
Abstract
Aim: ‘Participation and influence in society’ is the first of 11 objective domains in Swedish public health policy. The aim of this article is to investigate the views of the Swedish general population on the impact of a range of health participation activities, and whether these views were associated with sociodemographic characteristics. Methods: The study utilizes a national representative survey of the Swedish population, aged 15 years and over (n = 1500). Results: Apart from voting in regional elections – which most of the respondents believed to be an influential way to make improvements in healthcare (74%) – respondents believed more in individual patient activities than activities associated with adopting a citizen role and acting collectively. A majority of respondents believed in the impact of replying to patient surveys (67%), making a complaint (61%), talking directly to staff (58%) or changing their healthcare provider (54%). Fewer believed in the impact of joining a patient organization (46%), taking part in a citizen council (35%) or joining a political party (34%). Beliefs in impact increased with educational attainment and decreased with age.
Keywords
Introduction
One definition of the mission of public health is ‘the fulfillment of society’s interest in assuring the conditions in which people can be healthy’ [1]. To achieve this, Swedish public health policy covers 11 objective domains, of which the first is ‘participation and influence in society’ [2], further divided into democratic participation, social and cultural participation, and social and practical support [3]. The policy emphasizes that the ‘right to influence and participation applies regardless of gender, age, ethnic background, disability or sexual orientation’ [4].
Among Scandinavian countries, Swedish public health policy is distinctive in emphasizing participation as a strategy to improve social and living conditions [5]. The policy suggests that those who believe they have no control or influence over their own lives and the development of society feel alienated and powerless, negatively impacting on their health [3]. For instance, this might be understood as limited influence over one’s own care and, more broadly, over the local health system and its services. One response is patient and public involvement (PPI) that has been introduced across the European health systems. PPI – the ‘active participation of citizens, users and carers and their representatives in the development of healthcare services and as partners in their own healthcare’ [6] – is presented as promoting everything from greater democratic participation and learning, to empowerment of patients and disadvantaged service users, to enhanced individual health outcomes and public health [7,8].
Being a broad concept, PPI ranges from individual participation in clinical settings to collective participation in policymaking arenas. Typically, patient involvement (the user perspective) is associated with decisions about individual care and seeks to improve personal health outcomes and satisfaction, but may also refer to a patient population helping to shape a particular service [8,9]. In contrast, public involvement (the citizen or taxpayer perspective) takes a broader collective interest such as strategic decisions about health services, and addresses societal values and public health [9,10]. Arguments for public involvement are founded on democratic theory whereas patient involvement is justified on individual choice and patient rights and is a reaction against medical paternalism [8,11]. Benefits of participation may be intrinsic (good in themselves) as well as extrinsic (a means to an end); both may generate public health benefits. For the individual patient, PPI is most clearly linked to empowerment and better management of illnesses, whereas for the collective citizenry PPI is linked to social capital and community action to improve health.
In Sweden, healthcare is funded and provided by regions (county councils) that are democratically governed and elected locally. This makes PPI in Sweden closely entwined with local democratic procedures. The regions are sometimes referred to as ‘service democracies’ functioning as democratic arenas and as public organizations resolving collective needs and interests through service provision [12]. In relation to their democratic function, involvement is generally framed as mechanisms to influence the political process. In addition to voting, participatory activities have emerged; for example, different types of ‘citizen dialogue’. However, over the past decade, patient involvement and empowerment has been the primary policy objective and many national initiatives have been taken, for example the new Patient Law (2014:821) that promotes the individual patient’s position, integrity, autonomy and participation. Participation is increasingly framed as the possibility for patients to participate in patient surveys, express dissatisfaction through complaint mechanisms and to ‘exit’ providers [13]. These activities are more directly aimed at influencing the service provision function, and are part of a ‘consumerist’ movement in Scandinavian welfare states [12].
How people perceive different PPI activities within a region is largely unexplored; for instance, whether people perceive involvement having an impact (effect or outcome in a broad sense [14]). Many aspects determine whether people participate or not, but according to the CLEAR framework one central aspect is ‘that people have to believe that their involvement is making a difference’; that they are ‘responded to’ [15, p.289]. Other important factors include: individual resources, knowledge and confidence (in the health sector also, e.g. type and severity of illness); a sense of attachment or community, which may include a sense of civic duty; opportunities for participation; and being asked for input (i.e. mobilization). However, lack of response, either experienced or perceived, is one of the biggest deterrents to participation [15]. Therefore, it is crucial to understand whether people believe their participation in PPI activities can make a difference. Furthermore, for the benefits of involvement to be equally distributed it is crucial to determine whether sociodemographic differences shape these beliefs. In this article we focus on democratic participation which intends to influence the political process, but also, in line with the PPI concept, participation seeking to influence service delivery by (a) investigating the views of the Swedish general population on the impact of a range of involvement activities available to patients and members of the public, and (b) determining whether such positions are associated with sociodemographic characteristics. Overall, the article seeks to link the concept of PPI to public health policy in a Scandinavian setting.
Methods
Level of investigation
‘Participation and influence in society’ is apparent in many different policy areas and can be measured at different societal levels. Here we focus on participation in the Swedish regions in relation to health services. Population health is dependent on the activities of the regions, together with municipalities and civil society. As regions and municipalities have direct effects on people’s lives, many forms of involvement are best enacted at these levels [2].
Analysis framework
Many models detail different types of PPI activities; for example, according to the level of control over decision-making (consultation, involvement, partnership and shared leadership [16]) or whether participation is invited or not [17]. We focus on two distinctions. The first distinction is between the patient and the public: categories that have different roles, perspectives and interests (sectional vs. societal interests) which may be contradictory [10]. Some activities are classified as both patient and public as there is no clear distinction in the interest being expressed (see Figure 1). Second, we distinguish between individual and collective involvement: whether people contribute individually, or are approached, deliberate or act collectively as a group [1,17]. Collective activities have greater potential to generate social capital contributing to public health through offering membership in a network.
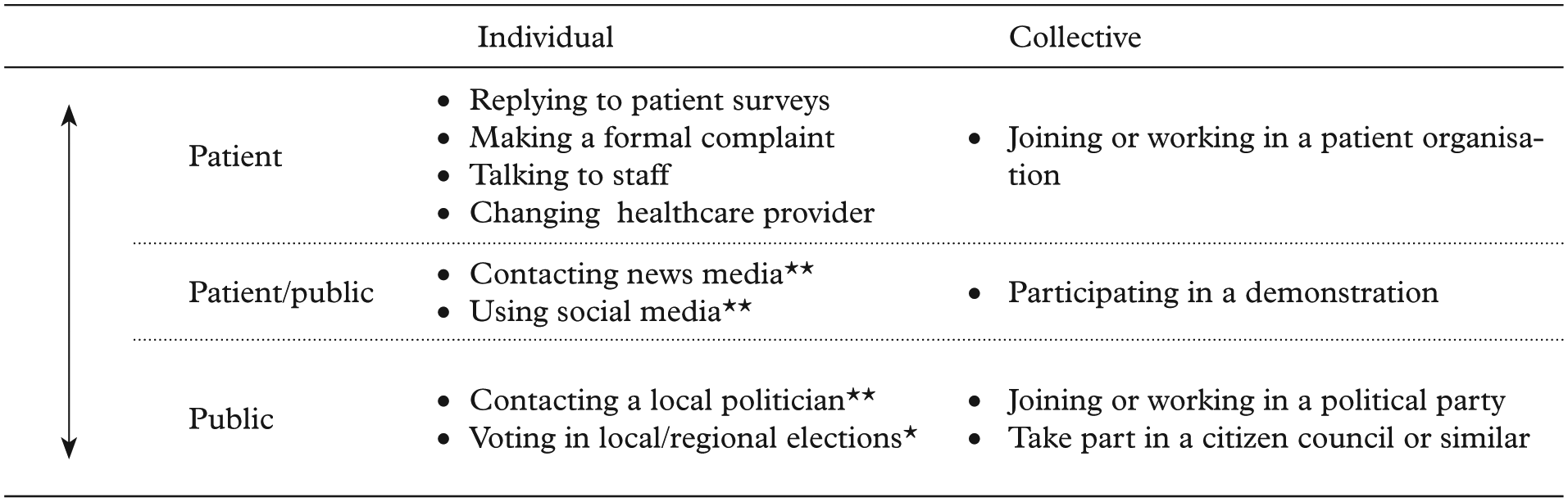
Participation spectrum and activities.
Sample and survey questions
The data is based on a Swedish telephone omnibus survey administered in September 2014 by TNS Sifo. The sample includes 1500 respondents, aged 15 years and over. The initial response rate among randomly selected residents in different regions was 35%. Substitute respondents were sought in pre-defined strata for those individuals that refused to participate or that could not be reached after multiple attempts. Data was weighted by gender, age, working status and area code to be representative of the Swedish population. While not perfect, this is a common approach to reduce non-response bias [18]. The researchers only had access to the anonymized sample and not personal identifiable data.
The respondents were asked on a binary scale (yes/no) which, if any, of 12 proposed involvement activities they thought would result in improvements to healthcare in their region. The activities were compiled from previous regional investigations of involvement and from official information on how people can influence regional healthcare. The order of the 12 involvement activities presented was rotated to avoid response bias. This crude measurement of their perception of the activities’ impact reduced the risk of respondent induced measurement error.
Sociodemographic characteristics
When investigating whether people’s views differ by sociodemographic characteristics we included gender, age and level of education. We also included a proxy for health status: whether people had a long-term condition or not (see Table I).
Sample characteristics.
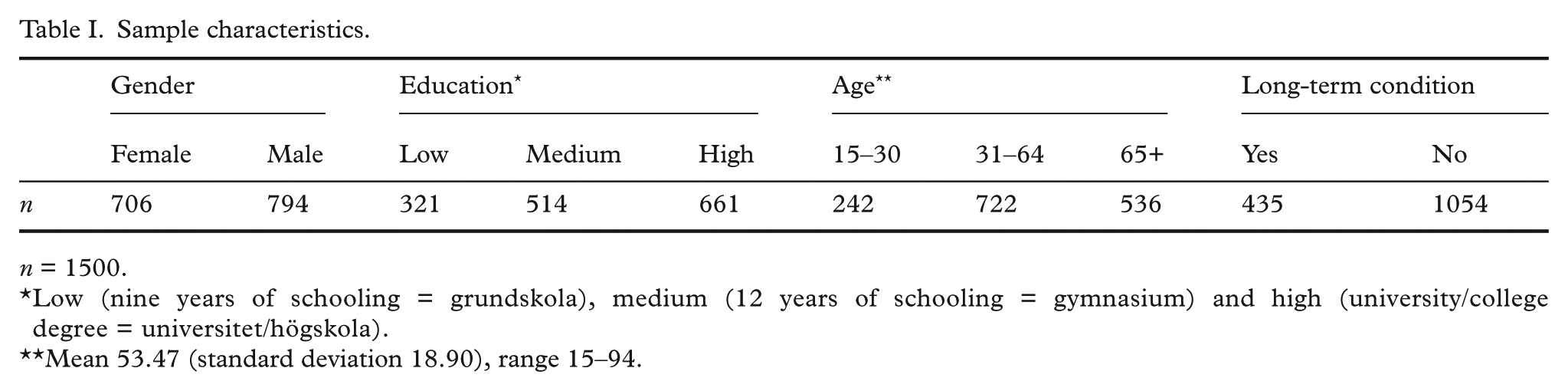
n = 1500.
Low (nine years of schooling = grundskola), medium (12 years of schooling = gymnasium) and high (university/college degree = universitet/högskola).
Mean 53.47 (standard deviation 18.90), range 15–94.
Data analysis
All data were analyzed using Stata (Version 13.0, Stata, College Station, TX, USA). Given the high number of observations, data was assumed to be normally distributed when calculating confidence intervals for proportions allowing for symmetric confidence intervals. The final models all assume a negative binomial distribution, regardless of activity type. Some activity types did display similar means and variance, thus suggesting a Poisson distribution. However, results were robust in either distribution and, thus, negative binomial link functions were used in all models to facilitate between model comparisons.
Results
Perceptions of involvement activities
Table II illustrates that over 50% of the respondents agreed that five of the PPI activities could lead to improvements in regional healthcare. All of these activities were individual. Voting in regional elections was the activity most respondents believed could lead to improvements (74%). Apart from voting, the respondents were most convinced of the impact of involvement activities aimed at individual patients compared to adopting a citizen role and acting collectively. The majority of respondents believed replying to patient surveys (67%), making a complaint to a patient board or to the Health and Social Care Inspectorate (61%), talking directly to healthcare professionals about the need for change (58%) and changing the healthcare provider (54%) could have an impact. Fewer respondents agreed that joining a patient organization, a collective activity, could improve regional healthcare (46%). The respondents believed that collective activities with primarily a citizen perspective were least likely to have an impact: taking part in a citizen council (35%), joining or working in a political party (34%) or participating in a demonstration (26%).
Views on the impact of involvement activities.
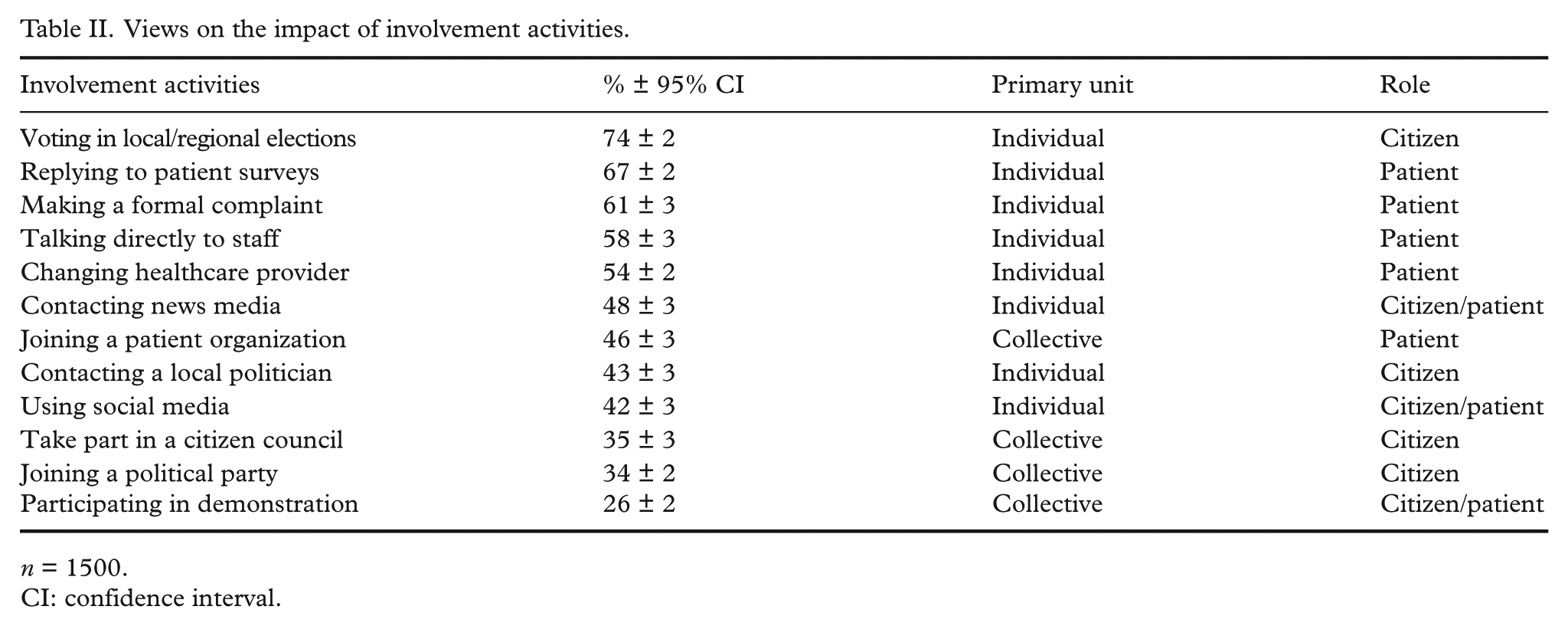
n = 1500.
CI: confidence interval.
Grouping the PPI activities according to unit of participation (individual/collective) and role (citizen/patient), Table III shows that respondents on average believed 4.9 of the nine individual activities would have an impact (normalized mean: 0.55) compared to 1.4 of the four collective activities (normalized mean: 0.35). Furthermore, respondents believed in the impact of 2.7 of the five patient activities (normalized mean: 0.54), 1.9 of the four citizen activities (normalized mean: 0.47) and 1.1 of the three citizens/patient activities (normalized mean: 0.39).
Views on the impact of involvement activities: grouped.
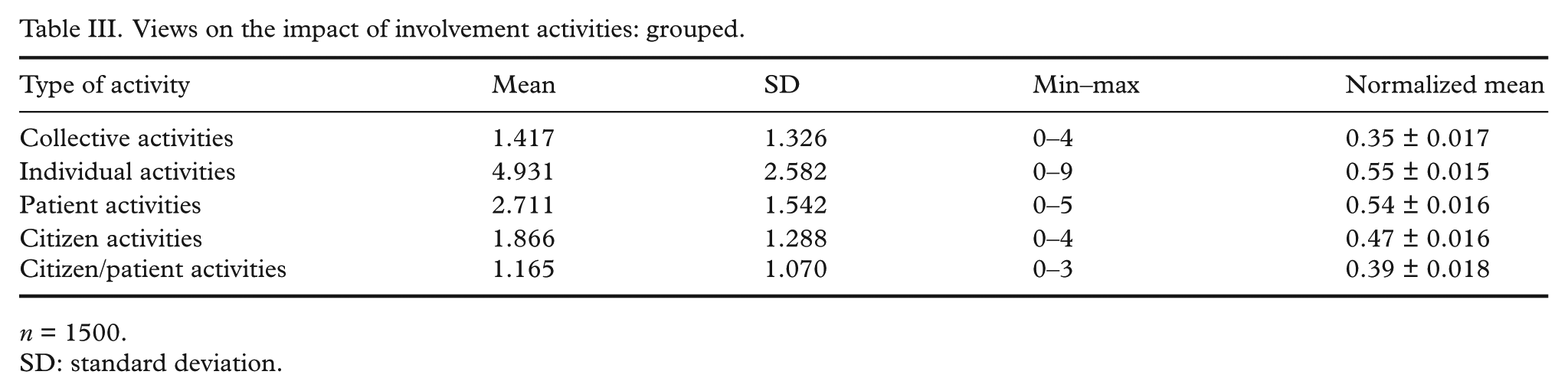
n = 1500.
SD: standard deviation.
Sociodemographic characteristics
In a model taking gender, education, age and health into account (Table IV), there was no significant effect of gender or long-term condition on beliefs in the impact of different types of activities (grouped by unit of participation and participation role). Those with a low level of education were, however, less likely to believe in the impact of involvement. The difference compared with respondents with an average or high level of education was most pronounced for collective PPI activities (−0.366*) and citizen activities (−0.264*). Furthermore, there was a small but significant effect of age on all activity types; beliefs in impact decreased with age.
Sociodemographic characteristics and views on the impact of involvement activities: grouped.
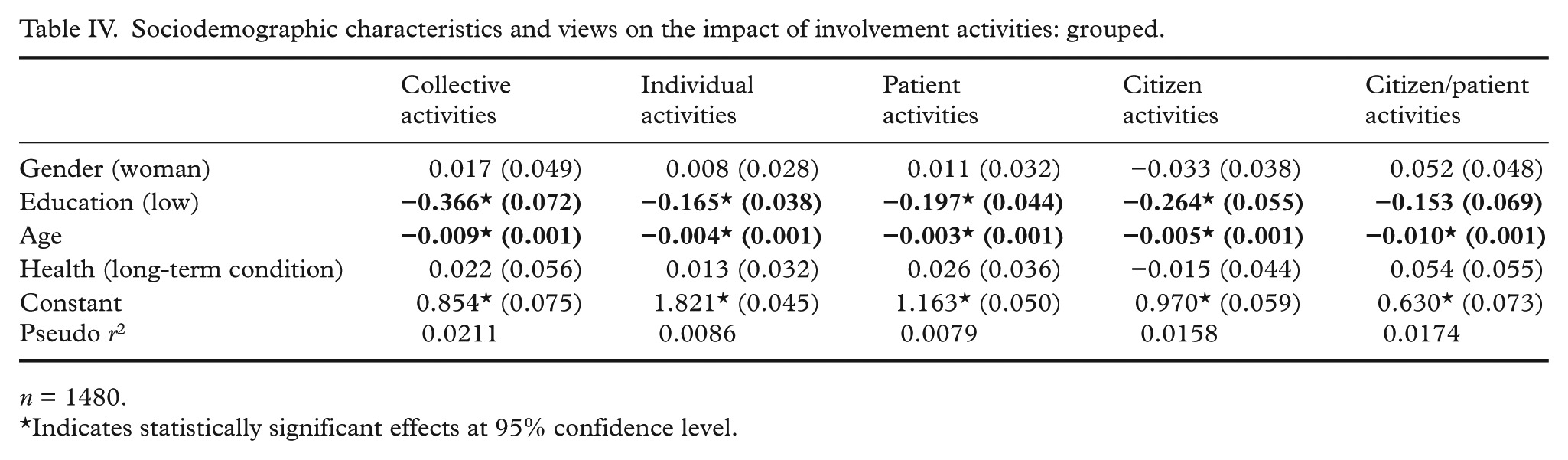
n = 1480.
Indicates statistically significant effects at 95% confidence level.
Discussion
We discuss three main results that have implications for public health: the general population’s greater belief in the impact of (a) individual versus collective participation, (b) patient versus public participation and (c) the association between belief in impact and educational attainment.
Voting in regional elections – an individual citizen activity establishing a representative assembly governing the region’s affairs – was the activity most respondents believed in. Overall, however, fewer believed in the impact of citizen activities compared to patient activities. A majority believed in the impact of involvement activities aimed at individual patients, for instance replying to a patient survey or changing healthcare provider (consumerist approaches [19]). Less than half believed that public activities such as contacting a local politician, joining a political party or taking part in a citizen council would improve health services. This suggests that people perceived that they are more likely to impact their own treatment and care than influence strategic decisions such as regional priorities. The respondents believed the least in participating in demonstrations (uninvited participation), despite evidence that protests are effective in forcing politicians to withdraw proposals to close emergency departments [20].
Encouraging patients to take more control when they are ill may be an effective tool for improving public health and particularly important to mitigate the negative health effects of chronic conditions [21]. The greater belief in individual patient activities in our study may be linked to the implementation of consumerist patient policies, or the evolution of a more individualized society where collectivity is de-emphasized and self-expression stressed [12]. Yet, international comparisons show that Sweden falls behind other high-income countries in information and involvement in decisions about care and treatment, particularly for patients with chronic conditions [22]. This may be associated with a policy focus on patient choice (the option to ‘exit’ service providers), rather than ‘voice’ activities. Defining patient choice as a form involvement is contested and distinct from active involvement in decision-making [23]. There is a risk that choice leads to fragmentation instead of continuity and undermines the patient–physician relationship and shared decision-making [8].
Notwithstanding the importance of having a mandate to make decisions concerning one’s own health, individual involvement does not promote membership in social networks [24], and may thus, to a lesser extent than collective activities, build the capacity for trust, reciprocity and cooperation [19] linked to health-supporting environments [25]. Society-centred explanations for the generation of social capital dominate the literature, pointing to the importance of civil society engagement and social relations [3]. For instance, research has recently noted that social media use under some conditions is linked to social capital and may facilitate community life, in particular social network sites that include opportunities for discussion [26]. However, institution-centered explanations suggest social capital is also generated by public policies and political institutions. This includes local government such as the Swedish regions, whose institutional design is decisive for the creation and mobilization of social capital [27]; not the least in-depth or longer-term involvement opportunities involving deliberation. As fewer respondents in our study believed in the impact of collective rather than individual and one-off activities, it may be productive for policymakers to reconsider the regions’ involvement approaches to benefit from this type of involvement as well. Perhaps, the introduction of Patient Participation Groups (PPGs), which are now a contractual requirement for all English primary care practices, might be a beneficial approach, although they have not been fully evaluated. PPGs may, for instance, advise practices on the patient perspective and communicate with the community, organize health promotion events and run support groups to meet local needs [28]. Depending on the composition of the groups, they may generate bonding, bridging and/or linking social capital [24].
Furthermore, belief in the impact of involvement decreased slightly with age and was lower among those with a low level of education. It is unclear how perceptions about impact interact with individual factors such as experience, cultural and political orientation [7], and how these affect actual participation. Evidence from Sweden suggests that both the young and those with a low level of education have relatively little experience of being involved in the political process [29]; the pattern likely being similar in healthcare. In fact, those not being involved are often those who have the most to gain, those with greater healthcare needs [7]. This applies particularly to people with a low level of education, who live six years shorter than those with a high level of education, feel less included in society and experience lower levels of control and influence [30]. Viewed as a ‘hard to reach’ group, involvement activities that are ad hoc or one off are not best suited for involving this group. Rather, ongoing involvement activities that build trust, relationships and meaningful communication should be encouraged [31].
Creating more equal health through involvement is not straightforward. Involvement activities intended to increase people’s influence may in fact exacerbate inequalities as these generally appeal to well-educated, resource-strong citizens [27]. Targeted recruitment may, therefore, be necessary [32] and regions have tried to give certain groups ‘advisory status’ by establishing citizen councils for the young, immigrants, elderly and those with disabilities [3]. The regions also collaborate with patient organizations; although without clear strategies and routines [33]. Even so, a great challenge in the regions is that involvement is limited. A survey in one Swedish region showed that 92% of the residents had not tried to influence a decision in the past year [34]. This is consistent with ‘participation and influence in society’ being given a low priority compared to other objective domains in Swedish public health policy [2]. There are no data on the frequency of influencing clinical decisions through activities such as those studied, and, therefore, we do not know whether greater belief in patient activities is mirrored in greater participation. Future research seeking to identify those who are actually involved is important as the interests of patients and patient groups may conflict with the interests of the wider public [10,13]. There are many examples of malfunctioning involvement, and some professionals and organizations are still threatened by the notion of active involvement [7]. This may affect how people are ‘responded to’ and lead to less involvement, which may be ameliorated by clear demonstrations of the positive impact of involvement.
We acknowledge some limitations in this study. We have only investigated ‘participation and influence in society’ in relation to health services and ‘known activities’. We may have missed some of ‘the action that publics take within their health systems’ [17, p.122]. As data about PPI are not collected by official national or European data sources, data were collected for the purpose of this study; this was done in collaboration with TNS Sifo. We only have a crude measurement of their perceptions of involvement impact and do not have information on whether respondents have been involved; neither do we have information on individual attitudes such as trust in the health service or beliefs about their capacity to be involved. Furthermore, our study did not include ethnicity or disability, which have been reported as barriers to involvement along with gender, culture, belief, sexuality, age and class [7,31]. This study should be regarded as an initial description of the perceived impact of involvement in healthcare and a basis for more nuanced studies of different groups’ participation. The relationship between beliefs about involvement and actual involvement patterns needs further investigation, not the least in relation to reported barriers to involvement. We suggest this requires accurate and systematic approaches to measuring both the intrinsic and extrinsic impact, while making a distinction between the perspectives of patients and the public.
Conclusions
PPI is one way of enhancing ‘participation and influence in society’, and thus improves individual and collective health by giving people opportunities to participate and influence health decisions. In this study there was a greater belief in the impact of individual activities and patient activities among the Swedish respondents. This points to a need to strengthen collective involvement to make people take part in strategic decisions and generate social capital underpinning community action to improve health. As those with a low level of education were less likely to believe in the impact of involvement despite generally having greater healthcare needs, it is crucial to develop PPI activities that members of this group find impactful and empowering.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Swedish Research Council (grant number 350-2012-6634).