
Abstract
Aim:
This study examined the barriers and opportunities in Sweden for integrating One Health practices. Sweden’s long tradition of working with One Health was used as a case to analyse persistent barriers as well as opportunities.
Method:
Thirteen semi-structured interviews with experts from the Swedish Veterinary Agency, Food Agency, Public Health Agency, and Environmental Protection Agency were carried out. A thematic content analysis was conducted on the interviews using inductive coding in NVivo.
Results:
The study revealed that while collaboration is the general aspiration across the Swedish agencies, barriers persist regarding the understanding of One Health, the integration of the environment sector and awareness of the different terminologies employed within the disciplines. There are legislative challenges and barriers to science to policy translation. Disease outbreak was identified as an opportunity for One Health integration.
Conclusions:
A One Health strategy needs to be developed at agency level to define One Health and clarify the roles and responsibilities. To overcome practical challenges, experts need to be aware of different terminologies and practices when collaborating. Further prospects for One Health integration include employing policy entrepreneurs to push One Health onto the political agenda. Preparations for disease outbreaks need to focus on reducing barriers to effectively integrate One Health. Experiences of One Health projects must be disseminated, and to raise awareness, education programmes must integrate One Health into curricula.
Keywords
Introduction
Worldwide, emerging and re-emerging infectious diseases are increasing due to globalisation and global warming [1]. It is estimated that more than 60% of infectious diseases are zoonotic, meaning that the diseases can be transmitted between animals and humans. In Europe, Campylobacter spp. and Salmonella spp. are the most commonly reported zoonotic bacteria [2]. The Covid-19 pandemic has highlighted the threats and risks at local, national and international levels associated with the emergence of an infectious disease that can spread quickly within and across species [3]. Such disease outbreaks pose challenges to public and animal health and highlight the relevance of sharing solutions to tackle infectious diseases already in their origin and with a One Health approach in mind [1].
The One Health approach refers to establishing coordination, communication and collaboration to achieve optimal health outcomes for humans, animals and the environment [4]. Previous studies have emphasised the need for interdisciplinary research and One Health projects [5,6]. The importance of bridging the silos of the sectors working on One Health themes has been pointed out [7,8]. This is the first study to investigate Swedish One Health practices by gathering the experiences of researchers working with One Health. Sweden can demonstrate a long tradition of working with One Health [9]. The One Health practices referred to in this study are comprehensive surveillance and control measures for infectious and zoonotic diseases as well as the effort of working together across agencies in general. Through thirteen qualitative interviews, the study aimed to identify barriers and opportunities of One Health cooperation, communication and coordination practices, to provide examples for integrating and optimising One Health practices in Swedish agencies as well as in other countries and agencies. The focus was on cooperation, communication and coordination, as these are three aspects that are crucial for successful One Health activities [10,11]. The research was based on the concepts of knowledge translation and transfer as well as agenda setting. Hitziger et al. and Conrad et al. provided the starting point by suggesting how networks can create a basis for knowledge translation and facilitate learning from existing examples and practices [10,12]. The view on agenda setting emphasised science to policy translation, as well as the narrative of pushing topics, in this case One Health, onto the political agenda [13,14].
Methods
Interviews with Swedish experts
Qualitative interviews were conducted from March to October of 2020. To identify relevant interviewees, a convenience sampling strategy was employed to take advantage of the facilitated access to interviewees [15]. All but one interviewee were part of the One Health European Joint Programme (OHEJP). OHEJP is a European Union-funded project, involving 44 institutes to enable interdisciplinary research projects on One Health topics such as zoonoses and antimicrobial resistance [16]. Targeting OHEJP participants ensured that interviewees had experience with One Health activities. The focus was on national experiences and practices to unveil unique insights into One Health practices and outbreak-related operations relating to One Health. Thirteen interviews with experts were conducted: four from the Public Health Agency, two from the National Food Agency, six from the National Veterinary Agency, and one from the Swedish Environmental Protection Agency. Supplemental Material 1 presents the interviewees who are in administrative and research positions, information about their workplace as well as their general background and work area. Each interviewee was assigned a number to be able to link them to their background and work area when quoted in the Result section. The limited number of interviewees from the National Food Agency and the Swedish Environmental Protection Agency was due to the lack of contacts and responses from experts in those agencies.
Data collection method and analysis
An interview guide was constructed on topics emphasised in the literature as well as themes arising regarding the Covid-19 pandemic (see Supplemental Material 2). The interview guide was reviewed by a social science and a veterinary expert. Subsequently, five pilot tests were conducted, the first with a PhD student to test the clarity and coherence of the questions as well as the approximate duration of the interview. The remaining four pilot tests were conducted with experts from the Danish National Food Institute and Public Health Institute to refine the questions, examine the duration and enhance the validity of the interview guide. Expert interviews were conducted to gather both technical and context-specific information pertaining to One Health practices within and across institutes [17]. Informed consent was obtained and the reasons for undertaking the research were explained before the start of each interview. The interviewees were contacted via email and interviews were held online via Microsoft Teams or Skype for Business where audio and video were recorded. The interviews were semi-structured and lasted between 40 and 60 min.
The files were transcribed applying intelligent verbatim transcription. This means that filler words were removed and there was light editing of grammar to facilitate the analysis and to reflect the accurate meaning when interviewees were quoted. After the transcription, all files were once again reviewed. NVivo software (NVivo Pro, version 12) was used for the thematic content analysis. The software supported the process of establishing codes. Based on the interview guide and informed by scientific literature on One Health implementation and institutionalisation, seven themes were deductively formulated. Each theme has several sub-themes under which the codes were categorised. The themes ‘communication’, ‘coordination’ and ‘collaboration’ pertained to One Health-related activities within and across sectors. The One Health ‘perspective’ theme captured interviewees’ opinions and perceptions of One Health and its implementation in the Swedish agencies. The theme ‘current pandemic’ included topics that emerged through talks about Covid-19 disease surveillance and their experiences with the pandemic, as many interviewees were involved in Covid-19 outbreak-related tasks. Lastly, the One Health ‘projects’ and ‘characteristics’ themes referred to job functions, experiences and tasks generally and within OHEJP. The sub-themes were established to capture how some codes showed patterns, fitting the theme but indicating a specific dimension (see Supplemental Material 3). After establishing the themes, everything was reviewed again to ensure consistent and appropriate categorisation. This paper focuses on the themes that occurred regularly in the interviews or themes that were linked to supporting literature. The COREQ checklist for reporting qualitative research (see Supplemental Material 4) was used to report the findings [18].
Results
To showcase the findings of the interviews, the Results section is split into two, listing the main barriers and opportunities relating to One Health practices in Sweden. For this study, a barrier was defined as an obstacle to successfully integrating the One Health approach in practice within and across the agencies. An opportunity was described as a scenario identified by the interviewee that allowed One Health to be implemented or enhanced.
Barriers
The content analysis identified three barriers to effective One Health practise:
1) Ambiguity of what One Health entails in practice
None of the four Swedish agencies had implemented a strategy for One Health and for many researchers the term remains intangible. This could impair potential collaborations and the sharing of knowledge, data and openness to different perspectives [19]. While the interviewees generally expressed support for the One Health approach, there was some confusion about how to translate the abstract approach into concrete practices. One of the interviewees, for example, working in the area of disease surveillance, emphasised the challenges of applying the concept of One Health, ‘So then I realised that all of us are talking about One Health surveillance but none of us really knew what it was and that it was just this abstract concept’ (9, Veterinary Agency).
2) Lack of engagement of the environment sector
Certain collaboration structures have been established between the Environmental Protection Agency and the Veterinary Agency in terms of wildlife, and with the Public Health Agency regarding outdoor recreation and access to green areas for schoolchildren, however, these collaborations are limited and case-specific. The analysis revealed no connections between the Environmental Protection Agency and the Food Agency, although an obvious avenue would be through their mutual topic of water management, ‘as nature-based solutions can contribute to clean drinking water’ (13, Environmental Protection Agency). Interviewees were uncertain about the role, contribution and engagement of the environment sector. The absence of environment in One Health projects was explained as the result of holding different priorities and focuses. Although One Health is not a work area of the Environmental Protection Agency, the interviewee referred to their personal advocacy for One Health:
I have been trying to develop these contacts, but the interest hasn’t been really great from the agency, from my agency, to develop a work area on this (13, Environmental Protection Agency).
3) Legislative differences
In Sweden, ministries steer the agencies, dictating the legislation and mandates that authorise the agencies to carry out policies [20]. Some interviewees lamented that legislation is not always straightforward, which leaves scope for interpretation. This can therefore influence the selection and method used to sample health-related data and how it is analysed, which can affect the comparability of the results. It can also pose problems in terms of identifying who is responsible for implementing and performing tasks. Further, agencies have different mandates, which has an impact on the prioritisation of different areas. In an outbreak situation, for example, this can lead to different aims and procedures within sectors. Interviewees from the Public Health Agency and the Food Agency noted that there have been different approaches in foodborne outbreaks. Staff at the Public Health Agency argued that they wanted to find the source of the outbreak and take measures ‘to stop the food getting into the market that we know is contaminated’ (4, Public Health Agency). An interviewee from the Food Agency also experienced this conflict and explained,
‘I guess something that sometimes becomes obvious is that different agencies will have their different focus and sometimes that can collide quite often, if you compare public health and food. [For] [t]he public health [agency], [it] is really clear that it is the public health that is their focus. And for the food sector, we also have the companies, the food producers . . ., it is in our mission to support them. And that can become a source of irritation perhaps’ (5, Food Agency).
Opportunities
The analysis identified four opportunities for improving One Health practise:
1) Well-established collaboration between the Veterinary, Public Health, and Food Agency
Interviewees described how the barriers to reaching out to colleagues at different institutes are low. Communication across sectors take place regularly, such as in meetings for disease surveillance and outbreak investigations, like the Zoonotic Council meeting once a month ‘where they have more strategic discussions around zoonotic issues. That has also been going on for more than 10 years’ (5, Food Agency). Further, the report Surveillance of Infectious Diseases in Animals and Humans in Sweden is published yearly in collaboration with the Veterinary Agency, the Public Health Agency, the Food Agency and the Swedish Board of Agriculture. Since 2009, the agencies ‘have created routines to share the results before writing the chapters. Instead of being three agencies writing pieces of texts that then get collected together, now the writing of the paper is a One Health initiative’ (9, Veterinary Agency). Another initiative is called One Health Sweden, which is a network of researchers and governmental organisations who work with zoonotic diseases and antimicrobial resistance [21]. The initiative was created to build a platform to share experiences and interact and it ‘tried to influence in different ways, so that the politicians in Sweden become aware about what One Health is’ (11, Veterinary Agency). It was emphasised that collaboration is well-received nationally, within and between Swedish agencies and internationally. To engage the environment sector, agencies should ‘invite[d] [them] to the forums where the One Health problems are discussed’ (12, Veterinary Agency).
2) Potential for different terminologies and methods
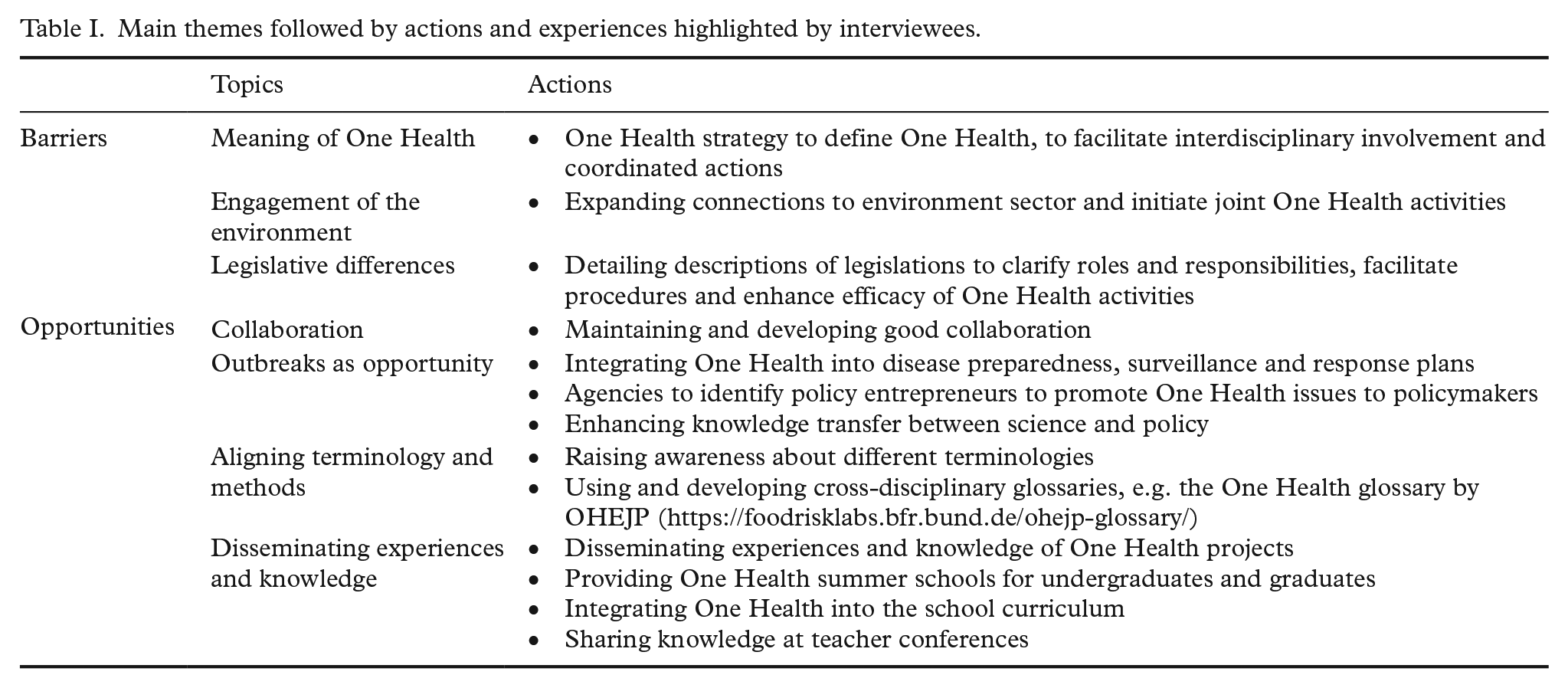
An interviewee emphasised the importance of acknowledging differences across disciplines, especially ‘being modest about that you only understand parts of the other sectors data’ (1, Public Health Agency). To understand terminologies used in different sectors, a cross-disciplinary glossary was mentioned. The glossary established by OHEJP was cited by some interviewees as an example of bridging between the disciplines (Table I).
Main themes followed by actions and experiences highlighted by interviewees.
Discussing methods, analytical approaches and data is crucial to comprehend the research of other disciplines. Different approaches can complement One Health implementation, as methods ‘that you use within the veterinary science can be applied to humans. . . . So we can learn from each other although we have different backgrounds’ (2, Public Health Agency).
3) Opportunity from disease outbreaks
During an outbreak, there is increased collaboration and communication, and policy decisions are more promptly implemented. Examples were the zoonoses Covid-19, salmonellosis and campylobacteriosis. The latter two are recognised as primary causes of foodborne diseases [2]. Covid-19 presents as a zoonotic disease, as it was likely to have been transmitted from an animal to a human, it spreads from humans to some animals and in the case of the Danish mink farms, back to humans [3,22].
An outbreak brings together multiple actors, such as the World Health Organization and national institutes like healthcare providers, medical professionals and research institutes [23]. For campylobacter or salmonella, additional actors are slaughterhouse operators, farmers, consumers and others that put pressure on the authorities [24]. An outbreak can help to ‘try the systems, both nationally and internationally and understand the limits’ (1, Public Health Agency). During a salmonella outbreak, an interviewee observed that this was the time ‘when you can build something together’ (9, Veterinary Agency). This was also apparent for the Covid-19 outbreak, as laboratory testing for Covid-19 was supported by the Veterinary Agency, which would not have been possible before the pandemic due to data safety restrictions. Nevertheless, to be able to assist in an outbreak situation, plans and strategies need to be already in place before the outbreak, as one interviewee put it,
If you don’t establish how this collaboration should work in peace time, in war time it would almost take more time to establish the collaboration than the time is safes [sic] by having that help (9, Veterinary Agency).
4) Disseminating experiences and knowledge
Learning from each other is key to aid other countries or institutes to build on existing knowledge. Experiences could describe ways to overcoming potential technical-, resource- or person-related challenges. Dissemination of examples of One Health projects was suggested, to share ‘what they are doing well, why and how this can be put in practice, what has been done and how it was done’ (9, Veterinary Agency).
Another way to promote One Health is education and to foster ‘knowledge building about the relationship that our life depends on nature and biodiversity’ (13, Environmental Protection Agency). Interviewees cited One Health summer schools and one interviewee shared their experience at a schoolteacher conference, presenting the One Health approach, suggesting that education about One Health should begin in schools.
Table I summarises the topics related to the barriers and opportunities that were identified by the interviewees. It goes further to present actions that were based on the interviewees’ suggestions or concluded from the literature. The actions were based on the Swedish case, however, they could be adapted to other agencies or countries.
Discussion
The analysis focused on practices and demonstrated that there were barriers and opportunities that need to be addressed for successful One Health institutionalisation and implementation.
In Sweden, the Public Health Agency, the Veterinary Agency, the Food Agency and the Environmental Protection Agency are all in close proximity to one another. The geographical closeness of the agencies might facilitate collaboration across agencies. However, there were only few interviewees from the Food Agency and the Environmental Protection Agency. This was a limitation of the convenience sampling strategy and indicates that the results cannot be generalised. However, the opinions of the interviewees relate to their work experiences and were interpreted in consideration of their respective contexts. Although the contexts of other countries might vary, Sweden could be used as an exemplar, showing that successful collaboration stems from regular exchange, from cooperation on reports and surveillance activities as well as from initiatives like One Health Sweden [9].
These established routines and cross-disciplinary meetings facilitate collaboration between the agencies and on an institutional level. However, practically, some challenges for the integration of One Health into everyday life still persist. Implementing a One Health strategy could clarify the meaning of the approach, facilitate interdisciplinary activities and foster the transformation of One Health into coordinated actions. A One Health strategy could be a basis for existing collaborations and encourage the engagement of the environment sector as well as its involvement in One Health networks and activities [25]. For meaningful cooperation between the Environmental Protection Agency and the other agencies, existing collaboration could be expanded by engaging in communication on common themes.
Disease outbreaks such as salmonella, campylobacter and Covid-19 can inspire the development and implementation of legislation. Some interviewees described the opportunities to shape the political agenda and to accelerate policy implementation in an outbreak situation. There can be opportunities for the political agenda to be set and for policies to be implemented when a policy window opens. The policy window opens when the problem, policy and politics streams align [13,26]. In this case, the problem stream refers to a disease outbreak, and the policy stream to proposed solutions, such as surveillance, preparedness and response plans. The politics stream refers to interest groups advocating for the issue and to the capacity and preparednessf politicians to acknowledge the problem. The rapid response to the Covid-19, campylobacter or salmonella outbreaks was due to several interest groups that came from various sectors, and due to public awareness of the urgency. In addition, there can be international pressure if an outbreak in one country spills over into a neighbouring country, or into many parts of the world, as was the case with Covid-19 [3]. This pressure forces governments to make rapid decisions. Consequently, scientific development in outbreak situations is quicker and the science to policy connection is closer [27]. The Covid-19, campylobacter and salmonella outbreaks opened policy windows that led to policy change. For example, campylobacter policies and the salmonella control programme implemented in Sweden enhanced surveillance and control measures and led to a decrease in cases [9]. For Covid-19, surveillance, preparedness and response plans were rapidly adapted and new strategies were developed [28]. The veterinary laboratory tested human samples for Covid-19, which would not have been possible before the pandemic due to data security issues. Other Covid-19 policies concerning the public sector were quickly released and subsequently adapted where necessary, such as restrictions on travel and public gatherings [28].
Interviewees who were involved in outbreak management remarked that during an outbreak, or in ‘war times’, outputs are generated faster to provide emergency responses. After the ‘war’, it is important to learn from the close collaboration and coordinated responses. In ‘peace time’, meaning routine work environments after (or before) an outbreak, there is an entry point for One Health considerations to be integrated into preparedness, surveillance and response plans. Consequently, effective collaboration across sectors could be maintained and awareness for One Health on institutional and political levels raised. Every outbreak is an opportunity for One Health to get through the policy window and onto the political agenda. To facilitate this, advocates or policy entrepreneurs who promote these issues to decision makers are needed. Policy entrepreneurs must be able to translate scientific findings for policymakers. Agencies need to identify their advocates to push One Health onto the political agenda. These policy items must be described well as the outcome may have implications for both human and animal lives. A clear stewardship of the respective ministries aids researchers in determining the roles, responsibilities and processes for the implementation of legislation.
Recognising the complexity of translating knowledge from various disciplines is important. It is unlikely to create a common terminology across all disciplines, but it is possible to be aware of the differences and to acknowledge them. A cross-disciplinary glossary could highlight sector-specific terminology and terms that share the same meaning across sectors. Using and developing the glossary could also strengthen cross-disciplinary research. It could foster knowledge translation and enable researchers and potentially policymakers to comprehend the work of various disciplines [14,29]. Simultaneously, researchers need to communicate effectively to reveal differences in terminologies, methods and analytical techniques. Establishing opportunities to discuss scientific themes across sectors would facilitate a comprehensive understanding of different contexts [11,30,31].
Further, One Health education via One Health summer schools and school-based education fosters knowledge building. Schoolchildren, for instance, are receptive to topics like sustainability and climate change and have influence on sustainable purchasing behaviour [32]. Education leads to more awareness of issues like sustainability and climate change, and teaching children about One Health could have the same effect, increasing the general awareness of those interconnected topics. Education could also be useful in promoting the topic within and beyond the commonly involved institutes (public health, veterinary, food and environment) and include other actors that could benefit from being aware of and acknowledging the benefits of One Health, such as hospitals, health insurances companies, pharmaceutical companies, economic stakeholders and many more.
Conclusion
This study has illustrated that while collaboration within and across veterinary, public health and food agencies is good, the environment agency still needs to be engaged. Further, there are some challenges to practically integrating One Health into the everyday work of researchers. A One Health strategy on an agency level could help to define One Health, and clarify roles and responsibilities. Experts need to be aware of the different terminologies and practices when collaborating. Further prospects for One Health integration include exploiting disease outbreak situations, implementing interdisciplinary approaches and advocating to policymakers. Agencies need to identify and employ policy entrepreneurs to push One Health onto the political agenda. The dissemination of One Health experiences and the integration of One Health into the school curriculum will raise awareness of the approach. Understanding the barriers and opportunities will be beneficial when integrating One Health considerations in the Swedish context and more widely. For a successful implementation of the One Health approach, more research should be conducted to enhance understanding of institutional contexts, cross-agency cooperation, and the needs and perceptions of researchers.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948211024483 – Supplemental material for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination
Supplemental material, sj-docx-1-sjp-10.1177_14034948211024483 for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination by Sarah Humboldt-Dachroeden in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-2-sjp-10.1177_14034948211024483 – Supplemental material for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination
Supplemental material, sj-docx-2-sjp-10.1177_14034948211024483 for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination by Sarah Humboldt-Dachroeden in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-3-sjp-10.1177_14034948211024483 – Supplemental material for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination
Supplemental material, sj-docx-3-sjp-10.1177_14034948211024483 for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination by Sarah Humboldt-Dachroeden in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-4-sjp-10.1177_14034948211024483 – Supplemental material for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination
Supplemental material, sj-docx-4-sjp-10.1177_14034948211024483 for One Health practices across key agencies in Sweden – Uncovering barriers to cooperation, communication and coordination by Sarah Humboldt-Dachroeden in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
I would like to express my great appreciation to all interviewees who shared their time and expertise with me for this study.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the One Health European Joint Programme for Work Package 7 ‘Sustainability’ (Grant Number 773830).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.