awareness was defined as alignment between objective and self-reported measures for having the conditions. Sampling weights and the Taylor series linearisation variance estimation method were used in the analyses.
Results:
The findings showed that 64.06% of people with hypertension, 54.71% of those with dyslipidaemia and 78.40% of those with diabetes were aware of having the respective condition. Age, sex and health insurance were associated with awareness of having all three conditions, but marital status was not associated with any outcome. Weight status was associated with awareness of having hypertension and dyslipidaemia, whereas ethnicity was associated with awareness of having hypertension and diabetes. Relative family income was only associated with awareness of having hypertension.
Conclusions:
Introduction
Hypertension, diabetes and dyslipidaemia globally ranked among the top 10 leading risk factors of deaths in 2017 [1]. In 2015–2018, about 122 million US adults aged 20 years and older had hypertension (systolic blood pressure (SBP) ⩾130 mmHg or diastolic blood pressure (DBP) ⩾80 mmHg), 94 million had total cholesterol levels ⩾200 mg/dL and about 28 million had diabetes [2].
Given the effect of these conditions on health, early detection can improve treatment and minimise complications. However, these conditions often show no symptoms, and regular check-ups are needed to detect them. It is recommended that healthy adults participate in screening for hypertension and diabetes every three years [3,4] and for dyslipidaemia every four to six years [5]. The screening frequency should be higher for those with increased risks (e.g. family history) [5].
Studies have indicated that many adults are unaware of having these conditions. Globally, it was estimated by Saeedi et al. that about 50% of 463 million adults with diabetes [6] and by the World Health Organisation that 46% with hypertension [7] are unaware of their conditions. Separate surveys have also shown the percentages of people aged 40–79 years with undiagnosed dyslipidaemia were about 78% in Thailand; between 40% and 60% in Germany, England, Jordan, Canada and Scotland; and less than 25% in Japan and Mexico [8,9].
In the USA, several studies examining awareness of having hypertension, diabetes and dyslipidaemia were conducted using National Health and Nutrition Examination Survey (NHANES) data. One study using NHANES data for 1999–2004 found that 75.9% people aged 65 years and older were aware of having hypertension, 65.7% were aware of having dyslipidaemia and 71.4% were aware of having diabetes [10]. Another study using NHANES data for 2011–2014 found that the prevalence of awareness among people aged 18–39 years was 62.7% for hypertension, 56.9% for dyslipidaemia and 70.0% for diabetes [11]. NHANES data for 2005–2016 showed that among adults aged 18–44 years, awareness was between 68.7% and 77.7% for hypertension, 46.8% and 54.1% for dyslipidaemia and 61.1% and 74.1% for diabetes [12]. These studies focused on younger (<45 years of age) or older adults (⩾65 years of age). To our knowledge, there have been two NHANES studies that included adults aged 20 years and older, but they only examined hypertension [13,14]. As these conditions often develop during middle age, early awareness may motivate early lifestyle changes and other interventions necessary to prevent severe complications.
This study used the most recent NHANES data (2011–2018) to examine awareness of having hypertension, dyslipidaemia and diabetes and their associated factors among US adults with the conditions. The findings of this study offer insights that could guide intervention strategies, potentially improving awareness and thus facilitating early detection of these chronic conditions in the community.
Methods
Data source
NHANES is a continuous survey conducted by the National Center for Health Statistics (NCHS) to assess the health and nutrition status of the US non-institutionalised population [15]. It uses a complex four-stage probability sampling method to select 5000 participants per year in 15 counties across the USA. This study only used adult data (i.e. participants ⩾20 years of age) collected between 2011 and 2018. The reason for this timeframe is due to changes over time in methodology for some laboratory measures and sample design. Approval for the NHANES was obtained from the NCHS Research Ethics Review Board (protocol #2011-2017). Informed consent was obtained from all participants.
Of the 37,017 screened adults, 21,646 (58.5%) were interviewed and examined. The examination response rates were 64.5% in 2011–2012, 63.7% in 2013–2014, 58.1% in 2015–2016 and 49.8% in 2017–2018 [16]. Pregnant women (n=247) were excluded from the analysis.
Measures
All variables primarily measured with details on how they were measured, including laboratory procedures, can be found elsewhere [15]. A summary of this information is provided below.
Demographic characteristics
Age, sex, marital status, ethnicity, education level, family income and health insurance status were self-reported. A ratio of family income to the poverty guidelines specific to the survey year, family size and geographic location was calculated, and if <1, family income was classed as being below the poverty line. This poverty/income ratio was categorised with cut-off points of 0–1.3 for ‘low,’ >1.3–3.5 for ‘middle’ and >3.5–5 for ‘high’ relative family income [17]. Participants were considered to have health insurance if they were covered by any plan obtained through employment or government programmes.
Participants’ height and weight were measured in the mobile examination centre by trained staff. Body mass index (BMI) was calculated by dividing the weight in kilograms by the height in metres squared. Those with a BMI <25 kg/m2 was classified as healthy/underweight, and those with a BMI ⩾25 kg/m2 were classified as overweight/obese.
Awareness
During the visit to the mobile examination centre, certified examiners measured participants’ blood pressure using a Baumanometer calibrated mercury true gravity wall model sphygmomanometer. Participants were seated at rest for at least five minutes. An appropriate cuff size was selected. Three SBP and DBP measurements were taken 30 seconds apart. A fourth measure was obtained if the previous measurement was interrupted. Participants were excluded if both arms had rashes, open sores, wounds or other conditions, or if the cuff didn’t fit properly. Blood pressure readings were averaged (for those with only one reading, that reading was used) and used to identify hypertension [18]. Participants with a SBP of ⩾130 mmHg or a DBP of ⩾80 mmHg or those on antihypertensive medication were considered to have hypertension [19]. Awareness of having hypertension was defined as those with hypertension and self-reporting ‘yes’ to the question ‘Have you ever been told by a doctor or other health professional that you had hypertension, also called high blood pressure?’
Serum total cholesterol levels were measured using enzymatic assays. A total cholesterol level of <200 mg/dL was considered healthy for adults [2]. Therefore, those with a total cholesterol level of ⩾200 mg/dL or those on anti-dyslipidaemia medication and answering affirmatively to the question ‘Have you ever been told by a doctor or other health professional that your blood cholesterol level was high?’ were classified as being aware of having dyslipidaemia.
The percentage of haemoglobin A1C (HbA1c), which reflects long-term blood glucose levels, was measured and used to identify diabetes. Participants with a HbA1c ⩾6.5% [4], taking insulin or diabetic pills and answering affirmatively to the question ‘Other than during pregnancy, have you been told by a doctor or health professional that you have diabetes or sugar diabetes?’ were considered as being aware of having diabetes.
Data analysis
SAS v9.4 (SAS Institute, Cary, NC) was used for analyses. Following the guideline, eight-year examination sampling weights were recalculated by dividing the two-year weights by four. Missing values were 9.9% (n=2120) for poverty/income ratio, 2.8% (n=588) for awareness of having hypertension, 4.8% (n=1033) for awareness of having dyslipidaemia, 4.1% (n=884) for awareness of having diabetes, 1.4% (n=306) for BMI and <0.2% for other demographic variables. Missing data were excluded in the analyses. Survey procedures in SAS were used to account for the complex survey design. The Taylor series linearisation variance estimation method was used for all analyses.
Weighted percentages and standard errors were reported for demographic characteristics, hypertension, diabetes and dyslipidaemia in the general population. Additionally, weighted percentages and standard errors of awareness of having each condition among those with the condition were presented by demographic groups. PROC SURVEYLOGISTIC was used to identify associations between demographic characteristics and the outcomes (i.e. awareness of having the condition). Model 1, including one of the demographic characteristics adjusting for survey cycles, was run for each outcome. As health insurance and relative family income were highly correlated, two multivariable models which included survey cycle, age group, sex, marital status, ethnicity, education level, weight status and either health insurance (model 2) or relative family income (model 3) were separately conducted for each outcome. Scheffe’s method was used to adjust for multiple comparisons for variables with more than two categories. Additionally, as the definition of hypertension was inconsistent over time, a sensitivity analysis was conducted for hypertension using the definition of SBP ⩾140 mmHg or DBP ⩾90 mmHg. Odds ratios were reported with 95% confidence intervals. p-Values were two-sided and were considered significant if <0.05.
Results
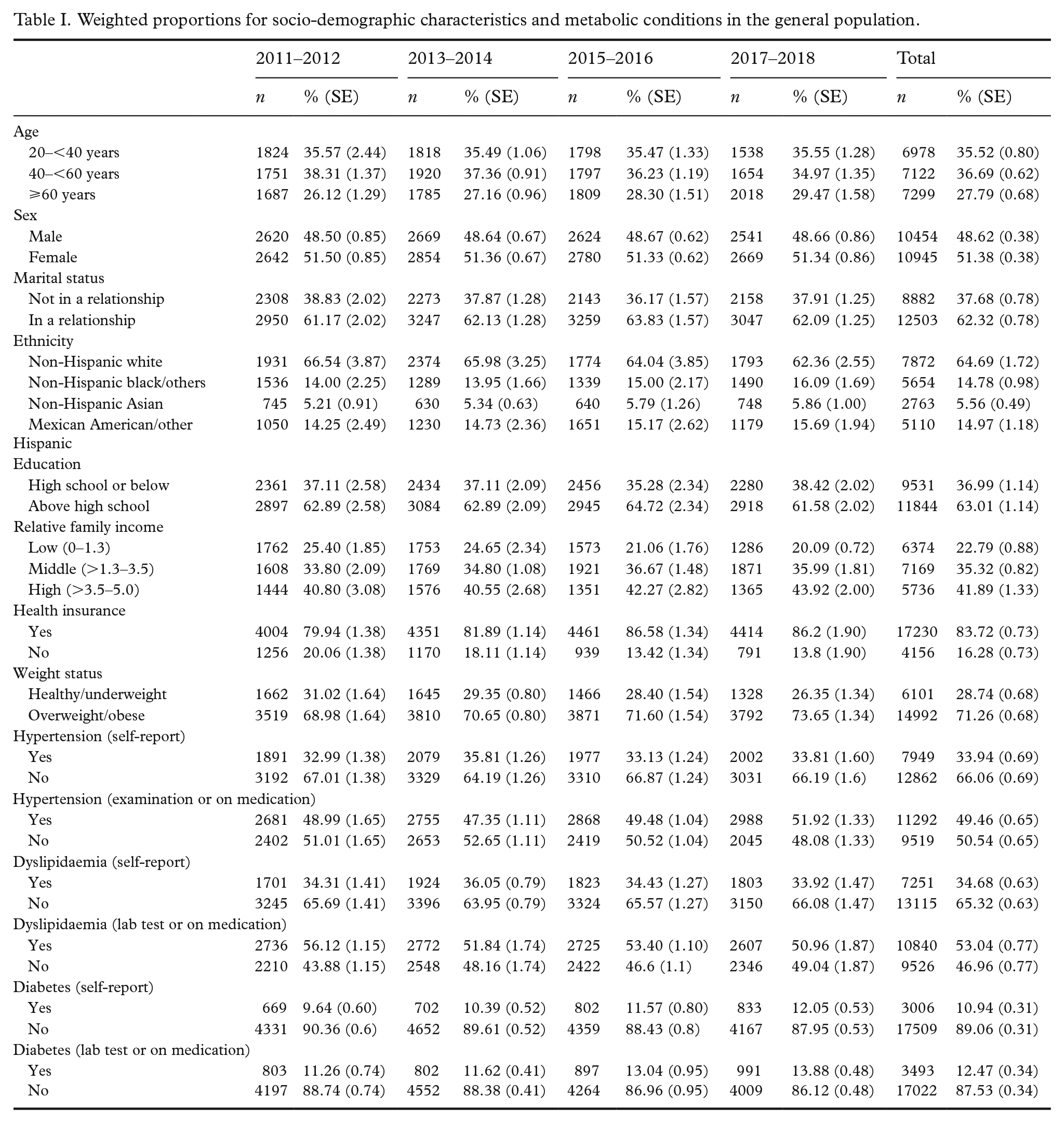
Table I shows weighted percentages for socio-demographic characteristics, hypertension, diabetes and dyslipidaemia, as well as awareness of having these conditions in the general population. About one third self-reported as having hypertension (33.94%) and dyslipidaemia (34.68%), and more than one tenth self-reported as having diabetes (10.94%). At the examination, about half (including those on medication) were identified as having hypertension (49.46%) and dyslipidaemia (53.04%), and about one tenth were identified as having diabetes (12.47%).
Weighted proportions for socio-demographic characteristics and metabolic conditions in the general population.
Among adults with hypertension, about 64% (n=7506) were aware of having the condition (Table II), while 36% (n=3786) were unaware. The weighted percentages were about 54% and 78% for awareness of having dyslipidaemia and diabetes, respectively. Across the demographic characteristics, the percentages ranged between 41.28% and 76.32% for awareness of having hypertension, 24.71% and 69.70% for awareness of having dyslipidaemia, and 62.17% and 82.96% for awareness of having diabetes.
Weighted percentages for awareness of having hypertension, dyslipidaemia and diabetes by socio-demographic characteristics among those with the conditions.
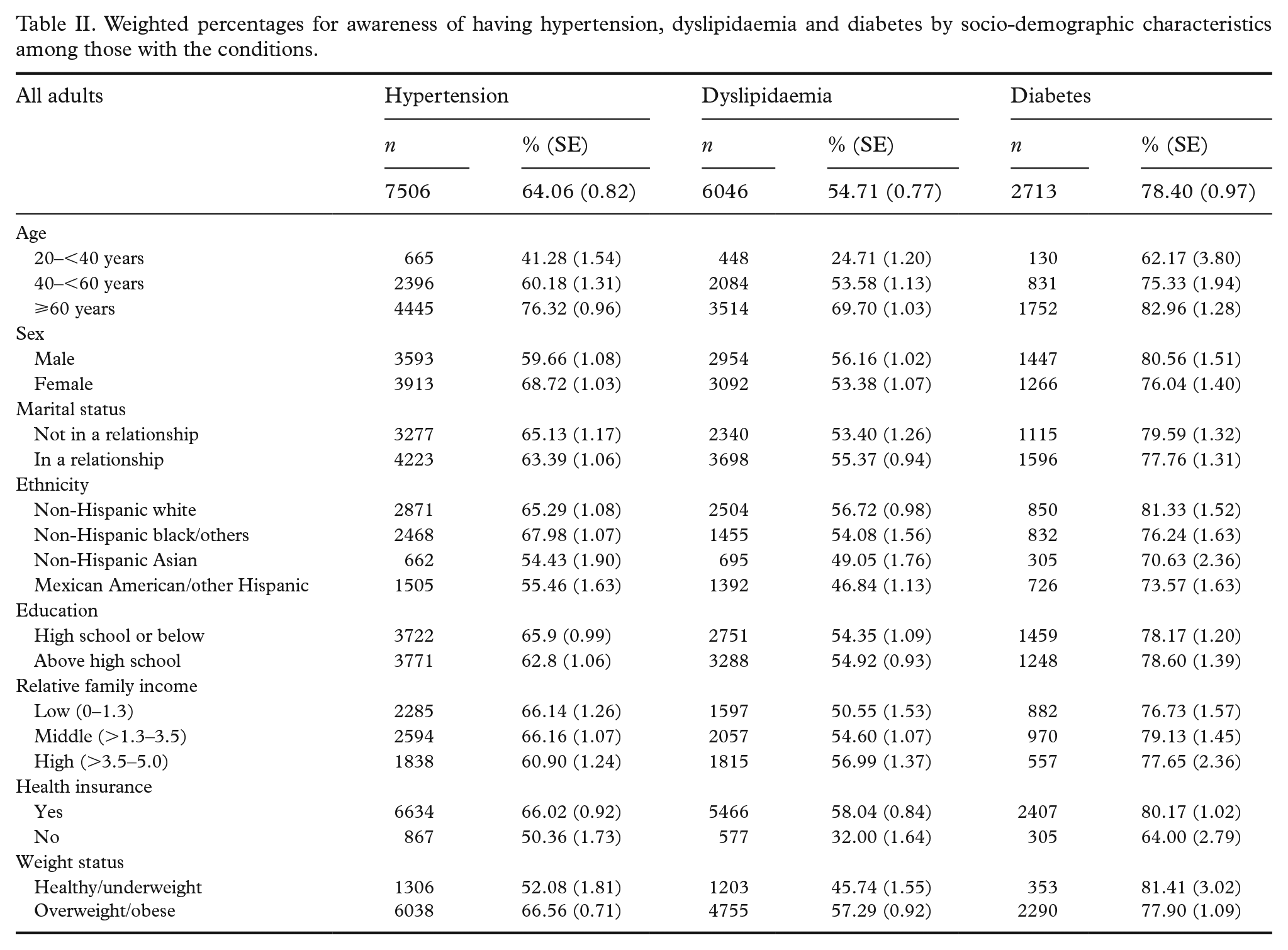
Table III shows the associations between awareness among people with the conditions and demographic characteristics. Across the models, people aged 60 years and older were more likely to be aware of having hypertension, dyslipidaemia and diabetes compared to those aged between 20 and 40 years (p<0.001). The odds of awareness among those aged 40–60 years were about twice (hypertension), three times (dyslipidaemia) and 1.6 times (diabetes) higher than among those aged 20–40 years. People with health insurance were also more likely to be aware of having the conditions (p<0.001). Although sex was a significant factor associated with awareness of having these conditions, the direction of association was inconsistent across the conditions. Men were less likely to be aware of having hypertension (p<0.001) but more likely to be aware of having dyslipidaemia (p<0.001) and diabetes (p<0.05) than women were. Marital status was not associated with awareness of having any condition. While overweight/obese adults were more likely to be aware of having hypertension and dyslipidaemia (p<0.001), the association was not significant regarding awareness of having diabetes. Relative family income was not associated with awareness of having dyslipidaemia and diabetes. However, adults with a high relative family income were less likely to be aware of having hypertension than those with a low income. While Hispanic adults were less likely to be aware of having hypertension, Asians were less likely to be aware of having diabetes than non-Hispanic white participants. The sensitivity analysis for hypertension with the cut-off of 140/90 mmHg shows similar results for all three models (Supplemental Table SI).
Associations between awareness among people with the conditions and demographic characteristics (odds ratios and 95% confidence intervals).
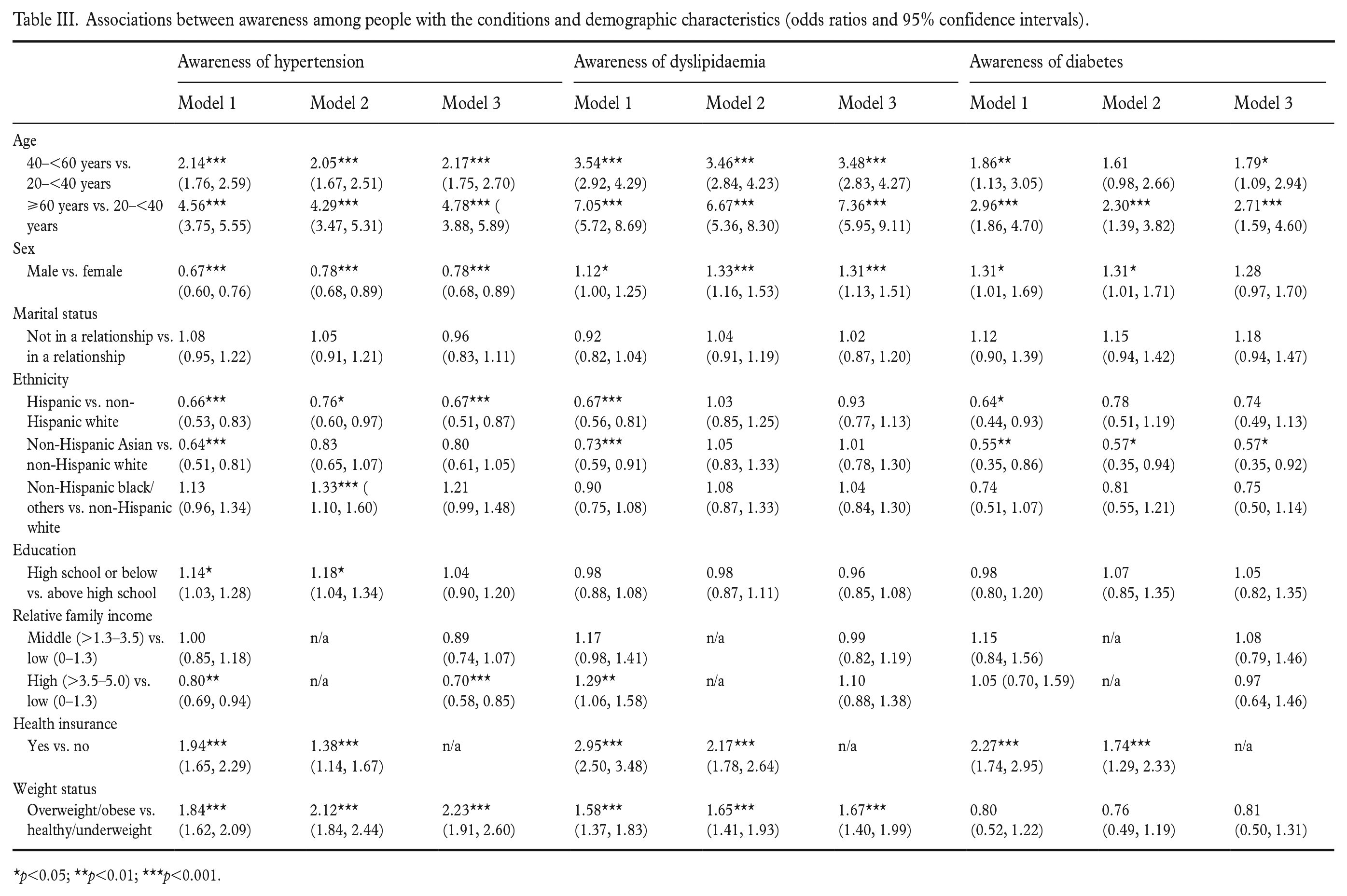
p<0.05; **p<0.01; ***p<0.001.
Discussion
Our findings showed that about one third of people with hypertension, half of those with dyslipidaemia and a quarter of those with diabetes were unaware of having the condition. While awareness of having hypertension in this study was less than that globally (36% vs. 46%), it was comparable to those in other high-income countries (33%) [20]. However, unawareness of having diabetes among US adults with the condition (about 23%) was lower compared to a global estimate of 50% and those in Europe (40.7%), North America and the Caribbean (37.8%) [6]. Although a global estimate of unawareness for dyslipidaemia was not found, studies found that the percentage of unawareness of dyslipidaemia was higher in Canada (57%) [9] and Italy (56%) [21] than in this study (45%). However, it is worth noting that comparisons on awareness of having hypertension, dyslipidaemia and diabetes across studies are relative, as criteria used in defining the conditions (e.g. HbA1C was used in identifying diabetes rather than other glucose tests) and sample characteristics were often different.
Across the three conditions, younger adults were less likely to be aware of having the conditions. This finding is consistent with studies in Canada showing that awareness of having dyslipidaemia [9] and in Malaysia showing that awareness of having hypertension, dyslipidaemia and diabetes increased with age [22]. An explanation may be that young adults were less likely to visit general practitioners and were therefore less likely to be examined for hypertension [23]. Given the low prevalence of these conditions in young adults, cost-effective methods need to be developed to identify at-risk people early so that lifestyle modification programmes and treatment can be implemented in a timely manner to minimise risks of developing cardiovascular diseases later in life.
Previous studies have found that men in Sweden [24], Sardinia (Italy) [25] and Mayotte (France) [26] were less aware of hypertension than women. However, no sex difference in awareness of dyslipidaemia and diabetes was found in the Sardinian study [25] and in Canadian adults [9]. Although our finding showed that men were less aware of hypertension, they were more aware of dyslipidaemia and diabetes than women were. One explanation may be due to differences in the screening recommendations in the USA for hypertension and dyslipidaemia. While the recommendation at the time for screening hypertension was the same for men and women (⩾18 years old), screening for lipid disorders was recommended for younger men (i.e. ⩾35 years old) compared to 45 years and older for women, and therefore men with the condition may be diagnosed earlier. However, the sex differences in percentages of awareness of having dyslipidaemia and diabetes were small (<5%).
Although weight status was associated with hypertension and dyslipidaemia, this was not the case for diabetes. This finding is consistent with the findings from a Swedish study that overweight/obese people were more aware of hypertension [24], whereas no association between weight status and awareness of hypertension was found in the Mayotte study [26]. Studies in Malaysia [22] and Singapore [27] also found that obese people were more likely to be aware of hypertension and dyslipidaemia. While our finding that weight status was not associated with diabetes is consistent with that from the Malaysian study [22], a Singaporean study found a reverse association that obesity was associated with greater unawareness [27]. This is interesting because it would be expected that overweight/obese people would be more likely to be screened for these conditions. As there was a lack of studies examining these associations, including those in high-income countries, it is difficult to reach a firm conclusion.
Having health insurance was associated with a higher awareness across the three conditions. This is to be expected, as health insurance was found to reduce medical costs and increase access to care and utilisation, resulting in increased rates of diagnosing and treating chronic conditions [28]. Another study in China found similar results, although the health-care system in China may be different from that in the USA [29]. Given that many Americans (11%; 29.6 million) had no health insurance in 2021 [30], attention to identify and provide treatment to the uninsured is needed to prevent higher costs imposed on the system later on due to the development of severe complications and cardiovascular diseases.
Consistent with studies in Sweden [24], France [26] and Malaysia [22], marital status was not associated with awareness of having hypertension, dyslipidaemia and diabetes in this study. While relative family income was not associated with awareness of having dyslipidaemia and diabetes, differences were found in some post-hoc comparisons for awareness of having hypertension. In particular, adults with a high relative family income were less likely to be aware of having hypertension than those with a low relative family income. While the reason is unclear, we speculate that people with a higher relative family income were likely to obtain an early diagnosis and treatment of hypertension and thus were able to control it [31]. In contrast, those with hypertension despite being wealthy may be too busy and pay insufficient attention to their blood pressure and therefore are unaware of it.
Moreover, this study found that Hispanic Americans were less likely to be aware of hypertension and non-Hispanic Asians were less likely to be aware of diabetes compared to non-Hispanic white participants. A reason for the difference between Hispanic Americans and non-Hispanic white participants may be due to the use of home devices to self-monitor blood pressure, which was lower among Hispanic Americans than non-Hispanic white participants (81.4% vs. 76.1%) [32]. For the difference between non-Hispanic Asians and non-Hispanic white participants, one explanation could be due to cultural pressure and social stigmas against Asian patients which discouraged them from disclosing their condition [33,34]. Another reason may be because Asians were likely to have worse access to care and be more hesitant to seek health care than white participants [35]. Although the associations were independent of socio-demographic factors (e.g. family relative income and education), there may be other social determinants of health which contributed to the ethnic differences. Identifying these factors may be of significant interest, as the information would help in the design of more targeted interventions to improve people’s awareness.
This study used nationally representative data from one of the highest-quality surveys in the USA. The large sample from multiple survey cycles improves the precision of estimates. Diagnosis of the conditions was based on the standard clinical measurements. However, there are limitations. First, the results may not be generalisable to other populations, especially those in low- and middle-income countries and with different health-care systems. Second, self-report of having the metabolic conditions was used to define awareness and thus was subject to recall and social desirability bias (i.e. some people may be reluctant to report their condition, as they are afraid of being judged by others). Third, HbA1C was used as a single criterion for diagnosing diabetes, whereas it is more typical to use multiple tests in clinical practice. The decision to use HbA1C was because (a) plasma fasting glucose and oral glucose tolerance test were only conducted for the morning section sample (half of the full sample), (b) these tests were not available for all survey cycles and (c) HbA1C better captures chronic hyperglycaemia which is more appropriate for studies on awareness that needs time to develop. Finally, types of diabetes were not identified, and including type 1 diabetes may overestimate awareness of diabetes. As type 1 diabetes usually occurs in young ages and requires insulin treatment, people with type 1 diabetes are likely already aware of their condition.
Conclusions
Prevalence of hypertension, dyslipidaemia and diabetes was high among US adults, with large proportions being unaware of having hypertension, dyslipidaemia and diabetes. Age, sex and health insurance were associated with all three outcomes. Weight status was associated with awareness of having hypertension and dyslipidaemia, whereas ethnicity was associated with awareness of having hypertension and diabetes. Relative family income was only associated with awareness of having hypertension.
These findings inform policymakers and revision of guidelines for screening recommendations. The information can also be used to develop interventions targeting groups at higher risk of unawareness. Policies and actions are necessary to improve health literacy among US adults. Future research examining differences in direction of associations between sex and awareness of hypertension, dyslipidaemia and diabetes as well as on associations between ethnicity, education and income are needed.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948241247612 – Supplemental material for Awareness of having hypertension, diabetes and dyslipidaemia among US adults: The 2011–2018 NHANES data
Supplemental material, sj-docx-1-sjp-10.1177_14034948241247612 for Awareness of having hypertension, diabetes and dyslipidaemia among US adults: The 2011–2018 NHANES data by Kien G. To, Corneel Vandelanotte, Anh N.V. Huynh, Stephanie Schoeppe, Stephanie Alley, Aamir Raoof Memon, Nhung T.Q. Nguyen and Quyen G. To in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.V. is supported by an ARC Future Fellowship (ID FT210100234), NHMRC Ideas Grant (ID 2012704), and NHF Vanguard Grant (ID 105816); S.A. by a fellowship from the National Heart Foundation of Australia (ID 102609); and S.S. by a fellowship from the National Health and Medical Research Council (ID 1125586).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.