
Abstract
Aims:
The development of effective interventions to reduce inappropriate use of antibiotics in the elderly population requires knowledge on who can benefit from such interventions. Thus, we aimed to identify and characterise antibiotic heavy users among elderly patients in general practice with respect to sociodemographic variables.
Methods:
We conducted a retrospective nationwide register-based study on all Danish elderly citizens (⩾65 years) who redeemed an antibiotic prescription in 2017. Heavy users were defined as the 10% with the highest excess use, that is, their recorded use minus the average use for their sex, age group and comorbidity level as estimated from a linear regression model. Comparative analyses of sociodemographic characteristics (civil status, employment status, urbanity, educational level and country of origin) of heavy users and non-heavy users were performed using logistic regression models.
Results:
The study population consisted of 251,733 elderly individuals, who in total redeemed 573,265 prescriptions of antibiotics. Heavy users accounted for 68% of all excess use of antibiotics. In multivariable analyses, individuals with an educational level above basic schooling, non-retired, residing in an urban municipality and being born in a country outside Scandinavia all had lower odds of being a heavy user. Widowed, divorced or single individuals had higher odds of being a heavy user compared with married individuals. Relative importance analyses showed that civil status and educational level contributed considerably to the explained variance.
Conclusions:
Keywords
Background
Since the discovery of antibiotics, we have witnessed an alarming increase in the antimicrobial resistance rate due to extensive and widespread use of antibiotics [1–3]. Despite several efforts to reduce antibiotic use and thereby curb the selection of resistant bacteria, antibiotic consumption remains high in certain patient groups [3–5]. In particular the elderly population (⩾65 years) is known for their extensive use of antibiotics, and studies have indicated both misuse and overuse within this population group [6–8]. However, knowledge on the characteristics of individuals with excess use (here referred to as heavy users) within this group is sparse. The group of heavy users carries a high risk of selection and dissemination of antimicrobial resistance and is accordingly highly relevant to identify and target in future interventions.
Several studies have shown differences in antibiotic prescribing rates in relation to age, sex and comorbidity, both at the individual and at the population level [5, 9, 10]. However, these factors cannot explain the large variation in antibiotic use among the elderly population [11]. This suggests that other factors also contribute to the variation. Sociodemographic factors have been linked to differences in antibiotic prescribing, but the evidence is contradictory and inconclusive [12–17]. For example, being a first-generation immigrant has been associated with both high and low prescribing rates and requires further exploration [12, 15].
We hypothesised that there is sociodemographic variation in the prescription of antibiotics for elderly people. Therefore, we aimed to examine the association between sociodemographic factors and heavy users in the elderly population in Danish general practice. To do so, we conducted a retrospective nationwide study on all Danish elderly people who redeemed an antibiotic prescription. We identified heavy users after taking account of sex, age and comorbidity, as these variables are known to influence antibiotic consumption [5, 18]. Subsequently, we compared sociodemographic variables in heavy users versus non-heavy users. Knowledge of patient-related sociodemographic characteristics of heavy users could complement the current efforts to reduce overuse and misuse of antibiotics within the elderly population and guide future interventions.
Methods
In this study, we included all elderly people in Denmark (aged ⩾65 years on January 1, 2017) who redeemed an antibiotic prescription from general practice in 2017. According to the anatomical therapeutic chemical (ATC) classification system, antibiotic prescriptions were defined as ATC code J01: antibiotics for systemic use and P01AB01: metronidazole. Data on antibiotic prescriptions were collected from the Danish National Prescription Registry (DNPR), a national database containing data on all prescriptions redeemed at outpatient pharmacies in Denmark since 1995. In this database all individuals who redeem an antibiotic prescription are identified by a unique personal identification number, enabling linkage with other Danish registries.
Patients were excluded from the study if they had missing information about age and sex, as these were regarded as tourists or administrative entries. Patients were likewise excluded if they immigrated to Denmark later than 2015 or if they died during 2017.
In a first step, heavy users were identified relative to their expected use, and in a second step, sociodemographic variables were compared between heavy users and non-heavy users.
Identification of heavy users
In this study we defined heavy users as individuals who received more antibiotics than expected given the individual’s sex, age and comorbidity. To identify heavy users, we first modelled the expected antibiotic use using a multivariable linear regression model of sex, age, number of hospital admissions and hospital admission days (the latter two as a measure of general morbidity) on the number of prescriptions in the year 2017. The explanatory variables were chosen to reflect factors associated with antibiotic use known from previous studies [3, 15, 18, 19]. To avoid overly influential outliers in data, the regression method employed was a robust regression with M-estimation using Huber’s weight function [20].
We then ranked the residuals of the model in ascending order. A residual is the difference between the expected use (predicted by the model) and the actual antibiotic use for the given individual. Individuals with a negative residual had a lower (actual) use than predicted by the regression model, while individuals with a positive residual had a higher use of antibiotics than predicted by the model, that is, an excess use.
Finally, we identified heavy users as the top 10% of individuals with the highest excess use, that is, the top 10% with the largest positive residuals.
Lorenz curve
To visualise the distribution of the excess use of antibiotics, we constructed a modified Lorenz curve on which we placed the cumulative share of residuals (y axis) and the cumulative share of the study population (x axis). As some individuals have a lower use than predicted, that is, a negative residual, these values were set to zero to reflect the distribution of the excess use of antibiotics.
Sociodemographic factors
Data on civil status, employment status, urbanity, educational level and country of origin were retrieved from Statistics Denmark.
Civil status was grouped into a four-level variable: married, divorced, widowed and single. All levels included the equivalence of civil partnership.
In the registries, employment status is based on an individual’s main income source and employment status. In the present study, the following groups were constructed based on these variables: retiree, employee and self-employed. Cash benefit recipients, individuals under education and ‘others’ were grouped as retirees.
Denmark consists of 98 municipalities and they were grouped into three groups according to their degree of urbanity, based on the size of the largest city in the municipality: fewer than 30,000 citizens (rural), 30,000–100,000 citizens (metropolitan) and more than 100,000 citizens (urban).
Highest achieved educational level was grouped as follows: basic schooling (⩽10 years), secondary education (11–13 years), vocational education (10.5–15.5 years), short and medium higher education (13–17.5 years), and graduates, long higher education and researcher education (14–22 years). Individuals with missing values were grouped as ‘no information’.
Country of origin was grouped into four categories: individuals born in: (a) Denmark; (b) Sweden or Norway; (c) Europe (except Norway and Sweden); and (d) others (including individuals with missing information on country of origin).
Sociodemographic characteristics of the study population were compared between heavy users and non-heavy users in logistic regression models, both separately in univariable models and jointly in multivariable models (including only those characteristics that were significant in the univariable analyses). The importance of the sociodemographic variables relative to each other was calculated as the percentage of the variance explained by the full multivariable model attributable to each of the sociodemographic variables [21]. All analyses were stratified by sex. For odds ratios, 95% confidence intervals not including one were considered statistically significant.
All data management and statistical analyses were performed using SAS Software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
We identified 282,562 elderly people aged 65 years and older who redeemed 595,781 prescriptions of antibiotics in 2017. Of these, 17,577 died during 2017, 13,102 were excluded due to missing data on age and sex, and 150 individuals were excluded because they immigrated to Denmark later than 2015, yielding a study population of 251,733 elderly individuals, who in total redeemed 573,265 prescriptions. The mean age of the study population was 75.6 years (interquartile range (IQR) 69–81), and 62.1% were women. The median prescription rate was 1 (IQR 1–2) prescription per year.
The distribution of the excess use of antibiotics (i.e. the positive residuals) is visualised in Figure 1 and shows that 40% of the study population was driving the excess use. This means that 60% of the study population used less than or equal to the predicted amount of antibiotics for an individual with the given characteristics. The figure also shows that the top 10% of the study population (i.e. the heavy users) was responsible for 68% of the excess use of antibiotics.
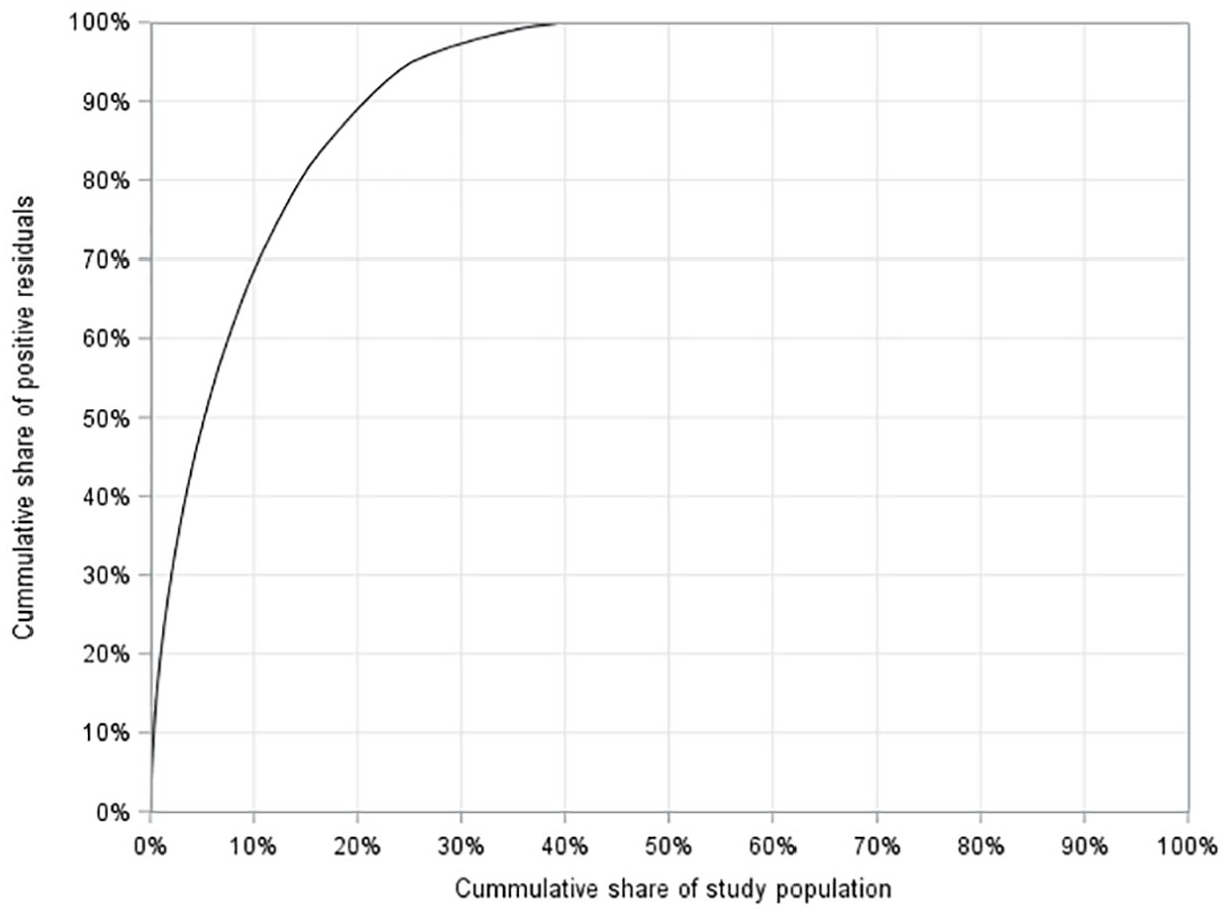
Lorenz curve illustrating the distribution of the excess use of antibiotics (positive residuals) from the robust regression model of antibiotic prescriptions.
Ranking the residuals from the robust regression model, the individuals were divided into heavy and non-heavy users. This yielded a group of 25,024 heavy user individuals (9.9% of the study population) consisting of 17,000 women and 8024 men. The general characteristics are presented in Table I.
General characteristics of heavy users and non-heavy users stratified by sex..
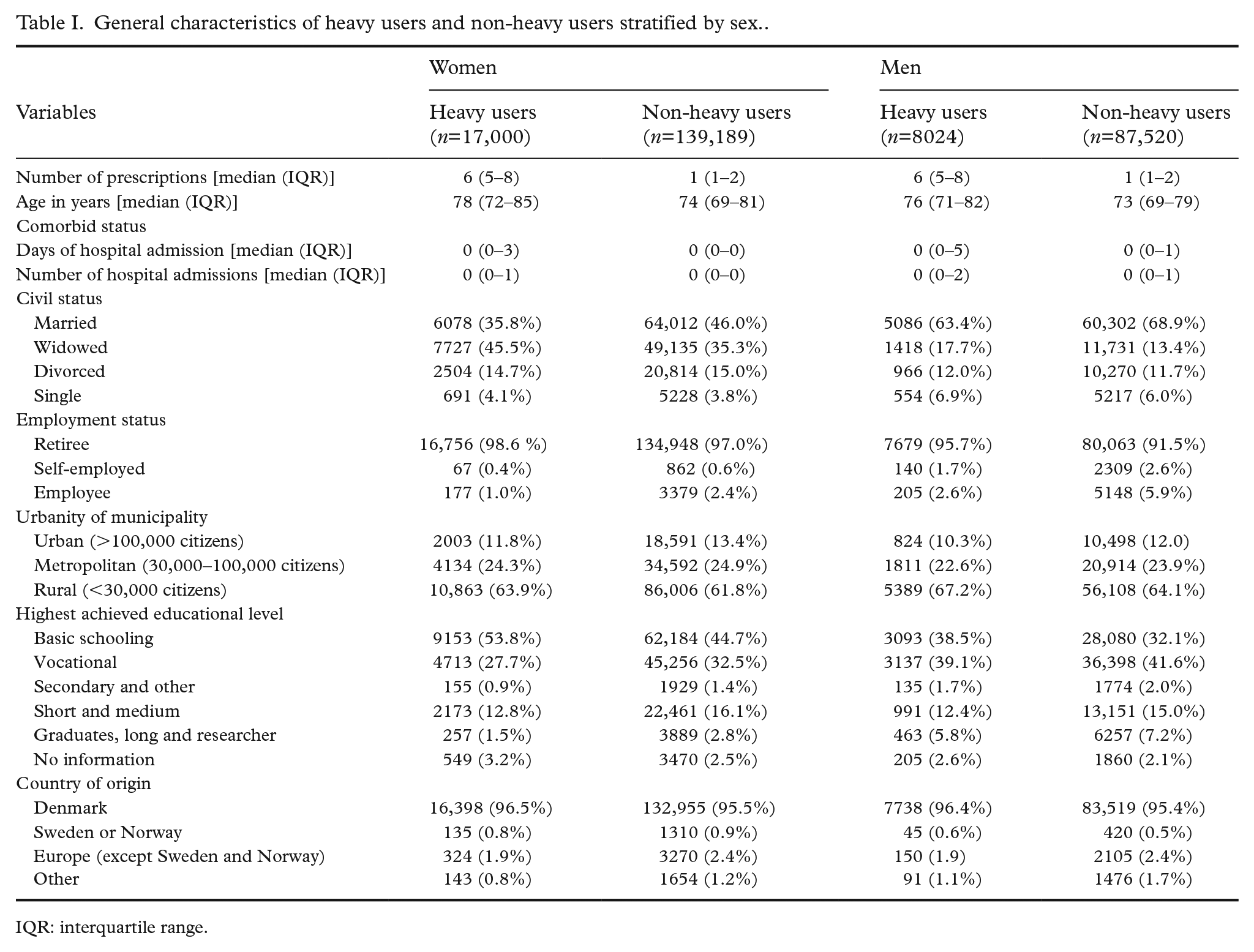
IQR: interquartile range.
The results of the univariable and multivariable logistic regression analysis are presented in Table II. All tested variables were included in the multivariable logistic regression analysis. The univeriable and the multivariable analysis gave similar odds ratios for all the tested sociodemographic parameters. For both sexes, being widowed, divorced or single significantly increased the odds of being a heavy user compared with married individuals. On the contrary, living in an urban municipality marginally decreased the odds for both sexes. All higher educational levels also decreased the odds of being a heavy user compared with individuals with basic schooling. The self-employed and employees had significantly lower odds of being a heavy user compared with retirees. Being born in countries outside Scandinavia (Denmark, Norway and Sweden) likewise lowered the odds of being a heavy user.
Multivariable analysis of sociodemographic factors and heavy use of antibiotics stratified by sex.
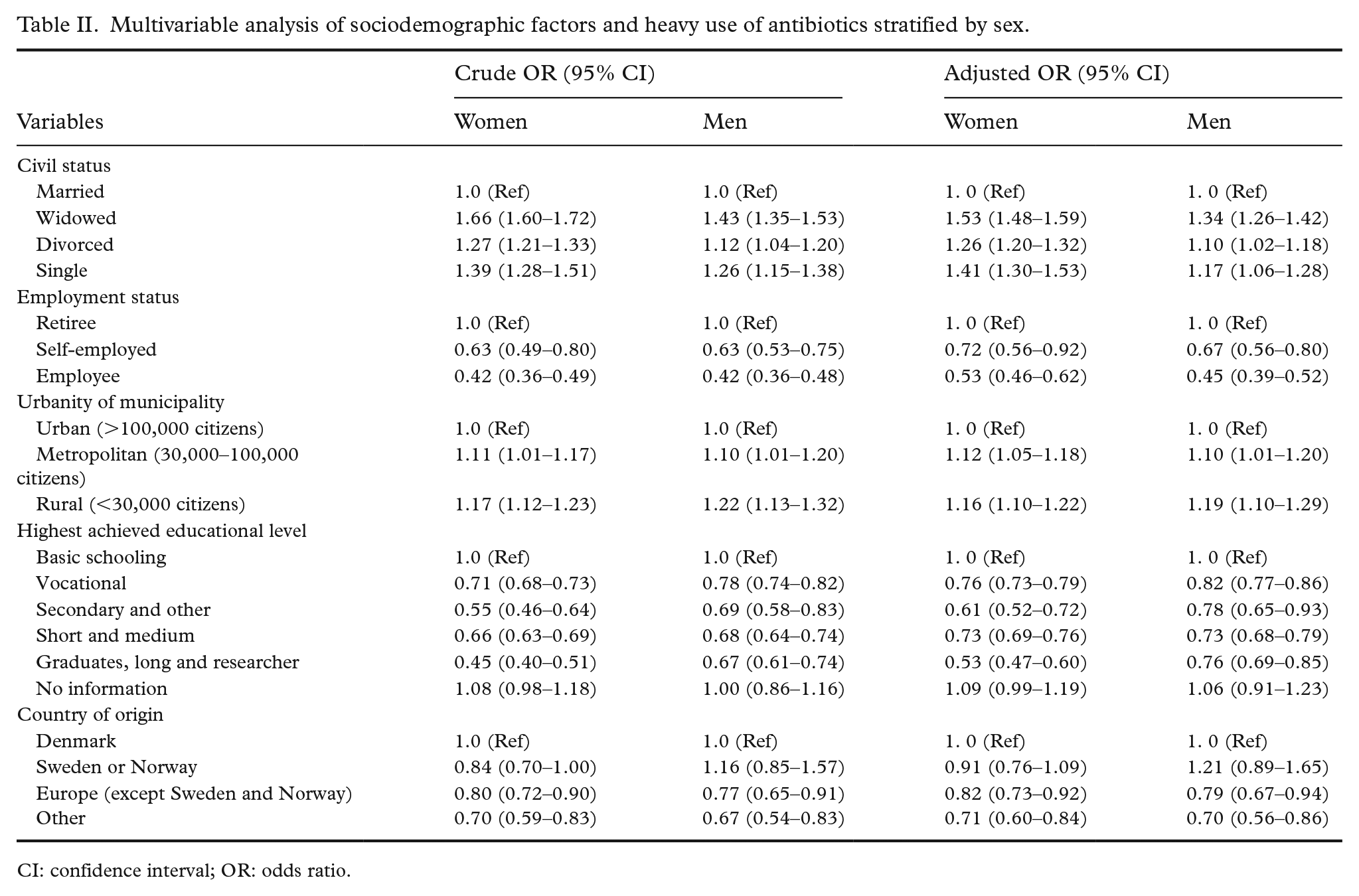
CI: confidence interval; OR: odds ratio.
The results of the analysis of relative importance are shown in Figure 2. For both sexes, civil status and educational level contributed considerably to the explained variance. For men, employment status was also an important factor.
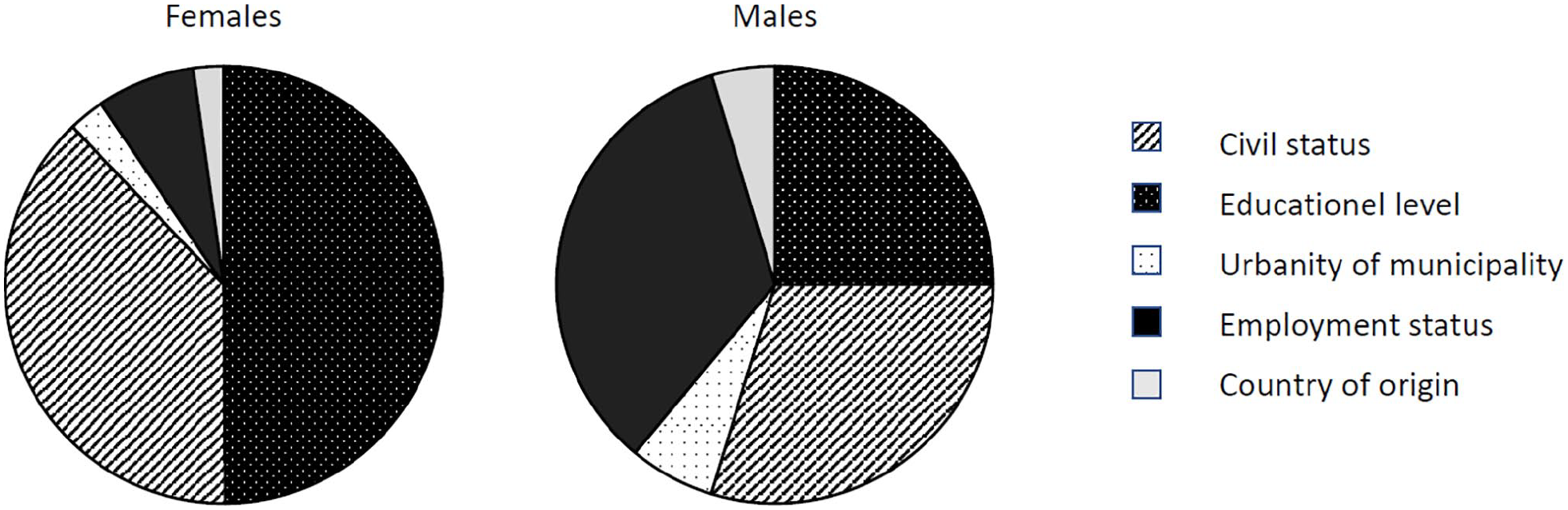
Relative importance analysis of the explained variance.
Discussion
Our findings showed that several sociodemographic factors were associated with the excess use of antibiotics among the elderly population in Denmark. We found that the heavy users were responsible for 68% of the excess use. Overall, not being married and living in metropolitan and rural municipalities increased the odds of being a heavy user. However, being part of the workforce (i.e. self-employed or employee) decreased the odds. Educational level beyond basic schooling and birth countries outside Scandinavia (Denmark, Norway and Sweden) lowered the odds of being a heavy user. The relative importance analysis showed that civil status and educational level contributed considerably to the explained variance for both sexes. For men, employment status was an important factor as well, but this did not apply to women.
Strengths and limitations
The present study has some strengths and limitations that need to be taken into consideration when interpreting the results. A strength of the study is that it is a nationwide study with a large sample size and the completeness of the data used in the analysis. The DNPR data are regarded as having high completeness and validity [22]. It should be noted that antibiotics are available only by prescription in Denmark, and over-the-counter sale is illegal. Another strength of our study is that we modelled the excess use of antibiotics and not crude prescribing rates. When identifying heavy user individuals, we were thus able to take into consideration that some individuals with certain health conditions would reasonably receive more antibiotics for medical reasons. Finally, we chose to measure antibiotic use as the number of prescriptions, as this is a reliable measurement, especially in settings with no over-the-counter sales [23].
Furthermore, all residents in Denmark have the right to choose a general practitioner (GP) close to their place of residence, and access to the services are free of charge at the contact point as the healthcare system is tax funded. To a large extent this guarantees equal access to healthcare across socioeconomic classes, hence bias due to different healthcare access is unlikely.
The limitations of the study include the fact that we excluded all individuals who died in 2017. This could bias our results as a high use of antibiotics in the end-of-life stage has been observed [24]. At the same time, these individuals often have less exposure time in general practice due to frequent hospital admissions. Thus they could have a falsely low use of antibiotics. Many complex and still unexplored mechanisms may drive end-of-life use of antibiotics, which we could not consider in the present work. To avoid these potential biases, we chose only to examine individuals who were still alive at the end of the study period.
In this study we used hospital admission data to adjust for comorbidity level. This could potentially underestimate the degree of disease for some individuals included in the study if their morbidity did not require admission to hospital. This would, in turn, bias the results due to residual confounding and should be taken into consideration when interpreting our results. However, a post hoc analysis showed that our results were robust. The inclusion of all ambulatory care visits to hospital in the regression analysis identifying heavy users did not change our results (data not shown).
Another reason to adjust for hospital admission is the fact that we have no knowledge of antibiotics received within this setting. Some individuals may have received considerable amounts of antibiotics during hospital admissions and when discharged, which could result in a lower antibiotic prescribing rate from general practice for these individuals. Subsequently, individuals with long hospital admissions have less exposure time in general practice. Finally, we did not have data on lifestyle factors known to influence antibiotic prescribing, such as smoking habits, and hence were not able to adjust for these factors.
Findings in relation to other studies
Several studies have shown that lower educational levels are associated with high antibiotic use in the general population [12, 14]. In line with this, we found that increasing educational level was inversely associated with the risk of being a heavy user in a purely elderly population.
A review on patient-related determinants of antibiotic use by Zanichelli et al. [12] showed that being a first-generation immigrant was associated with high antibiotic prescribing rates. Contrary to this, we found a protective effect of a non-Scandinavian (all other than Denmark, Norway and Sweden) birth country on the odds of being a heavy user. Our finding is in line with a Swedish study by Ternhag et al. [15]. There may be several potential explanations for this: either this group less often consults their GP and more often is directly admitted to hospital (and hence will receive antibiotic treatment at this level of care which is not registered in the DNPR), or this group could tend to receive antibiotics from other sources, for example, self-medication, which is more common in some cultures [25, 26]. On the other hand, being born outside Scandinavia could also simply be a protective factor against being an antibiotic heavy user among elderly people.
Our data only indicated a marginal difference between different degrees of urbanity. However, Denmark is a small country with short distances and, in general, socioeconomic and geographical differences are minor compared with other countries. A UK study from 2018 by Mölter et al. [27] illustrated an association between hot and cold spots of antibiotic prescriptions (i.e. places with high and low antibiotic prescribing rates, respectively) and socioeconomic factors at area level using a spatial cluster analysis. The study indicated that socioeconomic factors are indeed both related and inversely related to the level of antibiotic prescribing by GPs. As a GP’s prescription pattern can affect the risk of antibiotic prescription for any patient registered at the GP practice, this may also influence the risk of being a heavy user. However, we were not able to specify whether the patients were registered with a high or low prescribing GP practice or area, but this could be relevant to study in future research.
Conclusions
Despite several initiatives to reduce antibiotic use targeting general practice, few have focused specifically on heavy users within the elderly population. With increasing knowledge on antibiotic heavy users among elderly people, we hope that the knowledge obtained can help guide future interventions targeting this group. Our study shows that despite adjusting for age, sex and previous hospitalisation, a sociodemographic variance was present in antibiotic prescribing in the elderly population. Heavy users more often live alone or are individuals with a low educational background and/or not working. This knowledge could help guide GPs to become aware of potential heavy users. However, further studies are needed to explore how to intervene in this specific population group, and how to target antibiotic use without increasing mortality in this, in many ways, vulnerable group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Velux Foundation.
Ethical considerations
In compliance with European data protection rules, the University of Southern Denmark (the lawful owner of the data used in the study) approved the data work related to this study. This study is part of a larger scale study approved by the Danish National Health Data Board and the Danish Patient Safety Authority. According to Danish law strictly register-based studies do not need approval from an ethics committee.