
Abstract
Aims:
Cervical cancer (CC) over-screening has been understudied in Europe, yet is relevant for approaching inequalities in screening uptake. Focusing on countries’ screening strategies (opportunistic systems versus organised programmes), we assess in which contexts CC over-screening is more prevalent, and which women are more likely to have engaged in cervical cancer screening (CCS) within the past year.
Methods:
A two-level (multilevel) design among screening women (N = 80,761) nested in 31 European countries was used to analyse data from the second wave (2013–2015) of the European Health Interview Survey. We focused on over-screening, defined as screening more frequently than the three-yearly screening interval prescribed in the European guidelines – that is, having screened within the past year.
Results:
Higher levels of over-screening were observed in opportunistic systems compared to systems with organised programmes. In opportunistic systems, women with a higher socioeconomic position had a higher likelihood of being screened within the past year than their socioeconomic counterparts. Moreover, these differences diminished under organised programmes.
Conclusions:
Keywords
Introduction
Cervical cancer screening (CCS) by Pap smear has the benefit of early detection and prevention from death [1,2]. However, it also may potentially cause harms due to overdiagnosis, leading to unnecessary further testing (e.g. repeated Pap smears, colposcopies, biopsies) and overtreatment (e.g. conisations, later treatment, cryotherapy), particularly in contexts with short screening intervals [3,4]. These activities may be harmful, especially since the risk of preterm birth is significantly higher after conisation [5]. Considering these individual consequences, and to ensure adequate use of public health resources, European guidelines recommend that the three-yearly screening intervals should be enforced amongst 25–64-year-old women through organised screening programmes [1,6–8]. As the current research focuses on the screening interval, we define CC over-screening as engaging in Pap smear screening more frequently than recommended by European screening guidelines (once every three years). Despite limited data availability, estimating CC over-screening is crucial, because of its shown detrimental consequences [9,10]. We use a proxy indicator of cervical cancer (CC) over-screening at population level.
Whereas previous research on CCS has mainly focused on individual-level characteristics related to participation in CCS [2], recent studies have also incorporated the institutional level, paving the way to assess the context-dependency of the relationship between individual characteristics and preventive healthcare participation [11,12]. More specifically, as the adherence to the European recommendation on organised population-based CCS programmes varies across countries [1], previous literature on CCS uptake has focused on the screening strategy countries may use to implement those guidelines [7]. Some European countries have already fully implemented organised screening programmes, while others have not. These cross-national differences are captured in terms of organised versus opportunistic screening. In organised systems, screening-eligible women are systematically identified and personally invited to screen on a regular base, whereas in opportunistic systems CCS is left to the initiative of physicians and women [1]. However, even in organised systems, opportunistic screening may still take place outside the framework of the programme [13]. Whereas opportunistic cervical screening has been previously connected to a high level of over-screening [1,6,14], a comparison of over-screening in relation to the screening strategy has not been made in a European context, which this study complements.
Furthermore, the literature on CCS participation has predominantly focused on reasons for non-compliance to the screening recommendations, with the goal of improving women’s adherence to such recommendations and increasing screening uptake [2,15]. However, little is known about women on the other side of the spectrum, who screen more than the recommendations prescribe [16,17]. To complement this gap, in the current research we focus on women who participated in CCS within the recommended three-yearly time frame, and, among those screened women, assess which women were more likely to have screened within the past year.
Building on this framework, this study is the first to (1) assess over-screening from a cross-country institutional comparative perspective in Europe, and to (2) study the profile of women more susceptible thereto. In the following sections, we differentiate between (1) which institutional contexts may lead to over-screening, and (2) which individual factors are associated with a higher probability of over-screening.
Background
Contextual differences in CC (over)-screening
In opportunistic screening systems, compared to organised systems, higher levels of over-screening alongside higher inequalities in screening uptake have been found [1,6,14,18]. Both aspects may not only be explained by lower uptake among women with a lower socioeconomic position, but also by higher levels of over-screening among those with a higher socioeconomic position.
As physicians are central actors interacting between institutional health policies and individuals [19], and remain important gatekeepers concerning consumer-demanded health practices [20], this suggests that cancer screening policies are enforced throughout physicians’ practices. Moreover, for CCS uptake, an encounter with a physician is a precondition for screening as Pap smears are performed in a physician’s office or clinic [21]. In opportunistic contexts, providers have rapidly adopted new tests in response to screening guidelines, but have been reluctant to adopt longer screening intervals [1,7]. This resistance to interval change could be attributed to disincentives due to loss of reimbursements with longer intervals, and lack of well-organised information systems to track screening history and ensure patient recall when screening is due [7]. This commodification approach of physicians who get paid for the provision of healthcare [22] constitutes a breeding ground for CC over-screening. Furthermore, if the idea is supported that women should undergo CCS every year, then CC over-screening may become socially normalised, as many may deem it to be a hegemonic practice [23]. So, in opportunistic contexts the screening recommendations are ‘out there’, but not strongly adhered to by physicians [24], whereas in organised contexts, physicians’ practices overlap more with what the recommendations prescribe [1,7]. This leads us to hypothesise that:
Hypothesis 1: Over European countries, CC over-screening is more prevalent in contexts with opportunistic screening compared to contexts with organised programmes.
Individual differences in CCS uptake within the past year
Higher levels of CCS uptake have been observed among women with a higher socioeconomic position compared to their counterparts [2,15,18,25,26]. As the responsibility to engage in healthcare services has shifted from the physician to include collaboration with the individual patient/consumer [27], it has been suggested that the physician–patient interaction is important concerning CCS uptake [28], and for engaging in over-screening. The quality of the physician–patient interaction may depend on women’s characteristics, and socioeconomic position-related disparities in this interaction may lead to educational and income differences in screening participation [26,28]. Several explanations for these socioeconomic inequalities have been suggested, relating to both educational attainment and income – that is, higher educated women may be more likely than less educated women to turn to physicians to guide them in the evaluation of complex technoscientific knowledge [29], and whereas the financial cost of over-screening is less of an issue among better off women, engaging in preventive healthcare services may be perceived more costly for poorer women [30]. Hence, when experts advise to screen on a yearly basis (more than is reimbursed by a healthcare system with cost-sharing; with fee-for-service in private healthcare system), richer women can better follow what experts offer and can take consumerist attitude under free market forces [11]. They can also better cope with the psychological burden of false positive test results, and the potential supplementary economic burden of additional clinical exams. To sum up, as women with a higher socioeconomic position may be more inclined to follow physicians’ recommendations, this may push them towards more frequent screening uptake in opportunistic contexts and to screening according to the guidelines in contexts with organised programmes. This leads us to hypothesise:
Hypothesis 2: In contexts with opportunistic screening, women with a higher socioeconomic position are more likely to have screened within the past year compared to women with a lower socioeconomic position.
Methods
Data
Data from the second wave of the cross-sectional European Health Interview Survey (see also online Appendix A) were used, which were gathered between 2013 and 2015. All European Union (EU) member states, Norway, Iceland and Switzerland, are included in this study. Data for Switzerland originate from the Swiss Health Interview Survey 2012, collected in 2011. In total, 31 countries were included in this research. For the contextual characteristics, data were obtained from the United Nations Development Programme (UNDP) (gross domestic product (GDP) per capita), the World Bank (Gini index) and the International Agency for Research on Cancer (screening strategy). For the construction of an index on accessibility of the healthcare system, data were gathered from Eurostat (out-of-pocket expenditure as a percentage of total health expenditure), the World Health Organization (public health expenditure as a percentage of GDP) and the UNDP (physician density per 10,000 people). To allow for an assessment of CC over-screening in terms of screening frequency, this research focuses on CCS uptake among women within screening-eligible age from 25 to 64 years old, because the three-yearly screening guidelines only apply for this age-specific female population [8]. The final sample sizes (N = 80,761) consisted of women having engaged in CCS within the past three years (more information in online Appendix B).
Dependent variables
In the absence of over-screening, we expect the proportion of women who screened within the past year to be 33.33%, and 66.66% for screening between one and three years ago. In line with previous research [25], we use the proportion of screening uptake within the past year above 33.33% as a proxy indicator of over-screening at the population level (see online Appendix C). Accordingly, the outcome in this paper is computed as screening within the past year versus having screened between two and three years ago. In the survey, respondents were asked how long ago they had had a cervical smear test. Possible answers were as follows: within the past 12 months, one to less than two years ago, two to less than three years ago, more than three years ago or never. We dropped the two last categories, and constructed a dichotomous outcome variable for CC over-screening at population level by recoding the answer categories, measuring whether the respondent was screened within the past year (1) or between one and three years ago (0).
Independent variables
As predictors of interest at the individual level, to examine the socioeconomic profile of women who screened within the past year, we included educational attainment and monthly household income. We measured educational attainment as the highest completed level of education, in accordance with the International Standard Classification of Education (ISCED) 2011 classification, and recoded it into a three-category variable: low education (0) based on ISCED 0–2; middle education (1) based on ISCED 3–4; and high education (2) based on ISCED 5–8. For household income, we used the country-specific net monthly equivalised income of the household, ranging from low to high income: below first quintile (0); between first and second quintile (1); between second and third quintile (2); between third and fourth quintile (3); between fourth and fifth quintile (4); and missing (5). At the macro level, we took the national CCS strategy into account. A country’s CC screening strategy was attributed to one of these categories according to Willems et al. [12]: opportunistic (0) if no formal programme was implemented at the time of the survey; regional/rollout ongoing (1) if not the entire female population was exposed to a programme due to an incomplete rollout or only regionally organised programmes; organised (2) if there was an organised population-based programme.
To control for indicated associations with CCS uptake, we took the following covariates into account at the individual level: age (five-year categorical ranges), marital status (married, single, widowed, divorced/separated, missing), urbanity (urban, rural), self-rated health (good, poor), work status (employed, unemployed, retired, permanently disabled, housework, other, missing), country of birth (national, born in other EU country, not born in EU) and time since last GP visit (years) [2,17,18]. At the macro level we included an access to healthcare index to control for cross-country differences in the accessibility of the healthcare system (for detailed information see Tables 1 and 2 in online Appendix D). A low score on this index corresponds with low accessibility of the healthcare system, and a high score with high accessibility. Furthermore, we controlled for income inequality by including the Gini coefficient, and for the level of economic development by including GDP per capita. These macro-level control variables were grand-mean centred (see also online Appendix E).
Statistical analyses
First, proportions of CCS uptake within the past year were calculated for the predictors of interest, together with the estimations of CC over-screening at population level, as shown in Table I. Second, these proportions were portrayed on a graph (Figure 1) by countries’ cancer screening strategies (see online Appendix F for absolute numbers). Third, to examine the relation between individual level characteristics and screening uptake within the past year, in relation to the screening strategy, multilevel logistic regressions were performed. The multilevel models involve two levels: 80,761 women nested in 31 countries. In Table II, the first model shows the main effects of educational attainment and household income, to examine the socioeconomic profile of women who were screened within the past year. In the second model, the country-level variables were added. In the third and fourth model, the context-dependency of women’s tendency to engage in CCS within the past year was assessed, by adding cross-level interaction effects. In all models, coefficients were adjusted for the individual (age, marital status, urbanity, self-rated health, work status, country of birth and time since last GP visit) and country-level (access to healthcare, Gini and GDP) control variables. Regressions coefficients were presented as odds ratios (ORs), and their corresponding significance levels are shown. Lastly, the interaction terms were plotted to support interpretation (Figures 2 and 3). A sensitivity analysis was conducted where the age threshold was increased to 30, in order to exclude young women who screened for the first time (results not shown). Analyses were conducted using STATA 15.
Descriptive statistics of 80,761 women aged 25–64 with Pap smear uptake in the recommended time interval (0–3 years ago), subgroup of women with Pap smear within the past year and Pap smear over-screening at population level, in the European Health Interview Survey.
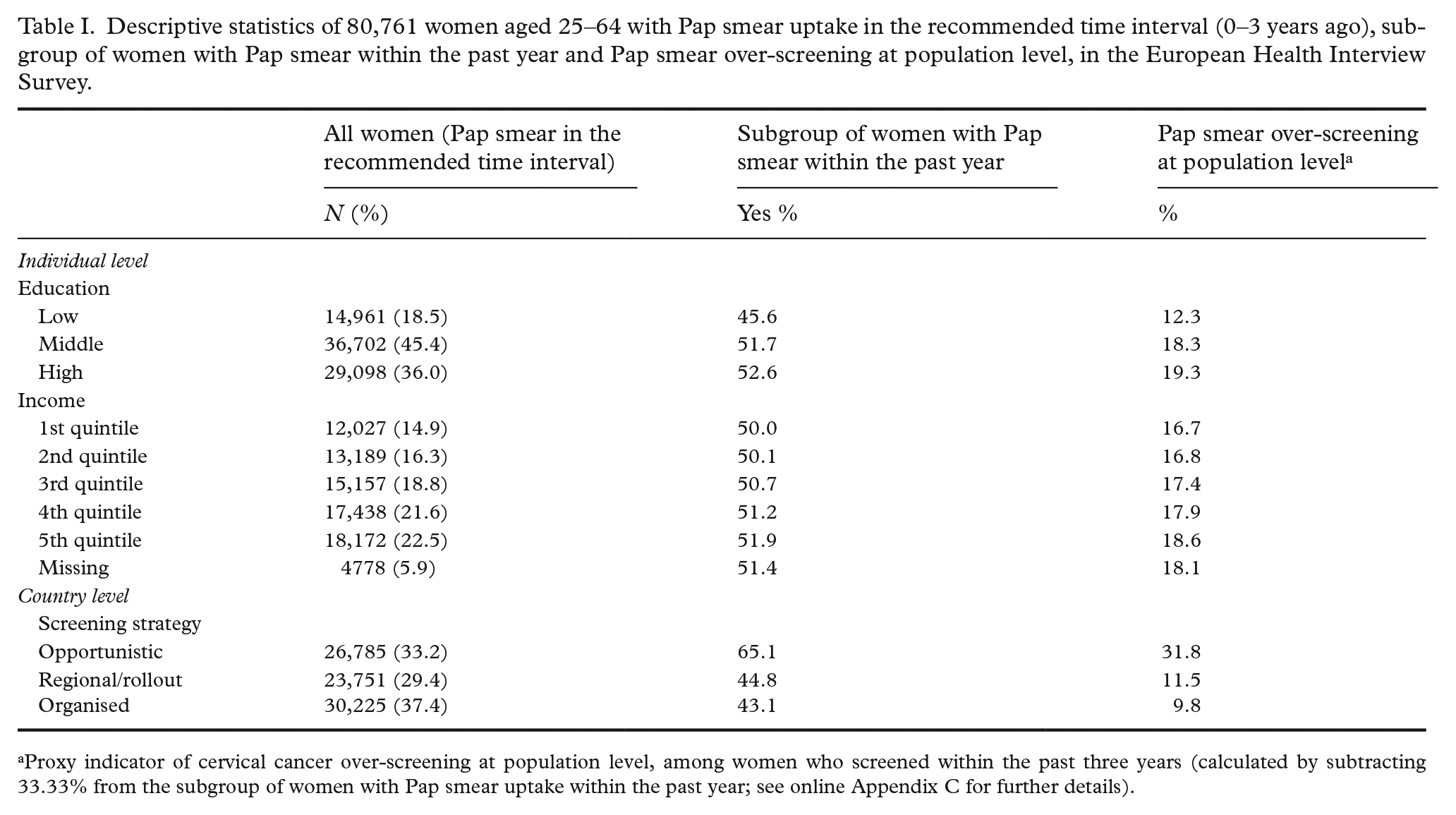
Proxy indicator of cervical cancer over-screening at population level, among women who screened within the past three years (calculated by subtracting 33.33% from the subgroup of women with Pap smear uptake within the past year; see online Appendix C for further details).
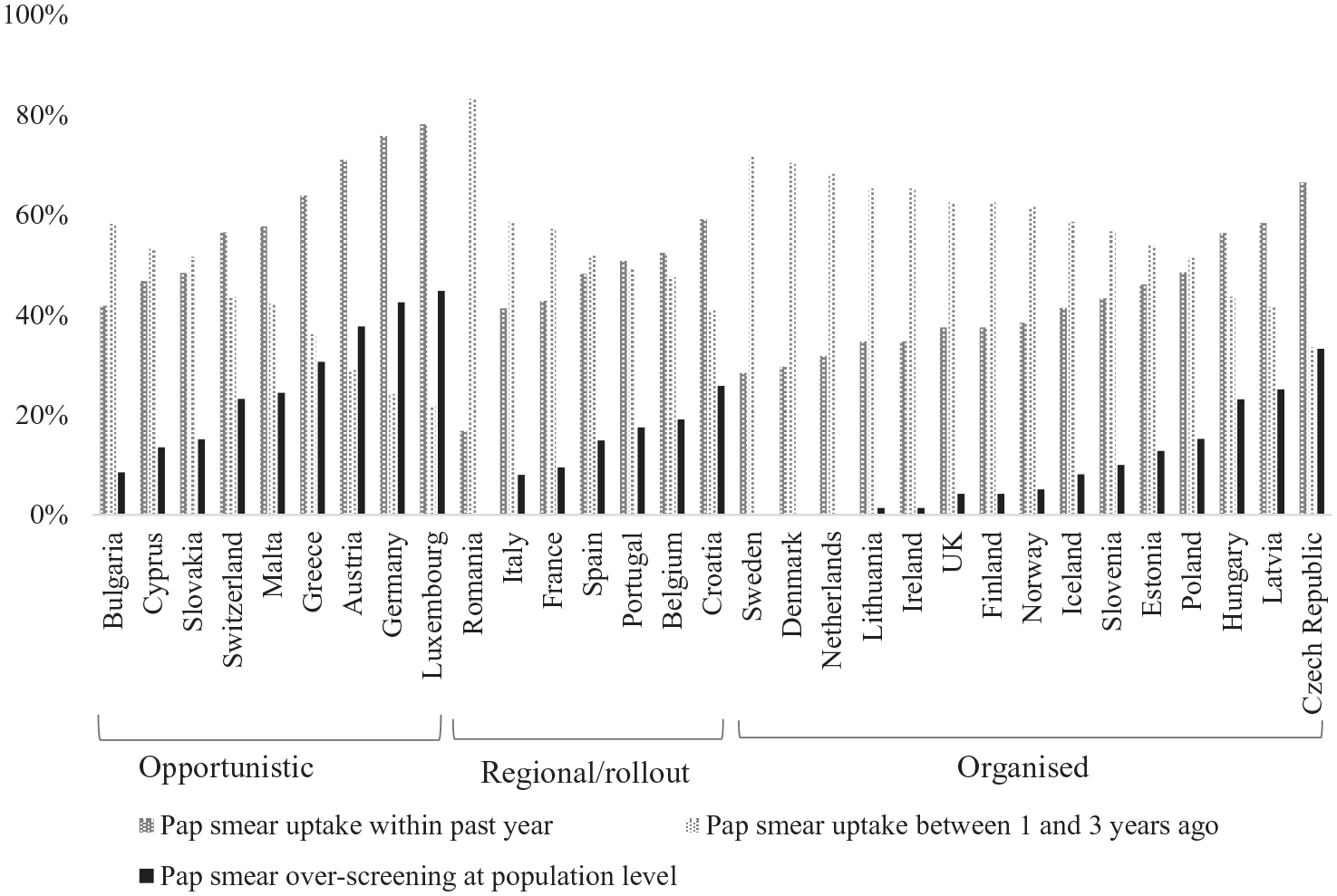
Proportions of Pap smear uptake between one and three years ago versus Pap smear uptake within the past year, and Pap smear over-screening at population levela among 80,761 screening women aged 25–64, by country and screening strategy.
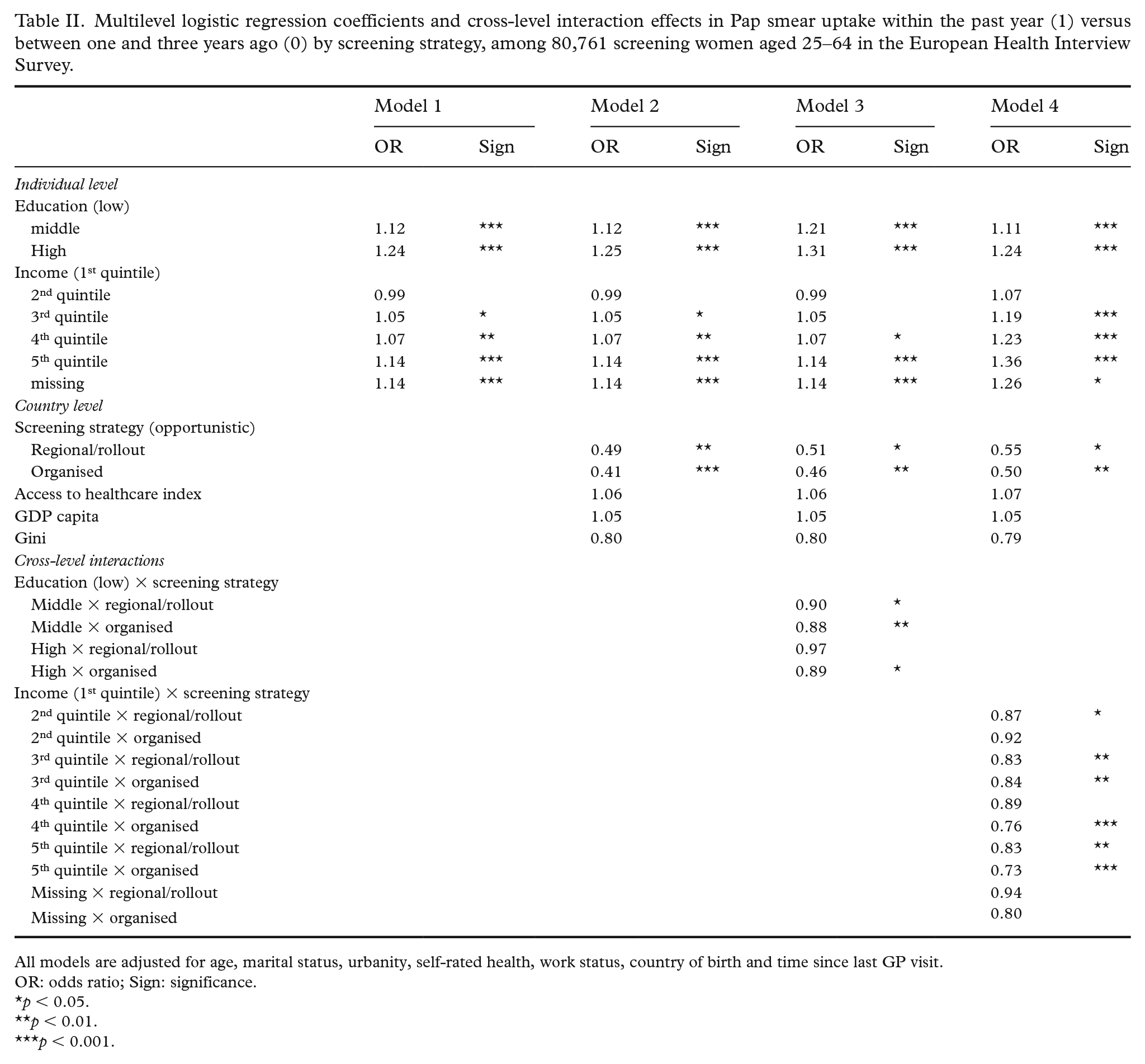
Multilevel logistic regression coefficients and cross-level interaction effects in Pap smear uptake within the past year (1) versus between one and three years ago (0) by screening strategy, among 80,761 screening women aged 25–64 in the European Health Interview Survey.
All models are adjusted for age, marital status, urbanity, self-rated health, work status, country of birth and time since last GP visit.
OR: odds ratio; Sign: significance.
p < 0.05.
p < 0.01.
p < 0.001.
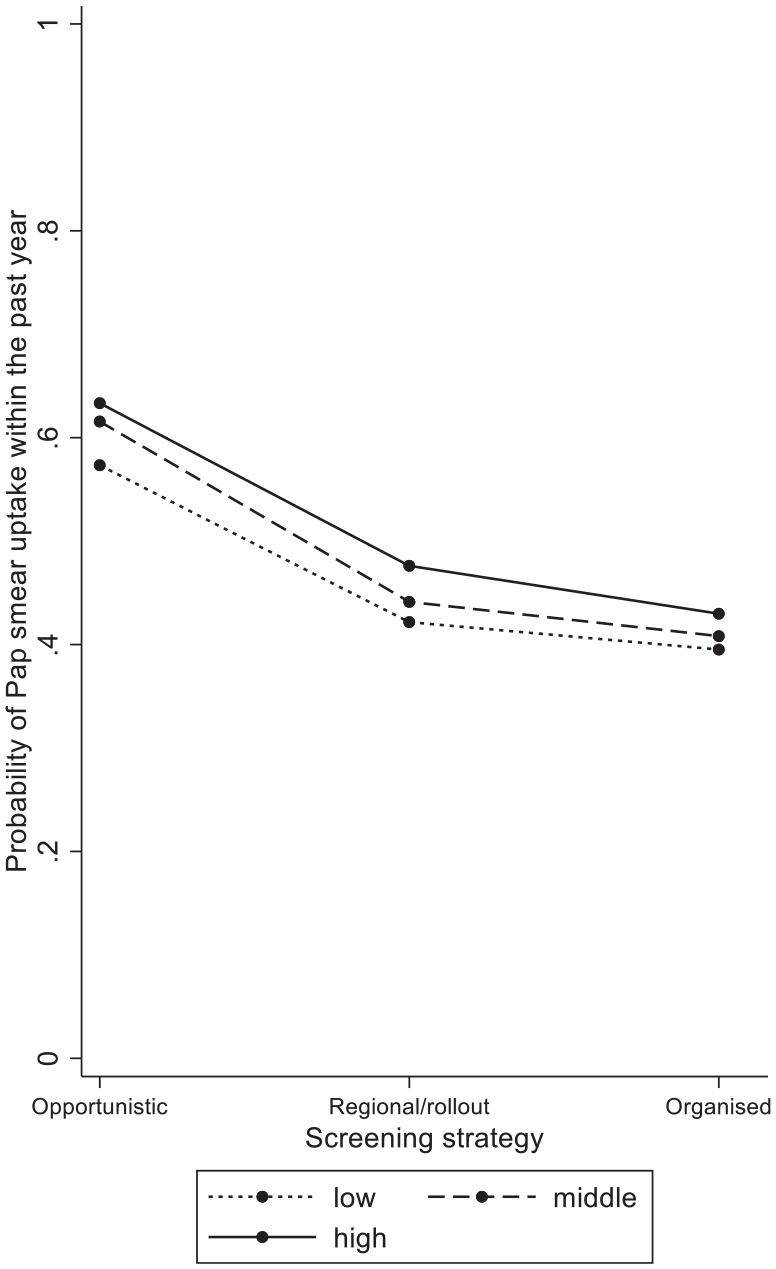
Predicted probabilities of Pap smear uptake within the past year in screening women aged 25–64 by educational attainment and screening strategy (from Table II: Model 3).
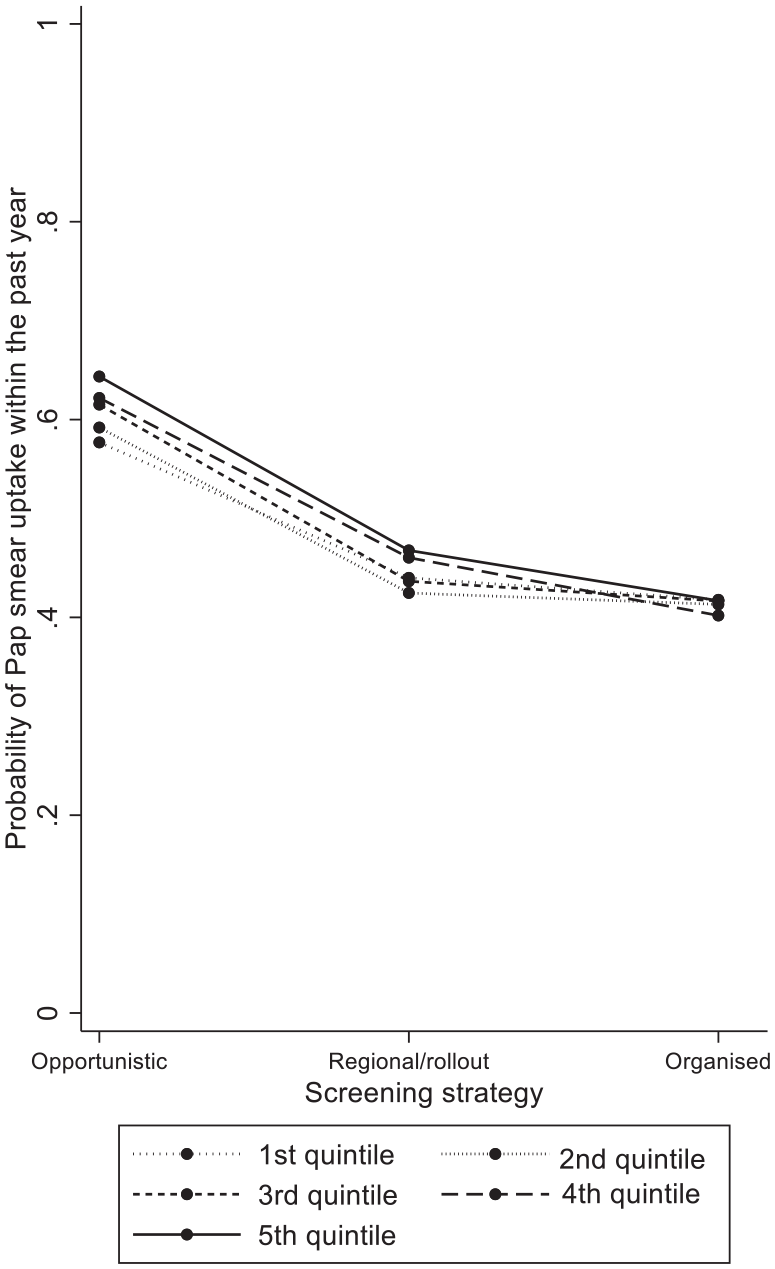
Predicted probabilities of Pap smear uptake within the past year in screening women aged 25–64 by household income and screening strategy (from Table II: Model 4).
Results
CC over-screening according to women’s socioeconomic position and country-level screening strategy
The descriptive statistics for CCS uptake can be found in Table I. A total of 50.9% of the women reported having had a Pap smear within the past year, corresponding with 17.6% of over-screening at population level. Proportions of Pap smear over-screening at population level were higher among women with a middle (18.3%) or high (19.3%) level of educational attainment compared to women with a low level of education (12.3%). Similarly, for household income a subtle gradient was observed with higher CC over-screening among richer (18.6%) compared to poorer (16.7%) women. As concerns countries’ screening strategies, on average, CC over-screening at population level appeared to be highest in opportunistic systems (31.8%), and lower in regional/rollout (11.5%) and organised (9.8%) systems. Country-specific proportions are presented in Figure 1. The highest rates of population-level CC over-screening were observed in Luxembourg (44.8%) and Germany (42.5%), which both have an opportunistic screening strategy. We observed significantly lower ORs of CCS uptake within the past year in countries with organised screening (ORmodel2 = 0.41) or regional/rollout (ORmodel2 = 0.49), compared to opportunistic systems (Table II).
Socioeconomic profile of women who were screened within the past year
The results of the multilevel logistic regression models are presented in Table II. For educational attainment, the odds of having undergone screening within the past year was significantly higher as women had a higher level of education (Table II: ORmodel1 middle = 1.12, high = 1.24), compared to lower educated women. For household income, richer women were significantly more likely to have had a screening test within the past year (Table II: ORmodel1 third quintile = 1.05, fourth quintile = 1.07, fifth quintile = 1.14) compared to poorer women.
Context dependency according to the screening strategy
To examine if the socioeconomic profile of women who were screened within the past year is modified by the country-level screening strategy, four cross-level interaction terms were estimated. It appeared that the tendency of women with a higher educational attainment (Table II: ORmodel3 middle × organised = 0.88 (p = 0.022), high × organised = 0.89 (p = 0.05)) and household income (Table II: ORmodel4 third quintile × organised = 0.84 (p = 0.004), fourth quintile × organised = 0.76 (p < 0.001), fifth quintile × organised = 0.73 (p < 0.001)) to engage more in screening within the past year than their counterparts was smaller in organised systems compared to opportunistic systems. These interaction terms are graphically displayed in Figures 2 and 3, and illustrate that the lower levels of over-screening observed in organised systems may be attributed especially to lower levels of screening within the past year among women with a higher socioeconomic position in such contexts.
Discussion
This research contributes to the epidemiological and healthcare services literature on CCS by assessing CC over-screening and how this may relate to inequalities in screening uptake [1,16,17,25], and by studying this phenomenon in a European-wide context.
Before turning to the main findings of this study, we first address a couple of its limitations. Firstly, due to lacking information on screening frequency, a proxy indicator was used for CC over-screening. We used screening uptake within the past year as an indicator of CC over-screening at population level, which is an approach at the aggregated level, and, consequently, not generalisable to the individual level [25]. Misclassification may have occurred for women whose three-yearly screening was due, and for women who engaged in their first CCS ever (yet the sensitivity analysis indicated the latter not to strongly affect the results). Secondly, crucial information on incentives for Pap smear uptake was missing, as indicators such as having symptoms of cervical lesions, or having had sexual intercourse, were not available, which would have been helpful to narrow down CC over-screening.
Notwithstanding these limitations, several important findings came to surface throughout this study. Firstly, we observed higher levels of CC over-screening in opportunistic contexts compared to organised contexts. Hence, we have found supportive evidence for hypothesis 1. This is in line with previous research that has indicated higher levels of over-screening in opportunistic contexts [1,6,14]. From previous research [12] it appeared that organised CCS does not necessarily correspond with higher levels of CCS uptake. The current research indicates that this may be explained by CCS overuse, which is less present in contexts with organised screening programmes compared to contexts with opportunistic screening. Based on the current research, contexts with organised CCS programmes appear more efficient in terms of the allocation of resources and equity by reducing over-screening, and establishing the European guidelines as a norm. Similarly, whereas organised screening may enhance screening uptake in the under-screening segment of the population [1,2,11], it appears from our research that it may also reduce the degree of over-consumption. Together, both processes contribute to lower levels of inequality.
Secondly, we observed that in opportunistic contexts women with a higher socioeconomic position were more likely to be screened within the past year than lower socioeconomic position women, compared to the situation in organised contexts. Hence, we found supportive evidence for hypothesis 2. Future research can scrutinise this finding to assess which underlying mechanisms are at play, and can further explore the role of the physician therein.
In summary, in the current research, we found that, in opportunistic contexts, women with a higher socioeconomic position engaged more than their socioeconomically disadvantaged counterparts in CCS uptake in the past year. Future research can assess whether women, or men, with a higher socioeconomic position also tend to overconsume other preventive healthcare practices, and may include other institutional factors at the healthcare and social system levels to further scrutinise cross-country differences. Such research is advised, as it is relevant to both the scientific field and the policy debate on the limitation of over-screening, equity in the access to care and the allocation of resources.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948221118215 – Supplemental material for Cervical cancer (over-)screening in Europe: Balancing organised and opportunistic programmes
Supplemental material, sj-docx-1-sjp-10.1177_14034948221118215 for Cervical cancer (over-)screening in Europe: Balancing organised and opportunistic programmes by Vincent De Prez, Vladimir Jolidon, Stéphane Cullati, Claudine Burton-Jeangros and Piet Bracke in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation – Flanders (grant number FWOOPR2018005701) and the Swiss National Science Foundation (grant number 176115).
Data availability
The data that support the findings of this study are available from Eurostat. Restrictions apply to the availability of these data, which were used under license for this study. Data are available to the authors with the permission of Eurostat.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.