
Abstract
Aims: To investigate the associations between physical activity and the pattern of risk health behaviour consisting of smoking, alcohol consumption, snuff (snus), cannabis, and condom use among 15-year-old adolescents, taking their educational aspirations and family affluence into account. Methods: The data were collected in the Health Behaviour in School-aged Children (HBSC) study in Finland in 2006. Standardised questionnaires were issued at schools to a 15-year-old nationally representative sample, of which 84.5% (1710 pupils) participated. Logistic regression analysis was used to explore the associations between physical activity, pattern of risk health behaviour, family affluence, and educational aspirations. Separate models for daily moderate-to-vigorous physical activity (MVPA) and leisure-time physical activity (LTPA) were tested. Multi-level analysis was performed in order to control the nested characteristics of the data. Results: Boys were significantly more physically active and used alcohol, cannabis, and snuff more often than girls. Girls had used a condom in their last intercourse less often than boys. The educational aspirations for higher education had the strongest association with the low-risk health behaviour, with the odds ratios in the MVPA model 3.30 (95% CI 2.41–4.55) for the boys and 3.46 (95% CI 2.56–4.67) for the girls. In the LTPA model, the corresponding odds ratios were 3.31 (95% CI 2.40–4.56) for the boys and 3.52 (95% CI 2.60–4.56) for the girls.
Introduction
A common belief is that physical activity in childhood and adolescence affects the patterns of health behaviour. The marketing of physical activity and sports, particularly among children and adolescents, often leans on the image linking physical activity to other health-enhancing behaviours. However, this perception is supported by limited scientific evidence.
It is of great importance to study the trends and associations of physical activity in adolescence, because it is a period of life during which many individuals adopt the lifestyles and habits which will last throughout adulthood [1,2]. Consistently recognised determinants or correlates of adolescents’ physical activity include previous physical activity, greater sensation-seeking tendencies, participation in community sports, and having opportunities to exercise [3,4]. Moreover, single health behaviours associated with adolescent physical activity seem to be numerous. Across the studies [5–7], probably the most reported health-related risk behaviour associated with low physical activity is smoking. In the literature, risk behaviour refers to sensation-seeking behaviour that has been reviewed elsewhere by Roberti [8].
There is little consistent evidence that, apart from smoking, other substance use behaviours such as alcohol drinking have corresponding associations with physical activity. In a review of 108 studies, Sallis et al. [4] found no clear associations between alcohol consumption and physical activity. Some studies have reported of a greater risk for the least physically active adolescents to drink more alcohol [9] or to use more cannabis [10]. Conversely, other studies have found that physically active adolescents drink more alcohol [11] and use snuff more commonly [12] than the less physically active adolescents.
Apart from substance use, also other forms of behaviour are recognised as risk behaviour in adolescence. Risky sexual behaviour often has consequences later in adolescence comparable to substance use. Metzler et al. [13] and Tapert et al. [14] studied sexual risk-taking as a part of risk behaviour. The relationship between sexual behaviour and physical activity has not been as extensively examined as the associations between substance use and physical activity. Sexual activity and physical activity have diverse associations according to authors [15,16].
Despite the increasing amount of evidence on associations of single risk behaviours, less is known about the prevalence and distribution of multiple behavioural risk factors in youth. This is the major reason why many studies concentrate on the clusters of the health behaviours. Aarø et al. [17] suggested a hypothesis of two-dimensional health behaviour in adolescence, whereas Mistry et al. [18] found a four-factor solution of healthy and unhealthy behaviours. Both of the aforementioned studies highlight the significance of physcial activity in the clustering of healthy behaviour. These results from different studies indicate that the clusters of health behaviour are diverse and more investigation is needed.
To make the associations even more multifaceted, associations between health behaviours and socioeconomic factors have been reported. Research has consistently documented social class gradients in child and adult health. Low socioeconomic status (SES) has been reported to associate with poorer diet, smoking, and less physical activity than high SES [19]. However, according to a recent review, substance use behaviours such as alcohol and cannabis use did not significantly associate with SES during adolescence [20].
Being a complex mode of behaviour, all physical activity is not inevitably associated with less risky behaviours than sedentary behaviour would be. The concept of physical activity encompasses a wide variety of physical movement. Physical activity may change daily and from one week to another. Therefore, also the additive effect of physical activity in the clustering of the health-enhancing behaviours can alter by the different modes of physical activity. The aim of this study was to investigate the associations between two different measures of physical activity and the pattern of risk behaviours (smoking, alcohol consumption, experiences of drunkenness, snuff (snus) and cannabis use, and condom use) among Finnish 15-year-old adolescents, taking their future educational aspirations and family affluence into account.
Materials and methods
Study population
The present study is based on the Finnish part of the Health Behaviour in School-aged Children (HBSC) 2006 study, which is a cross-national school survey conducted by an international network of research teams from 41 countries and regions in collaboration with the WHO Regional Office for Europe. Its aim is to provide key insights into the health-related behaviours of young people and to increase understanding of adolescent health, well-being, health behaviour, and social context [21]. The populations selected for sampling are young people aged 11, 13 and 15 years. The study methods are outlined below, with a more comprehensive description available elsewhere [21].
The data for this study were collected through school-based surveys; anonymous, standard questionnaires were issued to a 15-year-old nationally representative sample in Finland between March and May 2006. Standard cluster-sampling was followed regionally and conducted in accordance with the structure of the national education system. The primary sampling unit was the school and the questionnaires were sent to 100 schools, of which 95% participated. Of all the 15-year-old pupils in the sample, 84,5% (n = 1710) responded to the questionnaire. After statistical cleaning processes, the data consisted of 1670 15-year-old pupils from the nineth grade (mean age 15 years 8 months, p = 0.616 between gender).
Measures
The item measuring the amount of daily moderate-to-vigorous physical activity (MVPA) was developed by Prochaska et al. [22] as a single measure assessing the accumulation of 60 minutes of MVPA. The subjects were first provided with a definition and some examples of physical activity. After this, subjects were asked “Over the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” MVPA was dichotomised as follows: a group consisting of those physically active on 0–5 days during the preceding week and a group consisting of those active on 6–7 days during that time.
Leisure-time physical activity (LTPA) was measured by focussing on vigorous physical activity outside school hours, different from the MVPA measure: “Outside school hours, how often do you usually exercise in your free time so much that you get out of breath or sweat?” (every day; 4−6 times a week; 2−3 times a week; once a week; less than once a month; never). LTPA was dichotomised as following: a group consisting of those exercising at least four times a week and a group consisting of those exercising 2–3 times a week or less often outside school hours.
The selected risk behaviours included variables of smoking, alcohol drinking, experiences of drunkenness, cannabis and snuff (snus) use, and condom use in the last sexual intercourse. The risk behaviours were selected on the basis of scientific evidence in earlier studies concerning adolescent risk behaviours.
Smoking was assessed by an item: “How often do you smoke tobacco at present?” (every day; at least once a week, but not every day; less than once a week; I do not smoke). The smoking item was dichotomised by combining the last two options as “non-smokers” and the first two as “regular smokers”.
Snuff (snus) use was assessed by the question: “Do you use snuff at present?” (every day; at least once a week, but not daily; less often than once a week; I don’t use snuff). The item was dichotomised by keeping the last alternative “non-users” and combining the first three alternatives as “snuff users”.
Alcohol consumption was measured by the question: “At present, how often do you drink anything alcoholic, such as beer, wine, or spirits/liquor, other alcoholic drinks, and any other drink that contains alcohol?” (every day; every week; every month; rarely; never). A composite alcohol consumption measure was created by considering the pupils’ answers to any type of the above-mentioned alcohol as a single measure and dichotomised by combining the options “rarely” and “never” as “non-drinkers” and the first three alternatives as “regular drinkers”.
Experiences of drunkenness was measured by the question: “Have you ever had so much alcohol that you were really drunk?” (no, never; yes, once; yes, 2–3 times; yes, 4–10 times; yes, more than 10 times). The item was dichotomised by combining the first three options as “0–3 times” and forming the “4 times or more” group from the remaining two alternatives.
Cannabis use was evaluated with an item “Have you ever taken cannabis in your life?” (never; once or twice; 3–5 times; 6–9 times; 10–19 times; 20–39 times; 40 times or more). The item was dichotomised by keeping the option “never taken” as one group and combining all the remaining options as “taken at least once” group.
Sexual risk-taking behaviour was assessed by condom use in sexual intercourse as a combination of two items in the questionnaire: “Have you ever had sexual intercourse?” (yes; no) and “The last time you had sexual intercourse, did you or your partner use a condom?” (I have never had sexual intercourse; yes; no). The combined sexual risk-taking item consisted of two groups: First, adolescents in the “low-risk sexual behaviour group” either had never experienced intercourse or had used a condom in their last sexual intercourse. Second, the “risky sexual behaviour group” comprised the adolescents having experienced intercourse but had not used a condom in their last intercourse.
A confirmatory one-factor analysis demonstrated that the six risk behaviours may occur in the same factor (CFA (LISREL): p = 0.07, GFI = 1.0, AGFI = 1.0, CFI = 1.0, RMSEA = 0.022), and Cronbach’s alpha value (0.687) suggest a latent construct of risk behaviour. After each variable was dichotomised, a score for the composite risk behaviour was assigned by giving a score of “1” for risky exposure to the each of the factors and a score of “0” for no/less exposure. Thereafter, the scores were summed for each pupil across risk factors to calculate a risk behaviour index which represents the number of risk behaviours. Finally, the pupils were regrouped into two separate groups: The “low-risk behaviour” group (scores 0–2) and the “risk behaviour” group (scores 3–6).
The HBSC Family Affluence Scale (FAS) measure is based on a set of questions on the material conditions of the households in which young people live. The FAS comprise four items: “Does your family own a car, van, or truck?” (no; one; two or more), “Do you have your own bedroom for yourself?” (no; yes), “During the past 12 months, how many times did you travel away on holiday with your family?” (not at all; once; twice; more than twice), and “How many computers does your family own?” (none; one; two; more than two). The composite FAS score was calculated for each young person based on responses to these fourquestions. Subjects were divided into categories: FAS 1 (scores = 0–3) indicated low affluence, FAS 2 (scores = 4–6) indicated medium affluence, and FAS 3 (scores = 7–9) indicated high affluence [23].
Future educational aspirations were measured by the question: “What do you think you will be doing after elementary school?” (apply to general upper secondary school; apply to vocational education; apply for an apprenticeship/training; go to work; become unemployed; do not know). The responses “Do not know” and “Become unemployed” (n = 12) were excluded from the new variable. The remaining categories were dichotomised by renaming the general upper secondary school alternative as “higher education” and combining the remaining alternatives as “vocational education/work”.
Data analyses
The basic statistical analysis was performed using the SPSS 16.0 software package. The pairwise associations between the variables were tested with Chi-squared tests. Pearson’s correlation coefficients with t-tests were computed to test the relationships between the physical activity measures and the components in the risk behaviour index. Logistic regression analysis was used to test the multiple associations between the variables. Separate models for MVPA and LTPA were tested in order to examine whether the physical activity variables which were different in nature were also different according to the analysis. Structural equation modelling was used (LISREL 8.72) in the confirmatory factor analysis for the risk behaviours. Multilevel modelling (MLwiN 2.02) was used with the logistic regression analysis to control the nested characteristics of the data. The multilevel procedure modelled the pupils (level 1) within schools (level 2). The significance of the associations was measured with Chi-squared tests. The significance level was p < 0.05 in all statistical tests.
Results
Descriptive statistics
Table I shows that the boys were more physically active than the girls (p = 0.003, p = 0.002). Furthermore, the boys drank alcohol at least monthly more often (p = 0.009), used snuff (p < 0.001), and had tried cannabis more commonly than the girls (p < 0.001). About one out of 10 (10.2%) girls had not used a condom in their last sexual intercourse, whereas only about one in 20 (4.6%) boys had not used a condom in their last intercourse. The educational aspirations measure showed a statistically significant gender difference (p < 0.001), as the girls more commonly considered higher education than the boys did (66.0% vs 47.5%).
Distribution of health behaviours family affluence and educational aspirations among boys and girls
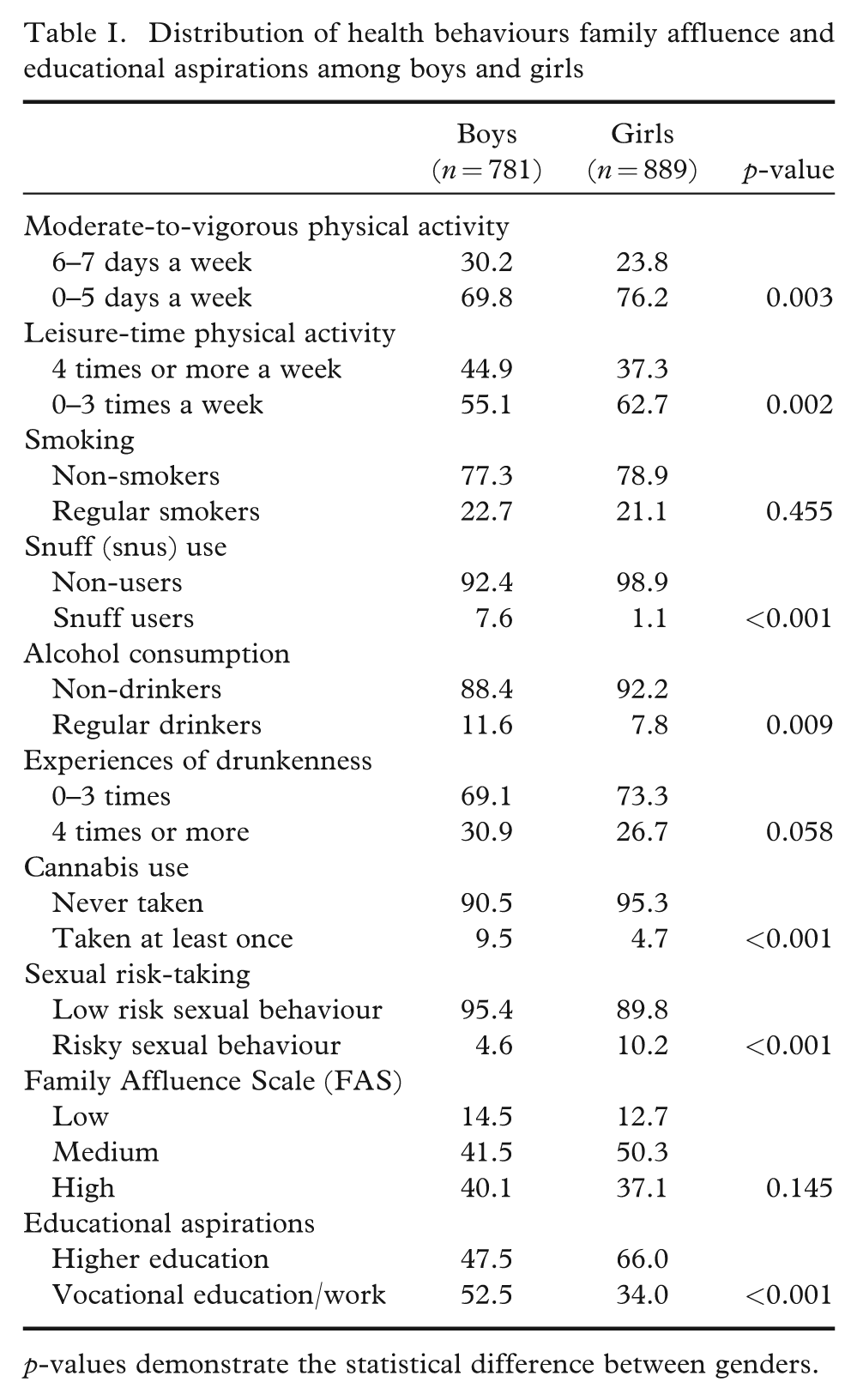
p-values demonstrate the statistical difference between genders.
Table II illustrates the correlations (Pearson) between the physical activity measures and the components in the risk behaviour index. The strongest correlations were found between smoking and the other risk behaviours (r ≥ 0.22). Only weak correlations (r ≤ 0.10) were found between the physical activity measures and the risk behaviours.
Pearson correlations between the physical activity measures and the components in the risk behaviour index
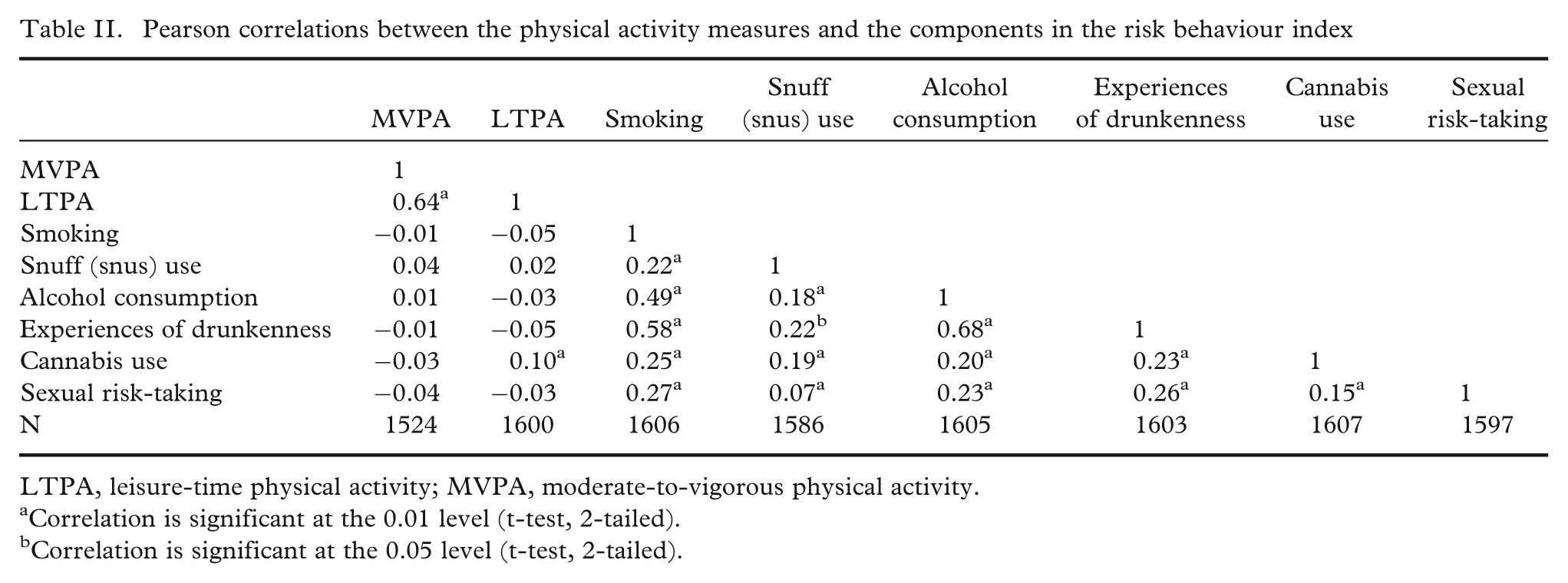
LTPA, leisure-time physical activity; MVPA, moderate-to-vigorous physical activity.
Correlation is significant at the 0.01 level (t-test, 2-tailed).
Correlation is significant at the 0.05 level (t-test, 2-tailed).
Table III shows that most of the adolescents were exposed to none of the risk behaviours, and gender was significantly associated with the number of risk behaviours; the proportion of girls in the low-risk group (with a maximum of two risk behaviours) being larger than that of boys. About one out of 10 (10.6%) adolescents possessed at least three of the selected risk behaviours.
Health risk behaviour scores among boys and girls
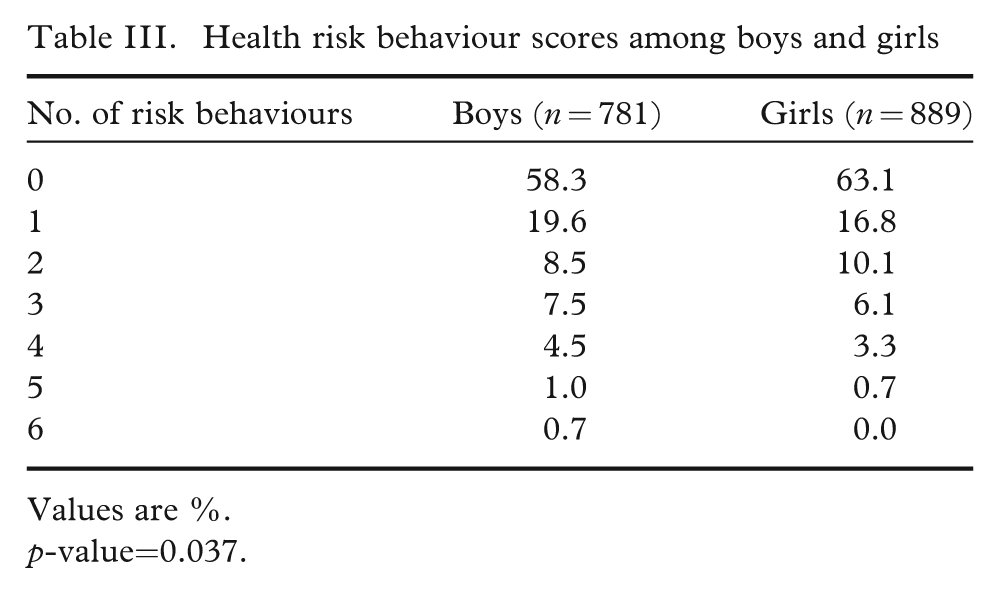
Values are %.
p-value=0.037.
Logistic regression model 1: daily MVPA and risk behaviours
In the model with MVPA, only the educational aspirations was associated with risk behaviour both in boys (OR 3.30, 95% CI 2.41–4.55) and in girls (OR 3.46, 95% CI 2.56–4.67). The higher education-oriented adolescents had more than three times the probability of belonging to the low-risk group than that of the ones planning for a vocational level education. Among the boys, a high level of MVPA was associated with the low number of risk behaviours, but this association disappeared after adjusting the model with family affluence. A high family affluence was associated with a low number of risk behaviours among the girls (OR 1.55, 95% CI 1.12–2.14) (Table IV).
Low-risk health behaviour by gender
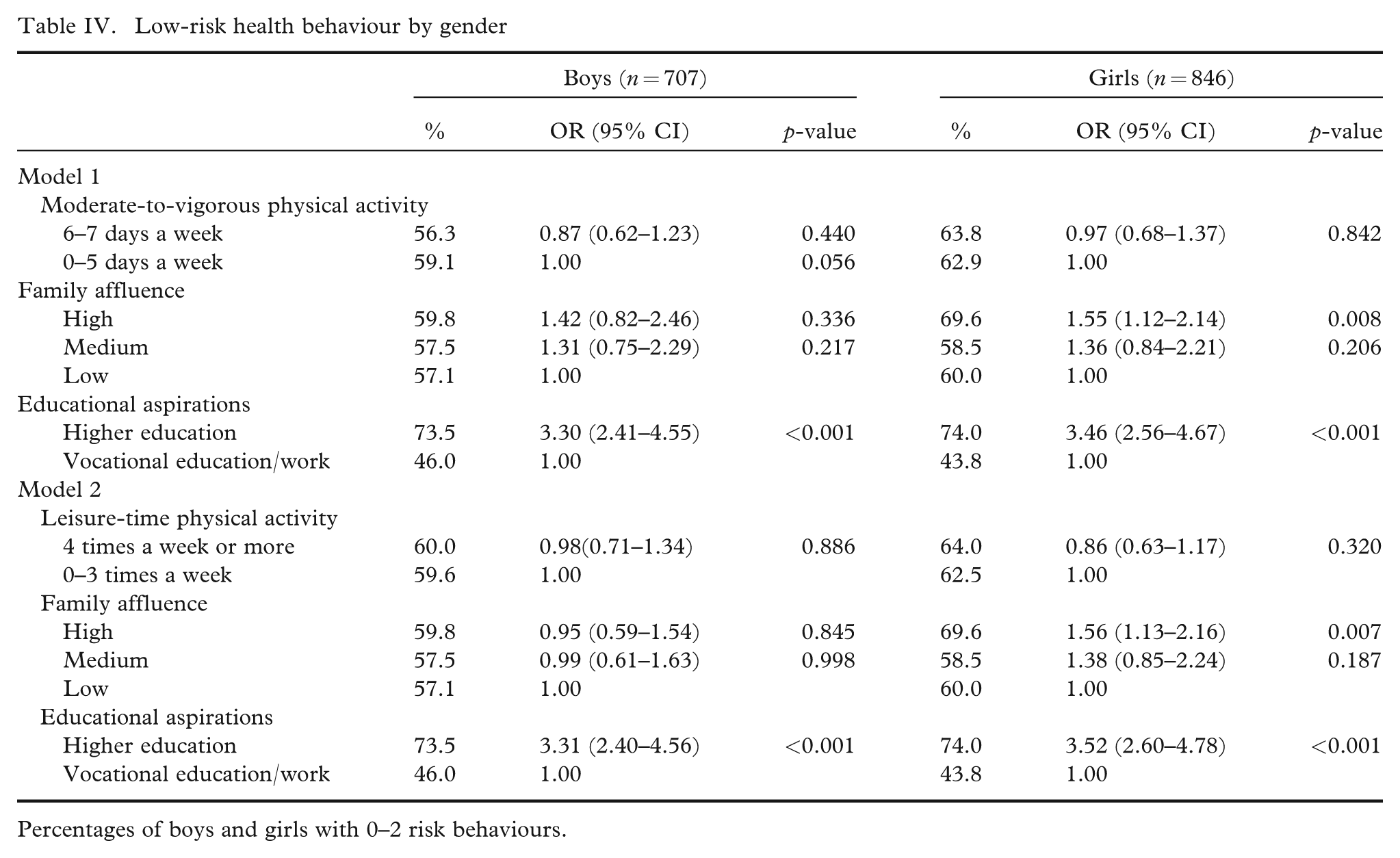
Percentages of boys and girls with 0–2 risk behaviours.
Logistic regression model 2: LTPA and risk behaviours
In the model with LTPA, the educational aspirations were associated with low-risk behaviour similarly as in the MVPA model among the boys (OR 3.31, 95% CI 2.40–4.56) and among the girls (OR 3.52, 95% CI 2.60–4.78). Futhermore, a high family affluence was associated with a low number of risk behaviours among the girls (OR 1.56, 95% CI 1.13–2.16) (Table IV).
Multilevel modelling was used to control the nested characteristics of the data. The procedure modelled the pupils (level 1) within schools (level 2). Despite the presumptions of the nature of the data, no significant clustering effect was found.
Discussion
In the present study, physical activity had no significant associations with low-risk health behaviours when the adolescents’ educational aspirations and family affluence were taken into account. The strongest correlations were found between smoking and other single risk behaviours. Most of the adolescents possessed none of the selected health risk behaviours and the proportion of girls with none of the risk behaviours was larger than that of boys. One in 10 adolescents had more than three risk behaviours that was classified as “risky health behaviour”. The strongest predictor of risk behaviour was the future educational aspirations, with boys and girls planning theoretical studies being exposed to less health-compromising and more health-enhancing behaviour than the ones planning vocational studies/work. This is consistent with the results of Friestad and Klepp [19]. Their study also indicated that educational aspirations as reported by the adolescents themselves may be a valid measure of their SES, as it is both stable from an early age and also related to parents’ educational status [19].
The results of this study indicate a social gradient when using a composite index of risk behaviour, in terms of a smaller number of health risk behaviours among those planning higher education. However, it is often suggested that socioeconomic inequalities in unhealthy behaviours already apparent in childhood level out in later adolescence, as a results of the declining influence of parents and an increasing influence of significant others (e.g. peers).
The results suggest that it is possible that other behaviours have a more distinctive clustering nature than that of physical activity. Physical activity may not protect children and adolescents from health-harming behaviour as such, but it provides a positive baseline for approaching the goals of health promotion. Moreover, this positive aspect has not been utilised sufficiently e.g. in sports associations or clubs. The development of health-promoting sports clubs has been a remarkable step forward in the fields of action [24].
The interpretation of the results is restricted by some methodological limitations. The cross-sectional study design does not allow drawing conclusions on causality. The observation is only based on a single point of adolescence and longitudinal studies are needed to investigate the stability of the associations, as the stability of physical activity has been studied [2]. Furthermore, this study is based on self-report measures which might lead to potential bias. The questionnaire answers commonly tend to underestimate physical activity [25]. In this study, the six risk factors were summed up to create a multiple risk factor index. This was supported by confirmatory factor analysis. There is also other theoretical and empirical evidence that use of equally weighted risk factor indices results in the identification of very similar “at risk” population subgroups than those identified by unequally weighted risk factor indices [26]. The key measures in this study have been either tested for validity or used similarly in wide international surveys [21,27].
Contrary to anticipations, physical activity was not significantly associated with the low-risk behaviour. Whilst considering the previously discussed methodological limitations, it is apparent that the physical activity phenomenon is difficult to categorise, and physical activity was measured here only in the two, yet different, types of general orientation. The first measure used here relate to time used to physical activity outside school hours and the second one sums up all physical activities during previous week, which encompasses a wider aspect. The MVPA measure functions today as the base for the recommendations for physical activity. A comprehensive examination of the phenomenon requires that the various modes of physical activity are taken into account. This is also important, because some forms of physical activity include components similar to sensation seeking and risk behaviour [8].
It should be considered, however, that different cultural settings provide variation also in the associations between health behaviours. In contrast to the results from many English-speaking and Western countries, in a Chinese study [11], participation in physical activity was a protective factor neither for smoking nor alcohol abuse. In fact, high-intensity physical activity was a risk factor for alcohol abuse.
Furthermore, as suggested by Koivusilta et al. [28], indicators of family’s material affluence should be developed further. The aspect of socioeconomic divergence in health has already turned into one of the most important priorities in public health policies internationally. Sound methods are needed for the comparability and applicability of the research.
Health-promotion implications
The results of this study suggest many health-promotion actions among adolescents. First, further studies are needed to find the most effective interventions [29]. Second, the promotion of physical activity is not solely enough for the prevention of risk behaviours. Parents, schools and sports clubs should underline that many of the risk behaviours in fact hinder physical activity, and the benefits of physical activity may disappear. The most effective method could be a combination of actions aiming at promoting physical activity, prevention of substance use, responsible sex behaviour, and also healthy diet. Third, clearly more action is needed to reduce the socioeconomic differences in health and health behaviour already in childhood and adolescence. In terms of physical activity, creating positive experiences and support by introducing a broad range of physical activities in physical education is probably the easiest and the most affordable action. School and extra-curricular physical activity are already highlighted in promoting daily physical activity and reducing the problem of overweight [30].
From the public health point of view, parents, schools, and even sports clubs should be able to offer affordable options for adolescents to be physically active. It is clear, however, that physical activity remains an applicable, yet little utilised, tool in promoting comprehensive health among adolescents.
Footnotes
Acknowledgements
The Health Behaviour in School-aged Children (HBSC) survey is an international study carried out in collaboration with WHO/EURO. The International Coordinator of the 2005/2006 study was Candace Currie (University of Edinburgh, Scotland) and the Data Bank Manager was Oddrun Samdal (University of Bergen, Norway). For details, see ![]() .
.
This study was supported financially by the Finnish Cultural Foundation (2006) and Juho Vainio Foundation (2006).