
Abstract
Objectives: The aims of this article are to (1) determine whether and to what extent general perceived health and quality of supervision predict voluntary early retirement pension (VERP) and (2) assess whether quality of supervision modifies the association between general perceived health and VERP. Methods: Employees aged 49–64 years who participated in the Danish Work Environment Cohort Study in 2000 were selected. Their questionnaire data about health and work were linked to register data on social transfer payments, among others VERP, from 2001 to 2012 in the Danish Register for Evaluation of Marginalization (N=1167). Cox proportional hazards analyses were performed to identify the prospective association of general perceived health and quality of supervision on VERP. Relative excess risks due to interaction (RERIs) were calculated to assess whether quality of supervision modified the association between health and VERP. Results: Employees with poor health at baseline had an increased risk of VERP during follow-up (hazard ratio [HR]=1.23; 95% confidence interval [CI] 1.02–1.49). Quality of supervision at baseline was not associated to VERP during follow-up (HR=1.04; 95% CI 0.90–1.21). There was no statistically significant interaction of poor health and poor quality of supervision with regard to risk of VERP (RERI=−0.33; 95% CI −1.79 to 1.14).
Keywords
Introduction
The population in many European countries is ageing rapidly. Consequently, the ratio of retired elderly to the active working population is increasing, causing pressure on social-security systems. 1 One strategy to counteract this development is to increase the number of people that keep working until the official retirement age. Many European governments have responded to the ageing of the population by increasing the statutory retirement age and discouraging early exit from the workforce. 2 For example, in 2011, the Danish government decided to raise the statutory retirement age at which individuals receive their state old-age pension by gradually increasing it from 65 to 67 years over the period 2019–2022. 3 However, although less generous than before, Danes with unemployment insurance still have the opportunity of a voluntary early retirement pension (VERP; called ‘efterløn’ in Danish). VERP is available from the age of 60 years for individuals born before 1954, whereas for individuals born 1954 and later, the age of eligibility is being gradually raised. 4 Officially, VERP is not health based, but it might be used as an informal way of health-based retirement for older workers with health problems who do not meet the eligibility criteria of the official health-based way of retiring in Denmark, that is, work disability pension (‘førtidspension’ in Danish).
Previous research has shown that poor health is a major reason for early exit from the labour market, in particular due to disability pension. As opposed to disability pension, early retirement is considered to be a more voluntary way to exit the labour market early, which is not conditionally linked to health. However, a review by Van den Berg et al. showed that poor health also predicted non-disability retirement. 5 Furthermore, a recent review by van Rijn et al. showed that perceived poor health is a risk factor for disability pension and unemployment and, to a lesser extent, early retirement. 6
There is considerable interest in factors that could buffer the relation between poor health and early retirement because health-related problems at work are not always easy to solve. Quality of supervision may be an important factor in this respect. Focus-group interviews by Van den Berg et al. indicated that according to employees, supervisors are well-equipped to support workers to prolong their working life because they know about the specific situation of the employees. 5 In addition, supervisors may have the power to adjust the working environment to facilitate prolonged employment. If immediate supervisors could buffer the relation between poor health and early retirement, this would offer possibilities to select and hire supervisors with certain characteristics, or to train them to acquire these characteristics. However, relatively little is known about the potential of supervisors to buffer the impact of poor health on early retirement. To the best of our knowledge, only one study of 365 workers by Lund and Villadsen quantitatively investigated the direct effect of quality of the immediate supervisor on voluntary early retirement, and this study found no significant association. 7 Another study showed that lack of help and support from a supervisor was associated with impaired work ability among breast-cancer survivors, 8 and work ability has been found to be a predictor of early retirement in other studies.9,10 De Lange et al. also pointed to the importance of the supervisor within the group of older workers. 11 They suggested that poor social support from supervisors was associated with emotional exhaustion in older workers (>50 years), whereas this was not the case in younger workers (<35 years) and middle-aged workers (35–50 years). 11 Emotional exhaustion might be a risk factor for early retirement, as previous research has shown that psychological health problems predict early retirement. 12 Altogether, these studies provide ample indications that there may be an important role for supervisors to help prolong their subordinates’ working careers, especially in the case of poor health.
This study aimed to determine whether and to what extent general perceived health and quality of supervision predict VERP in a representative sample of the Danish workforce. It was hypothesised that poor general perceived health and poor quality of supervision both predict an increased risk of VERP during follow-up. A further aim of the study was to investigate whether a possible association of poor health with risk of VERP is modified by quality of supervision. It was hypothesised that high-quality supervision buffers the association of poor health and risk of VERP.
Method
Study design and population
This was a prospective cohort study, which was based on the linkage of questionnaire data from the Danish Work Environment Cohort Study (DWECS) with register data on VERP from the Danish Register for Evaluation of Marginalization (DREAM). DWECS is a representative cohort of the Danish working population established in 1990, with follow-up surveys every five years. In 2000, 8577 Danish residents (75% response rate) completed a DWECS questionnaire on demographic characteristics, health, health behaviour and work environment. Using the participants’ unique personal identification number, we followed up the cohort in the DREAM register from 1 January 2001 to 1 December 2012. DREAM provides information on social transfer payments. A detailed description of the design and study population of the 2000 round of DWECS has been published by Burr et al., 13 while a detailed description of the research perspectives of linking DWECS to DREAM for research purposes has also been published. 14
Individuals were included in the analyses if they were employees, between 49 and 64 years of age and had unemployment insurance at baseline. We chose age 49 as the lower age limit in order to include all individuals who would turn 60 years at some point during follow-up and who therefore became ‘at risk’ for VERP. We chose age 64 as the upper age limit because these people still had one year left of being ‘at risk’ for VERP. Having unemployment insurance was required because such insurance is needed for accessing VERP. Individuals with missing information on one of the relevant variables were excluded from the study. Figure 1 shows in detail the application of the inclusion and exclusion criteria, resulting in the final study population of 1167 people included in the analyses.
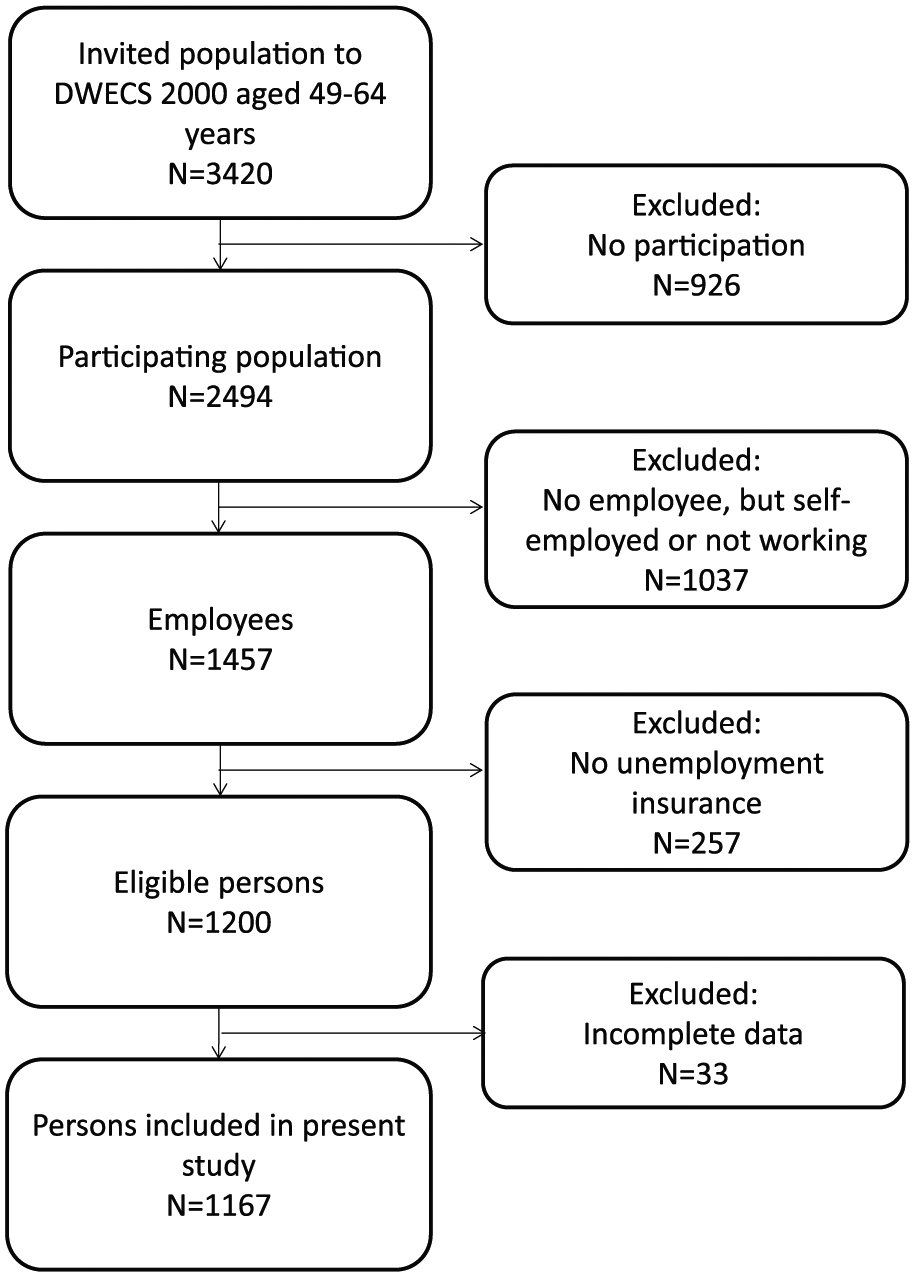
Flow of the study population resulting in 1167 persons included in the present study.
VERP
The outcome of the study was time to onset of VERP, measured by week until the first payment of VERP in DREAM (code 621) between 1 January 2001 and 1 December 2012.
Health
General self-rated health was measured with one item, derived and modified from the Short-Form 36 questionnaire 15 : ‘How do you rate your health in general?’, with the response categories ‘very good’, ‘good’, ‘fairly good’, ‘poor’ and ‘very poor’. The responses ‘very good’ and ‘good’ were classified into ‘good health’, and the responses ‘fairly good’, ‘poor’, and ‘very poor’ were classified into ‘poor health’. 15
Quality of supervision
Quality of supervision (as perceived by employees) was measured using the ‘quality of leadership’ scale, consisting of four questions derived from the Copenhagen Psychosocial Questionnaire (COPSOQ; Cronbach’s α=0.84)16,17: ‘To what extent would you say that your immediate supervisor (i) makes sure that the individual member of staff has good development opportunities; (ii) gives high priority to job satisfaction; (iii) is good at work planning; and (iv) is good at solving conflicts?’. The questions were answered on a five-point scale, with the response categories ‘to a very large extent’, ‘to a large extent’, ‘somewhat’, ‘to a small extent’ and ‘to a very small extent’. The quality of supervision scale has previously been used as a continuous scale in relation to early retirement. 7 For the purpose of calculating interaction terms, we dichotomised the quality of supervision score into ‘high quality’ versus ‘low quality’ by median split. To test whether this cut-off point yielded enough contrast between poor and good managers, we performed sensitivity analyses in which we used alternative cut-off values.
Covariates
As covariates, we included age, sex, socioeconomic status and physical work demands. Age and sex were derived from the Central Population Register. Socioeconomic status was based on self-reported occupation in DWECS, which was classified according to the European socioeconomic classification 18 consisting of six categories: (1) higher professionals and managers; (2) lower professionals and managers; (3) higher clerical, services and sales workers; (4) lower clerical, services, technical and farm workers; (5) skilled workers; and (6) semi- and unskilled workers. Physical work demands were measured using three questions on sitting, squatting and pushing/pulling, and one subscale on lifting. In line with previous research, a scale was constructed as the mean of these three questions and the subscale (Cronbach’s α=0.62). An example question is: ‘Does your job require that you kneel or squat?’ The questions were answered on a six-point scale, with the response categories ‘almost all the time’, ‘approximately three-quarters of the time’, ‘approximately half of the time’, ‘approximately a quarter of the time’, ‘rarely/very little’ and ‘never’.
Analyses
Using Cox proportional hazards analysis, we calculated hazard ratios (HR) and 95% confidence intervals (CI) for the prospective association of poor health and low quality of supervision with onset of VERP. We first calculated crude HRs for health and for quality of supervision. In the next step, the association between health and VERP was adjusted for quality of supervision. In addition, the association between quality of supervision and VERP was adjusted for health. Finally, we added the covariates age, sex, socioeconomic status and physical work demands to the model. Risk time began on the participants’ 60th birthday. Participants were censored at the time they reached the statutory retirement age of 65 years, died, emigrated, started receiving a disability pension or an unemployment compensation or until the end of the follow-up period (1 December 2012), whichever came first.
To investigate whether quality of supervision modified the association between general perceived health and VERP, we performed interaction analyses. Interaction may be defined as departure from either additivity or multiplicativity. We chose to analyse departure from additivity because this is relevant from a public-health perspective. 19 Interaction effects were analysed by calculating relative excess risk due to interaction (RERI) and their 95% CI using the Delta method.20,21 RERI for the combination of poor health and poor quality of supervision was calculated, with HR as estimates of relative risks (RR) using the following formula:
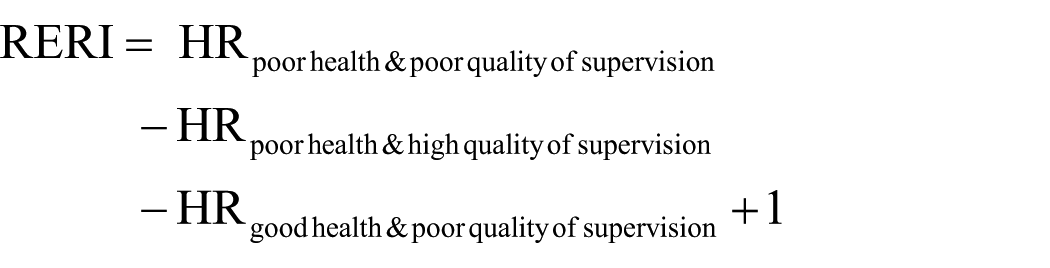
If RERI is not equal to zero, then an additive interaction is present. A negative RERI indicates a negative interaction (less than additivity). A positive RERI indicates a positive interaction (more than additivity). The interaction analyses were adjusted for the covariates sex, age, socioeconomic status and physical work demands.
Results
Table I shows the characteristics of the study population. The median age was 54 years, and 53% of the participants were female. The socioeconomic status group with the strongest representation was ‘higher clerical services and sales workers’ (22%), followed by ‘semi- and unskilled workers’ (20%). Poor self-rated health was reported by 17% of the participants. During the follow-up period, 746 (63.9%) employees went on VERP, and 421 (36.1%) employees were censored due to one of the defined criteria for censoring. Mean time to onset of VERP was 137 weeks (range 2–261 weeks). The mean age at which people went on VERP was 62.6 years.
Characteristics of study population (N=1167).
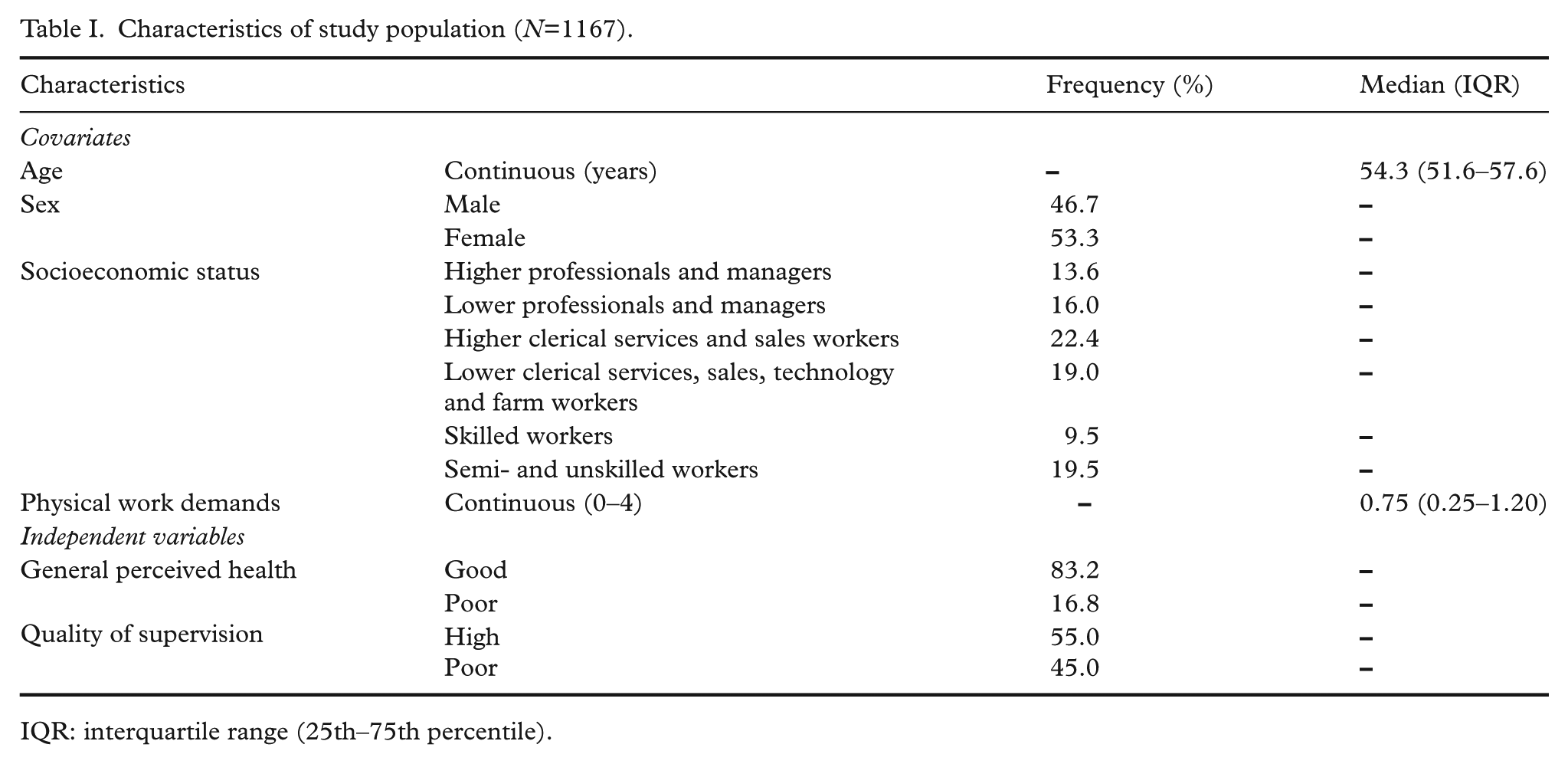
IQR: interquartile range (25th–75th percentile).
Main effects of health and quality of supervision
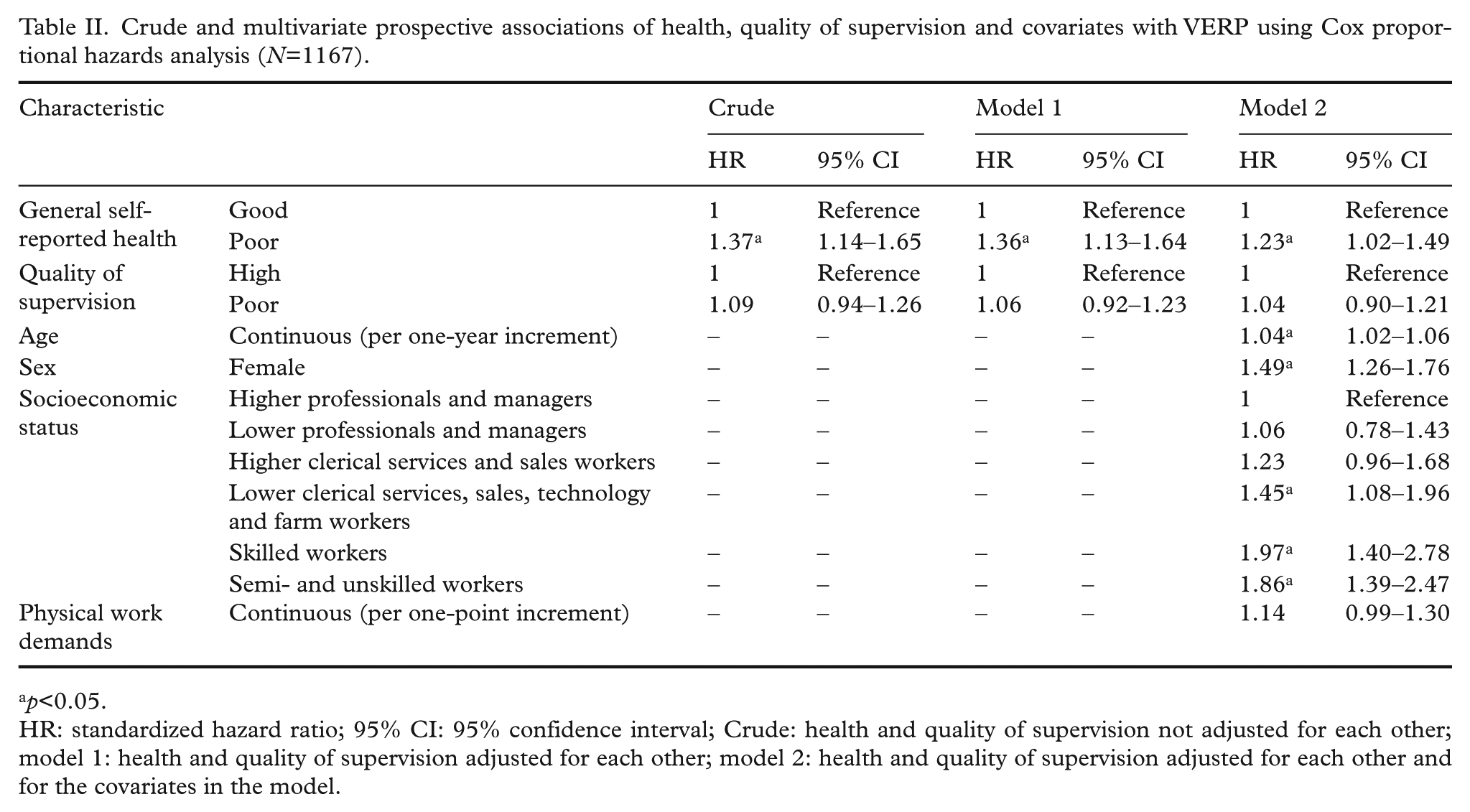
Table II shows the association of health, quality of supervision and the covariates with time to VERP. Poor health predicted VERP in the crude analysis (HR=1.37; 95% CI 1.14–1.65). The association was slightly attenuated but remained statistically significant in the fully adjusted model (HR=1.23; 95% CI 1.02–1.49). Low quality of supervision was not associated with VERP in any model.
Crude and multivariate prospective associations of health, quality of supervision and covariates with VERP using Cox proportional hazards analysis (N=1167).
p<0.05.
HR: standardized hazard ratio; 95% CI: 95% confidence interval; Crude: health and quality of supervision not adjusted for each other; model 1: health and quality of supervision adjusted for each other; model 2: health and quality of supervision adjusted for each other and for the covariates in the model.
Of the covariates, older age, female sex and lower socioeconomic status predicted VERP. Socioeconomic status showed a strongly graded association with VERP, with increasing HRs in the lower socioeconomic status groups.
Using alternative cut-off values to dichotomise between poor and good quality of supervision revealed that when the lowest quintile was contrasted with the other four quintiles, there was a tendency towards an association between low quality of supervision and early retirement (HR=1.17, p=0.10).
Interaction between health and quality of supervision
Table III shows the analyses for the interaction of poor health and low quality of supervision on risk of VERP, adjusted for age, sex, socioeconomic status and physical work demands. There was no indication that dual exposure to poor health and poor quality of supervision synergistically increased the risk of VERP. The HR in the poor health and poor quality of supervision group was 1.18 and was far from statistically significant (95% CI 0.68–2.08). The HR in the group of poor health and high quality of supervision was 1.42 and also not statistically significant (95% CI 0.48–2.40). This equates to a 17% lower risk of VERP among workers with poor health and poor quality of supervision than among workers with poor health and good quality of supervision. However, RERI was –0.33, and this was not statistically significant (95% CI –1.79 to 1.14).
Interaction of health with quality of supervision on risk of VERP (N=1167).
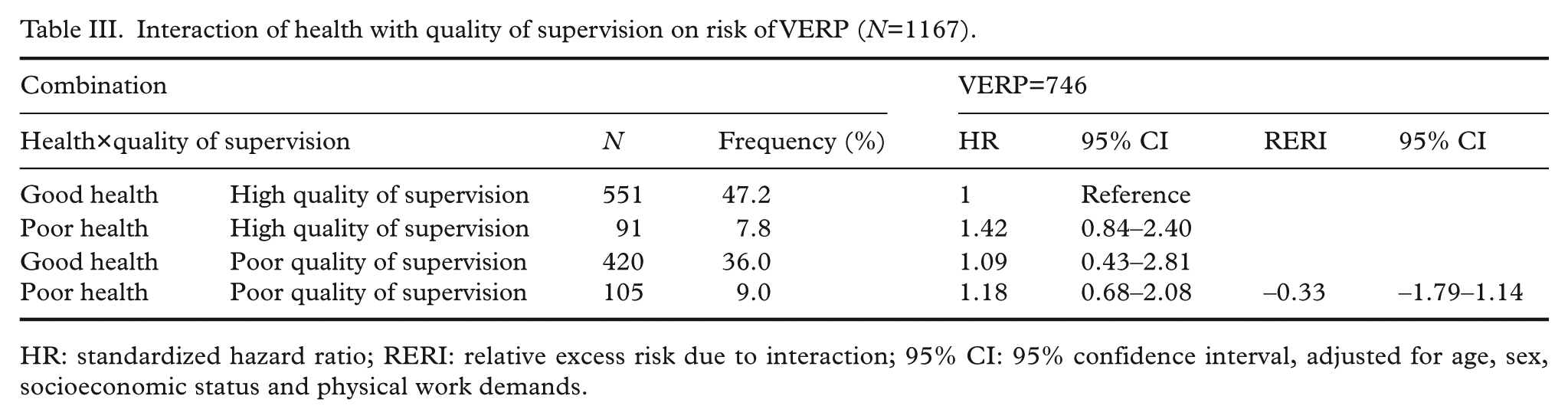
HR: standardized hazard ratio; RERI: relative excess risk due to interaction; 95% CI: 95% confidence interval, adjusted for age, sex, socioeconomic status and physical work demands.
Discussion
This study aimed to examine whether and to what extent general perceived health and quality of supervision predict VERP and to assess whether quality of supervision buffers the association between general perceived health and VERP. Poor health increased the risk of VERP, whereas poor quality of supervision did not. There was no interaction of poor health and poor quality of supervision with regard to risk of VERP.
Our finding that poor health modestly decreased the time to onset of VERP is in line with previous reviews showing that self-reported poor health predicts early retirement.5,6 As opposed to what we expected, quality of supervision was not associated with early retirement during follow-up. Although this is in line with a study by Lund and Villadsen, 7 which found no significant association between the quality of the immediate supervisor and early retirement, other studies pointed to the importance of supervisors with regard to the prolongation of working lives of their employees. 5 We expected the supervisors to be of influence because they can be assumed to have good insight into the specific situation of employees, and they have the power to adjust the working environment when necessary. Quality of supervision may also involve trust, which has been shown to be a determinant of retirement intentions. To illustrate, a study by Muurinen et al. showed that employees who trusted their supervisor were less likely to have strong retirement intentions compared with those who did not trust their supervisor. 22 Furthermore, we expected that high quality of supervision would buffer the association of poor health and early retirement, but we did not find such an interaction. Instead, we found that the association of poor health and early retirement was stronger when quality of supervision was high, although this association was not statistically significant. It might be that employees suffering from poor health with a good relationship with their supervisor coordinate their early exit in close collaboration with their supervisor, eventually resulting in a decreased time to onset of VERP. The supervisor may even take the initiative to help employees with health problems to retire early. Such a coordinated early exit is less likely in case of a less good relationship between the employee and the supervisor. Previous qualitative research by De Wind et al. indeed showed that poor health may more often result in early retirement when employee and employer agree that early retirement is the best solution. 23
Post-hoc analyses showed that quality of supervision tended to predict VERP when the lowest quintile was compared to all other quintiles combined. This may indicate insufficient contrast between poor and good quality of supervision in the main analysis. However, another explanation might be that it is not the quality of supervision that buffers the association between poor health and VERP, but rather the power of the supervisor to effectuate necessary adjustments in the working environment. A qualitative study by Leijten et al. 24 suggested that poor health could cause an imbalance in demands and resources, and pointed to the importance of workplace adjustments in the case of poor health to maintain high productivity at work. Our scale on quality of supervision did not cover these aspects, and may therefore be less suitable to investigate whether quality of supervision could buffer the effect of poor health on early retirement. Future research is needed to investigate which specific characteristics of supervision could play a role in the prolongation of working lives or whether there are other aspects regarding the management that have potential to contribute to longer working lives. Examples could be the quality of interaction between supervisor and employee, supervisor support or opportunities of supervisors to effectuate necessary workplace adjustments.
A strength of the present study is the linkage of questionnaire data from the DWECS with national register data of the DREAM. Questionnaire data for 100% of the participants could successfully be linked to the register data, which provides weekly information about whether a person receives early retirement pension. An advantage of register data of social transfer payments over self-reported employment status is that the former is not affected by recall bias. Another strength is the follow-up period of almost 12 years.
However, this study also has several limitations. First, self-reported health and quality of supervision were both assessed by questionnaires. Individuals in poor health might have had more intense communication with their manager than individuals in good health, and therefore may have experienced more support from their manager. This was also suggested in a previous study by De Wind et al., 10 showing that individuals who reported higher social support of colleagues and supervisor were more likely to retire early. On the other hand, individuals with poor health may experience less support than they think they would need, which may result in a more negative assessment of the quality of their supervisor.
A second limitation is that the time between assessment of the determinants, that is, general perceived health and quality of supervision, and the start of the period of becoming ‘at risk’ for early retirement differed largely between workers in the present study. Workers who were between 60 and 64 years of age at baseline were immediately ‘at risk’ at the start of the study, whereas for example workers aged 49 years at baseline became ‘at risk’ only after 11 years. It is likely that during these 11 years, many changes had happened at work, including job changes of the employees and changes in supervisors. Future research should investigate whether the strength of the association between different predictors and VERP depends on the period of time between assessment of these variables.
At the time of this study, VERP was accessible to those employees who had unemployment insurance, which was the case for the majority of the Danish population. 25 As in many other European countries, several pension-system reforms that promote prolonged working have been implemented in Denmark. 2 In 2011, the Danish government decided to raise the statutory retirement age at which individuals receive their state old-age pension by gradually increasing it from 65 to 67 years over the period 2019–2022. 3 Second, the number of years of VERP will decrease from five to three years.26,27 A previous Dutch study by Lindeboom and Kerkhofs showed that the eligibility for an early-retirement scheme substantially reduced the probability of early exit through work disability pension, which suggests that in the older age groups, early retirement might be a substitute of disability pension. 28 Nowadays, older workers, including those with health problems, are encouraged to prolong their working lives. Reasoning along this line, it might be that in a context of less opportunities to retire early, older workers may start to leave the workforce via other exit pathways, that is, those with health problems via disability pension, or if they do not qualify for disability pension, via unemployment or becoming dependent on social welfare. Some older workers may also continue working, despite health problems. In a context of a strong external driver to prolong working lives, it is important to search for ways that may contribute to well-being at work, especially among those with health problems.
In conclusion, our results indicate that general perceived poor health is associated with a greater risk of VERP, whereas quality of supervision is not associated with VERP. Furthermore, the present study did not support the notion that quality of supervision buffers the association between poor health and VERP. Future research is needed to determine whether other aspects related to quality of leadership, for example the quality of interaction between supervisor and employee, supervisor support or the supervisors’ opportunities to effectuate workplace adjustments, may modify the association between health and VERP.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a travel grant of the EMGO+ Institute for Health and Care Research (grant number 2014.016). The funding source had no role in the study design, data collection, analysis, interpretation of data, or the decision to submit the paper for publication.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.