
Abstract
Aims:
In pandemics, infection exposure and quarantine represent critical occupational risks for healthcare workers (HCWs). However, while the psychological consequences of HCWs’ quarantine have been reviewed, other potential implications of quarantine on HCWs, such as those that are work-, professional-, social- and private-related, have not been summarised to date. Summarising quarantined HCWs’ experiences in the current and past pandemics, as investigated with qualitative studies, might improve awareness of their needs, concerns, and the consequences of quarantine on their personal lives. Therefore, the lived experience of quarantined HCWs was reviewed and subjected to meta-synthesis and -summary.
Methods:
A systematic review of qualitative studies followed by a meta-synthesis and -summary allowing an interpretative integration of the findings of qualitative studies, was performed. PubMed, CINHAL and Scopus databases were explored up to 31 January, 2021, without any limitation in time. The methodological quality of the studies was assessed using the Critical Appraisal Skills Programme. Methods and findings are reported according to the Enhancing transparency in reporting the synthesis of qualitative research statement.
Results:
A total of 635 records were retrieved and five studies were included. Overall, five themes summarised the lived experience of quarantined HCWs: 1) Being emotionally challenged; 2) Living the quarantine limitations; 3) Losing freedom; 4) Accepting the quarantine; and 5) Staying away from me. The most frequent categories across studies were ‘Feeling stressed’ and ‘Being constrained’ (both 100%). The least frequent were ‘Feeling sad’ (20%), ‘Enjoying my family’ (20%) and ‘Being refused as a family member’ (20%).
Conclusions:
The lived experience of HCWs is multidimensional, the implications of which also affect private spheres of life: the immediate family and wider relatives. Understanding and learning from HCWs’ lived experiences might support policymakers, public health authorities and managers with the goal of maintaining the highest physical and mental health of staff during outbreaks. Timely services supporting HCWs, both during and after episode(s) of quarantine, are suggested to prevent additional burdens on frontline professionals.
Keywords
Introduction
From December 2019 when the first case of the novel coronavirus disease (COVID-19) was reported in China, the virus spread globally, achieving a rapid escalation of cases worldwide [1]. A few months later, in March 2020, the World Health Organization (WHO) declared COVID-19 a public health emergency of global concern [2]. Since the beginning of the pandemic, national and international governmental and public health authorities have implemented interventions to contain the spread of the virus, including lockdowns and different kinds of quarantine, such as en masse, individual, or self-quarantine [3]. Healthcare systems have been globally affected, involving thousands of healthcare workers (HCWs) in contact tracing, testing, diagnosing and taking care of individuals and entire populations [4].
During the pandemic, HCWs were highlighted as the population at major risk of contracting the virus, especially during the first wave when personal protective equipment was scarce [5]. By December 2020, more than 1.6 million HCWs had been infected with COVID-19 across 34 countries [6] with 893,871 cases and 3,506 deaths being reported in the United States alone by 28 January, 2021 [7]. The number of infected or contagious HCWs further weakened the healthcare services, which had been exposed to unprecedented volumes of patients requiring hospital and community care. Interim guidelines were established and continuously updated to restrict contact with HCWs potentially exposed to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), stipulating return to work protocols and preventing additional staff shortages [8]. As in previous pandemics, risk assessment and surveillance of HCWs were recommended (a) to promote early identification of professionals at high risk of exposure to COVID-19; (b) to establish the duration of restrictions for contagious or infected HCWs; and (c) to establish work restrictions for asymptomatic HCWs potentially exposed to the virus [8]. All such recommendations are aimed at limiting the spread of the infection within healthcare facilities and thus among patients. In this context, quarantine functions as an established multicomponent strategy to control and contain disease outbreaks. Although the main features of quarantine measures have been recognised as common [9, 10], its parameters and control measures have been reported to change according to the nature and degree of disease transmission risk, and also from country to country (e.g. the management of quarantined HCWs at home or in a medical facility) thus resulting in different consequences (e.g. fears of discrimination).
HCWs involved in the care of patients, and those quarantined, have been reported to suffer stressful experiences, such as worrying about contracting the infection themselves or infecting others, being stigmatised because of their profession, prevented from working due to being quarantined [11,12], and being isolated from their family [11]. As reported in previous outbreaks (e.g. SARS, Middle East Respiratory Syndrome (MERS)), despite differences in the diseases and in the geographical areas affected, HCWs involved in the diagnosis, treatment and care of infected patients have reported exceptional stress levels, depressive symptoms, post-traumatic stress disorder, and burnout [13], increasing the risk of HCWs leaving the profession after the pandemic [4]. More than a quarter of HCWs were reported to experience symptoms of emotional distress during MERS, and after months/years of SARS, many HCWs quarantined or at high risk of exposure reported post-traumatic stress symptoms or alcohol and/or substance abuse [14]. Furthermore, studies documented that quarantined HCWs felt higher levels of anxiety, frustration and powerlessness than non-HCWs [15]. Taking this evidence as a starting point, identifying appropriate strategies capable of protecting HCWs is paramount to maintaining a well-performing and resilient healthcare system that is able to cope with the current [16] and future pandemics. However, while the psychological consequences of quarantine among HCWs have been summarised by rapid review [13], no summary of other possible consequences (e.g. work, professional, social, and pertaining to private spheres of life [9, 10]) has been undertaken to date. Summarising quarantined HCWs’ experiences in the current and past pandemics as investigated with qualitative studies, may improve awareness of their needs, concerns and the consequences of quarantine on their personal lives. Moreover, it may serve as an evidence base in designing the strategies and actions required to prevent, protect and support HCWs in case of future epidemics. Therefore, the lived experience of quarantined HCWs was reviewed and subjected to meta-synthesis and -summary.
Methods
Study design and literature search
The following research question was addressed: What is the lived experience of quarantined HCWs as documented to date? A systematic review of qualitative studies was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [17] followed by a meta-synthesis and -summary [18]. The meta-synthesis approach was chosen because it allows an interpretative integration of the findings of qualitative studies, and a novel exploration and interpretation of the phenomenon under study through the voices of individuals involved in the primary studies [18]. The Enhancing Transparency in Reporting the Synthesis of Qualitative Research statement [19] guided the methods and the development of the findings (see Supplementary Table SI).
PubMed, Cumulative Index of Nursing and Allied Health Literature, and Scopus databases were searched up to 31 January, 2021, with no publication date limits, to ensure that all relevant studies were included in the review. The key terms used were quarantine, cordon sanitaire, self-quarantine, healthcare professional, healthcare personnel, healthcare worker, experience and perspective. Medical Subject Headings, free words and keywords were associated, modified when necessary, and combined using Boolean operators (see Supplementary Table SII). Moreover, manual searches, accessing the reference lists of eligible studies and snowballing strategies [20], such as following up the references of studies focused on quarantine experience and subsequent articles found during database exploration, were also carried out to identify additional studies.
Included were (a) primary qualitative studies; (b) those documenting the experiences of quarantined HCWs defined as paid professionals serving in healthcare settings who have the potential for direct or indirect infection exposure [8]; (c) reporting different types and locations of quarantine (e.g. home quarantine, home–work quarantine); (d) those published in English; and (e) with abstracts available. Therefore, studies concerning (a) the general population, (b) other experiences (e.g. isolation due to infection), and (c) published in a language other than English, were excluded. According to the inclusion and exclusion criteria, titles and abstracts of all studies were assessed independently by two researchers to confirm eligibility, before retrieving the full texts.
Search outcomes
Database searches yielded 635 records. After removing duplicates and screening titles and abstracts, 33 full-text studies were assessed by two researchers (VB, AP): two studies met the inclusion criteria. Through the manual research, three additional studies were found and a total of five were ultimately included (Figure 1).
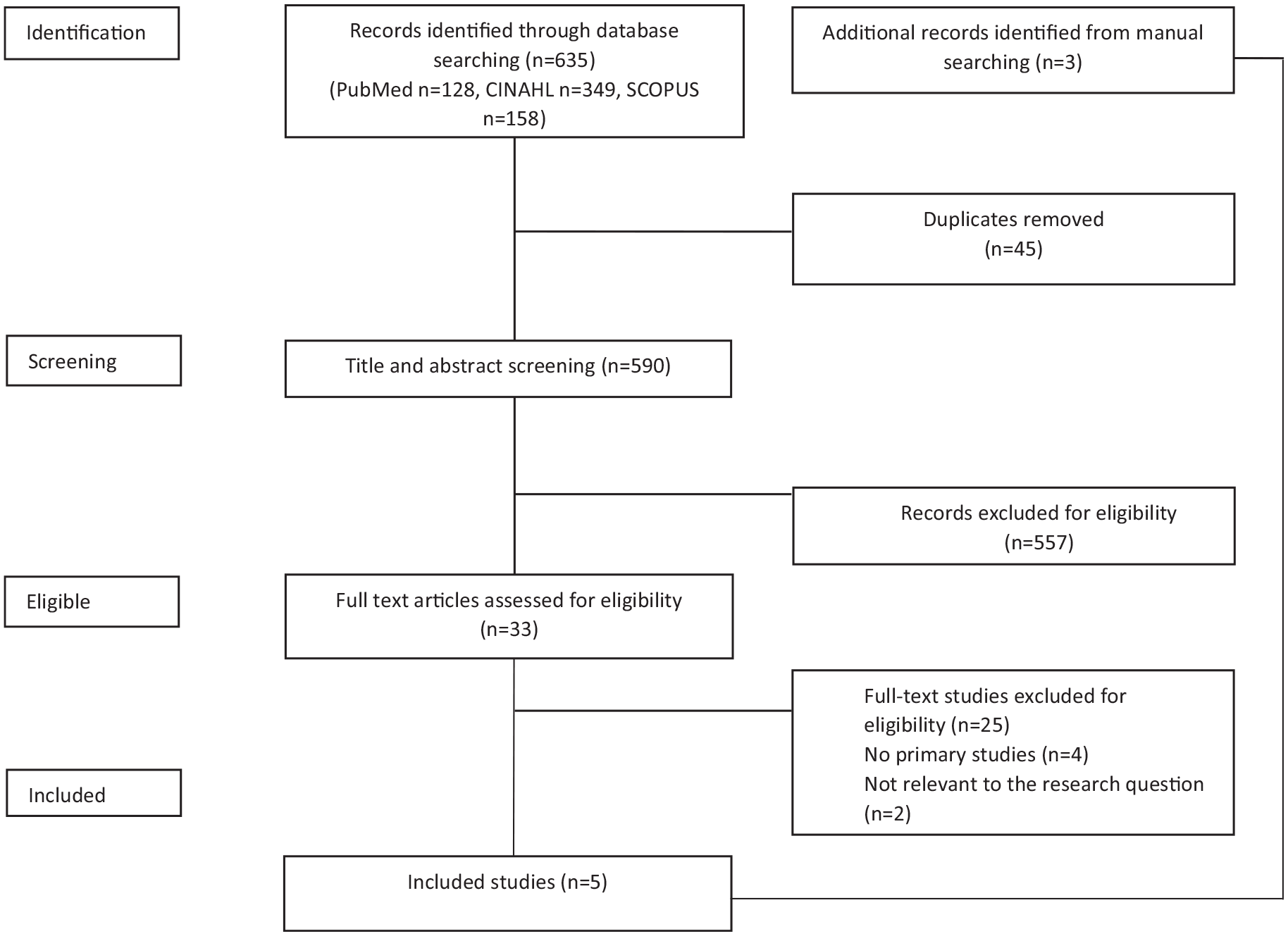
Search strategy development and results.
Quality assessment
The Critical Appraisal Skills Programme (CASP) [21] was adopted to evaluate the methodological quality of the included studies. The tool consists of 10 questions guiding researchers to examine certain methodological aspects resulting in three evaluation options, namely Yes (= 1), Unclear (= 0.5), and No (= 0) and, thus, in a score [22].
The assessment was performed independently by two researchers (in couples, see authors); in the case of a disagreement a consensus was reached and, if necessary, any further disagreement was discussed with a third researcher. The global evaluation of each study was then calculated by adding the score obtained by each question resulting in an assessment of low (CASP = from 0 to 5.5 score), moderate (6–8.5) or high (9–10) quality [23]. The methodological quality assessment was performed to better explore, interpret and value the findings of the included studies [24] and not as a criterion of inclusion.
Data abstraction and synthesis
A data extraction grid was developed and piloted on one study, to extract and summarise the findings: no changes were needed. One researcher then populated the grid by extracting the following data: author(s), publication year, country where the data collection was performed, and the infection requiring quarantine; the aim(s) of the study, the design, the data collection methods, the setting(s), who performed the interview(s), and the quarantine place/duration. The participants’ main characteristics and the themes/categories as documented by studies were then recorded. Only data referring to HCWs and their quarantine experience were extracted and analysed. Two studies included populations other than HCWs, that is, patients [25], students, HCWs’ family members, community volunteers and adult infective contact subjects [26]; their data were not considered in the analysis.
The findings of each study were recorded maintaining the original wording; they were then analysed and synthesised by researchers according to the following steps [18]:
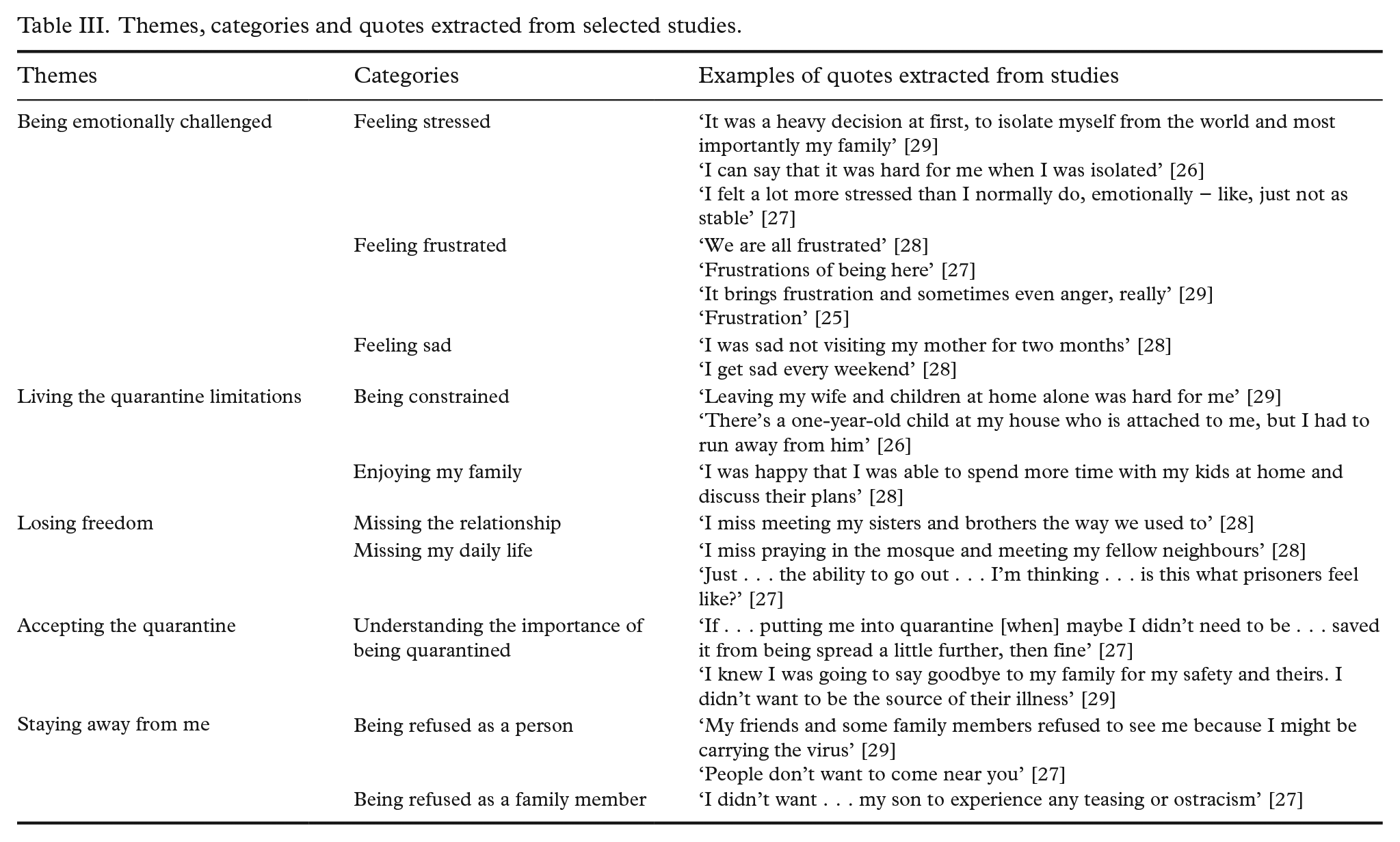
Line-by-line inductive coding of each study’s findings and, when available, by extracting the quotes: 41 codes were initially identified and categorised. For example, the following quote [27]: ‘I felt a little awkward with some of my neighbours . . . When they saw me, they ran, literally, in their house, and I felt angry’ was categorised in the ‘Staying away from me’ code.
The organisation and aggregation of identified codes: according to their similarities and differences, identified codes were aggregated into 10 main categories.
Theme identification: similar categories were aggregated and unified and five main themes emerged. For example, the theme ‘Staying away from me’, was derived from the following categories: ‘Being refused as a person’ and ‘Being refused as a family member’.
Researchers (VB, AP) independently labelled each theme and category according to its content, before reaching consensus. Thus, the inter-study frequency effect size (number of studies containing a category/total number of studies) and the intra-study intensity effect size (number of categories contained in each study/total number of categories) were also calculated [18].
Results
Studies included
Five studies published between 2003 and 2020 were included (Table I). Two were conducted in Canada, and one each in Lebanon, Oman and Senegal, and included HCWs quarantined because of COVID-19 [28, 29], SARS [25, 27] and Ebola [26]. The study designs (e.g. qualitative, exploratory qualitative) and settings (e.g. health facilities, hospitals, community care settings) varied, whereas data collection methods were similar and based mainly upon semi-structured face-to-face/telephone interviews; only one conducted focus groups [28].
Study characteristics.
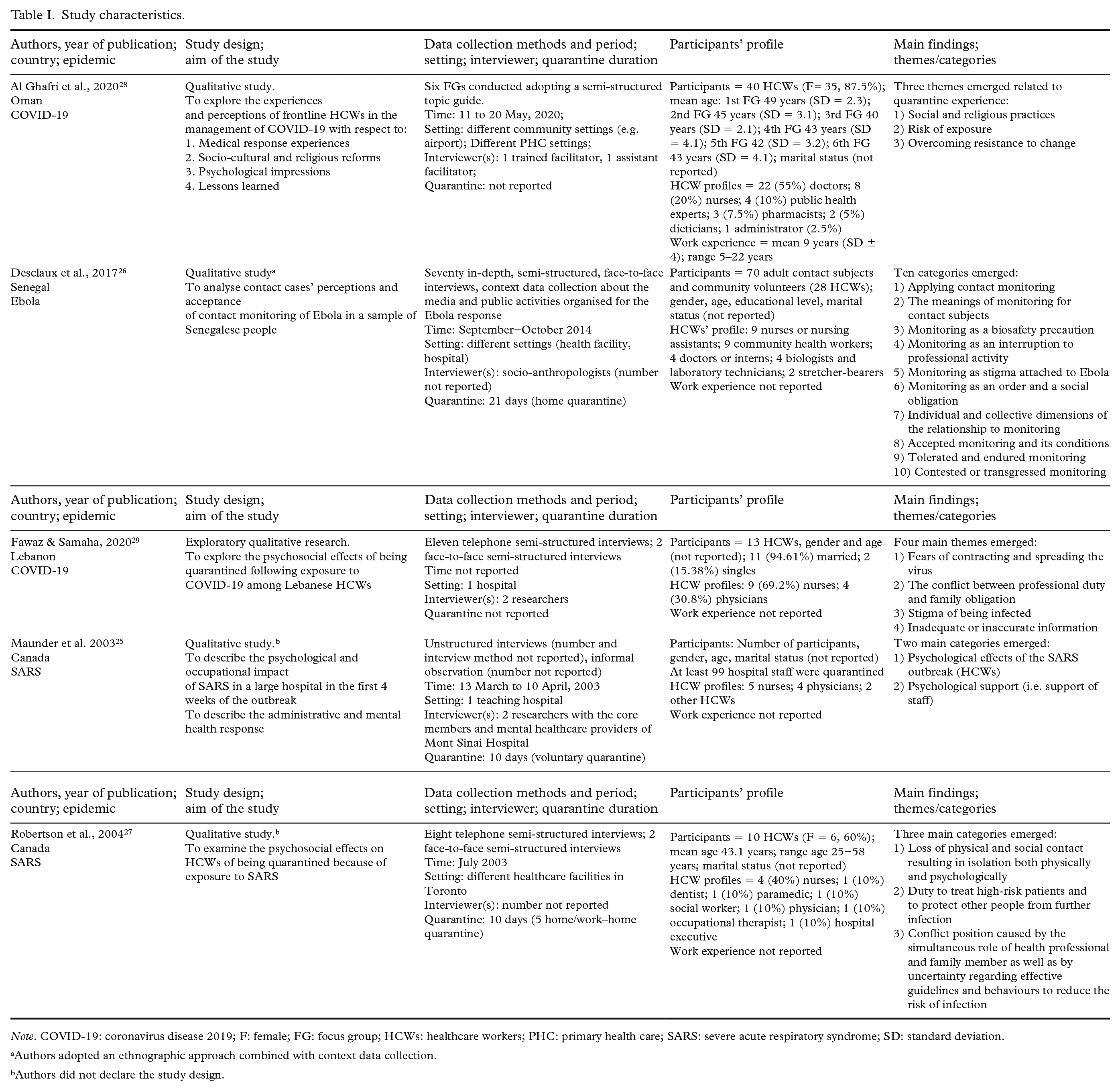
Note. COVID-19: coronavirus disease 2019; F: female; FG: focus group; HCWs: healthcare workers; PHC: primary health care; SARS: severe acute respiratory syndrome; SD: standard deviation.
Authors adopted an ethnographic approach combined with context data collection.
Authors did not declare the study design.
The number of HCWs involved in the studies ranged from 10 [27] to 40 [28], giving a total of 91 participants across four studies; in one study the number of participants was not reported, however the authors declared that at least 99 hospital staff were quarantined and reported the profiles of 11 HCWs [25]. The majority of participants were physicians (N = 35) and nurses (N = 35); participants’ work experience, ranging from five to 22 years, was reported only by Al Ghafri et al. [28].
When reported, the duration of quarantine ranged from 10 to 21 days [25-27]; however, the place or the type of quarantine was described in only three studies, as home quarantine [26], home–work quarantine [27], and voluntary quarantine [25].
Methodological quality evaluation
The studies’ methodological quality ranged from low to high (Supplementary Table SIII). In all, the research aims were clearly reported, and the qualitative methodology was appropriate; moreover, in three of the studies, the research design was appropriate to address the research question [26, 28, 29]. The recruitment strategies were appropriate and well described in two studies [28, 29], while in three the data collection methodologies adopted were clearly reported [27-29]. In one study the relationship between the researchers and study participants was clearly reported [29]; ethical issues were well addressed by three studies [26, 28, 29] as was data analysis in one study [29]. Findings were clearly reported in all studies and the clear value of the research was described in two studies [26, 28].
Meta-summary
As reported in Table II, a total of 10 categories emerged: the study by Al Ghafri et al. [28] reported the highest intra-study intensity effect size (80%) while those of Desclaux et al. [26] and Maunder et al. [25], the lowest (40%). Regarding the inter-study frequency effect size, the most frequent categories across studies were ‘Feeling stressed’ and ‘Being constrained’ (both 100%). Conversely, the least frequent categories were ‘Feeling sad’ (20%), ‘Enjoying my family’ (20%) and ‘Being refused as a family member’ (20%).
Intra-study intensity and inter-study frequency effect sizes of themes/categories.
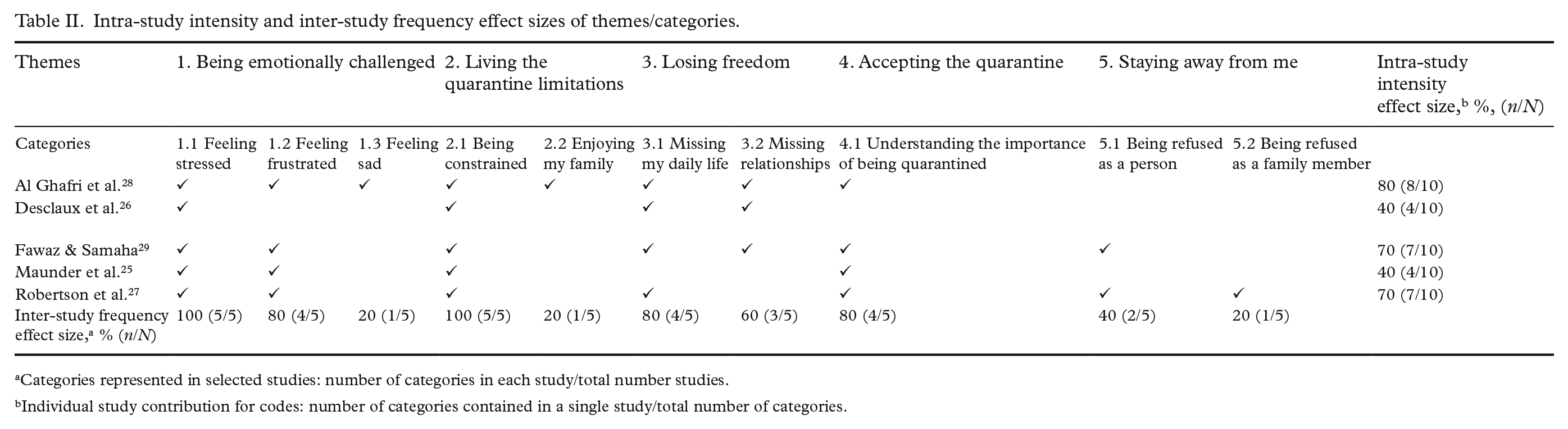
Categories represented in selected studies: number of categories in each study/total number studies.
Individual study contribution for codes: number of categories contained in a single study/total number of categories.
Meta-synthesis
As reported in Table III, the 10 categories resulted in five themes: 1) Being emotionally challenged; 2) Living the quarantine limitations; 3) Losing freedom; and 4) Accepting the quarantine.
Themes, categories and quotes extracted from selected studies.
Theme 1 − Being emotionally challenged
Quarantined HCWs undergo an emotional experience, where a range of feelings are perceived. They have been documented to experience concerns about the risk of spreading the disease to the community and, even more importantly, to their relatives. High levels of stress have been also reported as consequences of changes to HCWs’ daily routines [27, 29] and of choosing to self-isolate to avoid transference of infection [25-28]. Negative emotional consequences of quarantining have also been highlighted by HCWs, such as frustration when needing to align their professional duties with those relating to family and friends [27,29], or when they were kept at a distance because they were considered contagious [29]. Feelings of sadness and depression were also reported in relation to the need for new social norms, such as maintaining social distance from relatives [28]. This emotional burden was also found to trigger physical symptoms as insomnia, fatigue and irritability [25,27]. However, the support received by other colleagues living the same situation created a sense of camaraderie [27], altruism, collegiality and professional responsibility [25].
Theme 2 − Living the quarantine limitation
HCWs reported being quarantined to be an experience of limitation. In the included studies, HCWs suffered from limited physical contact [25, 28, 29] resulting in a loss of intimacy and modified social contact, triggering psychological and physical isolation [27]. Adopting precautions such as living in isolation at home, eating separately from the rest of the family [26, 29], wearing masks in front of the children [27], sleeping in separate rooms [27], and staying at home, not travelling to work as usual [28], were reported as challenging but necessary. Only in one study did participants report that staying at home with their family represented an opportunity to improve relationships and communication with, for example, their children [28].
Theme 3 − Losing freedom
Quarantine resulted in restrictions to individual freedoms [27] and changed HCWs’ daily routines in all aspects, including the spiritual dimension, such as praying in their neighbourhood mosque [28]. Losing daily routines triggered a sense of loss/bewilderment/incomprehension [26-29], with disruptions to routines, relationships with family members and acquaintances also changing dramatically, resulting in perceptions of loss of freedom [26, 28, 29]. For example, some spouses needed extra support in getting their child to school or to go shopping [27, 29], or were compelled to become dependent on their families, causing conflicts and difficulties, especially when the HCW was the person earning the main income [26].
Theme 4 − Accepting the quarantine
Quarantined HCWs have been reported to perceive the restrictions imposed as protective measures [27-29], thus something that should be accepted. They also understood the importance of keeping their distance from their families and friends, and that the imposed restrictions were the only solutions at that time [25]. However, the challenge of staying home because of the sense of professional responsibility emerged [25, 29], and some HCWs were concerned about their colleagues because of the impact of understaffing caused by the applied quarantine [25]. However, in one study, family support was found to be important in increasing acceptance of such restrictions and in motivating HCWs to carry out their professional duties [29].
Theme 5 – Staying away from me
In addition to the consequences experienced by quarantined HCWs, certain behaviours witnessed in others increased the burden and triggered new behaviours. Specifically, in two studies, HCWs specified that working and being quarantined triggered negative reactions from family members and other people both during and after the quarantine, and reactions were more extreme when it was known that the HCW had worked on the frontline [27, 29]. They also reported that often individuals manifested avoidance behaviours as an expression of their fear that HCWs could be infected and contagious [27, 29]. Participants interpreted such reactions as the consequence of a lack of knowledge about the disease and/or individual perceptions of risk; however, these avoidance behaviours caused feelings of anger and hurt among HCWs, especially when expressed by relatives and friends [27, 29]. In order to avoid negative reactions even after the quarantine, HCWs reported remaining cautious in their relationships, and, in some cases, neglecting to mention that they worked in a healthcare setting [27]. Individual worries also extended to family members and fears about their risk of being treated differently; for example, during the SARS outbreak, HCWs who were stigmatised, considered it their duty to protect their children from being mocked or stigmatised by association [27].
Discussion
Studies and methodological quality
To the best of our knowledge, this is the first systematic review of qualitative studies resulting in a meta-synthesis and -summary of the experience of quarantined HCWs during an outbreak. Only five qualitative studies have been published to date and only two concerning the COVID-19 pandemic [28, 29], which might affect the external validity of the findings. On the one hand, the priorities given by researchers during a pandemic are often linked to the capacity of the healthcare systems to respond to pandemics instead of investigating the lived experience of the HCWs; on the other hand, the risk of infection for HCWs might be considered to be an inherent professional risk, therefore of low merit for investigation. However, the quarantine experiences of the general population have also attracted only a few researchers to date [23], suggesting this field requires more attention and greater research investment, combining qualitative and quantitative research to better investigate the evidence derived from different study design methodologies.
Available studies investigating the quarantine experience of HCWs have mainly included nurses and physicians. Their experience might have been influenced by the context, the culture and, above all, by the nature of the risk, for example, its fatality rates (e.g. around 50% in the case of Ebola) [30]. Also, the duration of the quarantine (from a few days to prolonged periods), and the capacity of the healthcare system to cope and remain resilient [31] represented other factors influencing how the quarantine was experienced by HCWs. However, not all data were reported in the published studies, suggesting that future investigations should indicate more precise elements of quarantine, for example its duration, when it started and ended (e.g. fixed-term quarantine) and who ordered it (e.g. employer, national guidelines or self-imposed). Alongside details of the duration and nature of the quarantine, when the data were collected – during or as a follow-up – should also be reported, as this might change perceptions of the experience.
The methodological quality of the studies was found to be higher in those conducted more recently [28, 29] and lower [25] in that conducted around 20 years ago. In evaluating the quality, we used a recently developed tool [21] that might have introduced methodological standards not requested previously. Moreover, with regard to the lack of certain elements or their lack of clarity, researchers might have performed the studies rapidly to ensure immediate scientific communication of the findings [25, 28]: as a result, this might have threatened the methodological quality of the studies but, on the other hand, it ensured the timely sharing of data. Overall, more evidence is needed to capture the in-depth lived experience of quarantined HCWs. Moreover, given the difficulties of distinguishing between the experiences of being quarantined as an HCW and the general experiences of working as an HCW on the frontline during a pandemic, future studies should differentiate the consequences by applying appropriate data collection strategies.
Meta-summary and meta-synthesis
Being quarantined as an HCW is a complex and multidimensional experience. According to the ‘Being emotionally challenged’ theme, HCWs underwent negative psychological consequences, as was also documented in the general population [23, 32]. In previous outbreaks, quarantined HCWs have reported feeling more anxious, frustrated and helpless compared with non-HCWs [15]; during the COVID-19 epidemic, and during the last MERS and SARS outbreaks, numerous cases of infection and deaths among HCWs were documented, and many HCWs experienced feelings of worry, for themselves and their families. Specifically, stress, frustration and sadness [25, 27-29] emerged as being connected to the HCWs having to play simultaneous roles with specific duties: as professionals and as members of a family. However, in contrast to previous literature [15], no information about the symptoms of considerable psychological distress emerged. This might be explained by three lines of reasoning: (a) because the included studies investigated mainly the immediate consequences of being quarantined; (b) the work-related stress and exposure to traumatic experiences [33] with their associated mental health implications [28, 29] might have been considered by participants to be inherent aspects of being an HCW, and thus not strictly connected to the quarantine; and (c) because it might be difficult to distinguish the anxiety, fear and the tendency to isolate as a consequence of the quarantine specifically, from being associated with working as a frontline HCW in general.
However, the findings did suggest the need to offer additional support in the form of accessible and timely services to promote mental health among quarantined HCWs [15], and by educating them to adopt preventive strategies (e.g. taking time to rest; protecting themselves from the risks of harassment and stigma) [34, 35]. During the SARS outbreak in 2003, HCWs reported the positive effects of sessions with psychologists/psychiatrists, even when this support was provided remotely/online (e.g. by telephone or Skype) [14]. Emotional and psychological support could be offered to quarantined HCWs 24/7 through individual or in-group videoconference; more intensive support might be offered to those HCWs manifesting specific risks or needs. An increased awareness of the support available is suggested, with tailored communication materials being targeted at quarantined HCWs. Such multidisciplinary interventions promoting HCW resilience at both personal and organisational levels should be investigated for their effectiveness; further studies are also suggested to understand the implications of quarantine among HCWs over time and its connection with, for example, an increased risk of post-traumatic stress disorder, already documented during outbreaks [35].
Being quarantined and thus confined at home has been reported as a limiting experience (‘Living the quarantine limitations’): in all the studies included, HCWs reported perceiving themselves to be constrained and having to accept new social roles and ‘norms’, such as social distancing – especially difficult from their own children [26, 27]. However, in some cases, being at home is reported as an opportunity to stay with the family [28] and a chance to enjoy time with relatives (e.g. children). HCWs have been documented as being exposed to increased work demands in terms of hours/weeks and shifts, thus limiting the likelihood of spending time with the family [36]. Therefore, remaining at home might represent a sort of respite, benefiting both family relationships and potentially reducing work-perceived stress and tiredness.
In addition to the limitations, HCWs reported missing relationships and daily routines (‘Losing freedom’), which could be considered an expected consequence of quarantine, as was also reported in the general population [23]. However, in contrast to the general population [23], HCWs were found to ‘Accept the quarantine’ as a protective action, and some interpreted it pragmatically as an implicit risk of their professional role [27]. Receiving support from the family [29] and sharing such lived difficulties with other colleagues [27] were underlined as important, suggesting that, alongside the support offered the healthcare managers or services [37], the support offered by peers is crucial to promoting psychological well-being [38]. However, as emerged with the previously discussed theme, ‘Staying away from me’, which had lower inter- and intra-study intensity, negative and distancing reactions from family members, friends and people in general existed before the quarantine [29] but continued afterward [27, 29]. This seems to suggest that such reactions were not necessarily connected to the HCWs’ quarantining, rather to their role, thus exacerbating the challenges faced by HCWs. Avoidant behaviour directed towards and stigmatisation of HCWs during outbreaks were widely reported [15] by those quarantined for SARS [39] and Ebola [26]. The lack of knowledge and understanding about the disease from civil society could be considered an underlying cause of such behaviour, which was only exacerbated by the conflicting information spread by social media [40]. Therefore, dissemination of accurate, consistent information and promotion of interventions to educate the public/society [41] are recommended.
Study limitations
This systematic review resulting in a meta-synthesis and -summary presented several limitations. First, only studies written in English and published in indexed journals were eligible, grey literature was not searched; this strategy may have introduced information bias. Second, the methodological quality of the studies included was assessed by the authors, who also extracted and synthesised the findings: although all have received advanced education and have previous research experience in the field, their background (i.e., nursing) might have affected the results (for example, in evaluating the research findings). Third, the five studies included (only two of which were conducted during the COVID-19 pandemic) reported data that had been collected in different countries, and on outbreaks caused by infections with differing spread and case fatality ratios, therefore, the generalisability of the findings might be limited. Considering that the participants’ experiences may have been influenced by the nature of the disease, the historical period and the geographical contexts in which the data were collected may have affected the interpretation of the HCWs’ quarantine experiences. Future studies should consider categorising results according to the underlying infection. Moreover, two studies investigated specific aspects of the quarantine, for example, the psychosocial implications [27, 29] rather than the whole experience. Finally, different quarantine typologies emerged across the studies, but the limited data available did not allow for differentiation of the lived experiences, for example, when experienced at home, home–work or as voluntary quarantine. Given the multidimensionality of the quarantine experience, and the limited quantitative studies available in this field [42], mixed-method studies and reviews are encouraged.
Conclusions
Understanding HCWs’ lived experience and needs might support policymakers, public health authorities, managers, and peers in the crucial goal of maintaining the highest levels of health and wellness of the workforce during and after pandemics. Moreover, information derived from previous epidemics might be transferred to future outbreaks to enact early tailored interventions to promote the well-being and the resilience of HCWs and, thus, the capacity of the entire healthcare system.
Few qualitative studies aimed at exploring the experience of quarantined HCWs are available. The lived experience of quarantined HCWs is multidimensional, comprising psychological-, professional-, social-, and private implications that also affect the wider family. Timely, during and after services and strategies preventing and/or limiting the psychological and social implications of quarantining are needed to prevent additional burden to that already lived as frontline professionals; moreover, managerial and peer support is recommended. Examples might include encouraging peer support, offering institutional messaging, individualised guidance, and rapid access to information and psychological services. Further investigations are suggested to measure the effectiveness of tailored interventions aimed at preventing the negative consequences of quarantine, and at avoiding stigmatisation of HCWs in future pandemics. In this context, given the multidimensionality of the quarantine experience, qualitative and quantitative studies, integrated into mixed-method approaches, are recommended.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948221128158 – Supplemental material for The lived experience of healthcare workers in quarantine: Findings of a systematic review, meta-synthesis and meta-summary
Supplemental material, sj-docx-1-sjp-10.1177_14034948221128158 for The lived experience of healthcare workers in quarantine: Findings of a systematic review, meta-synthesis and meta-summary by Valentina Bressan, Matteo Danielis, Davide Caruzzo, Irene Mansutti, Renzo Moreale, Jessica Longhini and Alvisa Palese in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.