
Abstract
Aims: We examined the relationship between loneliness and health among young adolescents. We also investigated the validity of a single-item measure of loneliness by comparing this to a composite score. Methods: The current data come from a nationally representative sample of 11- to 15-year-old adolescents (N=3305; F=52%) from Denmark collected in 2014 as part of the Health Behaviour in School-aged Children (HBSC) collaborative cross-national survey. Results: A series of binary logistic regressions showed that higher loneliness among adolescents, whether measured using the single- or multi-item measurement, was associated with poorer self-rated health, higher frequency of headache, stomach ache, backache, difficulties sleeping, greater sleep disturbance and more instances of feeling tired in the morning. Those associations were relatively consistent across sex and age groups. Conclusions:
Introduction
Loneliness is a negative emotional state caused by the discrepancy between an individual’s desired and actual social relationships [1]. It affects people of all ages, following a U-shaped curve over the lifetime, peaking among adolescents and older adults [2,3]. The peak in loneliness among older adults and the association with various physical health and sleep outcomes have been extensively examined [4]. However, there is significantly less examination of whether the adolescent experience of loneliness is associated with physical health complaints. The current study addresses that gap in the literature.
Loneliness, health and sleep
Epidemiological studies show loneliness, among older people, is associated with a 26% increase in early mortality [5] and that it is an independent risk factor for incident myocardial infarction and stroke among adults [6]. Those health effects of loneliness, according to leading theories of loneliness [7], come from over-activation of systems that would normally encourage us to seek social affiliation, including the hypothalamic–pituitary–adrenocortical axis, with dysregulation contributing to inflammatory processes that play a role in hypertension and coronary heart disease, but also contribute to chronic pain, including chronic backache [8]. Some of those health effects have been explored among lonely youth, but there are few studies. Current evidence shows loneliness among youth is related to more frequent use of medical services [9], poorer self-reported health in early [10,11] and late adolescence [12] and the reporting of somatic complaints [13].
Research examining sleep and loneliness is also pertinent to our discussions, given the importance of sleep for youth brain development, including memory development, executive functioning [14] and cognitive performance [15]. Sleep also provides restorative effects for ensuring good health [16], with high co-morbidity between poor sleep and various mental-health and psychiatric disorders [17]. Loneliness among adults is associated with less efficient sleep and greater restless sleep [18] and more daytime sleepiness [19]; there is no association between loneliness and overall amount of sleep [18 –20]. Similar findings are evident among youth: among young adults, loneliness has been associated with poorer self-reported sleep quality and daytime sleepiness [21]; among young adolescents, sleep was still affected, even when youth no longer reported feelings of loneliness [11].Those findings, although scarce, provide some support for the Perfect Storm model [22]. Within that model, a combination of biological and psycho-social pressures result in poor quality sleep that is short and ill-timed. Given the scarcity of research examining sleep and loneliness among youth, and the importance of good sleep for academic achievement [23,24], further examination of the association between youth loneliness and poor sleep behaviour as a robust finding is essential.
Measures of loneliness
Loneliness is measured through the use of questionnaires and interviews. The Loneliness and Social Dissatisfaction scale [25] and the Loneliness and Aloneness Scale for Children and Adolescence [26] are commonly used measures for youth. Both scales are lengthy, which render them impractical for larger population surveys. Another commonly used loneliness measure, particularly in the adult literature, is the UCLA loneliness scale [27], which has been revised and shortened for use in population surveys, with the development of a three-item measure [28], an eight-item version [29] and a four-item measure [30]. Research has shown similar convergent validity across all adaptations of the UCLA [31]. Those shorter measures of loneliness are favoured in population surveys. Single items of any construct are also discernible for their practical advantages such as ease of application and brevity [32].
The use of direct measures of loneliness is a continued area of interest, and establishing concurrent validity of a single-item loneliness measure is important, particularly given its use in surveys where it can provide a practical advantage. Direct, self-labelling single statements to assess an individual’s loneliness have been used in previous research [33 –35]. However, such direct measures of loneliness may carry an element of social stigma, and people might be reluctant to self-identify as ‘lonely’ [36]. Therefore, it may be the case that direct measurement of loneliness will result in underestimated reports of loneliness, and more indirect measurement of loneliness – such as the UCLA – may be more accurate and thus preferable for inclusion in surveys. However, there is a lack of research examining the level of agreement between the two measures, and such an examination is absent among adolescents.
Shiovitz-Ezra and Ayalon [33] compared the three-item UCLA measure with a single-item loneliness question. Results showed that more than 50% of respondents who were identified as ‘lonely’ on the direct single item were classified as ‘not lonely’ on the more direct measurement. That result is supported by Victor et al. [36] who reported a 40% classification differentiation between direct and indirect measurements of loneliness. Few surveys with young people have included the two different measures of loneliness, so it has been impossible to explore differentiated classification of child and adolescents as lonely. In the current study, because a single-item loneliness measure and the four-item loneliness measure were completed by young people, we were able to explore the identification of young people as lonely using both measurements, exploring differences in classification. In addition, we could explore how the different measurement tools predicted health and sleep complaints among adolescents, examining whether they differentiated predicted outcome.
Current study
Using self-reported data from the Health Behaviour of School-aged Children (HBSC) survey from Denmark, we examined (a) comparisons between the two different measures of loneliness in terms of classification and key demographics, and whether (b) higher levels of loneliness during adolescence are associated with health and sleep complaints, (c) those associations are present when using a multi-item measure of loneliness and a single-item measure and (d) any associations with health and sleep are moderated by age and sex.
Method
Participants
The data used in the current study were collected as part of the HBSC collaborative cross-national survey. The HBSC collects data every four years from adolescents in three age groups (11-, 13- and 15-year-olds) from 47 countries and regions across Europe and North America. The current study utilises data from Denmark collected in 2014. The participants were all students in the fifth, seventh and ninth grade (corresponding to ages 11, 13 and 15 years) in a sample of schools drawn from a complete list of private and public schools. One hundred and seventy schools were invited to participate, and 48 accepted (participation rate for schools: 28.2%). The most common reasons for non-participation were (a) the school had recently participated in a similar health survey or (b) lack of time and resources caused by the implementation of a major national school reform. The response rate was 86.6% of all students in the participating classes, with numbers of adolescents as follows in each grade: grade 5 (aged 11 years): N=1480, 33% of sample, Mage=11.82 years, SD=0.41; grade 7 (aged 13 years): N=1575, 35% of sample, Mage=13.81 years, SD=0.41; and grade 9 (aged 15 years): N=1479, 32% of sample, Mage=15.83 years, SD=0.41. The current study includes 3305 students with complete data on all variables (73% of original sample; grade 5: N=841; grade 7: N=1202; grade 9: N=1262).
Measures
Data were collected through self-completion of the internationally standardised HBSC questionnaire in the classroom [37]. In Denmark, the following loneliness measures were included in the HBSC questionnaire: (a) a composite loneliness score comprised of items from the UCLA loneliness scale and (b) a single-item loneliness measure that asked ‘Do you feel lonely?’
With regard to the composite loneliness score, the four-item UCLA measure [30] includes the following items: How often do you feel isolated from others? How often do you lack companionship? How often do you feel left out? How often do you miss feeling close to someone? Participants answered each item using the following scale: 1=never, 2=rarely, 3=sometimes and 4=often. In the current sample, the four-item measure demonstrated high internal reliability (α=0.84). For each participant, responses on the four items were totalled to create a composite loneliness score, with higher scores indicated higher loneliness. Scores ranged from 4 to 16.
With regard to the single-item measure, participants were also asked ‘Do you feel lonely?’ on the following scale: 4=never, 3=sometimes, 2=often and 1=very often. The single-item measure was reverse coded so that a higher score indicated higher loneliness. Scores ranged from 1 to 4.
For health complaints, adolescents rated their own health as 1=really good, 2=good, 3=fair or 4=poor, with a higher score indicative of poorer perceived health. For the current analysis, self-rated health was dichotomised, in line with previous research [13], into ‘poor/fair’ and ‘good/really good’. Adolescents were also asked about the frequency of headache, stomach ache and backache in the past six months, responding on the following scale: almost every day, more than once a week, almost every week, almost every month and rare/never. Each somatic health complaint was dichotomised into ‘not true’ (almost every month and rare/never) and ‘true’ (almost every day, more than once a week and almost every week).
For sleep complaints, adolescents were asked: (a) how frequently, in the last six months, they experienced difficulties in getting to sleep (hereafter ‘difficulties sleeping’; 1=almost every day, 2=more than once a week, 3=almost every week, 4=almost every month, 5=never; scores were dichotomised into ‘true’ (responses 1, 2 and 3) and ‘not true’ (responses 4 and 5); (b) how often they felt tired in the morning; (c) how often they fell asleep in the afternoon after school; and (d) how often they experienced disturbed sleep. Measures (b), (c) and (d) applied the following response key: 1=never, 2=rarer than once a week, 3=approximately once a week, 4=several days a week and 5=every day. Sleep complaints responses where dichotomised into ‘not true’ (never and rarer than once a week) and ‘true’ (approximately once a week, several days a week and every day). A measure of sleep quantity was also included. Following guidelines published by the National Sleep Foundation [38] suggesting children and young adolescents in the current age range should have at least eight hours sleep a night, sleep quantity was dichotomised as either ‘adequate’ (⩾8 hours) or ‘inadequate’ (<8 hours).
Socio-economic status and family dynamics were controlled in our analyses, given their importance for physical health and sleep outcomes [39,40]. Data on family occupational class were derived from the schoolchildren’s reports of their parents’ occupation, which children have been shown to report with reasonable accuracy [41]. Schoolchildren also provided information on the structure of their families and the resources available within the family.
Family occupational class was based on the highest-earning parent and was classified as follows: high (family occupational class I–II), middle (family occupational class III–IV), low (family occupational class V), unclassifiable/missing information (VI) and inactive (VII, including economically inactive parents who received unemployment benefits, disability pension or other kinds of transfer income). In the current analysis, low and inactive were combined to form the ‘low’ category.
With regards to family structure, participants were also given a checklist of people from which they ticked those living in their main or only home. The checklist included mother, father, stepmother (or father’s partner), stepfather (or mother’s partner), siblings, grandparents and adults other than their parents (foster parents or care homes). From those data, respondents were coded as living with both parents, single parent, reconstructed family (i.e. step family) or other. In the current analysis, family structure was recoded into three categories: two-parent family, single-parent family and reconstructed/other (9%).
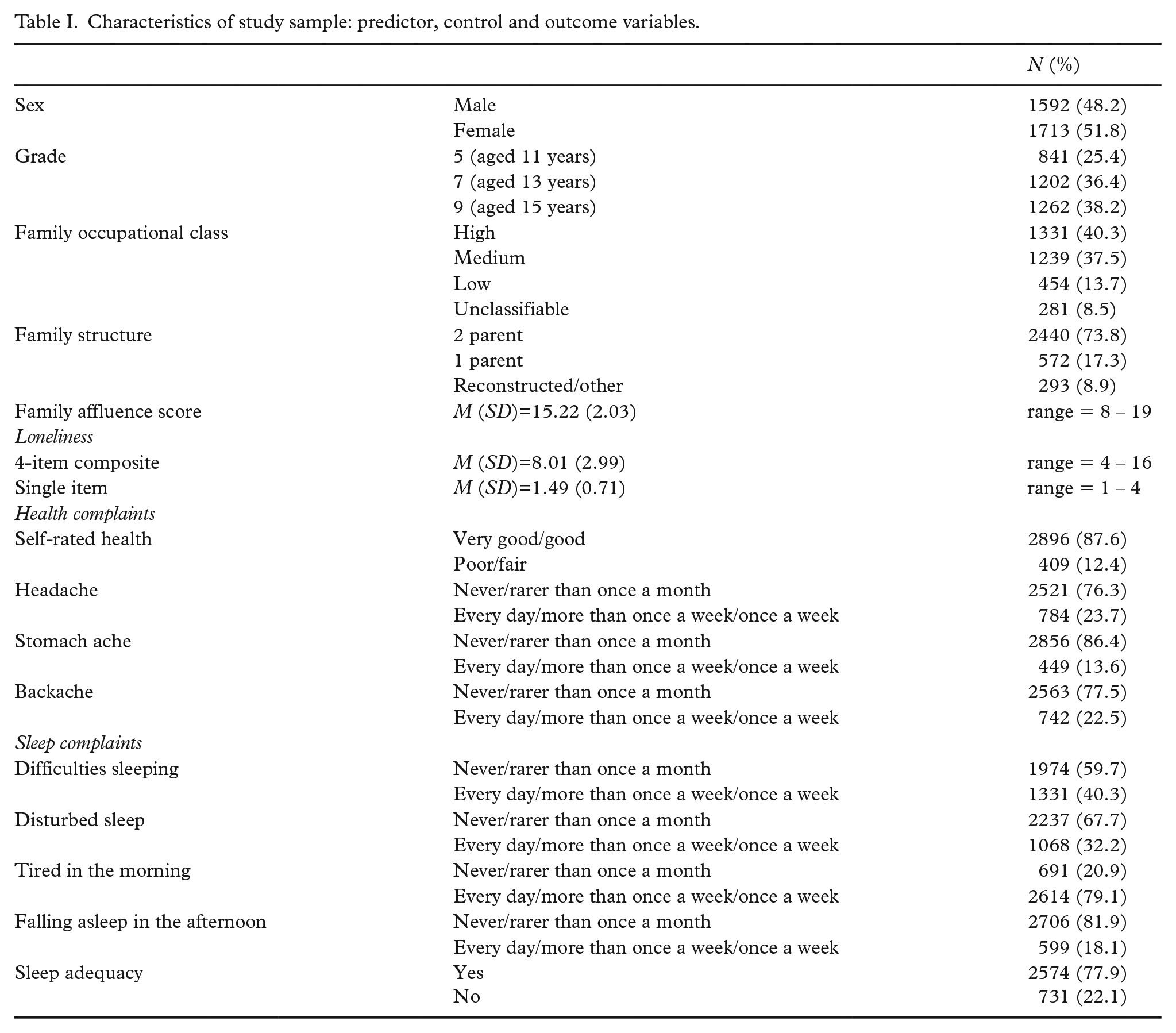
The Family Affluence Scale (FAS) [42] is a child-friendly measure of the resources available to the child’s family. The family affluence scales asks the following six questions: (1) Does your family own a car, van or truck? (2) Do you have your own bedroom? (3) How many computers are there in your house? (4) How many bathrooms do you have in your house? (5) Does your house have a dishwasher? and (6) How many times have you been on holiday abroad in a year? Responses to the items are as follows: items 2 and 5=yes/no responses; items 1, 3, 4 and 6=‘none’, ‘one’, ‘two’ or ‘more than two’, respectively. The FAS was treated as continuous variable, with a higher score indicating a higher level of family affluence. Table I shows the characteristics of the sample.
Characteristics of study sample: predictor, control and outcome variables.
Analysis plan
First, the relationship between the single-item loneliness measure and the multi-item measure of loneliness was explored through correlational analysis. Chi-square analysis was then used to explore whether we could correctly identify adolescents as lonely using the two measures. Participants were divided into two groups – ‘lonely’ and ‘non-lonely’ – using upper quartiles of the loneliness measurements (single item: a score of ⩾3 classified as lonely; composite score: a score ⩾12 classified as lonely). There are no published cut-off points for loneliness, but quartiles have previously been used in research [43 –45] and showed different profiles of behaviour for groups of people categorised using top quartile scores on self-reported loneliness measures. Differences between the two measures and two key demographics – age and sex – were also investigated through a series of analyses of variance (ANOVAs).
Second, a series of binary logistic regressions (BLRs) explored the association between loneliness and health and sleep complaints; regressions were conducting for the single- and multi-item loneliness scores. All analyses were adjusted for family structure, family occupational status and family affluence. The results from the regression analyses are presented, alongside odd ratios (OR) with 95% confidence intervals (CI). BLRs were first completed on the whole sample (N=3305), before being stratified by sex and then age. Moderation effects were examined by comparing the stratified models using Z-scores (Z-scores ⩽1.96 indicating a significant moderating effect). To reduce the potential for type 1 errors, the conservative value of p<0.001 was applied.
Results
Comparisons between the single- and multi-item measure of loneliness
Pearson’s correlation analysis demonstrated a significant and positive relationship between scores on the single- and multi-item measure of loneliness (r=0.622, p<0.001). In addition, the four individual items of the composite score demonstrated strong and significant relationships with both the composite total (r=0.796–0.844, p<0.001) and the single-item measure of loneliness (r=0.484–0.545, p<0.001).
Using the top quartile on each loneliness measure as a cut-off for loneliness, in the current study, 7.69% (n=254) of the sample were classified as ‘lonely’ using the single-item measure, and 14.22% (n=470) as ‘lonely’ using the UCLA composite score. Results from chi-square analysis (χ2(1)=703.76, p<0.001) suggested that children reporting loneliness using one measure did not always do so using the other measure: we found that 70.08% of those children classified as lonely using the single-item loneliness measure were also classified as lonely using the multi-item measure (males=62.9%; females=73.9%). In addition, the number of males who were classified as lonely using their UCLA score who were also classified as lonely on the single-item measure reduced across grades from 78.9% in grade 5 to 58.3% in grade 7 and 58.5% in grade 9; for females, the percentage of those classified as lonely using the UCLA and single-item loneliness scale was relatively stable (68.8%, 78.8%, and 72.8% in grades 5, 7 and 9, respectively). Thus, while there was a reasonable correlation between the two loneliness measures, children were (a) not always consistent in their reporting of loneliness across the two measurements, and (b) less likely to be classified as lonely using the single item if they were male, with that reporting reducing with age.
A series of 2×3 (sex: male/female×age/grade: 11/5, 13/7, 15/9) between-group ANOVAs examined the effects of sex and age on self-report loneliness. For the four-item composite score, there was a main effect of sex on loneliness (F(1, 3299)=136.58, p<0.001, η2=0.040), with females reporting significantly higher loneliness (M=8.61, SD=3.05) compared to males (M=7.36, SD=2.78). There was also a significant main effect of grade on loneliness (F(2, 3299)=11.52, p<0.001, η2=0.007), with post hoc analysis showing that grade 9 adolescents (aged 15 years) reported significantly higher loneliness (M=8.32, SD=2.94) than adolescents in grade 5 (aged 11 years; M=7.69, SD=2.94) or grade 7 (aged 13 years; M=7.89, SD=3.04); there was no significant difference between adolescents in grades 5 and 7 in terms of loneliness. We found no significant interaction between grade and sex on loneliness levels for the composite measure (F(2, 3299)=2.76, p=0.063, η2=0.002).
For the single-item measure, there was also a main effect of sex on loneliness (F(1, 3299)=87.29, p<0.001, η2=0.026). Consistent with findings using the composite loneliness scores, females reported significantly higher loneliness (M=1.61, SD=0.75) compared to males (M=1.37, SD=0.64). Also consistent with the composite loneliness results, there was a significant main effect of grade (F(2, 3299)=9.72, p<0.001, η2=0.006), with adolescents in grade 9 (aged 15 years) reporting significantly higher loneliness (M=1.55, SD=0.73) than adolescents in grade 5 (aged 11 years; M=1.41, SD=.66) and grade 7 (aged 13 years; M=1.48, SD=0.70). As with the composite score, there was no significant difference between adolescents in grades 5 and 7 on loneliness. There was no interaction between age and sex (F(2, 3299)=1.26, p=0.285, η2=0.001). Due to the lack of interaction effects, further moderation analysis will be conducted separately first for sex then by age.
Loneliness and health and sleep complaints
Table II shows that for both measures of loneliness, loneliness was significantly associated with self-rated health, headache, stomach ache and backache, with higher levels of loneliness resulting in an increased risk of reporting poorer health outcomes. In addition, loneliness increased the odds of reporting difficulties sleeping, disturbed sleep, feeling tired in the morning and higher instances of falling asleep in the afternoon. With the exception of sleep adequacy, both loneliness measurements were consistent in their associations with physical health and sleep complaints. For sleep adequacy, higher scores on the four-item UCLA composite measure reduced the odds of experiencing an adequate night’s sleep, but that was not the case for the single-item score.
Association between loneliness (predictor) and physical health and sleep complaints.
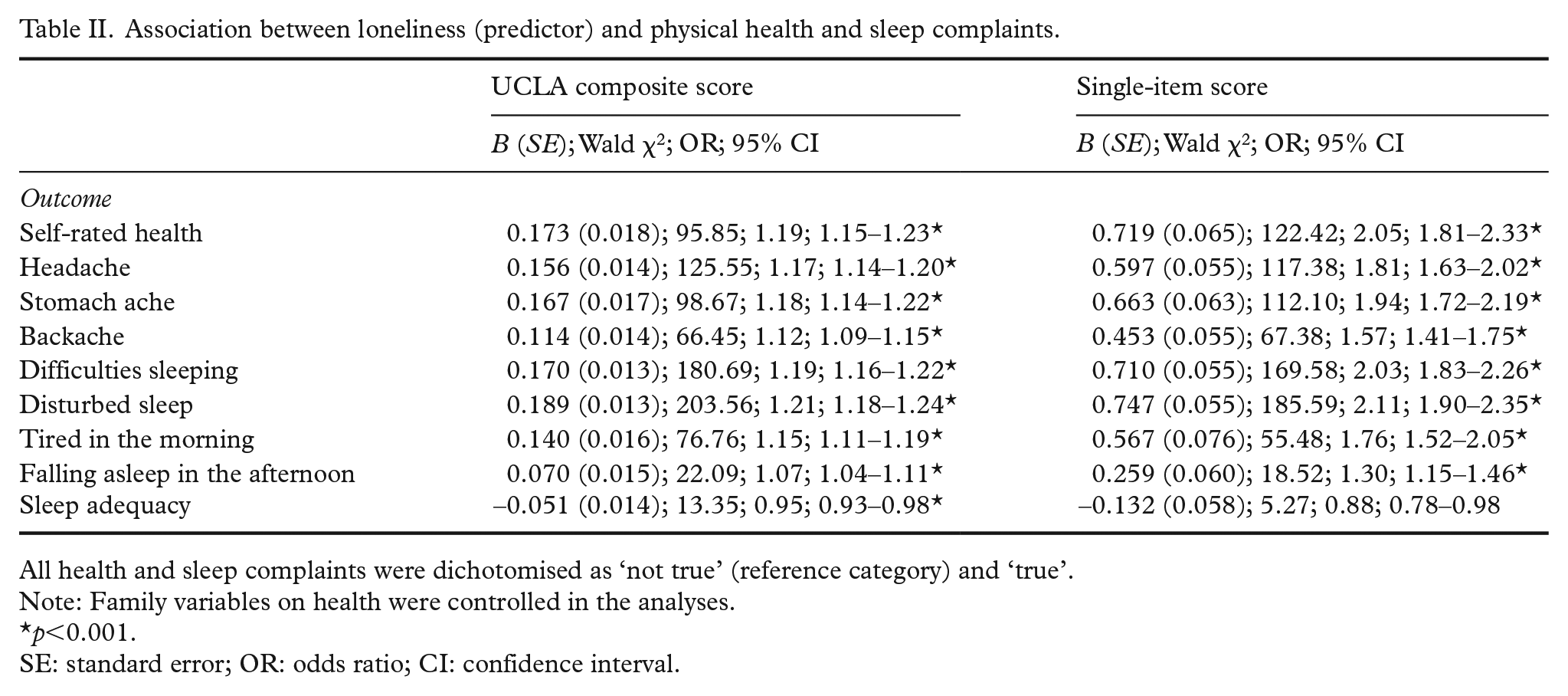
All health and sleep complaints were dichotomised as ‘not true’ (reference category) and ‘true’.
Note: Family variables on health were controlled in the analyses.
p<0.001.
SE: standard error; OR: odds ratio; CI: confidence interval.
It is important to note that effect sizes for all significant effects are small; examination of the confidence intervals of both measures of loneliness showed larger effect sizes for the single-item measure of loneliness compared to the UCLA composite score. Further examination showed the odds of reporting health complaints were reduced when loneliness was measured using the composite measure; odds for self-rated health, headache, stomach ache and backache reduced by 42%, 36%, 39% and 29%, respectively. The same pattern emerged with the sleep complaints, with the odds of reporting sleep complaints reducing when loneliness was measured using the composite UCLA measure (difficulties sleeping 41%, disturbed sleep 43%, tired in the morning 35% and falling asleep in the afternoon 18%).
Sex and age as potential moderators between loneliness and health complaints
Analyses examined the role of sex and age as moderators of the association between loneliness and health complaints, and loneliness and sleep (Tables III and IV). Table III shows that associations between loneliness and different measures of health, including sleep, were comparable for boys and girls. Examination of the two models showed that sex did not moderate the relationship between loneliness and most health/sleep complaints (Z-scores ⩽1.97); sex moderated the relationship only for falling asleep in the morning. There was a significantly stronger effect for females than males on the single item (Z-score=−2.39) but not the composite loneliness score (Z-score=−1.57).
Association between loneliness (predictor) and physical health and sleep complaints stratified by sex.
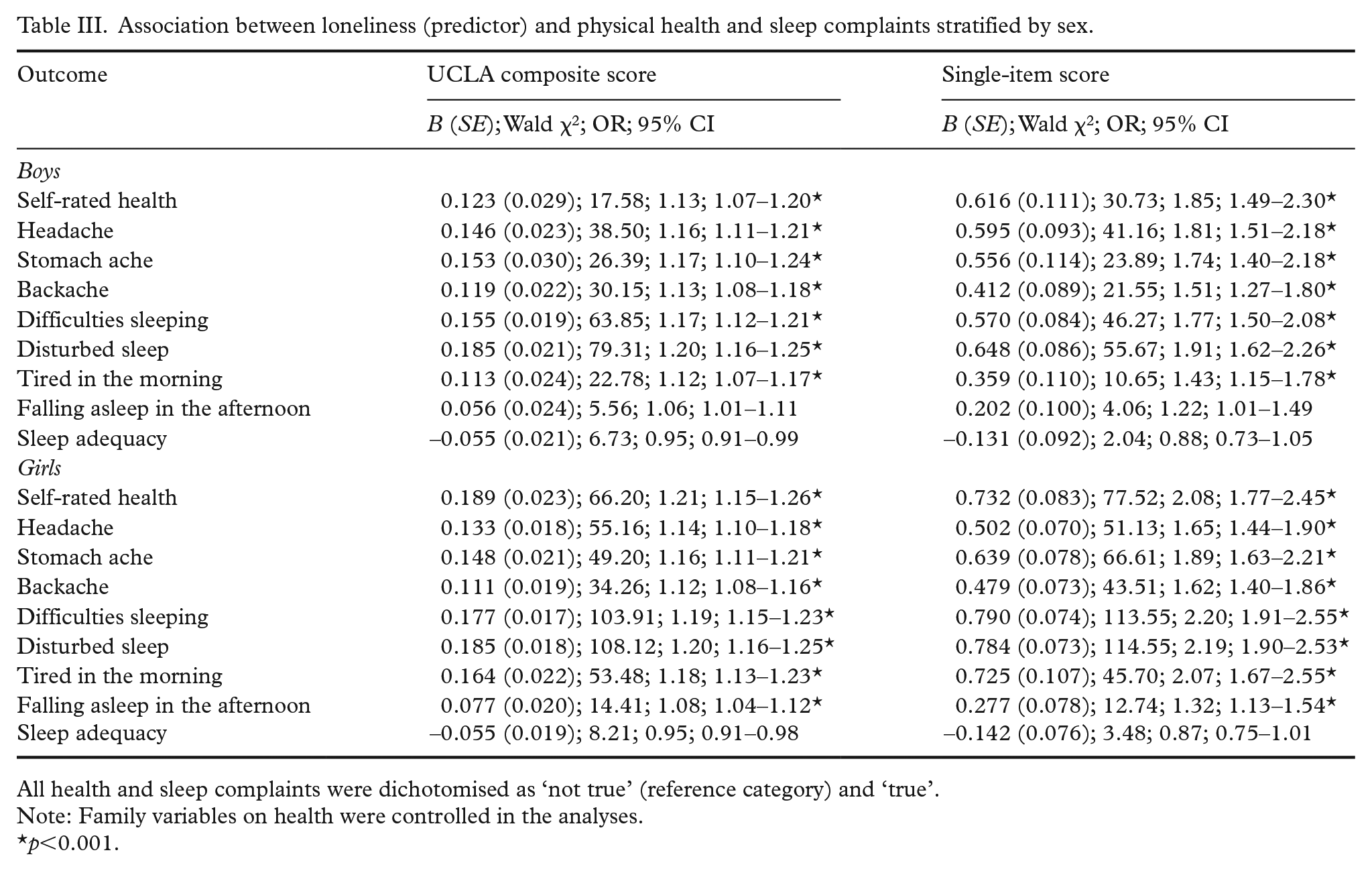
All health and sleep complaints were dichotomised as ‘not true’ (reference category) and ‘true’.
Note: Family variables on health were controlled in the analyses.
p<0.001.
Association between loneliness (predictor) and physical health and sleep complaints stratified by grade/age.
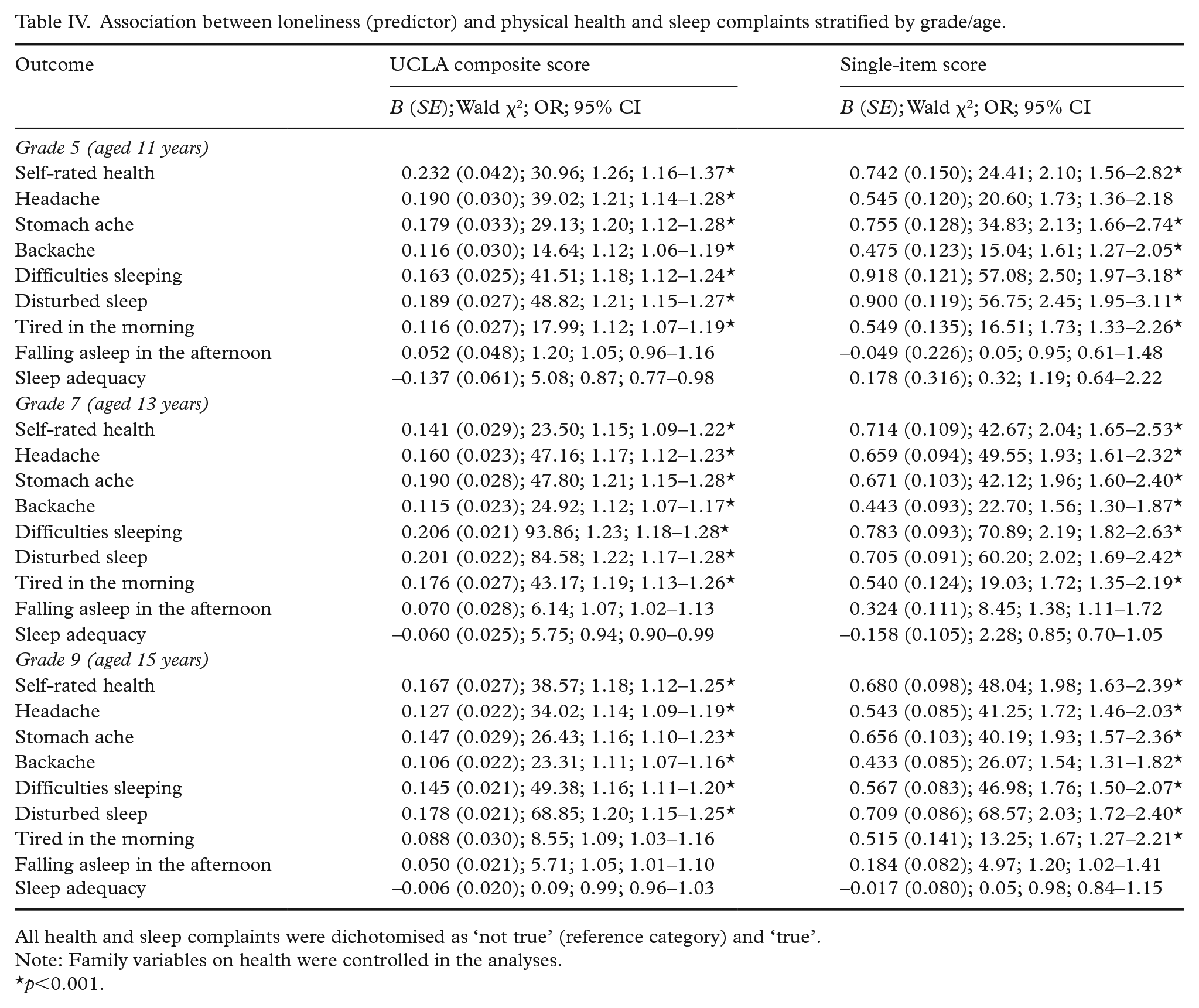
All health and sleep complaints were dichotomised as ‘not true’ (reference category) and ‘true’.
Note: Family variables on health were controlled in the analyses.
p<0.001.
Upon examination of the regression models stratified by age, it appears the association between loneliness and the different measures of health and sleep were robust across the different age groups (see Table IV). Moderation, explored using Z-score comparisons, showed that children aged 11 years demonstrated significantly worse difficulties sleeping than those aged 15 years on the single item of loneliness (Z-score=2.39); on the multi-item loneliness measure, those differences appeared between participants aged 13 and 15 years (Z-score=2.05; 13 years>15 years). Comparisons for feeling tired in the morning showed differences between those aged 13 and 15 years when the multi-item loneliness measure was used (Z-score=2.18). Difference in sleep adequacy between those aged 11 and 15 years were observed when measured by the multiple item.
Discussion
The current study examined whether loneliness was associated with health and sleep complaints among schoolchildren. There were four main findings. First, while there was a reasonable correlation between the single- and multi-item measures of loneliness, a large number of adolescents who were identified as lonely were not classified as such using the multi-item, indirect measure of loneliness. Second, there was a strong and consistent association between loneliness and self-reported general health and sleep complaints. Those findings were evident, even when the effects of family variables on health were controlled in the analyses. Additional analyses suggested the associations with health were robust across sex and age. The exception was falling asleep in the afternoon, which was moderated by sex when using a single-item loneliness measure. Third, the associations between loneliness and different health complaints were consistent across two measures of loneliness, suggesting the effects were robust, providing some justification for the use of a single-item loneliness measure in future population studies with youth. Fourth, the relationship between loneliness and sleep difficulties was picked up more strongly by different loneliness instruments at different ages, suggesting that future work should examine how views of loneliness change with age to impact reporting of loneliness using different measurement tools.
The correlational analysis supports previous research demonstrating a significant relationship between single- and multi-item measures of loneliness [46]. The classification analysis, however, suggests that adolescents identified as lonely using one measurement of loneliness are not always identified as such using the other. Results of the current study support previous research examining differences between direct and indirect measures of loneliness [33,36] that found low concordance between the two measurements approaches. The current results suggest that when children were classified using quartiles, more children were classified as ‘lonely’ when using an indirect, composite measure of loneliness. It could be the case that fewer children wanted to identify as ‘lonely’ due to the stigma surrounding loneliness [47]. It is important to note the classification differences present in the current study could have been influenced by the underlying differences in the response scale in the two measures. However, considering the results are in support of previous findings, it is a finding which warrants further investigation within other populations.
Exploring how views of loneliness change with age to impact reporting of loneliness using different measurement tools will be an important part of future research. In the current study, older male adolescents who scored high on the indirect measure of loneliness were less likely to identify themselves as ‘lonely’ using the single-item loneliness measure. Thus, male adolescents may be less likely to provide accurate information on their loneliness using the single-item measurement because they are more aware of societal stigmatisation of loneliness as it relates to their sex. Previous research demonstrated females were more likely to identify as lonely using a direct measure, whereas no sex differences appeared when using an indirect measure [47]. Exploration of sex-based stigma surrounding loneliness will be important in understanding how different measures lead to the reporting of different prevalence regarding loneliness, and how that might affect treatment options.
While it is difficult to compare the findings in this study with other studies due to differences in national context and study population, there are a number of other studies showing loneliness to be related to poor self-rated health among youth [11] and somatic health complaints [13], suggesting the associations are reliable. Those studies applied only one measure of loneliness, so it is a new observation that a single item and a composite measure show similar associations in this age group, so it is a new observation that a single-item measure shows similar associations with health complaints for this age group. There are only a few studies on loneliness and sleep among adolescents [11,21], but consistent with previous studies, we found a clear association between loneliness and sleep problems.
The current study is cross-sectional, precluding conclusions regarding causal pathways. Loneliness may be an antecedent of health and sleep problems and vice versa, or they may be a result of other factors. Future work will want to continue examination of the association between loneliness and poor health among youth using longitudinally designs, exploring the across-time relationships and other factors that might impact the relationship.
Another important finding was that the majority of young people in the current study reported an adequate amount of sleep, but also reported feeling tired in the morning. In line with the Perfect Storm model of adolescent sleep [22], it could be the case that adolescents need more sleep than adults to feel rested; such an idea gains ground when we consider the ever-growing pressures placed on youth as they develop into adults, including increasing academic, social and biological demands.
Within the current study, the two different measures of loneliness illustrated a strong and significant relationship, supporting the use of a single-item loneliness measure with youth. What has not been shown before is that the single-item measure and multi-item measures of loneliness show similar associations with health and sleep complaints, and can be used successfully with youth in population surveys. It is important to note that the relative chance that those classified as lonely would report poorer health and sleep complaints was different for the two loneliness measures. Loneliness, when measured using the multi-item UCLA scale, presented lower odds of poor health and sleep complaints than when the single-item measure of loneliness was used. Because those youth who reported being lonely using the single-item measurement were doing so despite the stigma attached to loneliness, the effects between loneliness and health were strongest. We recommend that both direct and indirect measures of loneliness are used in future work so that their predictive validity can be explored in more detail.
Strengths and limitations
It is a virtue of the study that it includes a large and nationally representative study population. However, although the participation rate was high (86.6%), non-participation may result in selection bias. It is possible that those students who were not present on the day of data collection had a high rate of health problems, sleep problems and loneliness. That means the analyses may have underestimated the prevalence of loneliness and its association with health and sleep problems. It is also important to note the included sample reported high levels of family affluence (40% high-income families, high mean FAS scores). Although that may be representative of Denmark as a generally affluent society [48], it is important to consider this when generalising the findings to other populations and samples across the world.
The different response scales to the two loneliness measures could be seen as a limitation: it means classification of youth as lonely was not based on the same underlying response categories. We attempted to overcome the problem by exploring quartiles in our analyses, viewing the HBSC study as a novel opportunity to examine two different loneliness measures, adding to the discussion surrounding the effectiveness and comparability of direct and indirect measurement of loneliness. The applied health measures used in the current study are valid, assessed by qualitative and quantitative studies [49,50]. However, the validity of the current sleep measures is unknown. Previous research has concluded adolescents’ self-reports of sleep are reliable and valid, but that was through the use of extensive and lengthy self-report measures. It may be the case that single items of sleep, or more direct questions relating to sleep quality, are less reliable. We therefore recommend future research focuses on adopting more objective measures of sleep (such as actigraphy watches) to investigate the relationship between loneliness and sleep in young people further. Another limitation in relation to the measurement of sleep in the current study is the lack of other confounding variables – including social media and use of technology before bedtime – that are important in current discussion relating to sleep [51,52]. Additionally, confounding variables to loneliness, such as personality and mental health, which have been previously identified as potential moderators [53], should also be included in future research.
Implications
Given the importance of good health and good sleep for life quality and academic achievement [23,24], it is important to continue to explore adolescents’ health, sleep and feelings of loneliness. We recommend (a) longitudinal studies to unravel whether those phenomena are causally related; (b) studies to uncover the processes that produce the statistical relations between health, sleep and loneliness; and (c) examination of other settings to establish whether the pattern of association is robust.
From a practice point of view, it is important to develop interventions and health-education efforts to fight loneliness among youth. While few published interventions have focused on how to prevent or reduce loneliness among youth, our findings show that those will be important to improve well-being, feelings of general health and sleep functioning. School may be an ideal setting for loneliness interventions because it is possible to target the entire population of adolescents, with current social and political climates ripe to address mental-health problems in the school setting [54,55]. Effective programmes aimed at preventing or decreasing adolescent loneliness may also have more general positive implications for adolescents’ well-being, future academic performance and mental health. Our findings suggest that interventions to reduce loneliness may also have a positive impact on sleep and physical health.
Changing the school class climate to be more including and accepting of differences, for example by focusing on increasing social capital in the school class [56], may also have a positive impact on loneliness. That makes school a unique and important arena for interventions that aim to reduce and prevent loneliness in adolescents.
Conclusions
Research consistently demonstrates an association between loneliness and perceived poor health and sleep problems. In the current study, those associations were evident within a representative adolescent sample when using both a single-item direct measure of loneliness and a multi-item scale of loneliness.
Footnotes
Acknowledgements
We wish to thank Mette Rasmussen, the Principal Investigator of the Danish HBSC study in 2014, for providing the data for analyses. The data sets analysed during the current study are not publicly available, but the data used in the current study can be requested from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.