
Abstract
Aims: The aim of this study was to explore the relationships between measured body size (body mass index (BMI)), perceived body size, weight change wishes and self-perceived health in young adults. Methods: The participants were recruited from a school-based population study in Norway, the Tromsø Study: Fit Futures 2, carried out in 2012–2013. A total of 629 young women and men (aged 18–23 years) reported on the main variables. The data were collected through weight and height measurements and questionnaires. The analyses were performed with descriptive statistics, the χ2 test and Student’s t-test. Results: A total of 20% of the women and 28% of the men were overweight or obese. There were considerable discrepancies between the measured BMI and perceived body size in both sexes. A substantial number of participants wanted to change their weight. Among the 174 women who reported that they were trying to lose weight, as many as 57 (32.8%) had a low normal weight (BMI 18.5–21.9 kg/m2). Correspondingly, among the 66 men who reported that they wanted to gain weight, as many as 19 (28.8%) had a high normal weight (BMI 22–24.9 kg/m2). We found no relation between body size perceptions, weight change wishes and self-perceived health.
Introduction
The increasing prevalence of overweight and obesity worldwide and the related health issues [1] have created a growing focus on weight reduction strategies. However, weight reduction has proved to be difficult to achieve at both the individual and population levels [2]. Lifestyle habits and energy balance have dominated the research field, both as explanatory factors and targets for intervention [3]. In recent years, sociocultural influences and perceptions of body size have emerged as important research topics in relation to weight issues [4,5]. The focus on body size and appearance in the media has a great impact on individuals and groups, not least young people [6]. With the growing focus on body size and appearance, discrepancies between actual body size measured as body mass index (BMI) and peoples’ own perceptions of their body size have also become a matter of interest [5].
Research findings regarding perceived body size and perceived health are both scattered and divergent. It has been suggested that an underestimation of body size in overweight young people can protect against depression [7], whereas an overestimation of body size in young people of normal weight can lead to health-compromising weight loss strategies [8].
The widespread wish to change weight status and expressions of dissatisfaction regarding bodily appearance [9] are important aspects in relation to health and well-being [10]. Negative feelings concerning body size are reported to be a risk factor for eating disorders and an inhibiting factor in lifestyle changes [11]. However, the effects of a discordance between actual and perceived body size on weight satisfaction and other health issues are unclear and further research is required [7].
This study aimed to extend existing knowledge about the relationships between BMI, perceived body size, weight change wishes, desired weight and self-perceived health in young adults from a school-based population survey. Special attention was given to sex differences because these have proved to be substantial regarding weight perceptions, weight change wishes and attempts to change weight [4,12].
Materials and methods
Study population, recruitment and design
Students in upper secondary school from two municipalities in northern Norway (Tromsø and Balsfjord) were invited to participate in the population-based Tromsø Study youth survey, Fit Futures, which has been described in detail elsewhere [13,14].
The survey was performed in two waves. This study is based on data from the second wave of the survey, Fit Futures 2, which was carried out in 2012–2013 when the participants were in the last year of upper secondary school and mostly aged 18–19 years. The total number of students invited to participant in the study was 1130, of whom 870 attended, giving an attendance rate of 77%. As our purpose was to study the young adult/late adolescence population, participants aged 23 years or older were excluded, in addition to those who did not report the data relevant for the current study. Thus the study included 629 eligible young adults. All examinations were performed by experienced study nurses in a clinical research unit at the University Hospital of North Norway, Tromsø. All the participants signed a written consent form before any procedures were performed. The studies were approved by the Regional Committee for Medical and Health Research Ethics North Norway (reference numbers 2009/1282 and 2011/1702).
Measurements
Height and weight were measured in all participants using a Jenix DS 102 stadiometer (Dong Sahn Jenix, Seoul, Korea) while they were wearing light clothes and no shoes. The BMI was calculated as weight (kg) divided by height squared (m2) and was categorized into weight classes in accordance with the World Health Organization definition [15]. All other data were self-reported and were collected through an electronic questionnaire at the same time as the other measurements were made.
Perceived body size was determined from the Figure Rating Scale adapted from Stunkard et al. [16] (Figure 1). The participants were asked to rate how they perceived their own body size by choosing between nine figures of gradually increasing size using the question, ‘Which of these figures looks most like your current body shape?’ To determine the discrepancies between the participants’ measured BMI (grouped in steps of one bmi unit) and their own perceptions of body size, we calculated the median bmi group for each of the chosen figure groups. The median was used as a result of the non-normal distribution of bmi in the sample. To compare actual and perceived body sizes, we included two bmi units in each direction from the median group to constitute the area beyond the range of measured BMI. Hence participants with a perceived BMI outside this range had perceptions of their body size that were considered discordant with their measured BMI. Accordingly, if their measured BMI was below this range, their reported body size was considered to be larger than the measured BMI. If their BMI was above this range, their reported body size was considered to be smaller than the measured BMI.
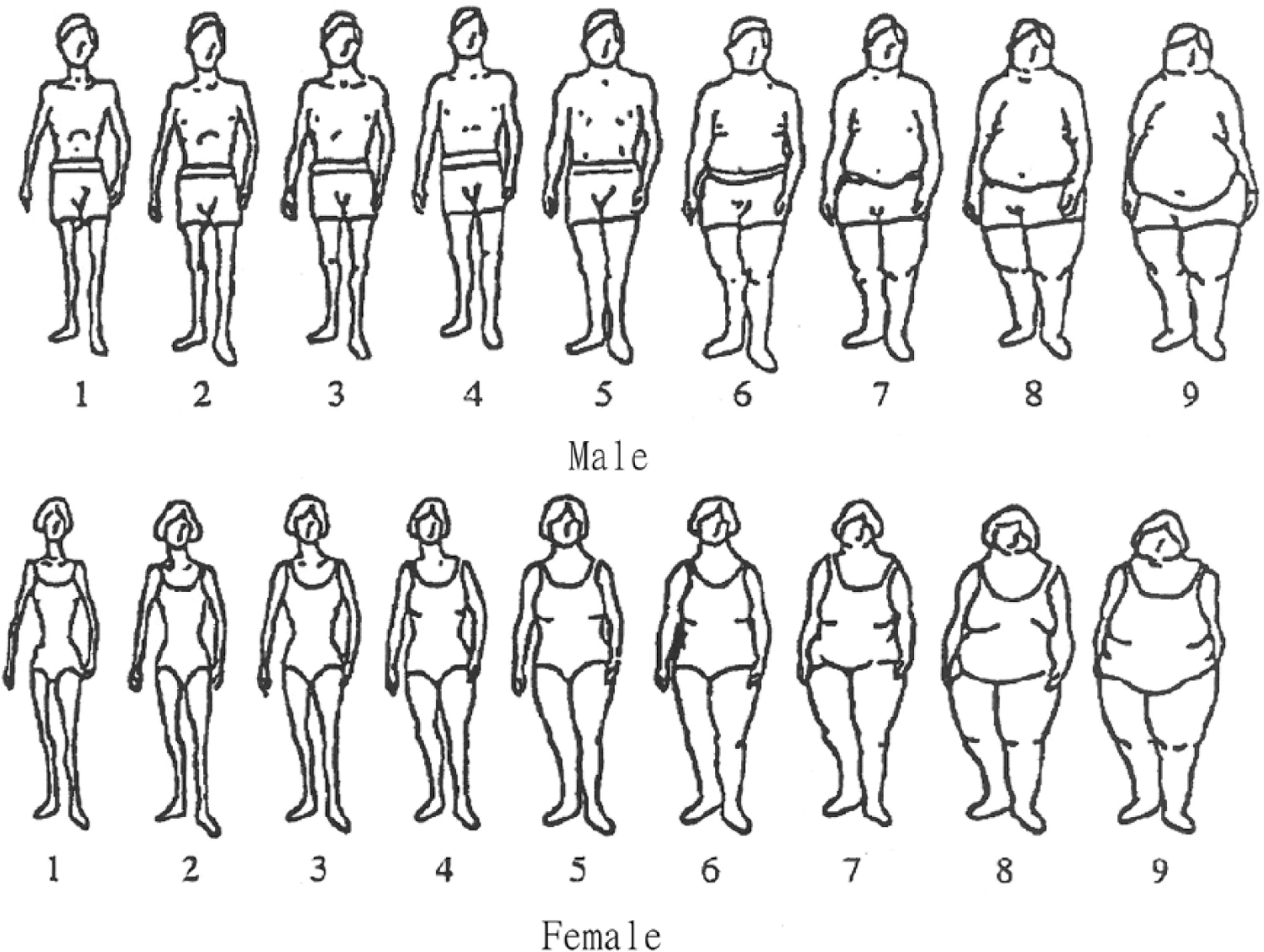
Images of perceived body shape from the Figure Rating Scale (adapted from Stunkard et al. [16]).
Weight change wishes were determined by the question, ‘At present, are you trying to change your body weight?’, followed by the response options ‘no’ or ‘yes, I am trying to put on weight’ or ‘yes, I am trying to lose weight’. The desired weight for those who were trying to change their weight was determined by the question: ‘Which body weight would you be satisfied with (in kg)?’
Self-perceived health was determined by the question, ‘How do you in general consider your own health to be?’ Answers were given as five categories: very poor, poor, neither good nor poor, good or excellent. In the analyses, we dichotomized the categories into ‘very poor/poor’ and ‘neither good nor poor/good/excellent’.
Statistical analyses
All analyses were sex-stratified. Numbers and percentages were calculated for the categorical variables, whereas the mean and standard deviation (SD) values were calculated for continuous variables. Differences between groups and sexes were evaluated with the χ2 test for categorical variables and Student’s t-test for continuous variables. All analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS version 23). p<0.05 was considered significant.
Results
The study population consisted of 364 young women and 265 young men. Their basic characteristics are given in Table I. The mean±SD age was 18.2±0.63 years for women and 18.3±0.57 years for men; none was younger than 17 or older than 22 years. There was no significant difference in the mean±SD BMI between the sexes: 23.0±4.17 kg/m2 in women and 23.4±4.12 kg/m2 in men. However, the BMI distribution showed marked sex differences (p=0.005). In women, 20.3% were classified as overweight or obese, whereas the corresponding percentage in men was 28.3%. There were also substantial sex differences regarding weight change wishes. In the women, 3.8% reported that they were trying to put on weight and 47.8% were trying to lose weight. The corresponding figures in men were 25.0 and 26.1%, respectively (p<0.001). There was no significant sex differences regarding self-perceived health.
Characteristics of the study participants in the Tromsø Study, Fit Futures 2.
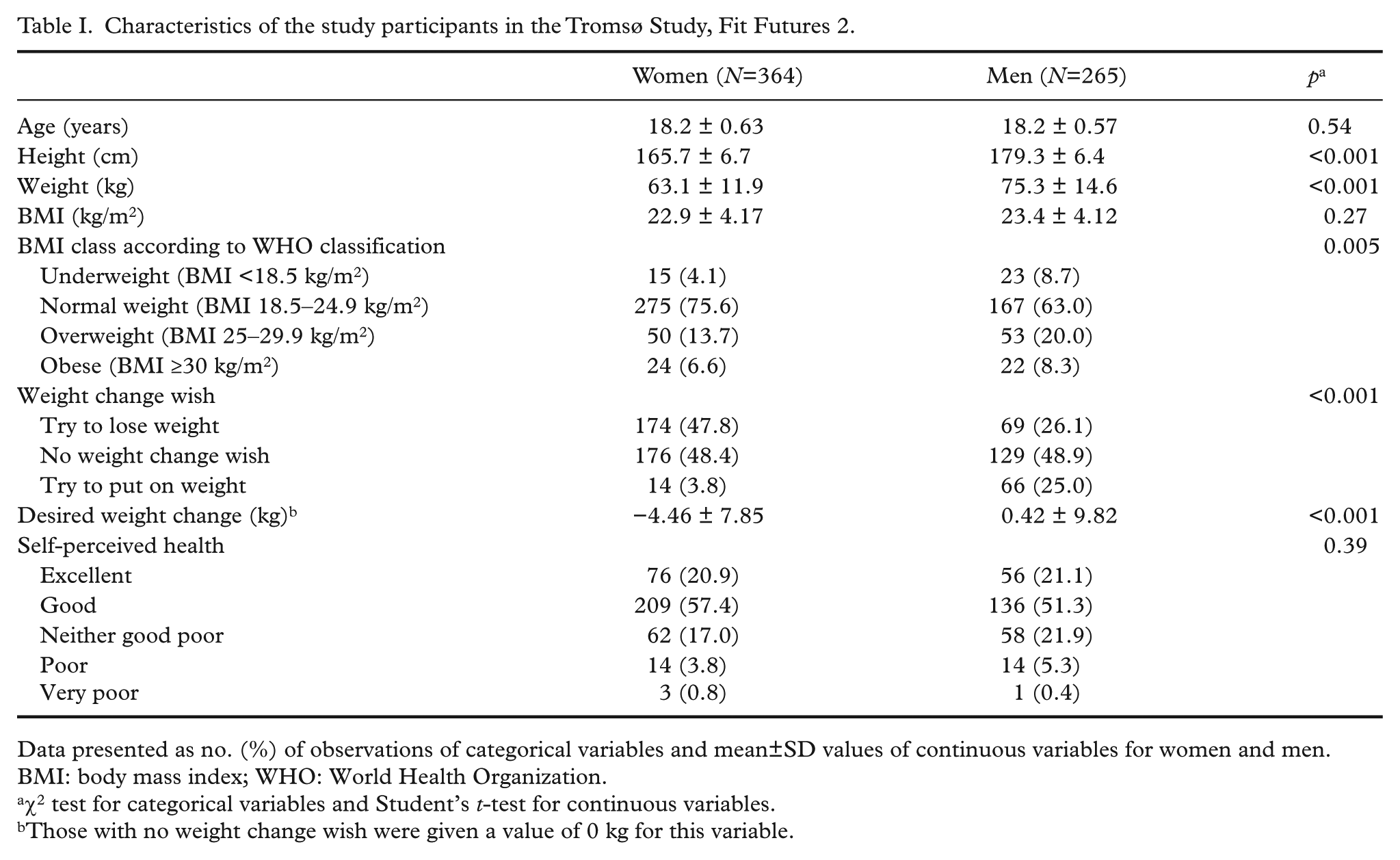
Data presented as no. (%) of observations of categorical variables and mean±SD values of continuous variables for women and men.
BMI: body mass index; WHO: World Health Organization.
χ2 test for categorical variables and Student’s t-test for continuous variables.
Those with no weight change wish were given a value of 0 kg for this variable.
Perceived body size
Relationships between measured BMI and perceived body size in women and men are shown in Supplementary Tables I and II, respectively (available online). None of the participants classified themselves as having the largest body size. There were only minor sex differences regarding the relation between actual BMI and body size. Thus, according to our definition, 79.8% of the women had a perception of their body size corresponding to their BMI; 9.3% perceived themselves as heavier than their measured BMI (‘false fat’) and 10.9% perceived themselves as lighter than the corresponding BMI (‘false thin’) (Supplementary Table I, available online). In men, the corresponding figures were 72.1, 13.6 and 14.3%, respectively (Supplementary Table II, available online).
In both sexes, the false thin participants had a higher BMI than those with a false fat classification, or those with a body size in correspondence with their BMI. In both sexes, the majority of the false thin group wanted to lose weight. Among the men, a substantial number of the false fat (30.6%) participants wanted to put on weight, whereas this desire was considerably less frequent among the false fat women (11.8%). There was no relationship between perceived body size discordant with measured BMI and self-perceived health (Table II).
Classifications of perceived body size as ‘false fat’, ‘concordant’ and ‘false thin’ in relation to age, BMI, weight change wish, desired weight change, self-perceived health and exercise level in the Tromsø Study, Fit Futures 2.
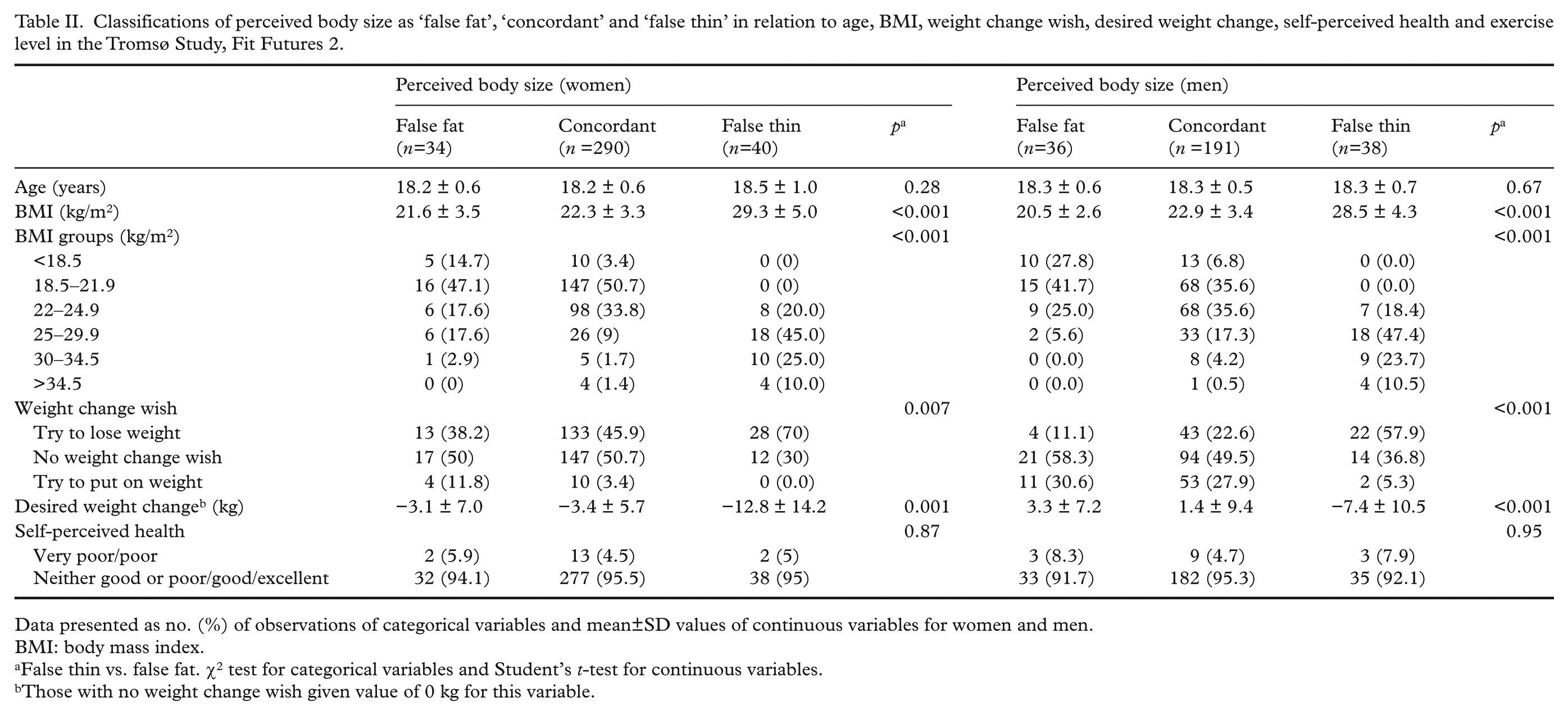
Data presented as no. (%) of observations of categorical variables and mean±SD values of continuous variables for women and men.
BMI: body mass index.
False thin vs. false fat. χ2 test for categorical variables and Student’s t-test for continuous variables.
Those with no weight change wish given value of 0 kg for this variable.
Weight change wishes
More than half of the sample (51.6% of the women and 51.1% of the men) reported that they wanted to change their weight. The general pattern was that those who wanted to lose weight were in the upper BMI groups, whereas those who wanted to put on weight were in the lower BMI groups (Table III). However, among the 174 women who reported that they were trying to lose weight, as many as 57 (32.8%) had a low normal weight (BMI 18.5–21.9 kg/m2). Correspondingly, among the 66 men with a high normal weight (BMI 22–24.9 kg/m2), as many as 19 (28.8%) reported that they wanted to gain weight.
Weight change wish in relation to age, body mass index and desired weight change in the Tromsø Study, Fit Futures 2.
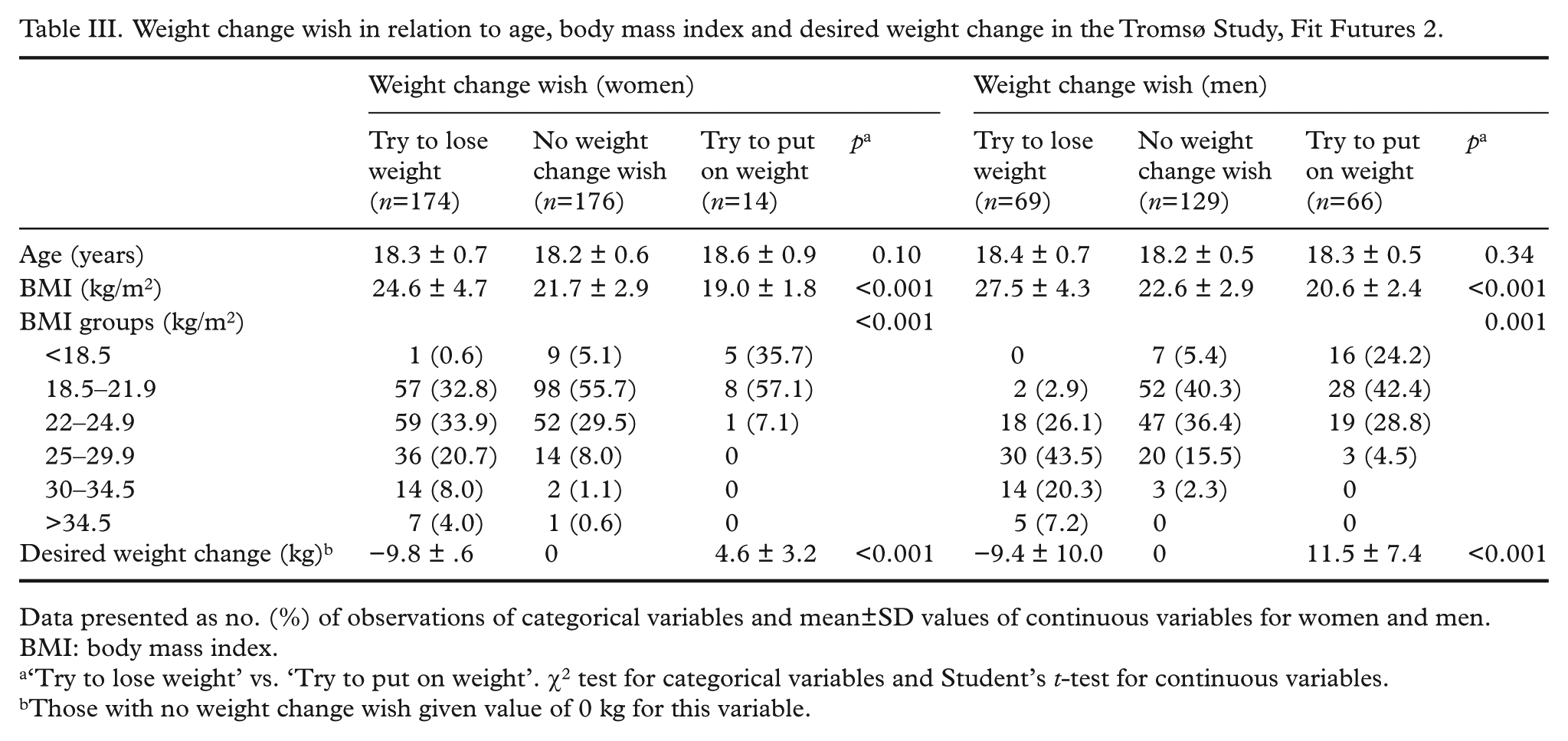
Data presented as no. (%) of observations of categorical variables and mean±SD values of continuous variables for women and men.
BMI: body mass index.
‘Try to lose weight’ vs. ‘Try to put on weight’. χ2 test for categorical variables and Student’s t-test for continuous variables.
Those with no weight change wish given value of 0 kg for this variable.
Self-perceived health
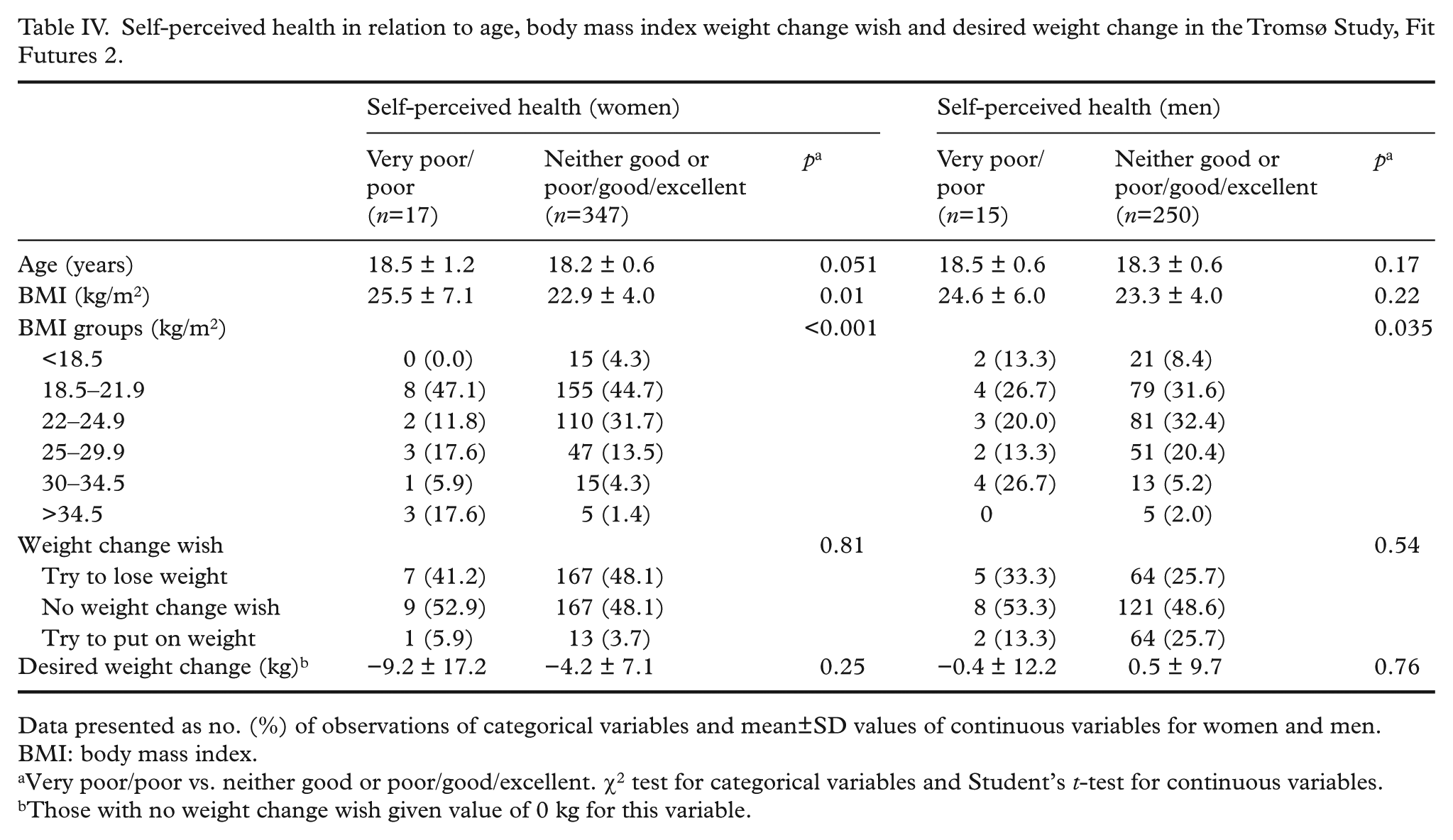
Few of the participants (4.7% of the women and 5.7% of the men) considered themselves to be in poor or very poor health (Table IV). Self-perceived health was related to BMI only in participants with BMI >30 kg/m2. In this group, a considerable number reported poor or very poor health (16.7% of the women and 18.2% of the men in this BMI group).
Self-perceived health in relation to age, body mass index weight change wish and desired weight change in the Tromsø Study, Fit Futures 2.
Data presented as no. (%) of observations of categorical variables and mean±SD values of continuous variables for women and men.
BMI: body mass index.
Very poor/poor vs. neither good or poor/good/excellent. χ2 test for categorical variables and Student’s t-test for continuous variables.
Those with no weight change wish given value of 0 kg for this variable.
Discussion
We have confirmed previous findings of high rates of obesity and overweight among young adults, with considerable discrepancies between measured BMI and perceived body size and remarkable differences in weight change wishes between women and men. However, no association was found between self-perceived health and misperception of body size or weight change wishes.
The mean BMI was 22.2 kg/m2 in women and 23.4 kg/m2 in men and the corresponding prevalence of overweight and obesity were 20.3 and 28.3%, similar to other national surveys [17]. In an international setting, this prevalence of overweight and obesity was lower than in the USA, UK and Australia [1,3], but similar to other European countries [18].
A considerable proportion of the participants, 20.2% of the women and 27.9% of the men, reported perceived body sizes that were discordant with their measured BMI. The number of participants with discrepancies between perceived body size and measured BMI depends on the definition used in the Figure Rating Scale of Stunkard et al. [16]. One option, as used by Bhuiyan et al. [19], is to standardize the actual BMI values and the perceived body sizes (Stunkard’s figures) to z-scores and subtract one from the other. However, as these scores (at least in our study) were not normally distributed, this approach would have been questionable. There is no ‘true’ BMI value for the nine figures used and attempts at assigning BMI values to the figures have given conflicting results [20]. We therefore chose the ‘true’ BMI for the figures to be the median BMI for those who selected a particular figure. To make sure that none (or only a few) were wrongly labelled as having a perceived body size in discordance with their BMI, we extended the ‘real’ BMI range by ±2 BMI units (Supplementary Tables I and II, available online). Even with this conservative definition, a considerable number of participants still reported body size perceptions that were discordant with their measured BMI. In both sexes there were an almost equal number of participants classified as false thin (chose thinner figures than their BMI would indicate) and false fat (chose fatter figures than their BMI would indicate). On average, the false fat participants had a low BMI (21 kg/m2), whereas the false thin had a high BMI (29 kg/m2). Thus most of these participants considered their weight to be more normal (or average) than it actually was.
The finding of an equal number of women classifying themselves as false thin and false fat is contradictory to findings in other studies, where more women than men typically perceive themselves as fatter than they actually are [4,21,22]. This discrepancy may reflect geographical and cultural differences in what is considered to be a normal or desirable body size. There are normative cultural and social rationales underlying human perceptions and behaviour and therefore the sociocultural context should be taken into account when questioning how and why people act as they do regarding weight issues [22]. There is also a need to understand the sociocultural determinants of food choices, physical activity and body perceptions when addressing weight issues [3].
More than half of the study sample reported that they had tried to change their weight. Not unexpectedly, the higher the BMI, the more of the participants wanted to lose weight, although some participants with a lower BMI (and in particular boys) wanted to gain weight.
Attempts to lose weight are more common in women than in men and these trends seem to be consistent across countries and regions [12]. It has been shown that men in general have higher levels of satisfaction regarding body size [4,12]. A focus on muscles is likely to be connected to the level of body size satisfaction in young men, whereas appearance and weight are more important for young women [23]. These aspects were, however, not part of our study.
It is a common finding that high proportions of women, and especially young adult women and adolescent girls, are dissatisfied with their weight [4,11,12]. This was also seen in our study, where 47.8% expressed a wish for weight loss, including a worrying number of participants with normal weight. The fact that more than half of the men wanted to change their weight was more surprising. However, our observation that men were more likely to wish for weight gain is consistent with previous research suggesting that underweight is undesirable for boys and men and may even predict depressive symptoms [9,24]. The sex difference regarding weight change wishes was highlighted by the average desired weight in those with weight change wishes, −4.46 kg in women and +0.42 kg in men.
In spite of the tendency for those who perceived their body size to be in discordance with the measured BMI to consider their weight as more normal, the majority of the false thin participants reported that they were trying to lose weight (both sexes) and, in men, 30% of the false fat participants reported that they were trying to gain weight. Accordingly, the discordance between their perceived and measured body sizes was not strong enough to alter their weight change wishes.
Self-perceived health is a commonly used single item for assessing individuals’ overall perception of their own health status, closely linked to the notion of general well-being [25]. In our study, about 5% of the men and women reported their self-perceived health to be very poor or poor, but these numbers were significantly higher (about 17%) in the obese participants.
The impact of overweight and obesity on psychological well-being and overall health is disputed [26]. Thus considerable attention has been paid to the positively correlated relationship between depression and obesity [11,12,27]. The association with depression has, however, been questioned by some researchers, who have pointed out the lack of alternative explanations for this besides obesity. There are some widespread myths about psychological maladjustment in people (especially children) who are overweight or obese, suggesting that not enough is known about the phenomena [26].
Our results indicated that, except for our obese participants, there was no relationship between self-perceived health and BMI. There was a lack of association between self-perceived health and discordance between perceived body size and actual BMI as well as with weight change wishes. This is contradictory to previous findings by Herman et al. [21] in a large population survey of Canadian adults, where weight status perceptions were strongly associated with self-rated health. One possible explanation for the lack of relation in our study could be that weight dissatisfaction is not important or damaging enough to influence the self-perceived health in younger age groups. Alternatively, this lack of association could indicate that weight change attempts are not driven by perceptions of poor health, but mainly by a wish for a more culturally defined appealing appearance. This may also reflect the suggestion that the possible consequences of obesity, such as an increased risk of diabetes and cardiovascular disease, are not perceived as relevant at such a young age.
This study, being cross-sectional and with a risk of potential selection bias, has several limitations. The use of a school-based survey with an attendance rate of 77% should minimize the risk, but we lack information about those who did not participate or report the relevant information. The original Figure Rating Scale [16] used to determine body size has been criticized as a result of the coarseness of the scale, the restricted range in options and inconsistent size differences between the figures [28,29]. It should also be noted that the nine figures do not show extremely thin or fat alternatives. Accordingly, with our definition of discordant classification, it would be impossible for very thin participants to classify their body as too fat. Also, in the almost 30 years that have passed since the figures were first presented, the average BMI has increased substantially. There are, however, several studies showing that the technique appears to be reliable and robust for distinguishing those who are overweight and obese from those with normal weight or as an adjunct to self-reported weight and height [28–30]. Unfortunately, we had no data on how muscularity was valued in relation to body size. This makes the results on weight change wishes, and especially wishes for weight gain in men, challenging to interpret.
We had the opportunity in this study to use simultaneously obtained accurate measures of height and weight and the Figure Rating Scale of Stunkard et al. [16]. As such, the study presents the figures as normative data and links them to current and precisely measured BMI in a population-based survey, which has been lacking in previous research [28]. Another advantage is the use of a school-based survey, high attendance rate and standardized anthropometric measures in a clinical setting.
Conclusions
Confusion and dissatisfaction regarding body size are widespread phenomena. This was confirmed in our study but, surprisingly, had little effect on self-perceived health. There is a need for more research on the perceptions of body size and weight change wishes and how these influence concerns about weight and health. In particular, more knowledge is needed about the causes and consequences of discrepancies between measured and perceived body size. In our opinion, these matters call for complementary research methods, including in-depth explorations and qualitative research approaches that are cognizant of the cultural factors that influence how people perceive their bodies and how they act upon these perceptions.
Footnotes
Acknowledgements
The authors thank the participants for attending and the staff at the Clinical Research Unit, University Hospital of North Norway for their excellent work in performing the survey. We are grateful to the Tromsø Study and the Fit Futures administration for giving us access to the data. We thank Professor TIA Sørensen at the University of Copenhagen, Denmark for kindly giving us permission to present Stunkard’s Figure Rating Scale in this paper.
Conflict of interest
None declared.
Funding
This study was supported by a grant from the Northern Norway Regional Health Authority (Grant number 8970/SFP1089-13).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.