
Abstract
Aims:
Among international immigrants, health changes by duration of residence are commonly interpreted as an expression of acculturation to the receiving country context. This study compares changes in immigrants’ health risk behaviors by duration of residence to changes by acculturation levels, in order to assess whether duration of residence can be regarded as a proxy for acculturation.
Methods:
Using data from a previous systematic review, we identified 17 quantitative studies examining changes in alcohol, tobacco and drug use, physical inactivity, and diet by both duration of residence and acculturation level in the same population. We compared the directionality and consistency of these associations through tabulation and vote counting.
Results:
The majority of studies reported no or inconsistent changes in health risk behaviors by duration of residence versus by acculturation, including with opposite directionality. Four studies reported significant estimates with consistent directionality, while five reported consistent, non-significant estimates.
Conclusions:
Introduction
Various acculturation measures have been designed over the past decades to categorize immigrants and their descendants by their level of belonging or proximity to the receiving country context, in terms of their ethnic identity, language proficiency, and cultural orientation, among other dimensions [1]. In turn, these indicators of acculturation have been used to explain immigrants’ behavioral changes [2]. Multiple reviews have shown that with greater acculturation, immigrants tend to adopt various health risk behaviors including alcohol, tobacco and drug use, physical inactivity, and poor diet (the so-called acculturation paradox), often converging with behavioral levels of the native population in the receiving country [3–6].
The cultural interpretation of immigrants’ behavioral changes is not limited to studies utilizing acculturation measures specifically. A recent systematic review on immigrants’ health risk behaviors highlighted that behavioral changes by duration of residence (DoR) are also commonly attributed to acculturation processes [7]. In other words, DoR is often used as a proxy for acculturation, based on the assumption that immigrants tend to experience greater levels of identification with native norms and practices of the receiving country over time. However, this has been contested from a health equity perspective, given that immigrants tend to adopt health risk behaviors that are already unequally distributed within the native population (so-called unequal assimilation) [8]. In fact, this unequal distribution of risk behaviors is key for understanding the reproduction of health inequalities in society.
Beyond acculturation, DoR is regarded as a valuable public health measure to monitor immigrants’ health over time, reflecting other processes such as cumulative experiences of socioeconomic inequalities and discrimination [9]. Yet, without empirical evidence, the assumption that DoR directly corresponds to acculturation limits consideration of these alternative time-dependent processes underlying immigrant health changes [1,7,9]. In order to assess the applicability of DoR as a proxy for acculturation, the aim of this study was thus to investigate how changes in immigrants’ health risk behaviors by DoR compared with changes by their acculturation levels.
Methods
This study is based on material from our previously published systematic review on international immigrants’ health risk behaviors by DoR [7,10]. In the review, the PubMed/MEDLINE, Web of Science and ProQuest databases were searched for English-language peer-reviewed articles published from 1 January 2000 to 31 December 2019, which quantitatively examined changes in health risk behaviors (i.e., alcohol, tobacco and drug use, physical inactivity, and diet) by DoR among international first-generation immigrants. For the current study, we included all articles from the review that additionally evaluated changes in risk behaviors by acculturation level. Data was extracted on receiving country, immigrant population, health risk behavior, and on DoR and acculturation measures. Tabulation and vote counting were applied to compare the directionality (i.e., increased, null, or decreased) and consistency of associations between DoR and risk behaviors, on the one hand, and acculturation and risk behaviors, on the other. No ethical approval was required for assessment of the secondary data.
Results
Of the 123 articles included in the original systematic review [7], 17 articles [11–27] examined one or more health risk behaviors among immigrants by both DoR and acculturation level (for study descriptions and comparisons, see Table I). All studies were cross-sectional, from the USA (n = 10) or Europe (n = 7), and examined alcohol (n = 7), tobacco (n = 4), drug use (n = 1), physical activity (n = 5), and/or diet (n = 3). DoR was measured categorically (n = 11) and/or continuously (n = 7). Acculturation indices captured one or more dimensions relating to social networks/interactions (n = 9), cultural orientation/competence (n = 8), language use (n = 6), ethnic identity (n = 3), sense of belonging (n = ), and/or cultural behaviors/preferences (n = 1).
Overview of the 17 studies included in the literature review and the consistency of associations between immigrant health risk behaviors and measures of duration of residence versus acculturation.
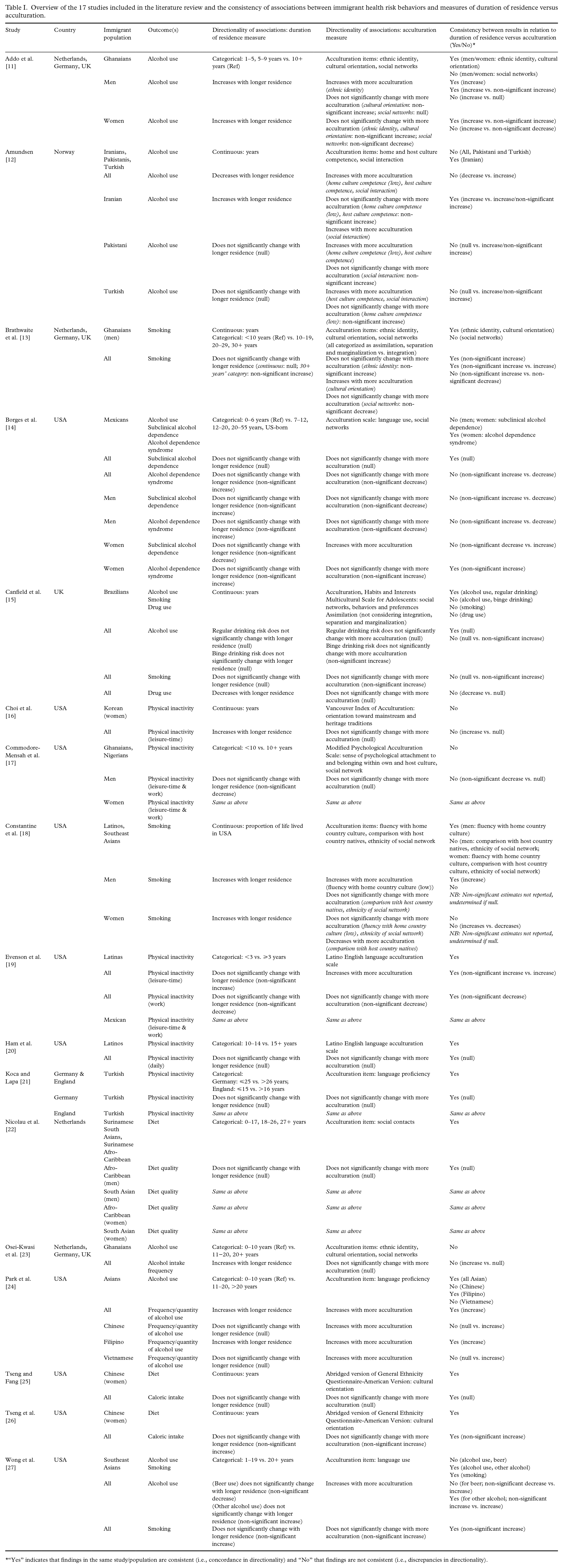
“Yes” indicates that findings in the same study/population are consistent (i.e., concordance in directionality) and “No” that findings are not consistent (i.e., discrepancies in directionality).
Eleven of the 17 articles reported inconsistent estimates with regard to the directionality of findings for health risk behaviors by DoR versus by acculturation, either with opposite directionality, irrespective of significance [11–14,18,27], or with one null finding [11,12,15–18,23,24]. This included studies with composite and specific measures of acculturation (i.e., social networks) [11,13,18]. For consistent findings, only four articles reported consistent, significant estimates [11,12,18,24], for men [11,18] or specific immigrant groups [12,24]. Five studies reported non-significant estimates of the same direction [13,14,19,26,27], and another six studies consistently null findings [14,15,20–22,25]. Consistent findings were found between DoR and composite or specific acculturation measures of cultural orientation/competence [11,13,18,25,26], ethnic identity [11,13], and language [19,20,21,24,27].
Findings from studies on alcohol use by DoR versus acculturation varied, demonstrating null or inconsistent changes [11,12,14,15,23,24,27] or consistent changes in the same direction [11,12, 14,24,27]. Studies on smoking [13,15,18], drug use [15], physical inactivity [16,20,21], and diet [22,25] also generally showed null or inconsistent findings, with some exceptions indicating same directionality [18,19,26,27].
Discussion
Most of the 17 reviewed studies showed discrepancies between international immigrants’ changes in health risk behaviors by DoR versus by acculturation levels. Only four studies demonstrated estimates with consistent directionality, while others reported inconsistently null findings or findings with opposite directionality. We noted important differences by specific measures of acculturation and population groups (i.e., by gender and origin). These findings challenge the use of DoR as a proxy for acculturation in immigrant health research.
The inconsistencies observed in this study support the need to consider alternative time-dependent explanations of immigrant health changes beyond acculturation, such as cumulative experiences of socioeconomic disadvantage and discrimination. These can influence the adoption of unhealthy habits over time as a means of stress relief [9]. Moreover, the fact that these health risk behaviors are socially patterned within the receiving society may suggest that their adoption among immigrants is also linked to social inequalities [8].
In addition to the inconsistencies between DoR and acculturation measures, our findings did not support the existence of a universal acculturation pathway—not all studies found that immigrants adopted risk behaviors with increased acculturation, irrespective of DoR. This contradiction with previous findings could be attributable to a select sample of acculturation studies (i.e., with DoR measures), although it is more likely that acculturation processes vary across immigrant groups. Moreover, we found no universal pattern of behavioral change by longer DoR, supporting the results of our previous systematic review [7].
This is the first effort to compare changes in health risk behaviors by DoR to those by acculturation within the same populations. Comparisons were challenged by a lack of between-study consensus on definitions and operationalizations of DoR and acculturation. The general reliance on statistically significant results, which are strongly dependent on how DoR and acculturation are measured, and the varied model specifications between measures and across studies, posed additional challenges for comparison. Yet, we found evidence of inconsistent results between measures that are unlikely to be influenced by the above-mentioned limitations.
To date, public health researchers have primarily relied on theories of acculturation to interpret changes in immigrants’ health behaviors [7]. This study suggests that the appropriateness of DoR as a proxy for acculturation needs to be carefully re-examined, with further consideration of the role of social factors alongside acculturative processes in the adoption of these behaviors [1,9]. Our findings support the need to detach evidence on DoR from the acculturation framework and consider alternative explanations for immigrants’ health changes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Council for Health, Working Life and Welfare (FORTE) (grant nos. 2016-07128, 2021-00271); the Swedish Research Council (Vetenskapsrådet; grant no. 2018-01825); and the Swedish Alcohol Retail Monopoly Research Council (Systembolagets Alkoholforskningsråd; grant no. 2021-0015).