
Abstract
Aims: The aim of this study was to investigate whether a workplace educational low back pain intervention had an effect on sick leave at the individual level and to identify possible predictors of the effect of intervention. Methods: Work units in two municipalities were cluster randomized to (a) educational meetings and peer support (45 units), (b) educational meetings, peer support and access to an outpatient clinic if needed (48 units) or (c) a control group (42 units). Both intervention groups attended educational meetings with information about back pain based on a non-injury model. A peer adviser was selected from among their colleagues. The outcome was days of sick leave at the individual level at 3, 6, 9 and 12 months, adjusting for previous sick leave at the unit level. As a result of similar effects on sick leave, the two intervention groups were merged (n=646) and compared with the control group (n=211). The predictors were different levels of belief in back pain myths, pain-related fear, helplessness/hopelessness and low back pain. Results: The intervention group had significantly less days of sick leave at the three month (4.9 days, p=0.001) and six month (4.4 days, p=0.016) follow ups compared with the control group. At three months, a low level of pain-related fear was the only predictor for the intervention effect (8.0 less days of sick leave, p<0.001).
Keywords
Introduction
Neck and low back pain (LBP) are the most common replace disorders with complaints related to long-term sick leave and disability in Norway [1] and LBP is globally related to more disability than any other disorder [2]. Despite much research, there is little evidence about the prevention of LBP [3]. It seems to be difficult to prevent LBP, but research has shown that it is possible to prevent the consequences of LBP, such as sick leave, fear of movement or injury, and inactivity [3]. Therefore it is important to prevent these negative consequences of LBP [3].
Brief interventions based on a non-injury model (NIM) with the aim of preventing the consequences of LBP have shown success in increasing the return to work (RTW) in clinical populations [4–6] and in reducing sick leave among employees [7,8]. The NIM was proposed by Indahl et al. [4] and is in line with the European Guidelines for Prevention in Low Back Pain [3]. According to the NIM, the spine is considered to be a strong structure and pain is seldom a sign of injury or disease caused by strain, but rather a functional disturbance [4]. Interventions based on the NIM are effective with respect to RTW among patients with LBP for a substantial proportion of participants [3–6]. More information about possible predictors for the effect of such interventions in preventing sick leave will provide valuable knowledge for future interventions.
For those who are already on sick leave as a result of LBP, fear avoidance beliefs, a low internal health locus of control and a negative expectancy of recovery are negative predictors for a RTW [6,9,10]. Fear avoidance beliefs are associated with sick leave, even when controlling for LBP, previous sick leave, age and work environmental factors [11]. However, evidence from non-clinical populations is scarce and it is therefore of interest to explore whether beliefs and expectations are valid as predictors of remaining at work in a non-patient population.
This study explored this issue in a sample of Norwegian employees who participated in atWork, a cluster randomized controlled trial of a workplace intervention based on the NIM. The aim of atWork is to prevent and manage the negative consequences of LBP in a population of municipal employees and it proved to be effective in reducing sick leave at the group level at the one year-follow up [8]. This study contributes data at the longitudinal individual level on sick leave among employees who participated in atWork and who consented to the gathering of individual data.
Changing misconceptions about LBP and enabling employees to cope with back and neck pain in the workplace are the core aims of atWork. The Cognitive Activation Theory of Stress (CATS) [12] is therefore an important theoretical framework for the intervention. CATS defines coping, which is essential for health, as the acquired expectancy that most or all responses lead to a positive result. Hopelessness (a negative response outcome expectancy) and helplessness (no response outcome expectancy), on the other hand, are associated with sustained activation, which may have major implications for health [12].
The aim of this study was to investigate the effect of atWork on sick leave at the individual level and to investigate whether belief in back pain myths, pain-related fear, helplessness/hopelessness and LBP predict the effect of the atWork intervention.
Materials and methods
Participants and procedures
All employees in two Norwegian municipalities were invited to participate in the atWork intervention in the period 2008–2010. There were estimated to be around a total of 3500 employees in the two municipalities at the initiation of the study. The effect of the intervention on sick leave at the unit level and details of the procedure and interventions have been published elsewhere [8]. As the intervention was carried out in workplace units, a cluster randomized design was chosen. A total of 125 work units (clusters) in the municipalities were randomized into three groups: (a) educational meetings and peer support; (b) educational meetings, peer support and access to an outpatient clinic; or (c) a control group that received treatment as usual (Figure 1). The randomization of whole units, stratified according to sector (e.g. schools or nursing homes) was carried out at Uni Health using computer-generated random numbers. As a result of the nature of the intervention, it was not possible to blind participants to their allocation.
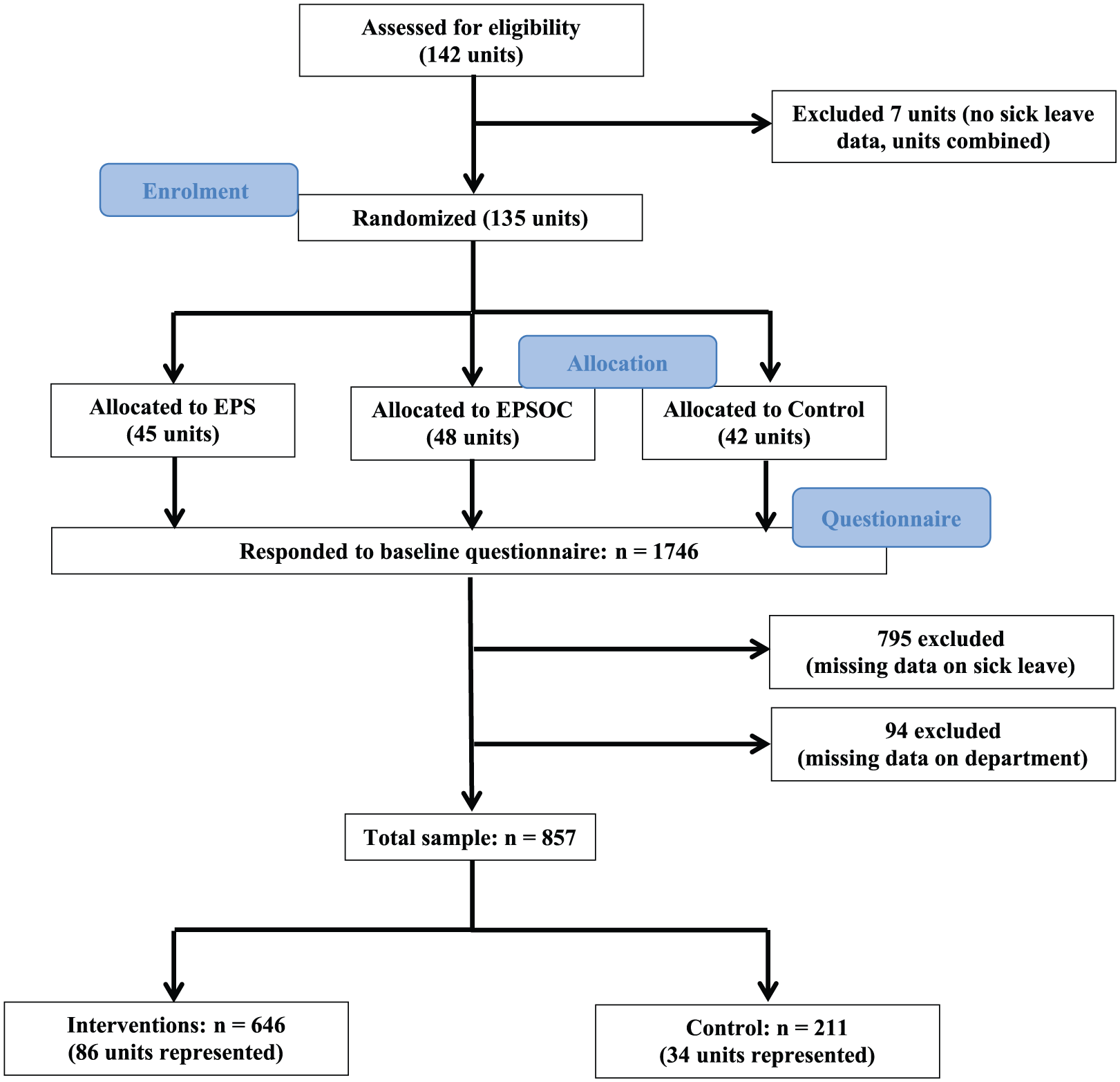
Flow chart for participants.
All employees who were randomized to any of the intervention groups received two to four educational meetings at their workplace. Evidence-based information about LBP based on the NIM and the European guidelines for LBP was presented at these meetings [6,7]. A peer adviser was selected from among the employees in each work unit. The peer adviser was a colleague who received a brief education regarding back pain and was able to assist colleagues with information and support to increase their likelihood of staying at work. In addition, in the intervention group with access to an outpatient clinic, the peer adviser could, if needed, directly refer the employee to the clinic. The control group did not receive any intervention. The control group and the intervention groups were free to receive treatment as usual from their general practitioners and the Norwegian health care system.
At baseline, 1746 employees responded to the questionnaire, a response rate of about 50%. Together with the baseline questionnaire, the participants received a consent form asking for permission to collect register data on sick leave from the Norwegian Labour and Welfare Administration (NAV). Only data from employees providing such consent were included in this study (n=795). Participants with missing data on their workplace unit (n=94) were also excluded because this information was necessary to determine which group the participants were randomized to. The two intervention groups were combined into a single intervention group because few workers attended the outpatient clinic and the result from either intervention was similar with respect to sick leave. Consequently, 646 participants (mean±SD age 44.2±10.81 years; 86% women) constituted the intervention group and 211 participants (mean±SD age 43.1±11.62 years; 88.2% women) constituted the control group (Figure 1).
Ethics
The study followed the Helsinki Declaration and was approved by the Norwegian Regional Ethics Committee in Western Norway (REK vest, ID 6.2008.117). The Norwegian Social Science Data Services recommended the study (NSD, ID 18997), in addition to the privacy authority at the Oslo University Hospital (Rikshospitalet, ID 08/2421).
Instruments
Outcome variable
Sick leave was measured at the individual level by individual registry data from NAV. In Norway, the employer pays the first 16 calendar days of a sick leave period. After the 16-day period, NAV covers the disbursement with sick leave benefits equal to 100% of past earnings. The available data were based on the sickness payment database from NAV. In cases where the employees were listed as sick for more than 16 days, these 16 days were also included in the data material. In this study, the number of days on sick leave was calculated for the 12 months prior to and during the intervention.
Predictor variables
All predictor variables were measured at baseline. LBP was measured by a single item from the Subjective Health Complaints inventory [13] asking whether the participants had experienced LBP in the last 30 days. This item was rated on a four-point scale from 0 (no complaint) to 3 (serious complaints). The item was dichotomized to 0 (no or some complaints) and 1 (many or severe complaints).
Attitudes and beliefs regarding LBP were measured by two items from Deyo’s back pain myths [14]. Deyo originally proposed seven myths that represent misconceptions regarding LBP [14,15]. Two of these myths were explored in the current study as these are specifically addressed in atWork [8], in addition to being the most prevalent in the general population [15]: (a) ‘Most back pain is caused by injury and heavy lifting’ (Myth lifting) and (b) ‘Everyone with back pain should have a spine X-ray’ (Myth X-ray). The items were rated on a five-point scale from 1 (totally disagree) to 5 (totally agree). The items were dichotomized to 0 (totally disagree, disagree, neither disagree nor agree) and 1 (agree and totally agree).
Pain-related fear was measured by the Tampa Scale for Kinesiophobia [16,17]. The scale consists of 13 items measuring fear of back (re)injury due to movement rated on a four-point scale from 1 (totally disagree) to 4 (totally agree). The scale was dichotomized based on the mean value for the sum-score (mean 25.4) into 0 (low, below the mean) and 1 (high, above the mean).
Helplessness and hopelessness were measured by six items from the Theoretically Originated Measure of the Cognitive Activation Theory of Stress (TomCats) [18], designed to measure response outcome expectancies in CATS [12]. The scale consists of three factors representing the three response outcome expectancies in CATS. In this study, helplessness and hopelessness were treated as one single factor based on factor analysis from a previous publication from the same sample [19]. Examples of statements are: ‘I really don’t have any control over the most important issues in my life’ (helplessness) and ‘All my attempts at making things better just make them worse’ (hopelessness). All items were rated on a five-point scale from 1 (not true at all) to 5 (completely true). The scale was dichotomized based on the mean value (10.2) into 0 (low, below the mean) and 1 (high, above the mean).
Statistical analyses
Differences between the intervention and control groups at baseline on the predictor variables were tested with independent samples t tests.
The means and SD values and the percentage of participants on sick leave in the three-month periods one year before and the year during the intervention were calculated. Mean values and 95% confidence intervals were calculated for days of sick leave stratified by the predictors (high/low) in the intervention and control groups for the year during the intervention.
Days of sick leave in three-month periods during the year of the intervention were analysed using generalized estimating equations [20]. Using this approach, corrections for the clustered nature of the data were accounted for [21]. The analyses were based on least-squares estimators and the identity link function. Standard errors were calculated based on a robust variance estimator corrected for clustering of data. Differences in days of sick leave for the year preceding the intervention were adjusted for in the analyses to control for differences in the initial sick leave between the intervention and control groups. No further variable was adjusted for in the analyses. Adjustment for clustering was carried out at the unit level, i.e. on workplace department.
For differences in the effect on days of sick leave between the intervention and control groups, adjusted mean difference scores and 95% confidence intervals with corresponding p values were calculated. Six models, including the interaction effect of days of sick leave for the dichotomized (high/low) predictors and intervention, were conducted to test whether there were statistically significant differences between the intervention and control groups regarding the effect of the predictors on sick leave. There was one for the total effect and five for each of the predictors. The selection of the predictors was based on the theoretical framework of the atWork intervention, i.e. the NIM and CATS scales. The interaction terms were composed by dummy variables for the predictors and dummy variables for the time dimension. Each model included four interactions terms based on the four time periods: 0–3, 3–6, 6–9 and 9–12 months. For significant results, stratified analyses of the predictors were conducted to calculate the effect within the two categories (high/low).
The statistical analyses were performed using SPSS version 21.0 (IBM Corporation, Armonk, NY, USA) for Windows; p < 5% (0.05) was considered statistically significant.
Results
Descriptive statistics
There was no statistical significant difference at baseline between the intervention and control groups in the predictor variable. The prevalence of days of sick leave in the year before the intervention differed between the intervention and control groups (Table II). The mean scores for overall sick leave days, stratified by high and low baseline scores on the predictor variables in the intervention and control groups, are presented in Table III.
Results for the predictor variables of low back pain, Deyo’s myths (myth lifting, myth X-ray), pain-related fear and helplessness/hopelessness in the intervention and control groups. Differences between groups at baseline tested with independent sample t tests.
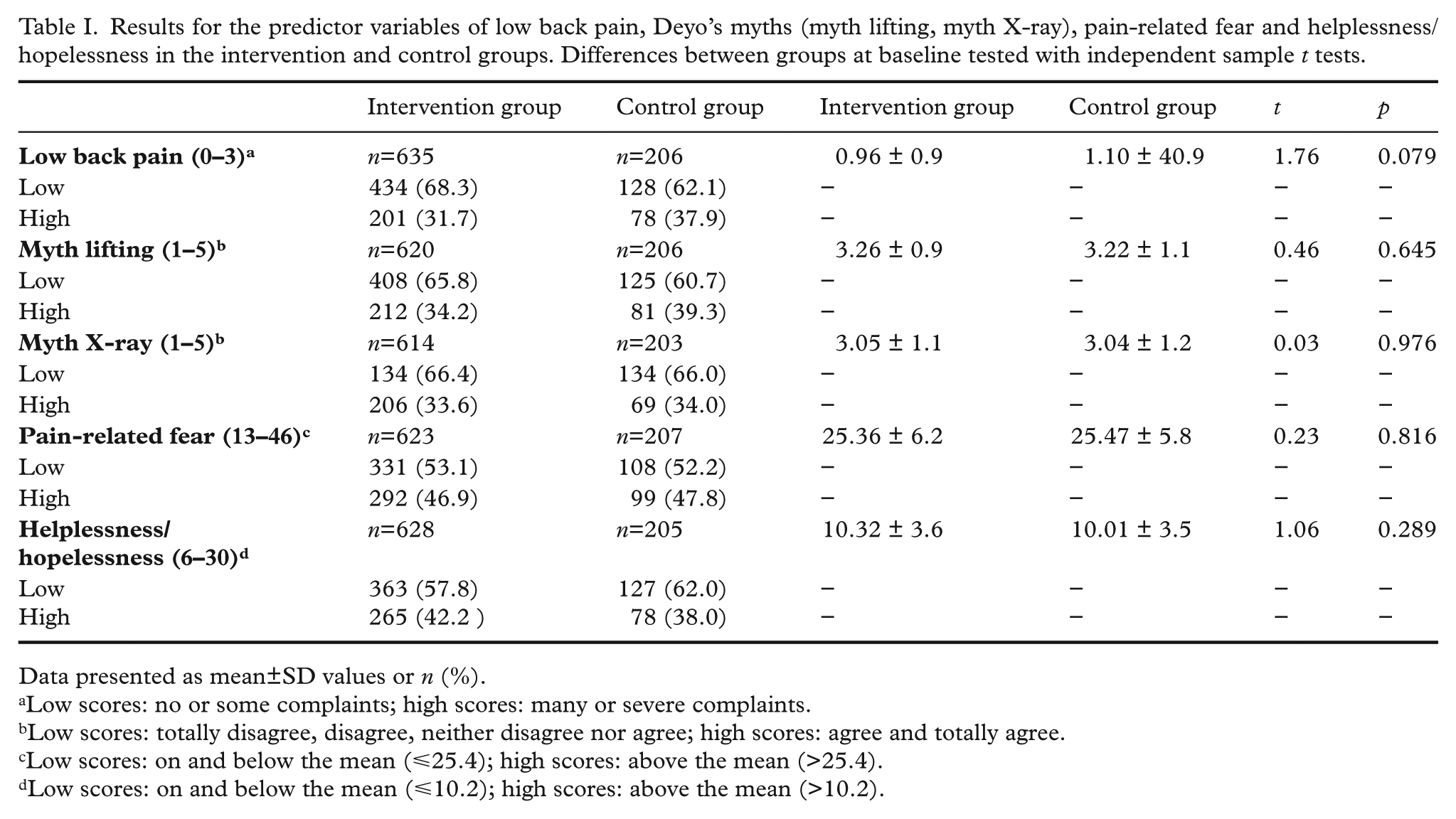
Data presented as mean±SD values or n (%).
Low scores: no or some complaints; high scores: many or severe complaints.
Low scores: totally disagree, disagree, neither disagree nor agree; high scores: agree and totally agree.
Low scores: on and below the mean (⩽25.4); high scores: above the mean (>25.4).
Low scores: on and below the mean (⩽10.2); high scores: above the mean (>10.2).
Number of days of sick leave in blocks of three months for the year before and the year during the intervention and percentage of participants on sick leave for one or more days during the three-month periods.
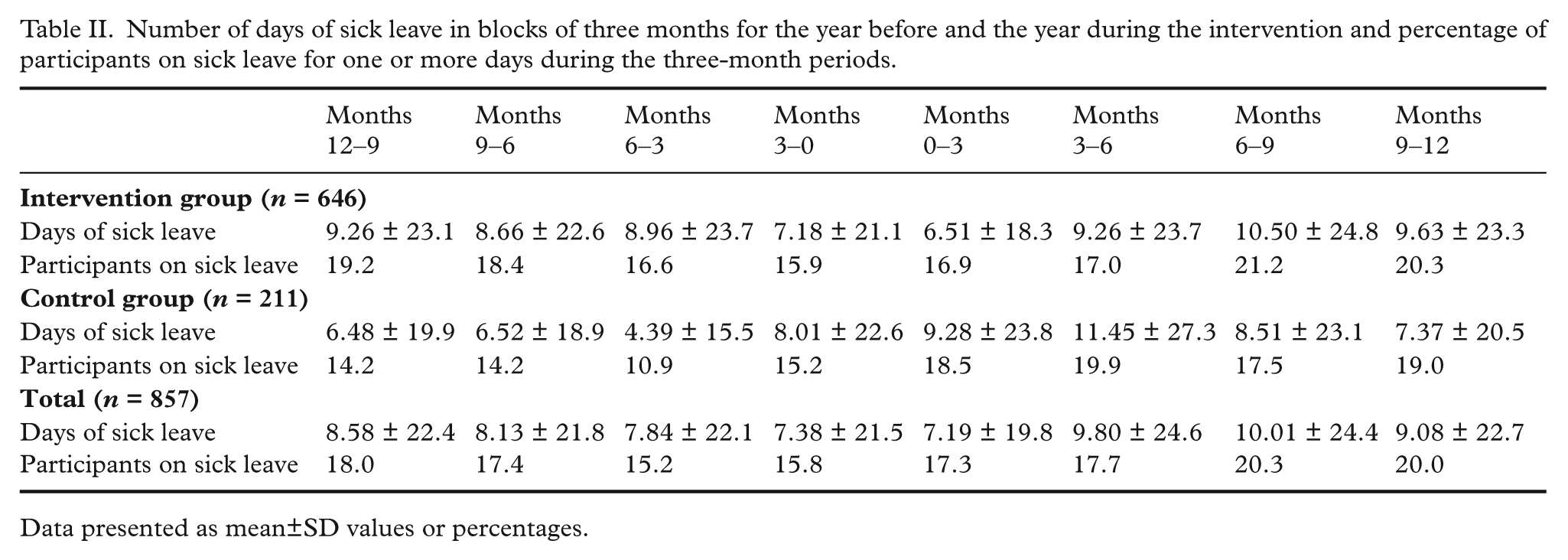
Data presented as mean±SD values or percentages.
Unadjusted mean scores and 95% confidence intervals (CIs) for days of sick leave stratified by high and low baseline scores on low back pain, Deyo’s myths (myth lifting, myth X-ray), pain-related fear and helplessness/hopelessness in the intervention and control groups.
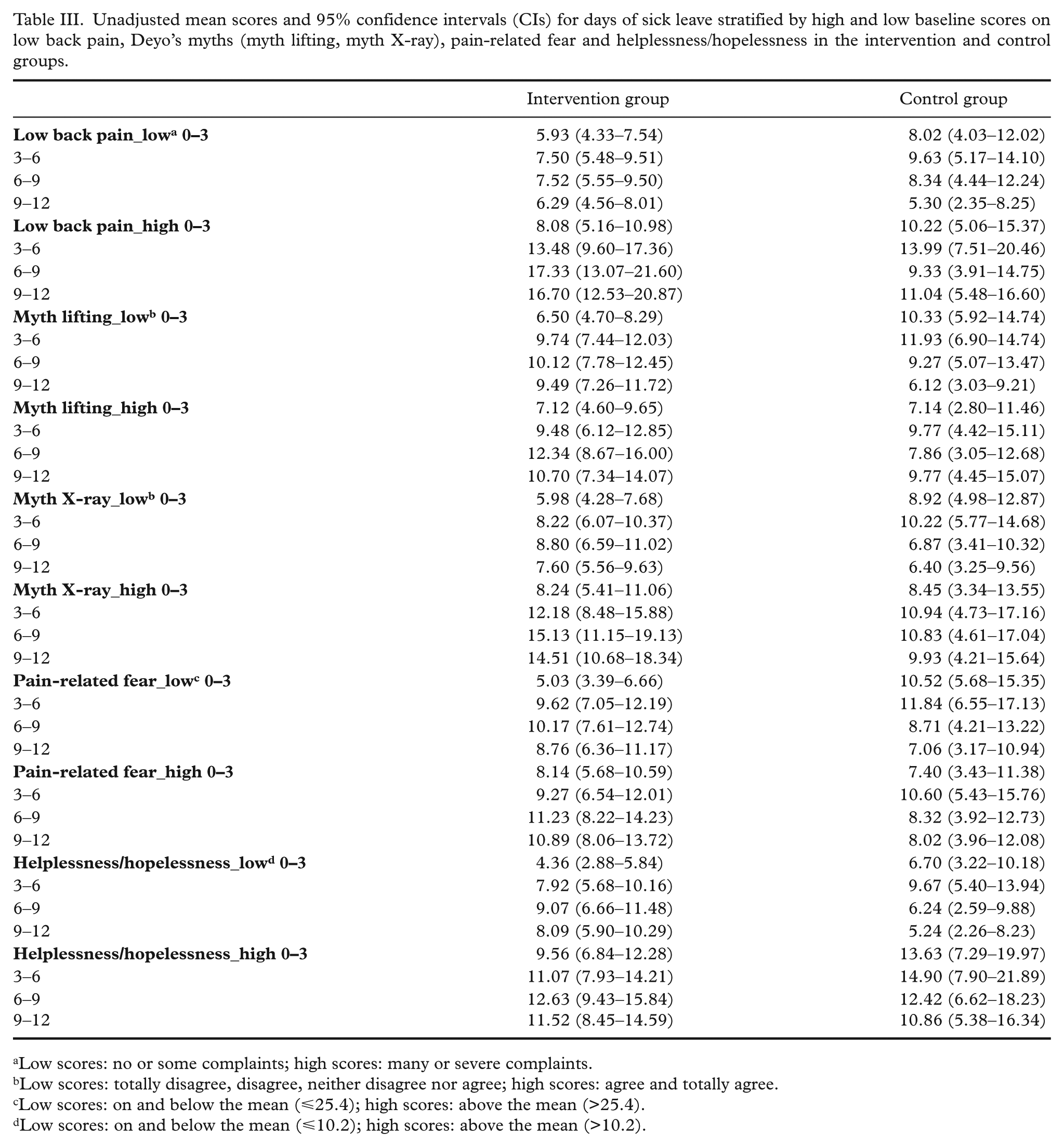
Low scores: no or some complaints; high scores: many or severe complaints.
Low scores: totally disagree, disagree, neither disagree nor agree; high scores: agree and totally agree.
Low scores: on and below the mean (⩽25.4); high scores: above the mean (>25.4).
Low scores: on and below the mean (⩽10.2); high scores: above the mean (>10.2).
Effect of the atWork intervention on sick leave
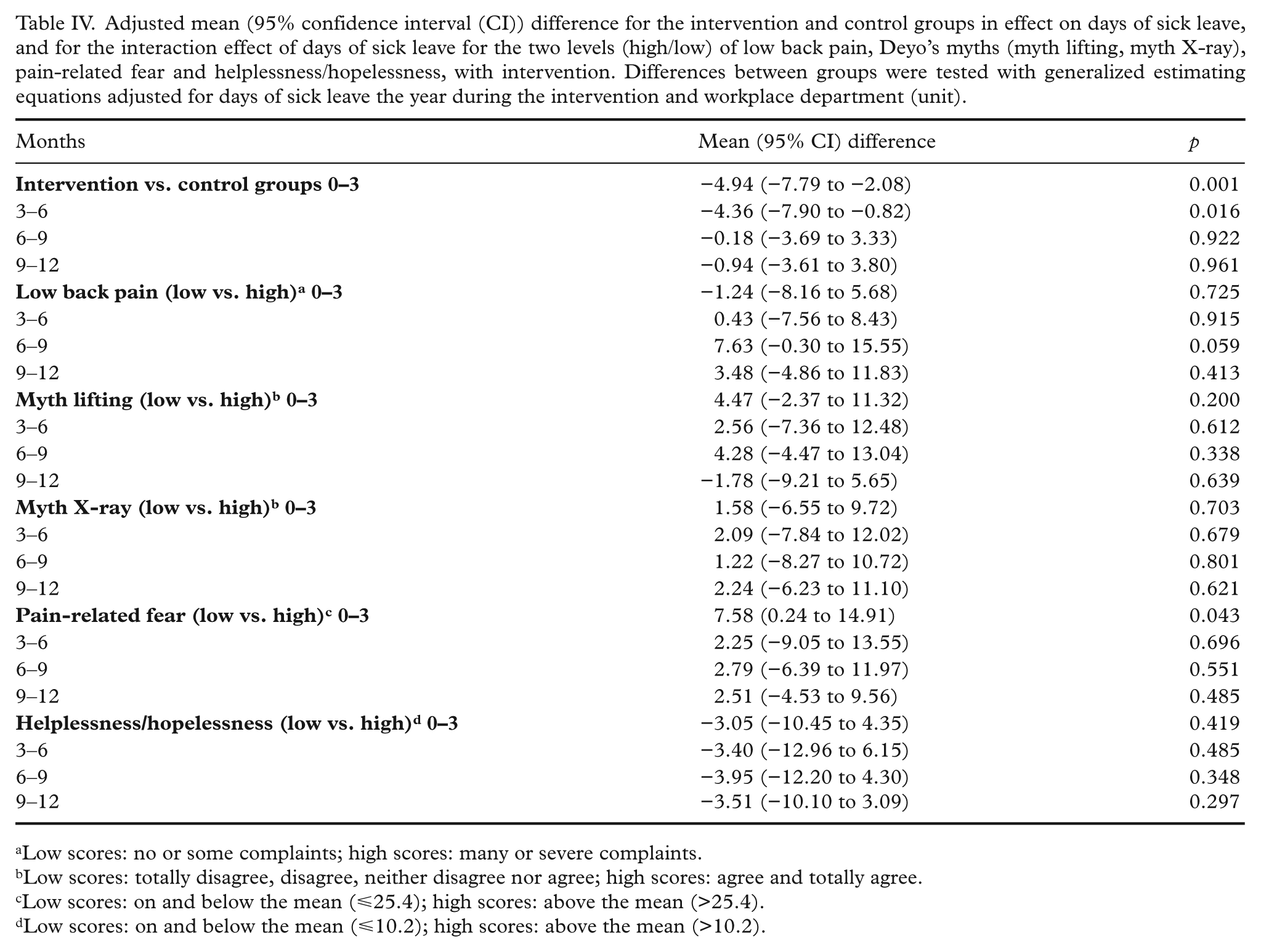
The adjusted analyses showed a statistically significant effect of the intervention on days of sick leave in the first six months during the intervention (Table IV). Employees in the intervention group had, on average, an effect of 4.9 less days of sick leave in the first three months and 4.4 less days of sick leave in the next three months during the intervention compared with the control group (see Table II for mean± SD values; also Table IV). When calculating the difference between the groups based on the estimated and adjusted means, the difference in change was 45.6% for the first three months and 41.4% for the next three months. There was no statistically significant effect of the intervention on days of sick leave subsequent to the first six months (Table IV).
Adjusted mean (95% confidence interval (CI)) difference for the intervention and control groups in effect on days of sick leave, and for the interaction effect of days of sick leave for the two levels (high/low) of low back pain, Deyo’s myths (myth lifting, myth X-ray), pain-related fear and helplessness/hopelessness, with intervention. Differences between groups were tested with generalized estimating equations adjusted for days of sick leave the year during the intervention and workplace department (unit).
Low scores: no or some complaints; high scores: many or severe complaints.
Low scores: totally disagree, disagree, neither disagree nor agree; high scores: agree and totally agree.
Low scores: on and below the mean (⩽25.4); high scores: above the mean (>25.4).
Low scores: on and below the mean (⩽10.2); high scores: above the mean (>10.2).
Effect of the intervention on sick leave within different levels of beliefs, expectancies and LBP
There was a statistically significant effect of the intervention on days of sick leave for the different levels of pain-related fear measured at baseline for the first three months (Table IV). Thus stratified analyses of this predictor were conducted to calculate the effect within the two categories (high/low). The adjusted mean difference between the intervention and control groups on low pain-related fear for the three first months was −8.03 (95% confidence interval (CI) −12.88 to −3.17, p<0.001), indicating that employees in the intervention group with low (⩽25.4) scores had, on average, an effect of 8.03 less days of sick leave in the first three months during the intervention compared with the control group (Table III). When calculating the difference between the intervention and control groups within the low levels of pain-related fear, the difference in change was 67.8% for the first three months. There was no statistically significant effect of the intervention for the levels of pain-related fear subsequent to the first three months.
There was no statistically significant difference in the effect of the intervention between individuals high and low scores on the other predictor variables (back pain myths, helplessness/hopelessness and LBP) (Table IV). Thus stratified analyses of these predictors to calculate the effect within the two categories were not conducted.
Discussion
The main aim of this study was to investigate whether there was an effect of atWork on sick leave and to identify the baseline characteristics of the participants that could contribute to this effect. There was an effect on sick leave the first six months during the intervention.
This is in line with, and expands on, the findings by Odeen et al. [8] by showing individual effects among those consenting to the gathering of individual data and also showing exactly when the effect occurred during the first year. Our results regarding the short-term effects are also in accordance with a previous similar intervention study among patients with LBP [5]. However, effects on RTW are found for up to five years in a clinical population [6]. In a clinical setting, the message is tailored to fit individual needs, which might result in a stronger effect than in the atWork study, which is designed to reach all employees present at work. The effect of atWork on sick leave is still important because population-based preventive interventions often require long-term implementation for an effect to occur [22].
In this study, low scores on pain-related fear predicted the effect of the intervention. This result is in accordance with a recent systematic review of back pain interventions, which showed that high fear avoidance beliefs at baseline were associated with poor treatment outcomes in terms of more pain and/or disability and less RTW [10]. Also in line with this study, Staal et al. [23] found that workers with scores equal to or above the median on fear avoidance beliefs at baseline RTW more slowly after participating in a graded activity intervention than those with scores below the median.
While expectancies are generalized, pain-related fear represents specific beliefs regarding fear of movement or (re)injury when in pain, which might explain why pain-related fear was the only significant predictor in this study. In a previous qualitative study, participants in an educational intervention similar to atWork emphasized trust in professionals and improved understanding as important aspects contributing to their coping with their disorders [24]. Strong pain-related fear can hamper confidence in professionals and the information they receive from the intervention. Furthermore, the NIM might be more conceivable for employees with low pain-related fear. For employees with low or moderate scores on pain-related fear, atWork might provide the reassurance they need to be able to stay at work despite pain. Employees with strong and deep-rooted pain-related fear may need something else, e.g. more extensive, multidisciplinary treatment than those provided in atWork, or an intervention targeting pain-related fears, including their performance of practical tasks. Cognitive behavioural therapy has been shown to be effective in reducing avoidance, catastrophizing and disabling beliefs among patients with LBP [25], but might also have a negative effect on disability for individuals with low scores on fear avoidance [26].
Strengths and limitations
A major strength of the current study is that the outcome was measured by registry data on sick leave that are considered to be highly accurate and thus to reduce the risk of measurement errors. The sample is relatively large and, as a result of the sample diversity regarding workplace size and work tasks, the possibility of group-specific effects and localization effects were reduced. The high predominance of women in the sample (87.2%) is representative of the municipality sector in Norway [27]. A further strength of the study is that all unit types (e.g. kindergartens and nursing homes) were represented in the sample and there was no systematic dropout from any unit type on responses to the questionnaire.
This study contributes to increasing our knowledge about the effects of a workplace-based, low-cost, low-threshold sick leave intervention. Municipal employees have a relatively high sickness absence compared with employees in the private and state-level public sectors [28]. This study addresses one of the sectors with the highest rates of long-term sick leave.
A limitation of this study is the lack of a published protocol. The low response rate of about 50% might increase the risk of non-response bias and limit the validity of the findings. It would have been relevant to investigate whether men and women showed different effects of the intervention, but the low number of men in the study could not justify such analyses. Caution should therefore be made when generalizing to private sector employees and to men.
In cases where employees are listed as sick for 16 days or less, sick leave is not registered in NAV and was thereby missed in this study. Although we were most interested in long-term sick leave as a result of its negative consequences, both for the individual person and for society, it would have been interesting to see how the intervention affected short-term sick leave. As a result of data protection issues, information about the diagnoses for which the individual participants were listed as sick was not available. However, there is a high degree of comorbidity in subjective health complaints [29] and a huge variation in which diagnosis the general practitioner chooses when presented with the same patient [30], making the specific diagnoses less relevant in this setting.
A further limitation of this study is that we cannot exclude the possibility of confounding variables because the unit of randomization was different from the unit of analysis. However, adjustment for sick leave the year before the intervention and for the clustering of data within the unit of randomization justifies the analyses. Some of the subgroups were small. This resulted in wide confidence intervals, which also indicated a low power for these analyses.
Implications
Knowledge of which individual people will benefit from workplace interventions is important for authorities in focusing such interventions. Excluding workers with high levels of pain-related fear seems unrealistic as well as unethical. The intervention has a preventive approach towards all employees present at work. More knowledge of the characteristics of individuals high scores on pain-related fear, and why these people do not respond to interventions such as atWork, is needed. Future studies should explore mediational effects, i.e. whether expectancies and beliefs change as a result of the intervention, and whether these changes predict the effect on sick leave.
Conclusions
The atWork intervention had an effect on days of sick leave at the individual level in the first six months during the intervention and low levels of pain-related fear predicted the effect. There was no difference in the effect of the intervention between individuals high and low scores on helplessness and hopelessness, belief in the back pain myths and LBP. As the effect of atWork on sick leave was limited to the first six months, indicating a need for repetition of the intervention message, the educational part of atWork should be tested in primary health care and considered implemented as a part of regular practice in primary care if the results are positive.
Footnotes
Acknowledgements
Trial registration ![]() , registration number: NCT00741650. Thanks to Erik Lindh and Magnus Odeen for coordinating the project, and to Camilla Ihlebæk for assisting in the design and in conducting the study. Thanks to Britt Øvregård and Berit Borge at the municipalities for help in the project and to Nina Konglevoll for technical assistance.
, registration number: NCT00741650. Thanks to Erik Lindh and Magnus Odeen for coordinating the project, and to Camilla Ihlebæk for assisting in the design and in conducting the study. Thanks to Britt Øvregård and Berit Borge at the municipalities for help in the project and to Nina Konglevoll for technical assistance.
Conflicts of interest
The authors declare that there is no conflict of interest.
Funding
The study was financially supported by the Norwegian Extra Foundation for Health, by the South-Eastern Norway Regional Health Authority and by the Hospital at Vestfold, Stavern.