
Abstract
Aims:
The aim of this study was to adapt the Health Literacy Questionnaire (HLQ) in English and Norwegian for use with parents.
Methods:
The research group evaluated all HLQ items and, where relevant, modified them to refocus the attribution of care to that of a child by a parent. Five cognitive interviews with parents were undertaken to gain a detailed depiction of the meanings and processes they used to respond to the HLQ items. Assessment of the psychometric properties of the revised HLQ was undertaken using data from a cross-sectional survey of 254 parents of children with epilepsy. Analysis included internal consistency (Cronbach’s alpha) and confirmatory factor analysis (CFA).
Results:
Some 22 out of 44 items and the names of three domains were modified (e.g. attribution changed from ‘me’ to ‘my child’). Cognitive interviews indicated that parents interpreted the HLQ-Parent items in the way intended. All but three factor loadings were high to acceptable. All nine HLQ scales showed satisfactory to good internal consistency (Cronbach’s alpha 0.70 to 0.87). When fitting one-factor CFA models, correlated residuals were required for four scales to generate an acceptable fit. One scale, ‘8. Ability to find good health information’, required inclusion of two correlated residuals to generate an acceptable CFA model fit, indicating that further work on this scale is warranted.
Conclusions:
The results from both the adaptation process and the CFA analysis supported the relevance, understanding and theoretical structure of the instrument in a parental context.
Keywords
Background
Epilepsy in childhood is a chronic disease characterised by unprovoked seizures that can have a significant impact on a person’s emotional, cognitive and social development and functioning [1]. Hence, many children with epilepsy are at increased risk of unsuccessful school experiences [2]. In childhood epilepsy, parents are expected to participate in their child’s healthcare. This may involve administering complicated treatment regimens (e.g. diet, medication), addressing their health needs, and navigating the different parts of the healthcare system [3]. Parents’ health literacy – that is, their ability to access, understand, remember, critically assess, and use health information and services to achieve successful collaborations with healthcare providers – is crucial to their child’s health [4]. Health literacy is a contextual and dynamic phenomenon, since factors such as stress and the complexity of treatments and services can affect health literacy. This is a salient point in complex medical conditions such as childhood epilepsy, as chronic stress is known to frequently affect the parents [5].
In a recent scoping review [6] on pathways linking parental health literacy with health behaviours directed at the child, researchers found that the most prominent pathway was a direct association. Variables considered to be mediators were self-efficacy, attitudes, beliefs and education. However, the review found an apparent lack of theoretical models to illuminate these pathways. An article on the relationship between parental health literacy and the health outcomes of children with medical complexity [5] underscores this knowledge gap and the need for novel research to examine the relationships between communication, healthcare delivery and the accessibility of the healthcare system for which parental health literacy is likely to be essential.
There is growing evidence that health literacy challenges in parents are associated with several poor health outcomes in children, including medical errors [7]. However, less is known about the relationship between parental health literacy and the health outcomes of children with medical complexity, for instance childhood epilepsy [6]. A study by Paschal et al. [3] showed that higher health literacy was associated with fewer missed medication doses and seizure frequency. Health literacy was estimated through parents’ confidence in filling out forms, understanding health information, and whether they needed help with reading [3]. In another study investigating the same topic [8], a 17-item public health literacy knowledge scale was used, and the caregivers’ health literacy knowledge was found to be associated with adherence to antiepileptic drugs. A third study [9] aimed to evaluate the content, quality, useability and efficacy of a web-based epilepsy education programme developed for youth with epilepsy and their parents. The results showed the positive effects of ehealth literacy, among other outcomes. In this study, ehealth literacy was measured by eHEALS [10].
Although several instruments have been developed to measure health literacy, there are important distinctions to consider when measuring health literacy related to caregiver roles compared with parents’ own health literacy. Children with medical complexity, such as epilepsy, are especially dependent on their parents’ skills and ability to conduct tasks related to understanding and critically assessing health information, to navigate the healthcare system, and to achieve successful collaboration with healthcare providers [6]. To achieve a broader and more in-depth knowledge about these tasks and skills, parental health literacy needs to be evaluated by comprehensive instruments that incorporate the full multidimensional nature of health literacy [11].
Few instruments provide specific information on the full range of health literacy elements for public health planning and clinical practice. To the best of our knowledge, parental versions of such instruments are sparse and cover a limited range of dimensions [11-14]. The Health Literacy Questionnaire (HLQ) is a generic, comprehensive instrument that measures health literacy. Originally developed using a validity-driven approach [15-18] in Australia by Osborne et al. [16], it has since been applied and tested in many countries and languages. The HLQ was designed to detect a wide range of health literacy strengths and needs, and to be used for a variety of purposes, such as describing the health literacy needs of populations in national health surveys, informing fit-for-purpose health literacy actions and interventions, and measuring outcomes of public health and clinical interventions designed to improve health literacy [16,18]. For these reasons, the HLQ was identified as a potentially useful tool to illuminate parental health literacy in childhood epilepsy and other parental contexts.
Aims
The aim of this study was to adapt the HLQ in English and Norwegian for use with parents of children with epilepsy in Norway. Qualitative (i.e. cognitive interviews) and quantitative (i.e. psychometric) analyses were undertaken to contribute evidence on the content of the parent version of the HLQ (i.e. HLQ-Parent) the response processes of the parents completing it, and its structure.
Methods
Design and sample
To adapt the HLQ [16] to a parental context, the research group discussed and came to a consensus about the changes needed in close collaboration with the HLQ development team in Australia. Five cognitive interviews with parents were performed to gain a detailed depiction of the meanings and processes used to respond to the HLQ statements. The psychometric properties of the HLQ-Parent were assessed with data from a cross-sectional survey of 254 parents of children with epilepsy obtained from two contexts:
1) parents of children with complex epilepsy admitted to a hospital in tertiary healthcare, and 2) parents of children with epilepsy that answered an identical survey on the National Epilepsy Association website from June to December 2020. In addition, data were collected on selected socio-demographic (sex, age, education and civil status) and clinical variables (duration of the child’s epilepsy, number of hospitalisations, comorbidity and self-assessed health status). The research was approved by the Norwegian Centre for Research Data (#187824) and the department for the security of sensitive information in the study site hospital (#20/07884). The study was conducted in accordance with the Declaration of Helsinki.
The adaptation processes
The HLQ had previously been translated and tested in the Norwegian context and used with many different populations in Norway [19,20]. The HLQ comprises 44 items representing nine independent health literacy domains. Each domain comprises four to six items. Items are scored from 1 to 4 in the first five scales (Strongly Disagree, Disagree, Agree, Strongly Agree), and from 1 to 5 in the remainder (Cannot Do or Always Difficult, Usually Difficult, Sometimes Difficult, Usually Easy, Always Easy) [18]. The domain scores are calculated as the average of the item scores, higher scores indicating better health literacy. For further information on the domains, content and keywords of the generic HLQ see Table I [19].
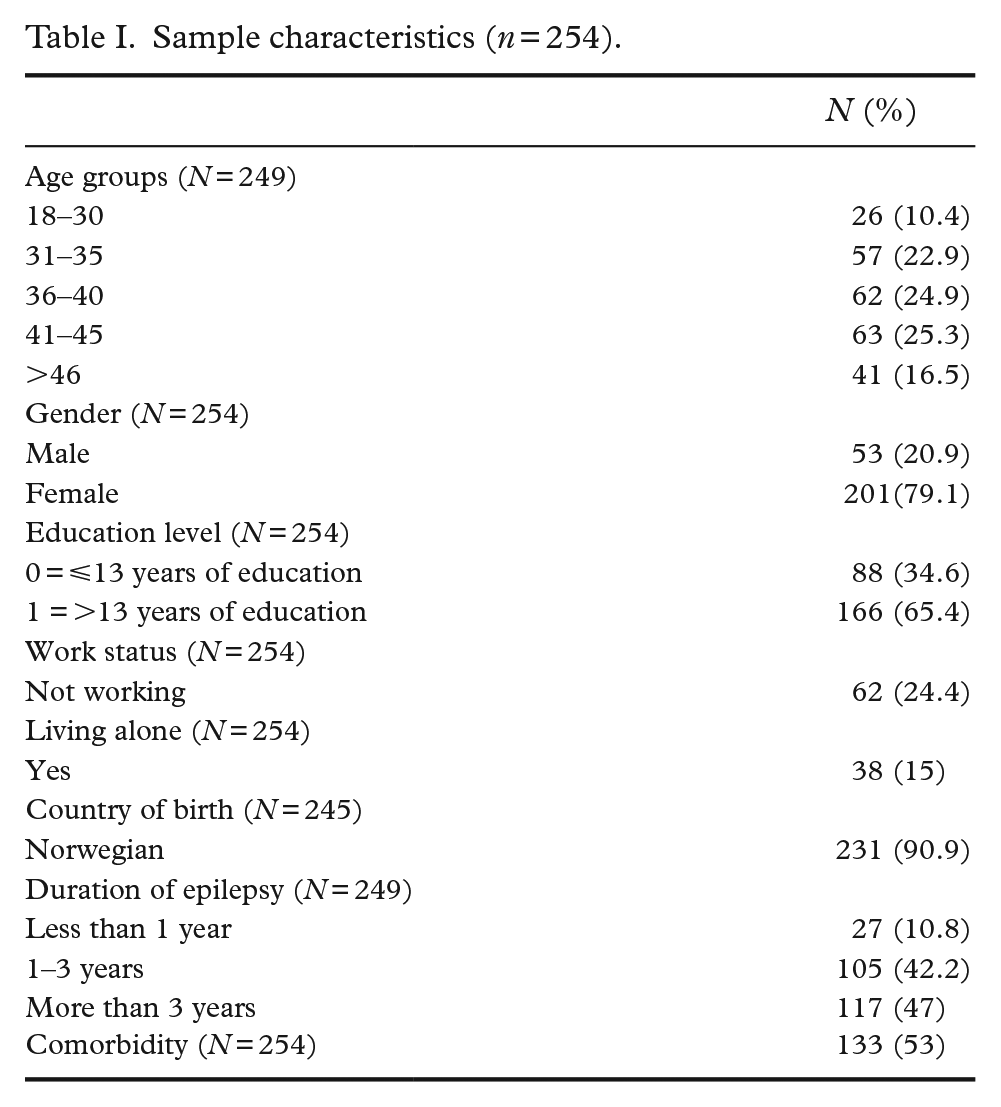
Sample characteristics (n = 254).
The process of adapting the HLQ to parents was as follows. Authors MKT, MHL, RJ and AKW (representing various backgrounds related to the healthcare of children with medically complex conditions and health literacy measurements) reviewed the HLQ and assessed what changes were necessary to orient the form towards children’s health for both the Norwegian and English versions of the HLQ. After reaching consensus in the group, the changes suggested were submitted to the developers of the HLQ (author RHO) and the Translation Integrity Protocol[17] was used to evaluate and coordinate comments, corrections and to facilitate consensus. Five cognitive interviews with parents were conducted. The parents were recruited from the Norwegian National Centre for Epilepsy. Each parent completed the HLQ-Parent version and was subsequently independently interviewed. The interviewer (MBT) assessed whether the parents understood the HLQ-Parent in the way that was intended (referenced against the item intent detailed in the management grid of the Translation Integrity Protocol). Furthermore, each parent’s response process was assessed, that is, the underlying process that led to their particular understanding of each question and answer. Qualitative questions included, ‘what was your first reflection of the item, and what made you answer the way you did?’. After the cognitive interviews, the research group discussed the parents’ comments and their consensus into the management grid. Two blinded translators – one authorised translator and one native English speaker fluent in the Norwegian language – independently back-translated the HLQ-Parent into English. The items of this version were ultimately approved by the questionnaire developers.
Data analysis – confirmatory factor analysis
Analyses were carried out using Stata v16 (StataCorp, College Station, TX). Descriptive analyses were undertaken and Cronbach’s alpha was calculated to investigate each scale’s internal consistency with Pearson’s r being used to estimate interscale correlations. As the structure of the original HLQ is established [16], the factor structure was specified a priori. Confirmatory factor analysis (CFA) was therefore employed to investigate the structure of each scale. Overall, the amount of missing data per HLQ item was low with an average of 0.78% of respondents having missing values on one of the nine HLQ scales. Maximum likelihood was applied for model estimation. Model evaluation was based on chi-square tests for model fit and additional model fit indices, including the root mean square error of approximation (RMSEA), comparative fit index (CFI), the Tucker–Lewis index (TLI) and the standardised root mean square residual (SRMR). For model fit to be interpreted as acceptable, an RMSEA of <0.05 was considered a close fit, while an RMSEA and an SRMR of up to 0.08 were considered acceptable. Comparing the fit of a target model to that of an independent or null model, the CFI has a cut-off for good fit of ⩾0.90. A TLI of 0.95 indicates the model of interest improves the fit by 95% relative to the null model; the cut-off for good fit was therefore set at TLI ⩾0.95 in the current study. Furthermore, the presence of correlated residuals among one-factor models was considered. Correlated residuals <0.2 were considered acceptable when fitting the models [21,22]. Potential model adjustments were based on modification indices, as provided in the Stata output using the ‘estat gof, stats (all)’ command. To obtain information on potential problematic items, nine 1-factor models were fitted to the data. To test whether modifications, in terms of correlated within factor residuals, led to significant model improvement, modification indices were obtained using the ‘estat mindices’ command in Stata.
Results
Sample characteristics (cognitive interviews)
Five cognitive interviews (three fathers, two mothers) were conducted with parents who broadly represented those of children with epilepsy (high/low education, residence, language, culture, age, gender).
Cross-sectional survey sample characteristics
The characteristics of the sample who provided data for the psychometric analysis are shown in Table I. The sample consisted of 79% women, 73% of whom were between 31 and 45 years of age. Over 90% were Norwegian born. Sixty-five per cent of the parents had completed higher education in addition to primary and secondary school, and 76% were working either full- or part-time. Forty-seven per cent reported their child’s disease duration to be more than 3 years. The proportion of children with one or more comorbidities was 53%.
Revisions made to the Health Literacy Questionnaire to generate a parent version
Twenty-two of the 44 items and the names of three of the original domains were changed as a result of the adaptation process. The changes made were to items and domains containing wording related to ‘my health/situation’ and renamed as ‘my child’s health/situation’. The revised domain names were 1. Feel that healthcare providers understand and support my child’s situation, 2. Having sufficient information to manage my child’s health, and 3. Actively managing my child’s health.
The cognitive interviews
The parents were observed to interpret the HLQ-Parent as intended when their interpretations of the items were matched against the item intent. In addition, they understood that the questions were directed towards their child’s health and healthcare support, not their own health. However, the cognitive interviews revealed some specific information on the content of the questionnaire. The parents understood the questions about health information regarding their child to be general health information, but also specific information about the child’s diagnosis that was necessary to adequately care for their child’s epilepsy. General information covered nutrition, being physically active, and getting enough sleep. Information about the child’s diagnosis included, for example, receiving adequate information to follow the recommended treatment. Specific information from the parents is shown in Table II.
Cognitive interviews with parents on the content of the Health Literacy Questionnaire parent version (HLQ-Parent).
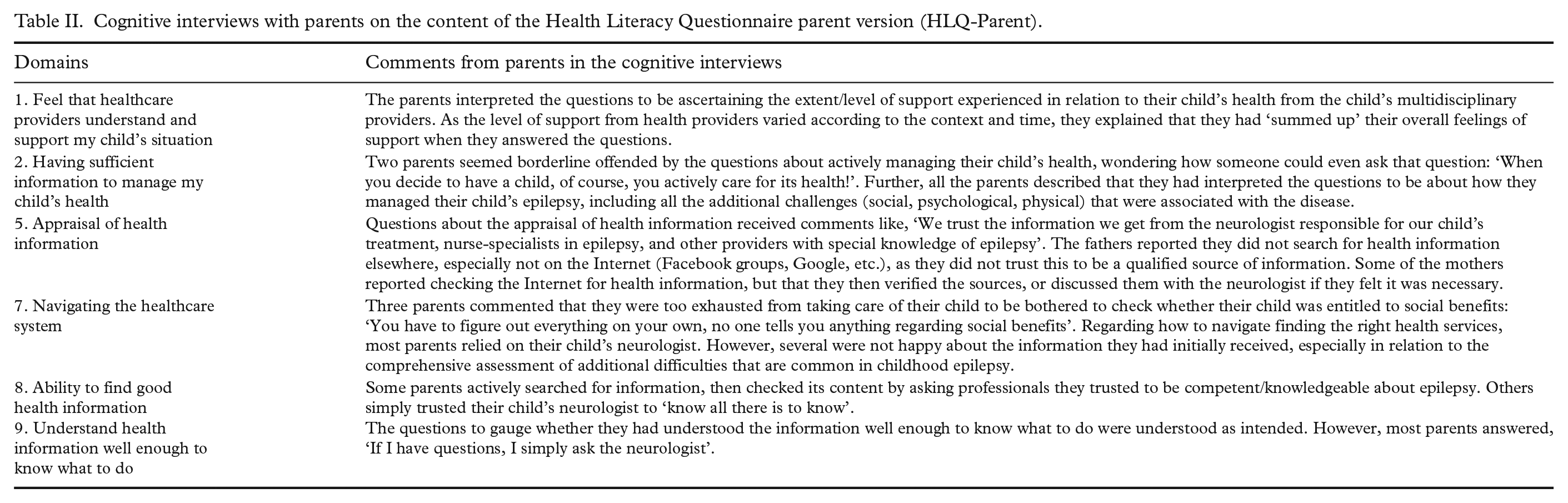
Based on the cognitive interviews, only minor grammatical adjustments were made to the questionnaire.
Confirmatory factor analysis
Nine 1-factor models were fitted to the data (see Table III). The factor loadings from the nine 1-factor models, with no correlated residuals, are shown in Table IV.
Confirmatory factor analysis and internal consistency (Cronbach’s alpha) of the HLQ-Parent (one-factor models).
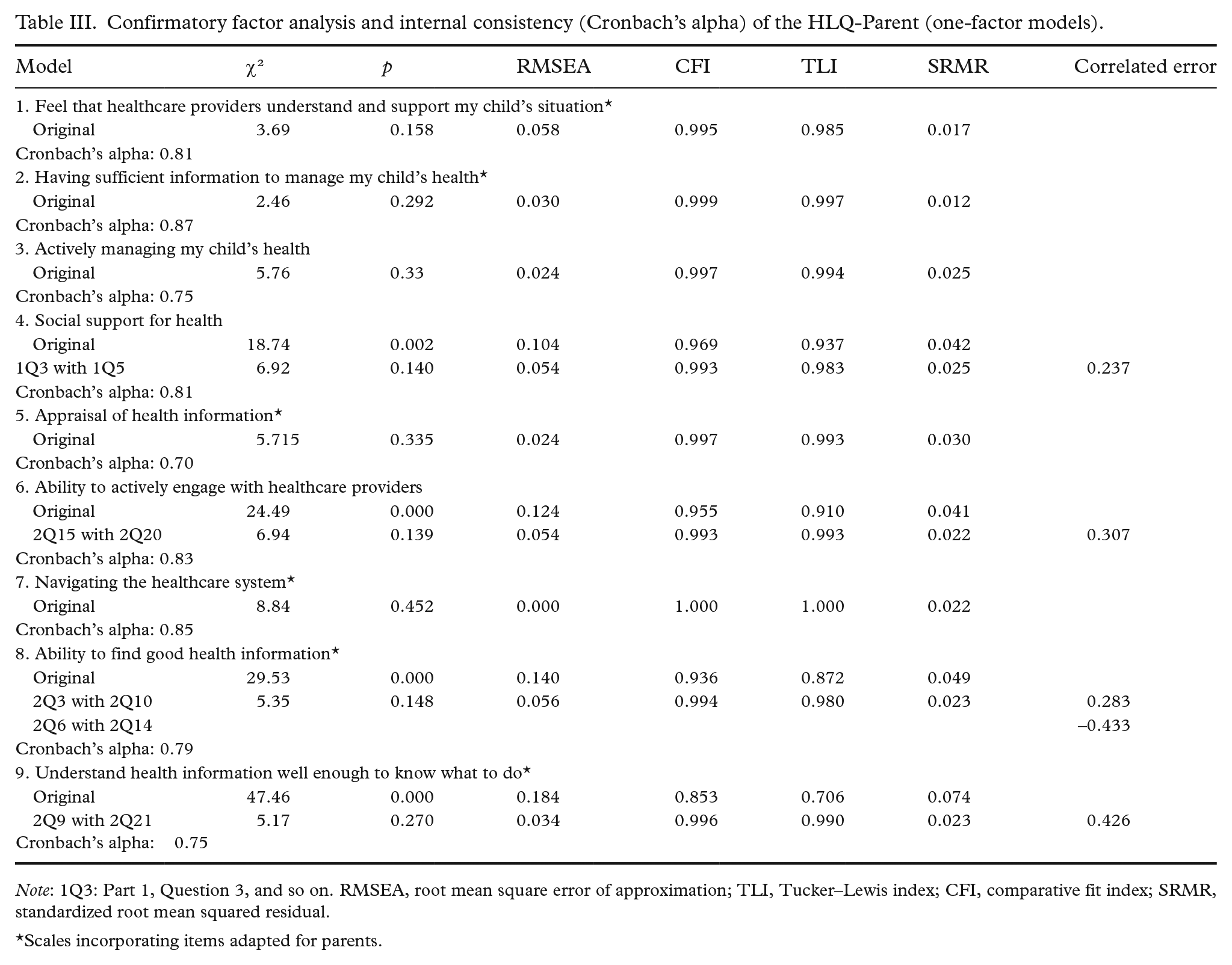
Note: 1Q3: Part 1, Question 3, and so on. RMSEA, root mean square error of approximation; TLI, Tucker–Lewis index; CFI, comparative fit index; SRMR, standardized root mean squared residual.
Scales incorporating items adapted for parents.
Confirmatory factor analysis of the HLQ-Parent, nine 1-factor models, standardised factor loadings and standard errors.
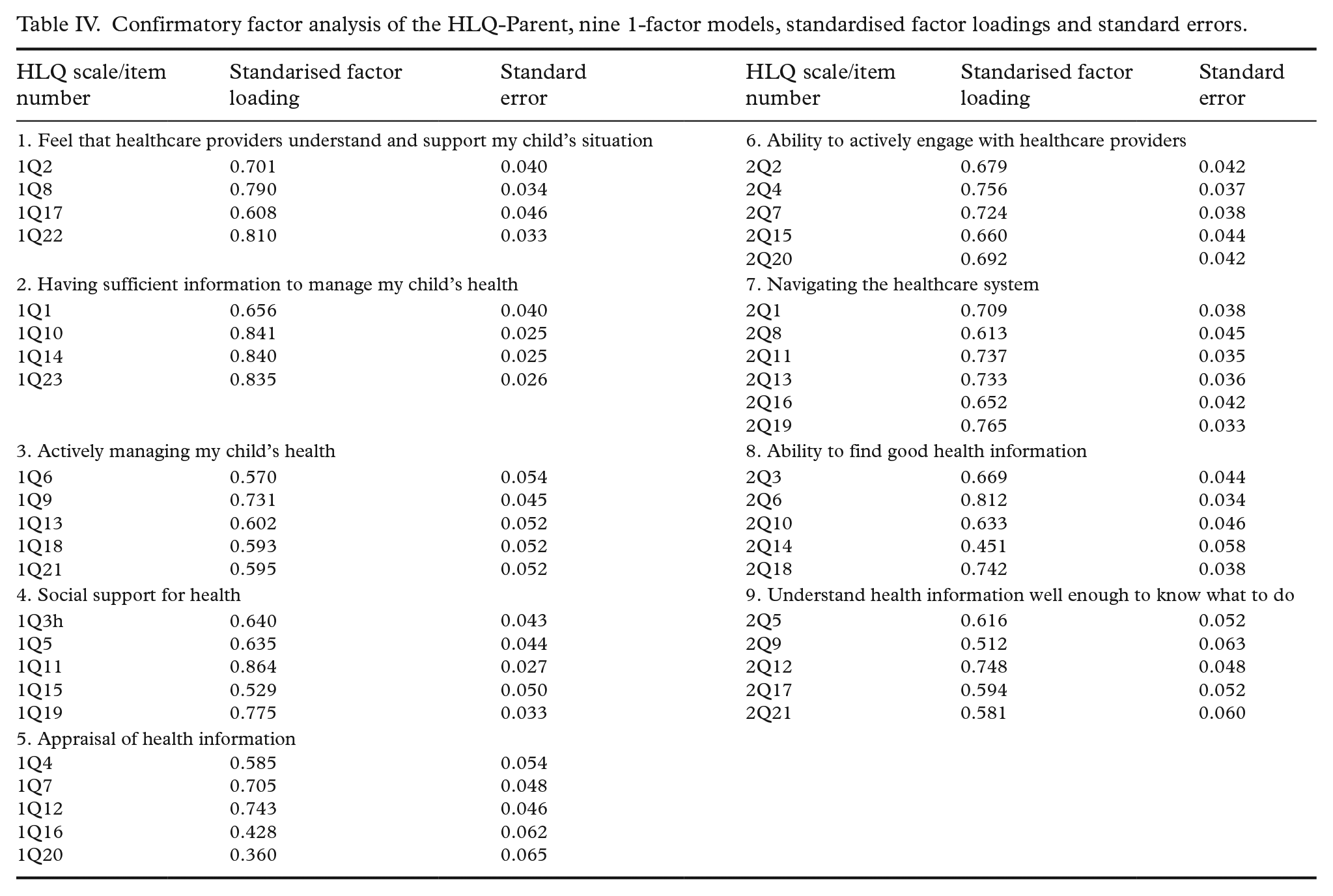
All but three factor loadings were high to acceptable (i.e. >0.5; see column headed ‘Standardised factor loading’ in Table IV); the three items that had a somewhat low loading were 1Q16 (i.e. Part 1, Question 16) (0.428) in Scale 5 (Appraisal of health information); 2Q14 (0.451) in Scale 8 (Ability to find good health information); and 1Q20 (0.360) again in Scale 5 (Appraisal of health information’). When fitting the one-factor models, correlated residuals were sequentially added, which improved each model fit significantly.
Table III shows the results of the CFAs for the nine HLQ-Parent scales. While model fit without modifications was acceptable for five scales, 1. Feel that healthcare providers understand and support my child’s situation 2. Having sufficient information to manage my child’s health, 3. Actively managing my child’s health, 5. Appraisal of health information, and 7. Navigating the healthcare system, one or more correlated residuals were observed in the remaining four scales (Domains 4, 6, 8 and 9). The correlated residuals were 0.237 for one adjustment in Domain 4: Social support for health; and 0.307 for the one adjustment in Domain 6: Ability to actively engage with healthcare providers. In Domain 8: Ability to find good health information, there were two adjustments (0.283, –0.433) and one adjustment in Domain 9: Understand health information well enough to know what to do, with a correlated residual (0.426). After the respective model adjustments, the one-factor models were acceptable. All nine HLQ scales showed satisfactory to good internal consistency, with Cronbach’s alpha ranging from 0.70 to 0.87 (see Table III).
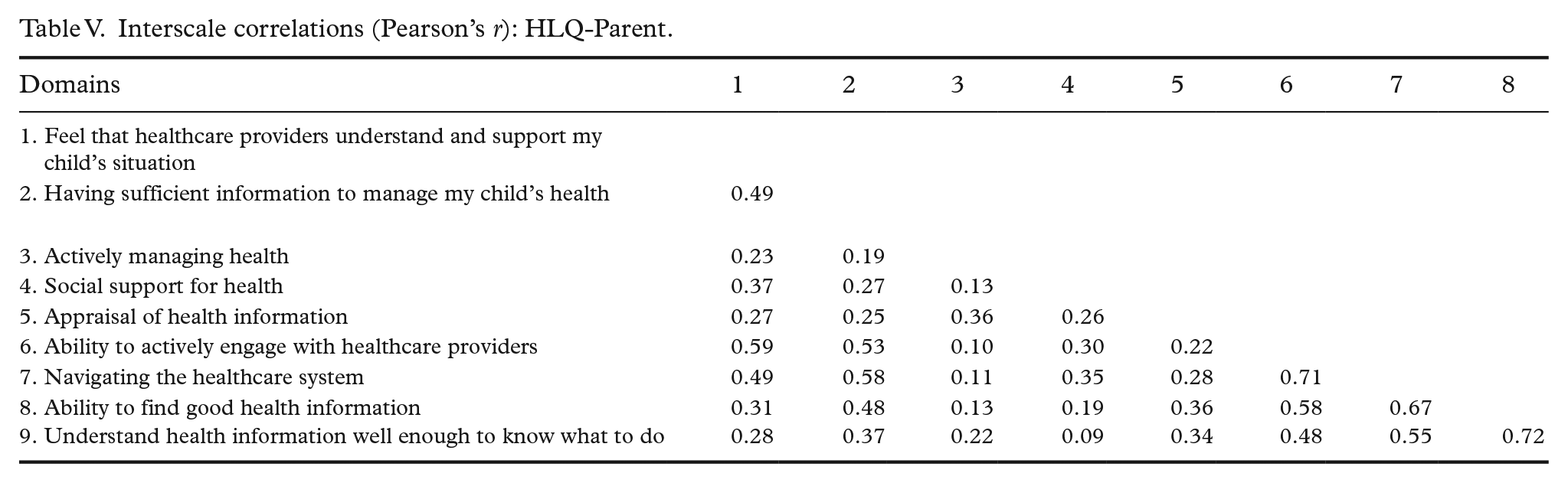
The interscale correlations of the HLQ-Parent are shown in Table V. The highest correlations were between Domains 8: Finding good health information, and 9: Understanding health information (r = 0.72), and between Domains 6: Ability to engage actively with healthcare providers and 7: Navigating the healthcare system (r = 0.71), which were modest and indicated, overall, that the scales tended to broadly measure the different constructs as intended and therefore had reasonable discriminant validity.
Interscale correlations (Pearson’s r): HLQ-Parent.
Discussion
In this paper, we have reported the adaptation process and psychometric properties of the HLQ-Parent in the context of childhood epilepsy. The results from both the adaptation process and the CFA analysis, with some adjustments, supported the relevance, understanding and coherence of nine aspects of parental health literacy derived from the well-tested and widely applied HLQ.
The adaptation process made use of thorough methods and was performed in close collaboration with the developers of the HLQ [16]. The adaptation team easily reached consensus on the wording and structure of the parental version and the participating parents were observed to interpret the HLQ-Parent the way it was intended. The parents quickly understood that the questions were directed towards their child’s health and healthcare support, not their own health.
A few other instruments measure aspects of parental health literacy, such as the PHLAT (Parental Health Literacy Activity Test) [12], the CPHLQ (Chinese Parental Health Literacy Questionnaire) [13], and the PPSI (the Parenting Plus Skills Index) [14]. The PHLAT measures functional health literacy (i.e. restricted to health-related reading and numeracy ability), the CPHLQ is limited to parents of children between 0 and 3 years of age, and the PPSI is a performance-based comprehension test. Consequently, a more comprehensive and generic measure of parental health literacy, suitable for a diversity of health literacy settings, was needed. Rather than developing a parental health literacy measure de novo, which involves extensive, highly specialised developmental work over several years, we adapted an existing widely used and well-tested measure as a starting point. This is both time- and cost-effective. Another positive element related to the adaptation of the HLQ to a parental context is the possibility of using the widely applied Ophelia (OPtimising HEalth LIteracy and Access) community co-design process to develop comprehensive health literacy-informed interventions in a paediatric setting to improve healthcare access, equity and outcomes for families with a child with medical complexity [23].
A previous validation study of the HLQ showed that the Norwegian language version replicated the original factor structure of the English version, indicating that the questionnaire has cogent, independent scales with good reliability [19]. For the HLQ-Parent, this conclusion was further supported in the context of parental health literacy. The one-model approach resulted in acceptable values for RMSEA, SRMR, CFI and TLI for five of the scales without any adjustment, and needed just one adjustment in three scales and two adjustments in one scale. The factor loadings were acceptable for all but three items. Cronbach’s alpha showed acceptable internal consistency across all scales, and interdomain correlations indicated that the scales had acceptable discriminant validity.
Strong parental health literacy is likely to improve child health outcomes through effective parental health behaviours such as optimal healthcare use, engaging in a healthy lifestyle and/or increased adherence to treatment [24,25]. The HLQ-Parent, with its multidimensional structure, capturing both strengths and challenges related to a wide range of domains, has the potential to contribute to uncovering pathways between parental health literacy and child health outcomes. Factors related to parents, health personnel and the health services, in addition to factors such as physical and emotional support, can affect children’s health outcomes. The HLQ-Parent measures several of these factors, including social support for health, ability to actively engage with healthcare providers, and navigating the healthcare system.
This research has some noteworthy strengths and limitations. As noted, we started with a widely used and well-tested multidimensional questionnaire and were therefore able to relatively quickly adjust it to provide rich information on parents’ health literacy. However, a potential weakness of the study was the population the HLQ-Parent was tested in. Because parents of children with epilepsy will have specific health-system experiences, they are unlikely to be representative of parents in the general community, however, the sample was large and the demographics were diverse. Consequently, we recommend further testing of the HLQ-Parent in diverse populations before making generalisations about the applicability of the questionnaire to the wider community. While the results of these initial psychometric tests were promising, further qualitative and quantitative work might improve the Norwegian language framing of certain items to reduce the number and size of correlated errors. Validity testing of patient-reported outcomes is an ongoing endeavour and a range of tests needs to be applied in each distinct target population [17,18]. Future analysis should examine the psychometric structure in more depth, including whether items cross load and whether the domains are sensitive to change.
Conclusions
The cognitive interviews and the range of psychometric tests applied to the HLQ-Parent have provided preliminary evidence that it is likely to be a useful health literacy tool in a parental setting. Although the instrument was developed in the context of childhood epilepsy, it is generic in nature and therefore likely to be useful in other parental health literacy applications.
Footnotes
Acknowledgements
We would like to thank the parents responding to the questionnaire and Swinburne University of Technology who provided the licence to adapt the HLQ to a parental version. RHO was funded in part through a National Health and Medical Research Council of Australia Principal Research Fellowship (APP1155125).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author R. Osborne is one of the developers of the Health Literacy Questionnaire.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.