
Abstract
Background:
Migration presents numerous significant changes in a person’s life, physically, emotionally and socially. How health develops in the host country depends on a range of factors, including language proficiency. We aimed to investigate associations between language proficiency and health.
Methods:
Statistics Norway carried out the Living Conditions Survey for Immigrants (2016), conducting telephone (82%) or face-to-face (18%) interviews with immigrants (two or more years of residence) from 12 countries. The survey collected data on self-reported proficiency in the Norwegian language, health and socio-economic variables, and included 4077 people aged 16–66 years.
Results:
In logistic regression models adjusted for age, sex and duration of residence, poor or medium self-reported Norwegian proficiency, as compared to good, was associated with poorer health outcomes, including lower odds of self-rated health (odds ratio (OR)=0.46; 95% confidence interval (CI) 0.39–0.54) and higher odds of hypertension (OR=1.74; 95% CI 1.34–2.26), back or neck pain (OR=1.52; 95% CI 1.28–1.80), mental health problems (OR=1.34; 95% CI 1.09–1.65), sleep disturbances (OR=1.51; 95% CI 1.23–1.86) and being overweight (OR=1.20; 95% CI 1.03–1.40). Adjustment for socio-economic status attenuated the associations, but further adjustments for perceived discrimination and lifestyle (smoking and physical activity) did not further alter the estimates.
Conclusions:
Host language proficiency has implications for health among immigrants. Equitable access to health services and quality of care requires adjustment to the language level needs of patients. Facilitating language learning for immigrants may be vital in providing access to health services and supporting newcomers in being more active participants in managing their health.
Introduction
Migration is a demanding process and presents numerous significant changes in a person’s life, physically, emotionally and socially. Often, the healthiest in a population are those with sufficient resources to migrate, and newly arrived migrants tend to be particularly healthy. However, any health advantages diminish over time in the host country, and immigrants’ health becomes poorer compared to the population in general [1]. Immigrants who have been forced to leave their country despite poor health (e.g. refugees) lack such health advantages, leaving them particularly vulnerable.
How health develops in a new environment depends on a range of factors, including the economy, education, social network and environment, access to health services and lifestyle. Limited proficiency in the host country’s language constitutes a barrier to understanding written and oral health information and accessing health care or preventive services [2]. Proficiency in the host language also influences how other assets, such as occupation or social relations, translate into health [3]. Previous studies have shown that poor skills in the language of the host county are associated with poor health. These studies have primarily been carried out in English-speaking countries [4–12] and many among older immigrants [5,9–11].
A patient’s limited proficiency in the host language is particularly salient during consultations with doctors, who can address patients’ physical complaints and concerns directly. Based on a physical examination and what a patient can convey about their symptoms and general situation, a doctor will propose a course of clinically relevant action [13–16]. Patients require advanced vocabulary and grammar skills to describe their medical history, situation and symptoms. Moreover, for patients to adhere to planned treatment, they must understand what it is and what they need to do [17].
In Norway, immigrants have worse outcomes on an array of diseases and conditions compared to the general population. However, considerable variations exist between groups [18]. No published studies exist of the association between proficiency in the Norwegian language and health among immigrants. Any association between poor proficiency in the Norwegian language and poor health, even if bidirectional, suggests potential for mitigation: by adjustments to health services (to meet the needs of these immigrants better) and facilitated language education (to support immigrants in accessing and using these services more effectively and to manage their health in general better).
We aimed to assess the association between self-reported Norwegian language proficiency and aspects of health (self-rated health, diabetes, cardiovascular disease, back and neck problems, mental health problems, sleep disturbances and being overweight) among immigrants to Norway from 12 countries, aged 16–66 years. We further aimed to assess the importance of age, sex, duration of residence, education, income, smoking, physical activity and perceived discrimination in these associations.
Methods
We used data from the Statistics Norway Living Conditions Survey for Immigrants 2016 [19]. Inclusion criteria were a minimum of two years’ residence, age 16–74 years and country of birth Poland, Bosnia-Hercegovina, Kosovo, Turkey, Iraq, Iran, Afghanistan, Pakistan, Sri Lanka, Vietnam, Eritrea or Somalia. In total, 4435 immigrants were interviewed (response rate 54%), by telephone (82%) or face-to-face (18%), in their preferred language (Norwegian, English or the primary language in each of these countries). The response rate varied from 46.6% among Somalis and 47.7% among Vietnamese to 61.0% among Sri Lankans and 62.4% among Eritreans. The following participants were excluded: those aged ⩾67 years (n=85), those who had missing values on all questions on health (n=11) and those where data on Norwegian proficiency was lost due to a programming error (n=262). Thus, our sample consisted of 4077 participants. Participants missing data on Norwegian proficiency were most likely to be from Eritrea, Somalia, Afghanistan or Iraq.
Variables
The survey provided Likert scale options to elicit participants’ Norwegian proficiency in three domains: in general, when reading newspapers and when talking with a doctor about health issues. Ultimately, participants’ answers were collapsed, with ‘very good’ and ‘good’ classified as ‘good’, and ‘medium’ (own category) and ‘poor’ and ‘very poor’ classified as ‘poor’. Those who reported having medium or poor Norwegian proficiency were asked whether during the last 12 months they had used an interpreter (a professional, a family member or a friend) in a consultation with a doctor or dentist or had needed one but not received one.
Questions on health included ‘In general, do you consider your health to be very good, good, neither good nor poor, poor or very poor?’ (with answers collapsed as above ) and whether participants during the last 12 months had experienced one or more of the following health problems: coronary heart disease, stroke or angina pectoris (merged into ‘cardiovascular disease’), hypertension, diabetes, back problems or neck problems (with the latter two merged into ‘back or neck problems’). The five-point Hopkins Symptoms Checklist Scale [20] assessed mental health problems. It included questions on experiences during the last 14 days of ‘nervousness or shakiness inside’, ‘feeling fearful,’ ‘feeling hopeless about the future,’ ‘feeling blue’ and ‘worrying too much about things’, providing the response options of ‘not at all’ (1 point), ‘a little’ (2 points), ‘quite a bit’ (3 points) or ‘extremely’ (4 points). Mean scores were calculated for participants having answered at least four of the five questions, and an average score >2 indicated symptoms of clinically significant mental health problems. Finally, participants were asked whether during the last 14 days they had experienced sleep disturbances, with the same four answer categories as above and with ‘quite a bit’ or ‘extremely’ classified as having trouble with sleep.
Socio-demographic variables were collected from register linkages: age (years; 16–24, 25–44, 45–66), level of education (primary school, upper secondary high completed and university/higher education started or completed), income (NOK, monthly household income adjusted for household size: 10,000–19,999, 20,000–29,999, ⩾30,000), participants’ age at immigration (years; 0–6, 7–15, 16–19 and ⩾20) and duration of residence in Norway (years; 2–3, 4–6, 7–10, 11–15, 16–20 and ⩾21). Since many of the youngest participants had not yet completed their education, we replaced the education of these participants with a proxy of expected education, namely the highest parental education attained if it was higher than the child’s education. Participants reported smoking as ‘no’ or ‘yes’ (‘daily’ or ‘sometimes’), and those reporting being physically active at least once a week were considered ‘physically active’. Participants also provided their perceived experience of discrimination (‘no’ or ‘yes’) in five areas (at work, when seeking work, at an educational institution, in health services or other places).
The proportion of missing values was between 0% and 0.2% for health indicators, except for being overweight (3.9%). No values were missing for age, age at immigration and duration of residence. However, 2.1% was missing on education and 4.6% on income. The correlation between predictor variables was in general low, with the highest being between age and duration of residence (0.4).
Analyses
We used chi-square tests to assess associations between Norwegian proficiency, socio-demographic and migration-related background characteristics, and health indicators. We carried out logistic regressions to assess associations (reported as odds ratio (OR)) between Norwegian proficiency (both in general and when talking with a doctor about health issues) and health outcomes crude and adjusted for covariates: model 1 – age, sex and duration of residence; model 2 – as model 1 plus education and income; model 3 – as model 2 plus perceived discrimination, smoking and physical activity. The association between education and health and between education and Norwegian proficiency is possibly bidirectional (with education predicting better health and better language proficiency, and health and language proficiency predicting education). Likewise, health and Norwegian proficiency could influence income, and income may influence health and, indirectly, language skills enhanced at the workplace. There were no significant interactions between sex and Norwegian proficiency for any of the health outcomes studied, and women and men were analysed together. In sensitivity analyses, we excluded those who had used an interpreter in communication with doctor during the last 12 months. We hypothesised that these groups would represent those with the lowest level of Norwegian proficiency.
Ethics
Because the data set was anonymised, specific ethical approval was not required for this study and was waved by the Norwegian Centre for Research data. To use the data set, we signed a confidentiality agreement with the Norwegian Centre for Research Data.
Results
More than half of the participants preferred to be interviewed in Norwegian (57.2%), while only 1.3% preferred English. Those who preferred to be interviewed in the language of their country varied from 20.4% among Iraqis and 20.8% among Somalis to 83.4% among Polish immigrants.
Our sample consisted of a slightly higher proportion of males than females, and approximately half of the participants were in the age group 25–44 years (Table I). Most participants (65%) had immigrated after 20 years of age; 31% had lived in Norway for ⩾21 years, and 28% for ⩽6 years. The proportion of participants who reported good Norwegian proficiency decreased with older age groups and older age at immigration; good Norwegian proficiency increased with educational level, income level and length of residency. While 62.2% of participants reported good Norwegian proficiency in general, 70.3% reported good Norwegian proficiency when talking with a doctor and 66.2% when it came to reading newspapers. Of those choosing Norwegian as their interview language, 80% reported good, 17% medium and 3% poor Norwegian proficiency.
Background characteristics of participants in the Living Conditions Survey for Immigrants 2016 and self-reported Norwegian proficiency according to background characteristics (N=4077).
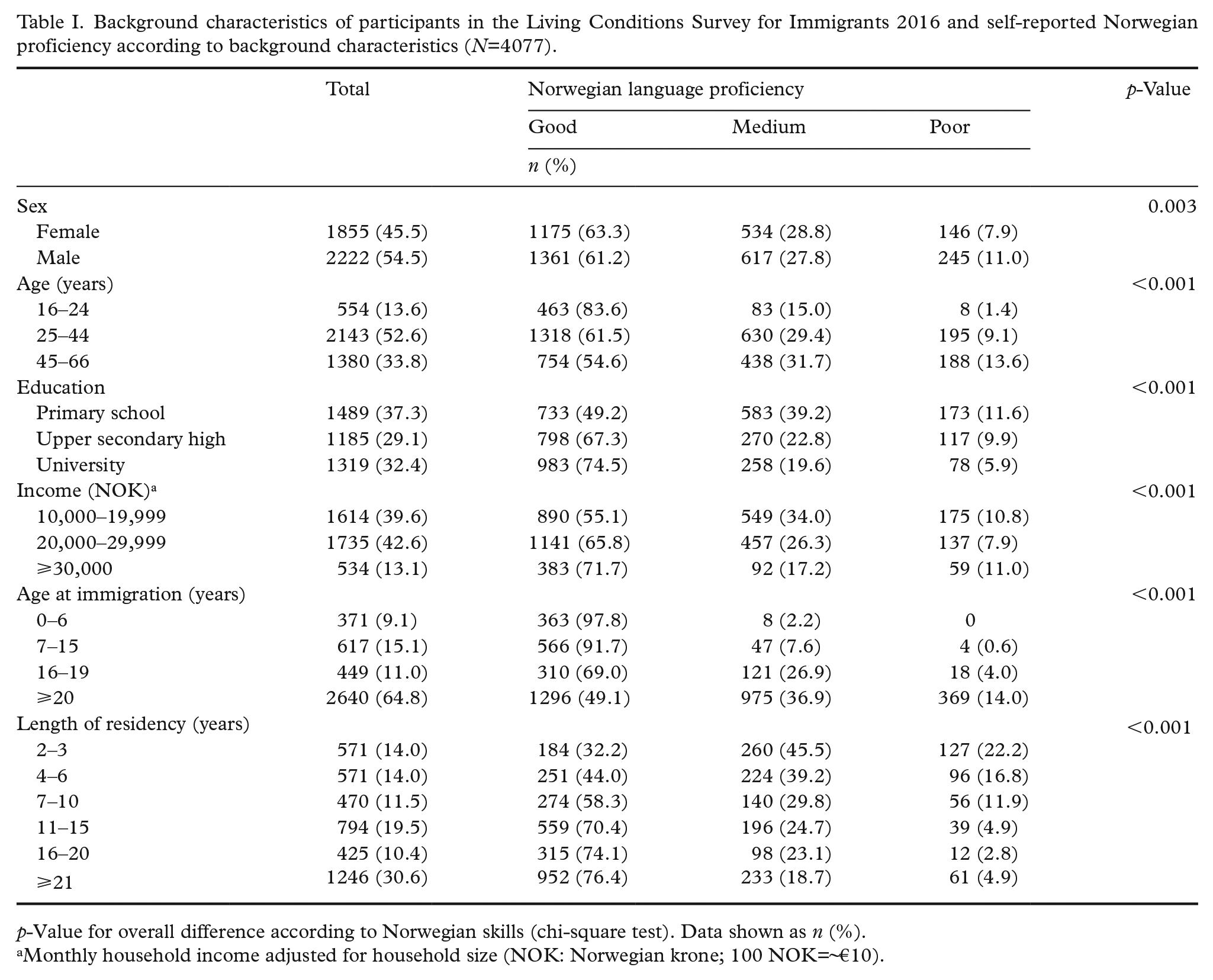
p-Value for overall difference according to Norwegian skills (chi-square test). Data shown as n (%).
Monthly household income adjusted for household size (NOK: Norwegian krone; 100 NOK=~€10).
Those who reported having medium or poor Norwegian proficiency (n=1542) were asked about the use of interpreters in a consultation with a doctor during the last 12 months. Of the 584 (37.9%) participants who answered, 283 (48.5%) reported that they had used an interpreter: a professional one (n=201), a family member or friend (n=142) or both (n=60).
Participant-reported Norwegian language proficiency (poor/medium vs. good) influenced health-related variables. In general, compared to those with good self-reported Norwegian language proficiency, significantly fewer participants with medium and poor proficiency reported having good health, with a similar pattern on the following specific health-related variables. Compared to good language proficiency, participants who reported poor Norwegian language proficiency were significantly more likely to report having diabetes, cardiovascular disease, hypertension and being overweight (Table II). Those who reported medium Norwegian proficiency were significantly more likely to report having hypertension, mental health problems, sleep disturbances and being overweight. Smoking was more prevalent among those with poor versus good Norwegian proficiency, and a higher proportion of those with good Norwegian proficiency reported being physically active compared to others (Table II).
Proportions with various health outcomes among participants in the Living Conditions Survey for Immigrants 2016 in total and by self-reported Norwegian language proficiency.
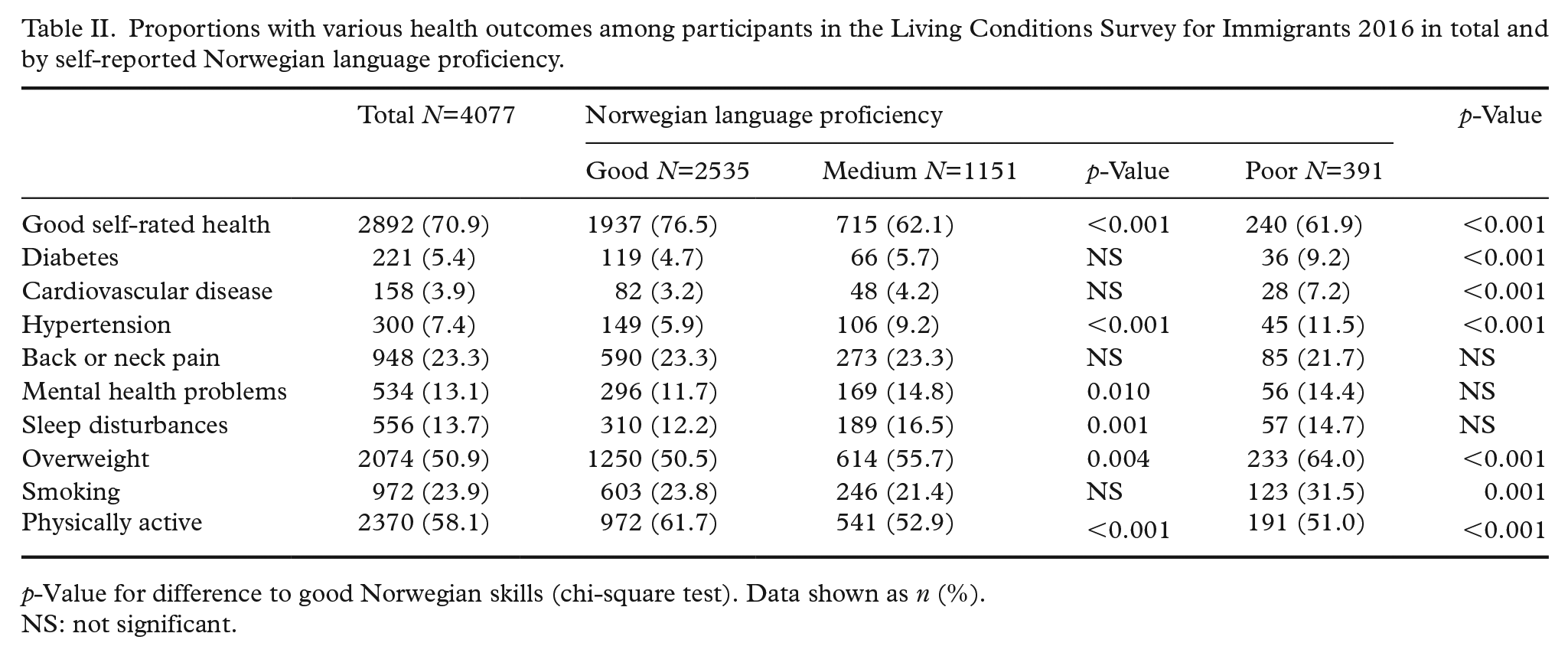
p-Value for difference to good Norwegian skills (chi-square test). Data shown as n (%).
NS: not significant.
In regressions adjusted for possible confounding variables (age, sex and duration of residence), poor/medium Norwegian proficiency was inversely related to good self-reported health (OR=0.46; 95% confidence interval (CI) 0.39–0.54; Table III) and positively associated with hypertension (OR=1.74; 95% 1.34–2.26), back or neck pain (OR=1.52; 95% CI 1.28–1.80), mental health problems (OR=1.34; 95% CI 1.09–1.65), sleep disturbances (OR=1.51; 95% CI 1.23–1.86) and being overweight (OR=1.20; 95% CI 1.03–1.40; Table III). After further adjustment for education and income, poor/medium language proficiency remained inversely related to good self-reported health (OR=0.54; 95% CI 0.46–0.64) and positively associated with hypertension (OR=1.69; 95% CI 1.28–2.24) and sleep disturbances (OR=1.32; 95% CI 1.06–1.65). Further adjustment for smoking, physical activity and experience of discrimination did not attenuate estimates notably. In similar analyses using Norwegian proficiency in communication with a doctor about a health issue as the exposure, associations with diabetes and cardiovascular disease were stronger, the association with back and neck problems was significant and the association with sleep disturbances weaker (Table III). Further, using proficiency in reading Norwegian as exposure, associations with diabetes, cardiovascular disease and hypertension were stronger than when using Norwegian proficiency in general.
Odds ratios (95% confidence intervals) for various health outcomes among those with poor or medium self-reported Norwegian proficiency (compared to good) among participants in the Living Conditions Survey for Immigrants 2016.
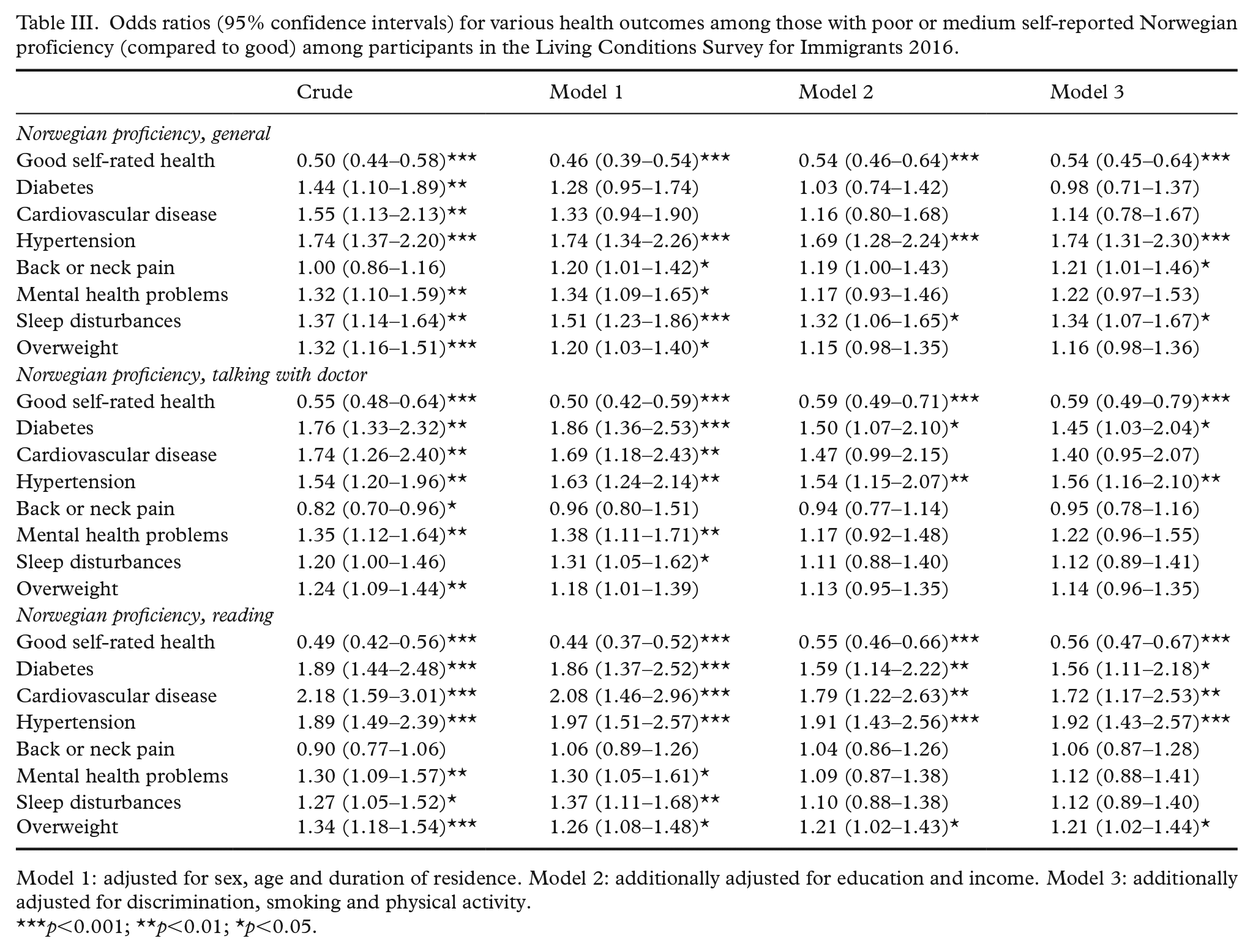
Model 1: adjusted for sex, age and duration of residence. Model 2: additionally adjusted for education and income. Model 3: additionally adjusted for discrimination, smoking and physical activity.
p<0.001; **p<0.01; *p<0.05.
In sensitivity analyses excluding those who reported involving an interpreter in communication with the doctor during the last year, estimates were attenuated for all health measures except being overweight, further pointing towards a relationship between limited proficiency in the Norwegian language and health (Supplemental Table SA).
Discussion
Among immigrants in Norway, poor or medium self-reported Norwegian proficiency was associated with poorer health outcomes, including self-rated health, hypertension, cardiovascular disease, mental health problems, sleep disturbances and being overweight, as compared to good Norwegian proficiency. Adjustment for socio-economic status attenuated the associations, but further adjustments for perceived discrimination and lifestyle (smoking and physical activity) did not further alter the estimates.
Strengths and limitations
This article is among the first to investigate the association between limited proficiency in the Norwegian language and health [21]. Data came from a national living condition survey among immigrants, with a reasonable number of participants originating from 12 countries, representing about one third of immigrants in Norway. With some precautions, the results could be generalised to most immigrants in Norway. The population register was the source of participants and did not include people who are undocumented immigrants or temporarily working in Norway. The response rate was 54%, in line with the Living Condition Survey among the general population (59%), which often under-represents immigrants [22]. Statistics Norway noted that some immigrants had changed their phone number or address or had emigrated without registration [20]. Selection bias is likely, and immigrants with poor self-reported Norwegian proficiency may be under-represented, even though interviews were offered in the primary language of participants’ country of origin. Moreover, participants had to have lived in Norway for a minimum of two years, further excluding immigrants who likely have the poorest Norwegian proficiency. Statistics Norway report that people with high education are slightly over-represented, but that there are no substantial differences in age, sex or duration of time in Norway between respondents and non-respondents [22]. The sample may also under-represent participants with poor mental and physical health.
All health measures were self-reported and may not match actual clinical diagnosis. However, self-rated health consistently predicts morbidity and mortality [23,24] and is thus considered a reliable and simple measurement of a person’s health status. Immigrants and ethnic minorities generally rate their health as good less often than majority populations [25].
To shed light on the importance of written information, we included a measure of proficiency in reading Norwegian. The available measure in the survey was Norwegian proficiency in reading newspapers, which is perhaps not a true proxy for reading health information. However, it might capture exposure to more general health information, including lifestyle advice presented in newspapers and other written media. Suggestive of this link is the associations between language and lifestyle-related diseases (hypertension, diabetes and cardiovascular disease), which were stronger when Norwegian proficiency was measured as reading than when measured in general. Reading abilities relate to health literacy, for which we had no measure available but which has been shown by others to be important for health and to modify the association between language proficiency and health [4]. We also speculate that immigrants may overestimate their speaking skills: native speakers may adjust (not always revealing non-understanding and simplifying their own speech), masking non-native speakers’ actual level of proficiency. In this respect, reading in Norwegian could be a more objective measure of Norwegian proficiency.
Comparison to other studies
In the Living Condition Survey among immigrants in Norway in 2006, poor Norwegian skills were associated with poorer health [21]. In that study, poor health was measured as an index consisting of self-reported health, self-reported diseases and physical and mental ailments, as well as their influence on everyday life. Language was a composite measure of self-reported skills in reading, writing, talking and understanding Norwegian. In the USA, poor English proficiency has been associated with poor self-rated health among Chinese, also when adjusted for participants’ need for interpreter, health literacy, socio-economic variables and health [5]. Among elderly immigrants, limited English proficiency has been associated with both poor self-rated health and poor emotional health [9]. In Canada, poor English proficiency was associated with poor self-rated health among newly arrived immigrants [7]. Finally, among Arab Americans, immigrants were more likely to report poor self-rated health than those born in the USA, and those who answered the study in Arabic even more than those who answered in English [8].
Our findings also resemble the results of qualitative studies among several immigrant groups in Norway. Polish migrants have expressed insufficient Norwegian language competence in difficulties understanding written information provided only in Norwegian, navigating Norwegian health-related websites and communicating with health personnel [26]. Further, access to qualified interpreters was often limited [27]. Interviews with female migrants from Thailand identified language difficulties obstructing access to information and health care in Norway, even amongst those living in Norway for several years. Over time, persistent communication challenges decreased their willingness to engage with the Norwegian health-care system [28]. Immigrants from Sub Saharan Africa have expressed difficulties in gaining and understanding information about available health services, especially for mental health issues, as well as about other health issues commonly presenting in their community [29].
Explanatory mechanisms
Adjustment for age and duration of residence did not alter associations between host language proficiency and health notably, and further adjustments for education and income attenuated but did not eliminate these associations. Stronger Norwegian proficiency may open doors to higher education and income (via work), which are both determinants of better health. Conversely, good health supports learning a new language, accessing higher education and better job opportunities, and poor physical and mental health could create barriers to language learning. Thus, improving physical and mental health among immigrants could also facilitate language learning, possibly reinforcing better health. Language may be a prerequisite for social connections in the host country, which could be positive for both mental and physical health. While many immigrants will have relationships within their community from the same country or region, relationships with people from the host population could increase a sense of belonging, coping with everyday life and navigating new systems.
In Norway, all inhabitants have the right to a general practitioner, who is the gatekeeper to all specialised health services. Thus, there are no formal barriers to accessing health services. However, practical barriers linked to poor language proficiency and lack of knowledge about the system may impede access to necessary health care and beneficial outcomes upon access. The most direct access immigrants have to the health system is face-to-face meetings with health practitioners. These consultations constitute the nexus of care, during which system resources are matched to the patient’s particular needs. Ineffective communication during these interactions could further explain poorer health, either because the medical decisions do not fit the patient’s condition (delaying appropriate treatment) or because the patient did not understand the plan sufficiently to adhere to it (e.g. not filling prescriptions, not attending diagnostic tests). Sufficient and adequate use of interpreters would be important for facilitating effective communication between some immigrant patients and health practitioners. Consequent perceptions that the host country’s health system is not meeting their needs may decrease trust and motivation to seek further care.
Conclusions
In Norway, immigrants with poor and even medium Norwegian language proficiency had significantly poorer levels of health compared to those with good proficiency. Our findings suggest that host language proficiency plays a role in health among immigrants and that means to meet immigrants with poor proficiency in the host language more effectively are warranted. First, equitable access to health services and quality of care requires adjustment to the language level needs of all patients, including adequate use of interpreters. Second, language learning is not only a generic matter of integration and inclusion; it is specifically implicated in health outcomes. Facilitating language learning for those who have immigrated to Norway may be key to supporting newcomers in being more active participants in managing their health.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948211025158 – Supplemental material for Proficiency in the Norwegian language and self-reported health among 12 immigrant groups in Norway: A cross-sectional study
Supplemental material, sj-docx-1-sjp-10.1177_14034948211025158 for Proficiency in the Norwegian language and self-reported health among 12 immigrant groups in Norway: A cross-sectional study by Marte K.R. Kjøllesdal, Jennifer Gerwing and Thor Indseth in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The survey was supported by the Norwegian Ministry of Justice Analysis was supported by the Norwegian Directorate of Health and The Norwegian Institute of Public Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.