
Abstract
Aims:
This study examined the incidence of attention-deficit/hyperactivity disorder medication among children and adolescents by sex and age group in Finland during 2008–2019.
Methods:
The data on children and adolescents aged 6–18 years receiving reimbursement for any attention-deficit/hyperactivity disorder medication was collected from the nationwide register on reimbursed purchases. The incidence was calculated as a ratio of the number of new users and the number of age and sex-matched population at risk. Negative binomial models were used to calculate rate ratios (RRs).
Results:
In 2019, the incidence of attention-deficit/hyperactivity disorder medication was 13.4 per 1000 boys and 4.8 per 1000 girls. Among boys, the incidence became 3.7 times greater during the observed years (RR 95% confidence interval (CI) 2.0, 6.5, P<0.0001), whereas in girls it was 7.6 times greater (RR 95% CI 2.1, 27.4, P=0.0019). The boys had 2.8 times the incidence rate compared with the girls (RR 95% CI 2.2, 3.6, P<0.0001). The increase was associated with age only among boys (P=0.0001). The highest incidence rate 23.4 per 1000 individuals (95% CI 22.5, 24.4) was found in 2019 among 6–8-year-old boys.
Conclusions:
The incidence of attention-deficit/hyperactivity disorder medication use among children and adolescents increased significantly in Finland during the study period. Incidence was higher among boys, but the increase was greater among girls. The most common group to start attention-deficit/hyperactivity disorder medication was 6–8-year-old boys. These findings warrant critical evaluation of the diagnostic and treatment policies currently available in Finland for the treatment of attention-deficit/hyperactivity disorder and related symptoms.
Keywords
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder typically diagnosed in childhood. It affects around 2.9–7.2% of school aged children and adolescents globally [1, 2].
Since 2007 the Finnish clinical guideline for the treatment of ADHD has recommended medication for children aged 6 years and over if their ADHD symptoms are causing persistent significant impairment and other psychosocial interventions are considered insufficient [3].
In recent years, the prevalence of ADHD medication among children and adolescents has increased in several Nordic countries [4, 5], also in Finland [6, 7]. In 2018, the prevalence in Sweden was around 3.0% and around 2.0% for Norway and Denmark [4]. By 2018 in Finland, the prevalence of ADHD medication was 4.4% among boys and 1.0% among girls [6]. Just recently, it was recommended to Finland by the UN Committee on the Rights of the Child to ensure that medications for children, including those to treat ADHD, are prescribed only when strictly medically indicated after an individualised assessment of the best interest of the child [8]. However, recent data on the incidence of ADHD medication use among this vulnerable patient group in Finland and other Nordic countries are scarce, although trends in incidence may better reflect changing prescribing patterns.
The aim of this study was to evaluate the incidence of ADHD medication prescriptions by age and sex among Finnish children and adolescents.
Methods
Data
This was a descriptive study based on nationwide administrative registers maintained by the Social Insurance Institution of Finland (SII) [9, 10]: dispensations reimbursable under the National Health Insurance (NHI) scheme register including information on all reimbursed purchases from all Finnish pharmacies, and the register of disease-based reimbursement entitlements. All permanent residents of Finland are covered under the NHI system maintained by the SII.
We identified ADHD drug purchases (the anatomical therapeutic chemical (ATC) classification codes N06BA02, N06BA04, N06BA09, N06BA12 and C02AC02) from dispensations reimbursable under the NHI scheme register. For each purchase, pseudonymised ID, age and sex of the patient and the dispensing date were collected.
According to national regulations, the study required no ethical approval. As the register holder, SII approved the use of the data for the current study.
Cohort definition
The study population included all children and adolescents 18 years of age and under, who had received their first reimbursement for ADHD medication purchase between 1 January 2008 and 31 December 2019 in Finland (n=41,920). To ascertain true ‘naïve’ use we excluded all patients with any purchases during the years 2006–2007 (n=4831). To avoid misclassification, we also excluded patients diagnosed with narcolepsy (n=67) using the register of disease-based reimbursement entitlements. In addition, children aged under 6 years (n=1162) were excluded.
Statistical methods
The population was classified by sex into four age groups (6–8, 9–12, 13–15 and 16–18 years). The incidence rate (IR) was calculated as a ratio of the number of new users and the number of subjects at risk.
The annual, sex and age-specific IR was reported with 95% Jeffreys confidence interval (CI).
Rate ratios (RRs) were modelled using negative binomial models. The initial model included as factors: the year of initiation, sex and age group and all interactions. From this model, non-significant factors were gradually omitted. As the interaction between sex and age group was statistically significant, the modelling was repeated separately for both sexes.
A significance level was set at 0.05. Analyses were performed using SAS (version 9.4) for Windows. Graphs were constructed in R version 4.2.1 using the ggplot2 package.
Results
In total 40,691 subjects aged 6–18 years purchased their first ADHD medication during 2008–2019. The median age of the subjects was 9 years (Q1=8, Q3=12) and 77.4% were boys.
The incidence of ADHD medication use increased for all study years (P<0.0001). In 2008 there were 1653 new users (IR 2.1, 95% CI 2.0, 2.2) while in 2019 there were 6760 (IR 9.0, 95% CI 8.8, 9.2). In 2019 the incidence was 4.3 times greater than in 2008 (RR 95% CI 2.5, 7.2, P<0.0001).
The statistically significant change was already seen among boys from 2015 onwards, whereas it was seen from 2017 onwards among girls (Table I).The IR was also associated with sex (P<0.0001). The boys had on average 2.8 times the IR compared with girls (RR 95% CI 2.2, 3.6, P<0.0001) (Figure 1). The increase was greater among girls with the incidence increasing 7.6-fold (RR 95% CI 2.1, 27.4, P=0.0019), whereas among boys the increase was 3.7-fold (RR 95% CI 2.0, 6.5, P<0.0001).
The annual numbers of new users of ADHD medications, incidence per 1000 subjects with 95% confidence intervals by sex and the statistical significance of change compared to 2008.
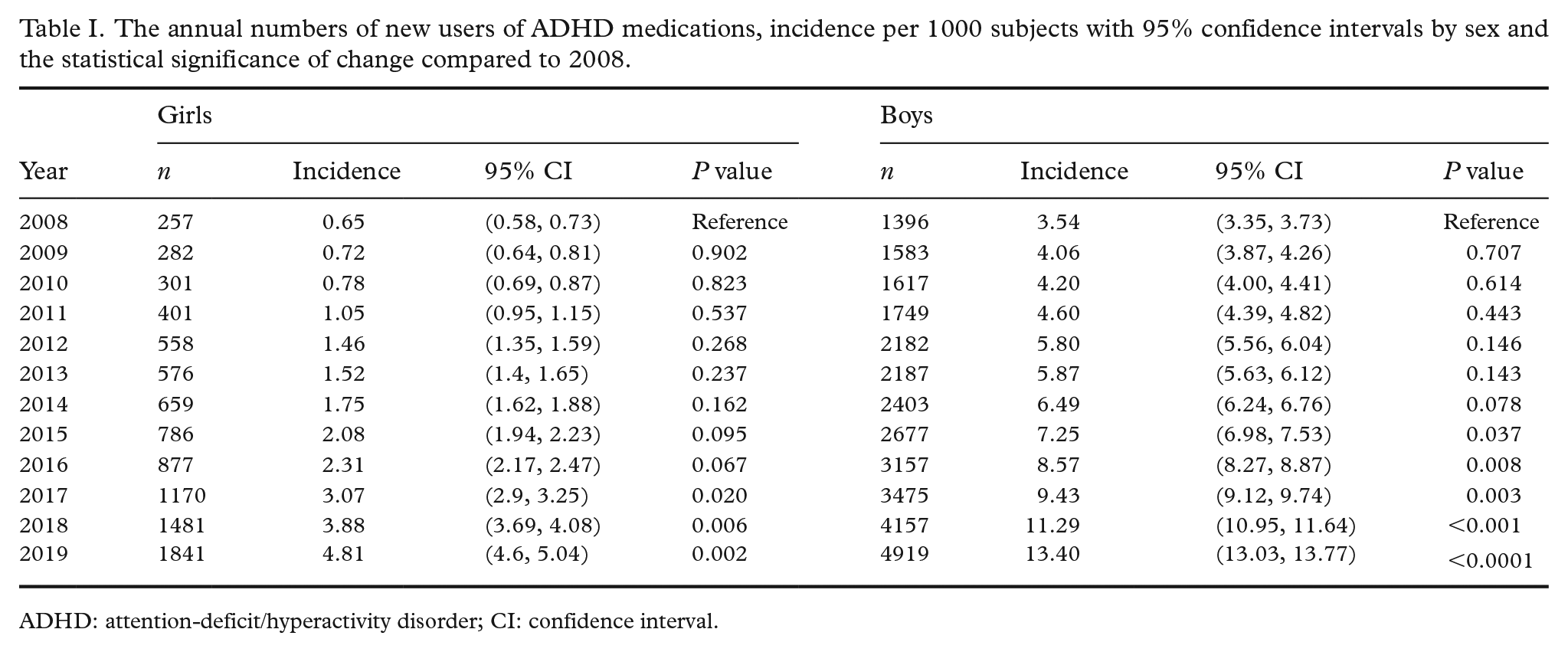
ADHD: attention-deficit/hyperactivity disorder; CI: confidence interval.
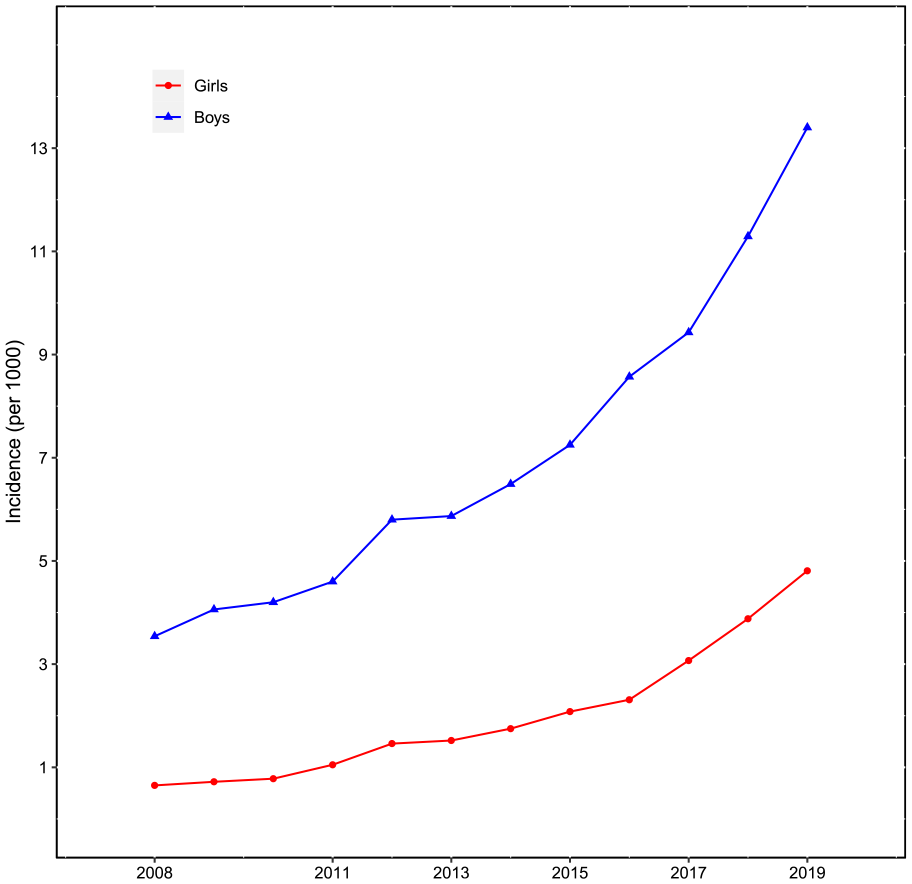
The incidence of attention-deficit/hyperactivity disorder (ADHD) medication use among Finnish children and adolescents by sex between 2008 and 2019.
The IR was associated with age among boys (P=0.0001) (Figure 2). The IR was 6.8 times higher among 6–8 year-olds as compared with the reference group of 16–18 year-olds (RR 95% CI 4.3–10.6, P<0.0001). By comparison, the incidence rate was 3.8 times higher among 9–12 year-olds (RR 95% CI 2.4, 6.0, P<0.0001) and 2.5 times higher among 13–15 year-olds (RR 95% CI 1.5, 4.1, P=.0003).
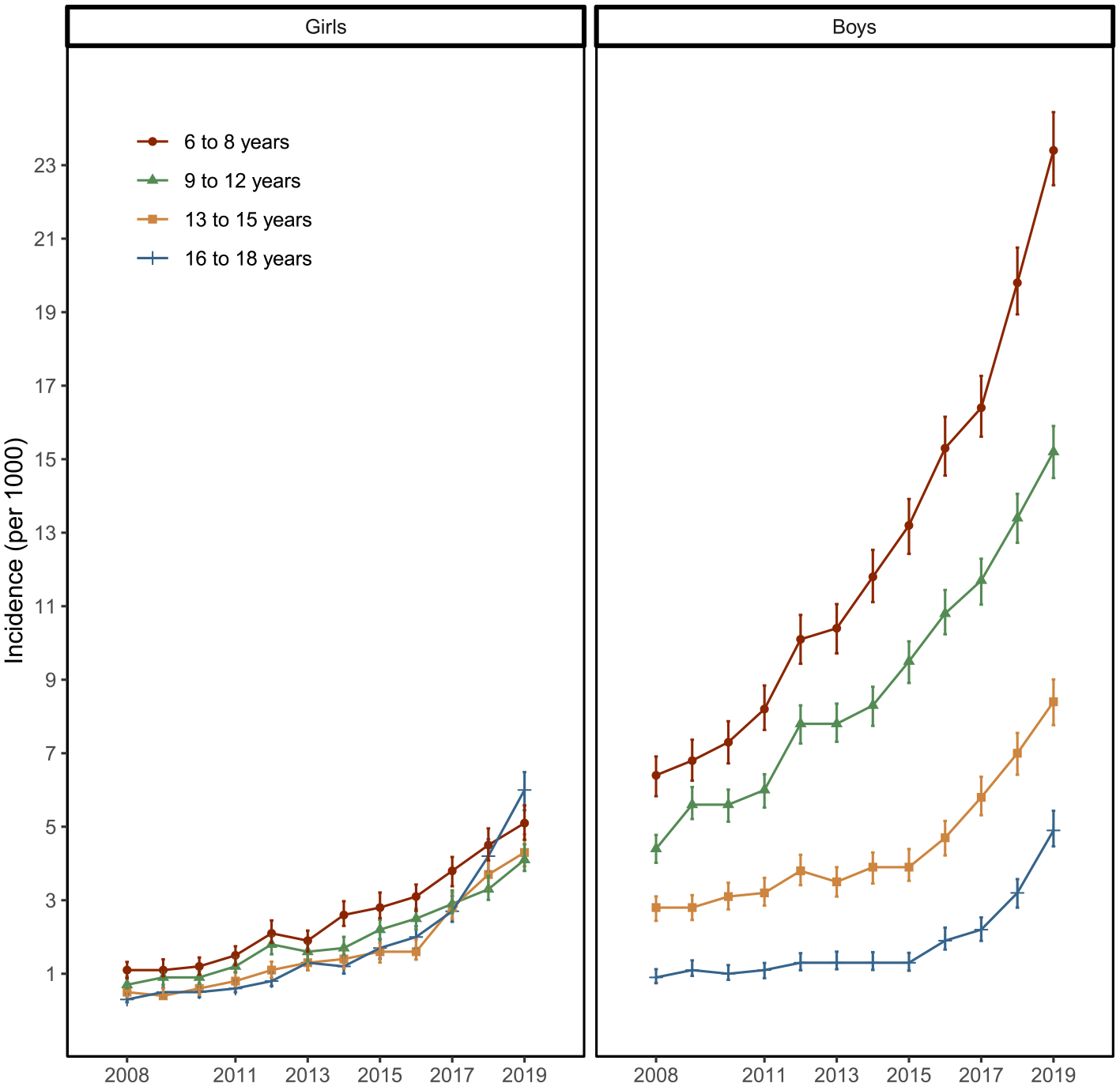
The incidence of attention-deficit/hyperactivity disorder (ADHD) medication use among Finnish children and adolescents by sex and age group between 2008 and 2019.
Discussion
The incidence of ADHD medication use among Finnish children and adolescents increased steadily from 2008 to 2019. The incidence remained higher for boys but increased more for girls. However, incidence was especially high among young boys.
The direct comparison of our results with other European countries is difficult because no European studies on incidence covering our full study period are available. Furu et al. assessed the incidence of ADHD medication use for all five Nordic countries during 2008–2012 [11]. In 2012, the incidence among 6–17 year-olds was highest in Iceland (17 per 1000 boys, nine per 1000 girls) and lowest for girls in Finland (two per 1000 girls and six per 1000 boys) [11].
We observed diminishing sex disparities since the incidence increased more for girls. Similarly, a recent study from Australia reported the incidence of ADHD medication use during 2012–2020 to increase the most among 13–17-year-old girls (from 1.4 to 5.3 per 1000) [12]. The incidence for 6–12-year-old boys in 2019 in Australia was 15.8 per 1000.
The use of ADHD medications for children and adolescents appears now to be more common in Finland than in Norway or Denmark [4, 6]. Until now, increasing rates of ADHD medication use in Finland have been speculated to reflect the better recognition of ADHD in childhood instead of a true increase in the frequency of ADHD diagnoses or unwarranted channeling of ADHD medications. Considering our findings, better recognition might still explain the increase among girls but should eventually result in the incidence also plateauing among young boys. This was not observed here despite the more than 10 years of follow-up in narrow age categories in which small practice changes could be noticed.
A recent review on over 300 published studies found convincing evidence of ADHD overdiagnosis and overtreatment in children and adolescents, especially on the milder end of the ADHD spectrum [13]. In Finland, younger relative age was associated with an increased risk of receiving a diagnosis and medication for ADHD [7, 14], especially during the first school years (ages 6–8). Furthermore, excessive exposure to screens [15–20] and shorter sleep duration during childhood [21] are known risk factors for inattentive or hyperactive symptoms. Also, the changes in school environments [22] and increasing social inequalities [23, 24] may play a role. Data from France indicate that the pharmacological treatment of ADHD may be prioritised over psychosocial support for children from underprivileged families [25]. Thus, concern arises that psychosocial interventions including parental support are not appropriately utilised or available in Finland for the treatment of ADHD and related symptoms especially for young boys starting school.
The major strength of our study is that the data cover the whole Finnish population over a 10-year study period. Major limitations were that only reimbursed purchases were included and there were no records available for clinical analysis of patient-level data on ADHD risk factors nor the non-pharmacological treatment approaches applied. As a further limitation common to all register-based studies, purchases of ADHD medication may not always translate to actual use.
Nonetheless, the present findings warrant critical evaluation of the current diagnostic and medical treatment policies in ADHD and related symptoms in Finland, and of the sufficiency of parental and other psychosocial support offered by society especially for young children and their families.
Footnotes
Acknowledgements
The author(s) would like to thank E Juulia Paavonen for her valuable comments during the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.