
Abstract
Background
Traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) are emerging contributors to the development and progression of dementia.
Objective
This study examined how traumatic brain injury and post-traumatic stress disorder relate to cognitive function and neuroimaging markers in U.S. veterans from the Department of Defense Alzheimer's Disease Neuroimaging Initiative (ADNI-DOD).
Methods
TBI severity was quantified with a new scoring system, and PTSD symptoms and combat exposure were assessed using the Clinician-Administered PTSD Scale (CAPS) and Combat Exposure Scale (CES). Cognitive performance was evaluated with the Mini-Mental State Examination (MMSE), Alzheimer's Disease Assessment Scale–Cognitive Subscale (ADAS-Cog), and Clinical Dementia Rating Sum of Boxes (CDR-SOB). Neuroimaging included amyloid-β (Aβ) and tau positron emission tomography (PET), diffusion tensor imaging (DTI), vascular imaging, and resting-state functional MRI (rs-fMRI).
Results
As expected, higher Aβ and tau burden were significantly associated with worse cognitive performance on the MMSE, ADAS-Cog, and CDR-SOB. Greater PTSD symptom severity was also linked to poorer cognition measured by all three tests, and higher TBI severity correlated with lower MMSE scores. However, neither TBI severity nor PTSD symptoms were associated with neuroimaging biomarkers of neurodegeneration or vascular damage.
Conclusions
These findings suggest that cognitive impairment in veterans is related to the prior history of TBI and PTSD, but these risk factors may not affect the cognition directly through the accumulation of AD pathologies or vascular injuries. Although these results need further validation by other cohorts who have more recent trauma and wider range of cognitive impairment.
Introduction
Growing evidence suggests traumatic brain injury (TBI) and psychiatric disorders, particularly post-traumatic stress disorder (PTSD), contribute to the complex, multifactorial etiology of dementia and its potential mechanisms of progression. The Lancet Commission on Dementia Prevention, Intervention, and Care has shown TBI as one of the 12 modifiable risk factors using population-attributable fractions. The incidence of TBI shows a relative risk factor of 1.7 as a midlife factor. 1 Based on two meta-analyses involving 53 studies with 16 million participants, male sex and individuals under 65 years of age at the time of TBI were identified as being associated with dementia,2,3 with the incidence of all-cause dementia nearly doubled by moderate to severe TBI history.4–6 Likewise, PTSD following combat has been linked to an increased susceptibility to dementia in later life,7,8 which occurs more frequently in military personnel than in civilians, with rates of 37% versus 16%, particularly as a comorbid condition with TBI. 9 Despite all this evidence, the pathways through which TBI and PTSD may affect brain function or cognition are not truly understood. There are controversial results in the literature on the association between these risk factors and biomarkers in Alzheimer's disease (AD) and non-AD dementia.10–12 Some of these conflicting results might stem from the constraints such as dependence on imprecise diagnostic classifications or removing participants with mild TBI who did not pursue treatment. 13 The variation in exposure-outcome risk estimates between studies can be explained by methodological factors such as different diagnostic criteria for clinically diagnosed dementia compared to biomarkers-based diagnosis and also exposure misclassification. 14 Following TBI, axon severance and swelling, acute upregulation of amyloid-β (Aβ) protein precursor, and subsequent accumulation of Aβ peptide due to transport disruption can occur.15–17 On severe TBI, a study conducted between 4 h and 2.5 years post-injury indicates that 30%-38% of postmortem and surgical tissues exhibit the presence of Aβ plaques.18–20 However, comparable levels of Aβ were observed in a study involving long-term survivors of severe TBI, with durations ranging from 1 to 47 years, 16 indicating a possible threshold for initiating the Aβ cascade and suggesting that Aβ pathology in TBI may not be intrinsically progressive. In addition, hyperphosphorylation of tau in neurodegenerative disorders post-TBI occurs rapidly with the widespread and transcellular progression of tau, which differs from normal aging.21–23
Clinical diagnosis of dementia post trauma is also challenged by disentangling the direct effects of TBI on the neurodegenerative progression or psychiatric impairment.24,25 Nonetheless, the literature lacks consensus, with studies not identifying a correlation between TBI and AD12,26,27 while others claimed the association between the two. 28 Many epidemiologic studies examining this relationship exhibit limitations in evaluating self-reported incidents to ascertain trauma exposure, often providing vague explanations of the connection between trauma and dementia instead of utilizing quantifiable biomarkers and precise terminology.29,30
This study aimed to examine the associations of TBI and PTSD risk factors with cognition in a veteran population, leveraging neuroimaging markers of cognitive decline such as Aβ and tau burden, white matter (WM) integrity and connectivity, and brain vascular health, to identify potential pathways linking these risk factors to neurodegeneration and cognitive decline.
Our central hypothesis was that TBI and PTSD may affect cognition through distinct biological pathways, not necessarily by increasing AD pathology. Accordingly, we first examined the relationships between each risk factor (TBI, combat exposure, and PTSD symptom severity) and cognitive performance independently. Next, we conducted univariate analyses to assess the associations between each risk factor and AD biomarkers (amyloid-β and tau), brain vascular health (quantified using perivascular space (PVS) volume fraction), microstructural integrity (assessed via WM tractography and diffusivity metrics), and functional connectivity, focusing on the default mode network (DMN). Finally, to determine whether the co-presence of multiple risk factors (TBI, combat exposure, and PTSD) increases the likelihood of AD pathology, vascular abnormalities, or white matter disruption, we performed multivariate analyses and regression models evaluating their combined effects.
Methods
ADNI-DOD
Data used in the preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (
The integration of advanced neuroimaging modalities, such as MRI and PET, along with cerebrospinal fluid (CSF) biomarkers and genetic information provides a comprehensive framework for examining brain structure and function. The initial Department of Defense Alzheimer's Disease Neuroimaging Initiative (DOD-ADNI) grant enrolled Vietnam Veterans with PTSD and/or TBI, as well as control participants with other service-related conditions unrelated to PTSD or TBI who demonstrated normal cognition. A subsequent grant expanded the study to include individuals meeting criteria for MCI. The resulting cohorts include Vietnam veterans, with and without MCI, representing groups with TBI, PTSD, combined TBI and PTSD, and controls without either condition. By including participants across the spectrum of normal aging, MCI, and Alzheimer's disease, ADNI-DOD provides a valuable resource for investigating the mechanisms underlying cognitive decline and dementia. ADNI was approved by the Institutional Review Boards (IRBs) of all participating institutions and all participants provided written informed consent.
Study participants
Participants in this study were Vietnam war veterans (n = 289) within an age range of 50–90. Inclusion neurological criteria for individuals with TBI involved a history of moderate to severe non-penetrating TBI related to military service or another trauma and loss of consciousness (LOC), Post-Traumatic Amnesia> >24 h, or alteration of consciousness or mental state> >24 h. Inclusion criteria in the PTSD group required a minimum Clinician Administered PTSD Scale (CAPS) total score equal or higher than 50 points, and no loss of consciousness or, if occurred, LOC <5 min. Exclusion neurological criteria included mild cognitive impairment/dementia, seizure disorder, stroke, unstable medical conditions, or clinically significant neurological/systemic illness; exclusion psychiatric criteria included major psychiatric illness (schizophrenia, bipolar, psychosis), substance abuse within 5 years. Exclusion criteria for the TBI and cognitively normal (CN) arms were a CAPS score of >30 (both current and/or a history of PTSD will be excluded). Exclusion criteria for the PTSD and CN arms were LOC >5 min and any history of head trauma associated with injury onset cognitive complaints. Additional criteria imaging and safety-related included abnormal MRI or lab findings, contraindications to MRI/PET/lumbar puncture, use of exclusionary medications, recent investigational or radiopharmaceutical exposure, prior amyloid-targeting therapy. Excluded medications were anti-coagulant and drugs used to enhance cognition. Centrally acting anticholinergic medications were considered exclusionary, unless approved on a case-by-case basis. Participants unable to safely undergo study procedures were also excluded. Most participants presented a normal level of cognition (n = 231), whereas 58 participants presented cognitive impairment features, either at baseline or developed over time.
Risk factors: TBI and PTSD assessment
TBI severity was calculated by defining a new clinical rating, calculated by summing up scores of the loss of consciousness (LOC) level, amnesia and brain fogginess duration at each traumatic event. We gave a score=1 when the TBI event was< < 5 min; a score of 2 when between 5–9 min; a score of 3 when 10–29 min; a score of 4 when the TBI was between 30 min-24 h; and a score of 5 when the TBI was ≥ 24 h. For each participant, the three component scores were summed for each TBI event, and the event-level scores were then summed across all events to calculate the final TBI severity score for each participant.
Together with the TBI severity score, the total Combat exposure score (CES) 31 was also considered. The CES is a brief self-report tool used to assess the level of combat-related stress experienced by military personnel. It includes 7 items that evaluate the frequency, intensity, and proximity of exposure to combat situations, such as being under enemy fire or witnessing injury and death. A score of 1 indicated no combat experience, a score of 2 indicated being in a combat experience from 1 to 3 times, a score of 3 was from 4 to 12 times, a score of 4 from 13 to 50 times, a score of 5 if they were in a combat experience more than 51 times. Total scores range from 0 to 41, with higher scores indicating greater exposure to combat, which can help in identifying individuals at increased risk for conditions like PTSD. Veterans were asked to indicate whether they had combat experience and the severity of each experience.
To assess the severity and presence of PTSD symptoms, the CAPS total score 32 was used for each participant. It evaluates 20 PTSD symptoms, which are categorized into three clusters: re-experiencing, avoidance, and hyperarousal. The CAPS asks about the frequency and intensity of these symptoms, as well as their impact on daily life. It also includes questions about the individual's trauma history.
Finally, diabetes, hypertension, and history of heart disease were also considered as cerebrovascular disease risk factors.
Cognitive assessment
The clinical assessments used in this study to identify levels of cognitive impairment were the Mini-Mental State Exam (MMSE), 33 Alzheimer's Disease Assessment Scale (ADAS), 34 and Clinical Dementia Rating Sum of boxes (CDR-SOB). 35 Total scores for each test were used to define the level of cognitive impairment for each participant. The ADAS-Cog includes four cognitive areas helpful to determine cognitive impairment: language; memory; praxis; and orientation. The score ranges from 0 to 70, with greater scores indicating more cognitive impairment. The MMSE consists of 30 items, and based on the total score, participants can be defined as having mild dementia (score between 20–24), moderate dementia (a score between 13–20) and severe dementia (score < 12). The CDR-SOB helps monitor dementia progression over time. The scores go through 0.5–2.5: questionable impairment, 3–4: very mild dementia, 4.5–9: mild dementia, 9.5–15.5: moderate dementia and 16–18: severe dementia. 35
Imaging
MR imaging acquisition
Details of MRI, PET, and white matter hyperintensity (WMH) segmentations were previously published. 30 3 Tesla MRI T1-weighted 3D gradient echo sequences with inversion recovery images at screening and month 12 follow-up visits were used to obtain grey matter cortical and subcortical areas segmentation by using Freesurfer 5.1, white matter tracts with diffusion tensor imaging (DTI). The resting state data, and the white matter hyperintensities were acquired by following the protocol that can be found here: https://adni.loni.usc.edu/wp-content/uploads/2013/09/DOD-ADNI-IRB-Approved-Final-protocol-08072012.pdf. Our analysis focused on the functional connectivity resting state measures of the default mode network, which registers the brain activity when no task is performed.
PET imaging
PET images are acquired using the radiotracers 18F-Florbetapir ([18F]AV-45) for Aβ and 18F-Flortaucipir ([18F]AV1451) for tau. Acquisition and analysis details were previously published and followed the ADNI criteria, described here: http://www.adni-info.org/Scientists/ADNIStudyProcedures.aspx. AV1451 and AV45 standardized uptake value ratio (SUVR) used for tau and Aβ measurements respectively, acquired at baseline and 1 year later follow-up.
Imaging processing
Diffusion MRI preprocessing and diffusivity metrics extraction
The diffusion-weighted imaging (DWI) data preprocessing and white matter analysis steps were based on previous work. 36 DWI data were processed using the FSL Diffusion Toolbox, 37 the Advanced Normalization Tools (ANTs; https://stnava.github.io/ANTs/) 38 , and the Quantitative Imaging Toolkit (QIT; http://cabeen.io/qitwiki) 39 .
Initially, a nonlocal means filter was applied to the DWI data using the VolumeFilterNLM module in QIT. 40 This adaptive denoising approach removes high-frequency spatial noise at a single-voxel level while preserving the signal intensities of fine structures, which is particularly important for accurate diffusion metrics in regions with subtle microstructural changes. Subsequently, FSL's eddy tool was used to correct for both eddy current-induced distortions and subject motion, with outlier replacement enabled to mitigate the effects of signal dropout caused by bulk head motion during acquisition. 41 A subject-level quality control assessment was conducted using FSL-eddy_quad 42 to evaluate data quality, including metrics for motion parameters and signal-to-noise ratio; subjects with excessive motion or artifact were flagged for manual inspection.
Brain extraction was performed using FSL BET 43 , and DTI parameters were estimated using weighted-linear least squares estimation implemented in the VolumeTensorFit module of QIT. 44 Parameter maps for DTI metrics (fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD)) were generated and retained for quantitative analysis. 45 For tractography analysis, ball-and-sticks modeling was performed using the Monte Carlo Markov chain approach in FSL BEDPOSTX. 46 For spatial normalization, diffeomorphic registration of subject FA maps to the IIT ICBM diffusion MRI template 47 was performed using ANTs symmetric normalization, 48 and the resulting deformation fields were used to transform atlas-based bundle delineation masks into subject native space for tractography.
White matter tracts analysis
A quantitative tractography analysis was conducted to assess the microstructure of 33 key fiber bundles, covering association, commissural, projection, and cerebellar pathways, with separate analyses for the left and right hemispheres. Using an atlas-based, bundle-specific approach, fiber bundle models were extracted from each participant. Volumetric masks were manually defined for each bundle, including seed, inclusion, exclusion, and stopping regions, based on anatomical references.
To generate subject-specific fiber bundles, we employed a hybrid reinforcement tractography approach 39 with ball-and-sticks voxelwise models and specified parameters: a maximum turning angle of 75°, minimum volume fraction of 0.05, trilinear interpolation, step size of 1 mm, and minimum length of 10 mm.
Bundle-specific DTI metrics were calculated by sampling voxel-wise parameter values at each vertex along the fiber curves and averaging across each bundle to derive the final DTI metrics for statistical analysis. Additionally, each fiber bundle was summarized by its morphometric properties, such as average tract density, volume, mean length, and mean thickness. For each bundle parameter, left and right hemisphere values were averaged, with lateralization analyses performed as secondary analyses.
Perivascular space analysis (PVS)
PVS was segmented using a previously published technique developed in our institute, based on an enhanced PVS contrast. 49 After data acquisition and preprocessing, T1- and T2-weighted images were filtered by using nonlocal mean filtering, used to remove bias intensity of the Rician noise observed in MRI. This was done to remove spatial noise at a single-voxel level and preserve the signal intensities of PVS voxels. Enhanced PVS contrast was obtained by dividing filtered T1w and T2w images. MRI images were parcellated using ANTs to obtain masks of WM and basal ganglia. WM masks were used for PVS analysis. For PVS segmentation, a Frangi filter 50 was applied using QIT, which estimated vesselness measures at different scales and provided the maximum likeliness. The scale was set to a large range of 0.1 to 5 voxels to maximize the vessel inclusion. The output of this step was a quantitative maximum likelihood map of vessels in regions of interest. A threshold was then applied to the vesselness map to obtain a binary mask of PVS regions. A map of total PVS in the white matter was obtained, and the PVS volume fraction was calculated by dividing the PVS volume by the total white matter volume in each participant. Higher PVS volume fraction indicates bigger PVS, i.e., enlargements of PVS.
Statistical analysis
Data distribution was assessed using histograms and D'Agostino's test to evaluate deviations from normality. If a significant departure from normality was detected, Wilcoxon ranking score transformation was applied as a non-parametric approach. 51 Given the high dimensionality of the MRI and clinical features, we avoided individualized variable transformations to prevent overfitting and statistical artifacts. Applying unique mathematical manipulations to each outcome can artificially inflate associations; therefore, we implemented a unified rank-based transformation across all variables. This ensured a consistent and conservative approach to normality while maintaining the integrity of the underlying biological signals. Additionally, comparing the strength of associations across outcomes was difficult due to varying data ranges. To address this and ensure effect size comparability on a consistent scale, the following procedure was implemented: 1) Both outcome and exposure variables were transformed using Wilcoxon ranking scores; 2) all outcome variables (transformed and original) were adjusted for covariates, including age, education, age at TBI injury, history of diabetes, and systolic blood pressure (SBP); 3) correlations were obtained between the residuals of outcome (imaging or clinical outcomes) and exposure variables (TBI, PTSD, and combat exposure). 52 The final dependent and independent variables were standardized to the z-score; thus, associations between exposures and outcomes were approximated to Pearson or Spearman correlation coefficients. A substantial discrepancy between Pearson and Spearman correlations indicated that either the outcome, exposure, or both, violated the normality assumption. Scatter plots of residuals against exposures were examined for potential non-linear associations. The consistent findings between Pearson and Spearman will prove the association is a true phenomenon, and not a byproduct of a specific mathematical calculation. Model integrity was further assessed using an automated outlier detection method based on Cook's distance (d > 0.1). Identified outliers were aggregated for manual inspection. Neurocognitive outcomes included MMSE, CDR-SOB, and ADAS scales. Imaging markers comprised Aβ burden (measured by composite SUVR), tau deposition SUVR in various brain regions, and structural markers such as fractional anisotropy and vascular health indicators like PVS and WMH. Exposure measurements included PTSD severity, TBI, and combat exposure. A multivariate model was used to fit a model with all three combat risk factors. To evaluate the interplay between TBI, PTSD, and combat exposure, we incorporated two-way interaction terms (e.g., TBI*PTSD) into our multivariate models. All variables were treated as continuous to preserve the full distribution of the data and maximize statistical power. To facilitate the quantification and clinical interpretation of these interactions, we calculated predicted point estimates and 95% Confidence Intervals (CIs) for outcomes at the 1st (Q1) and 3rd (Q3) quartiles of each exposure variable, representing “low” and “high” exposure levels, respectively. We specifically examined the joint effects of exposure pairs by reporting predicted cognition and PET marker values across four distinct conditions: High/High, High/Low, Low/High, and Low/Low. The significance of these interactions was assessed using post-hoc contrast tests for the “difference of the difference.” For example, we tested whether the slope of an outcome (e.g., the change in MMSE from Q1 to Q3 TBI exposure) differed significantly depending on the level of PTSD exposure (Q1 versus Q3). The Benjamini-Hochberg procedure was applied to control the false positive rate. A sensitivity analysis was conducted with scanner manufacturer included as a covariate to assess the robustness of the findings. All statistical analyses were conducted using SAS 9.4.
Results
Demographic, clinical, and imaging characteristics
The baseline difference between cognitively normal and people with MCI features is presented in Table 1. We observed statistically significant differences in the CAPS scores (adjusted p < 0.01) between CN and people with cognitive impairment, with higher scores of PTSD in the MCI group. No differences were seen in terms of sex, age, education level, and CVS risk factors between the two groups.
Demographic and cognitive information of participants.
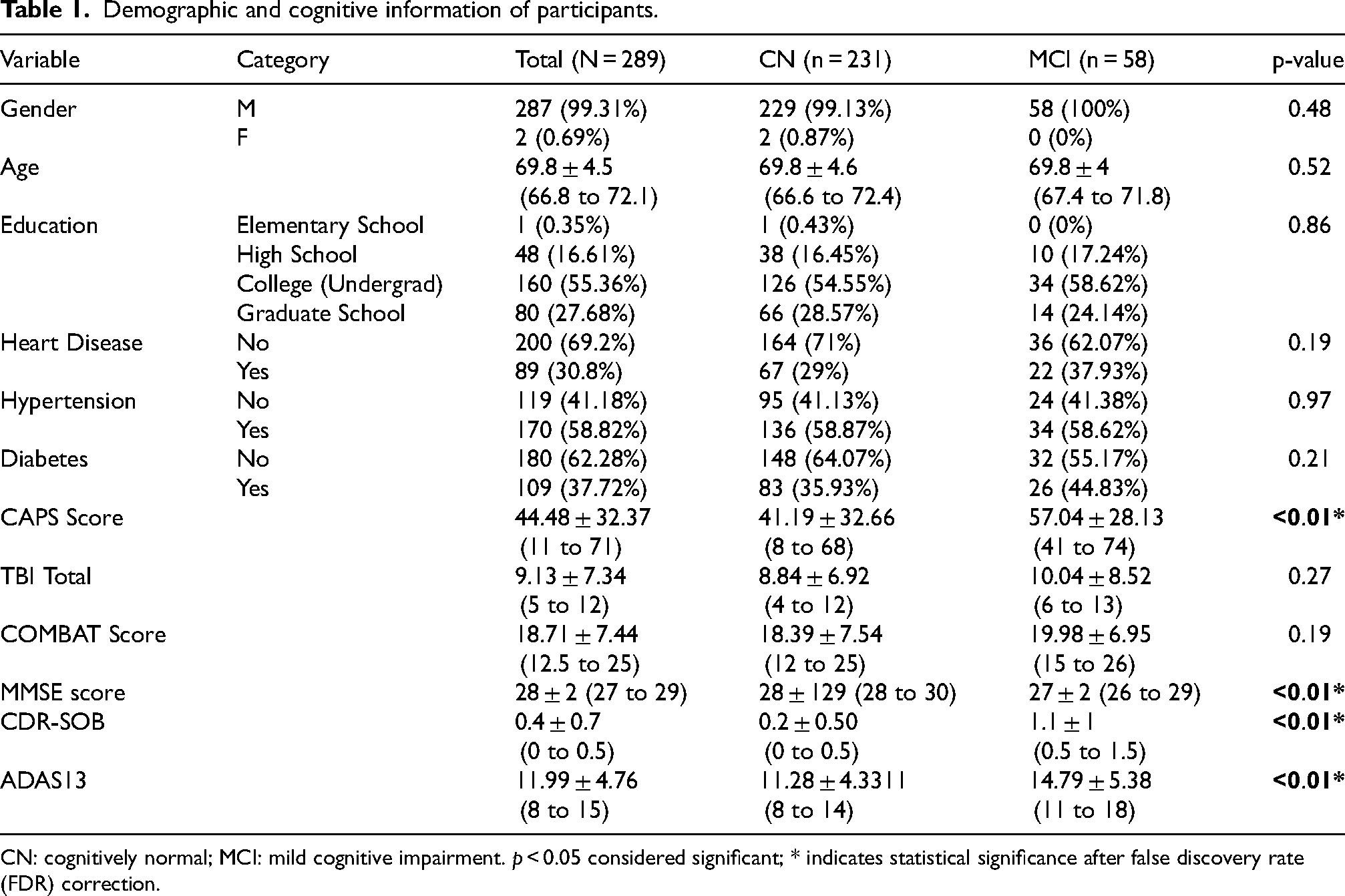
CN: cognitively normal; MCI: mild cognitive impairment. p < 0.05 considered significant; * indicates statistical significance after false discovery rate (FDR) correction.
We did not observe statistically significant differences in TBI severity (p = 0.25) or combat exposure scores (p = 0.20) between the CN and MCI groups in our sample.
In relation to imaging biomarkers, there were statistically significant differences between CN and MCI in PET composite SUVR for Aβ (adjusted p < 0.04), whereas no between-group differences were found in tau SUVR measurements, either in Braak stages (Braak 1–2, Braak 3–4, Braak 5–6, adjusted p = 0.28, p = 0.14, p = 0.08 respectively) or entorhinal and meta-temporal regions (adjusted p = 0.27 and p = 0.5 respectively).
There were no statistically significant differences in perivascular space volume fraction in the basal ganglia (p = 0.25) or white matter (p = 0.09) between CN and MCI groups.
Between-group differences in FA values of specific WM tracts were found, in particular fornix (adjusted p < 0.01), cortical spinal tract (adjusted p < 0.01), right (adjusted p < 0.05) and left (adjusted p < 0.03) superior cerebellar peduncles, and right and left cerebral peduncles (adjusted p < 0.01 for both).
Risk factors and cognition
Correlation analyses based on residual after covariate adjustment were conducted to examine the relationships between risk factors (CAPS score, Combat exposure, and TBI scores) and cognitive performance (ADAS, MMSE, and CDR-SOB scores) in our veteran cohort. All the analyses were corrected for multiple comparisons using the false discovery rate (FDR) correction.
CAPS total scores (indicating PTSD severity) showed statistically significant positive correlations with all cognitive tests including the CDR-SOB (Spearman r = 0.2, p = 0.018 FDR corrected), ADAS (r = 0.28, p = 0.001 FDR corrected) and a negative correlation with the total MMSE score (r = -0.21, p = 0.018 FDR corrected), indicating that higher PTSD symptom severity was associated with worse cognitive performance.
We found that the total TBI score was negatively correlated with MMSE score (r = -0.18, p = 0.027, FDR corrected). Combat exposure showed no statistically significant correlation with any of the cognitive scores (Table 2).
Results of associations between risk factors of PTSD and TBI with cognition, ρ = Spearman's rank correlation coefficient.
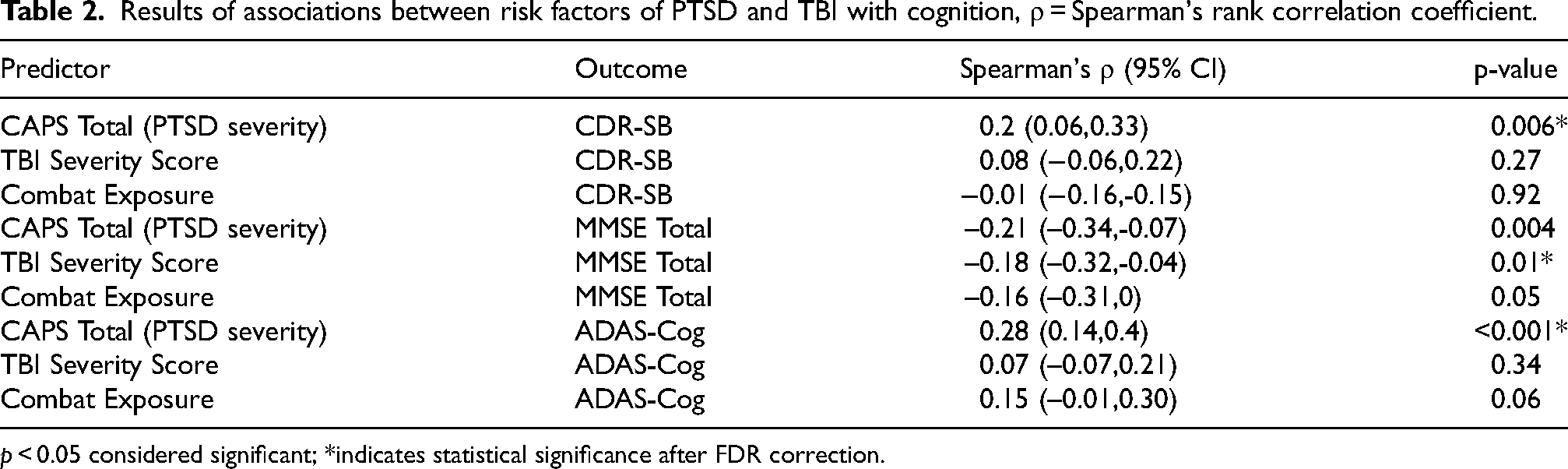
p < 0.05 considered significant; *indicates statistical significance after FDR correction.
Through the interaction test, we further investigated the joint effect of any two risk factors. The point estimates of high (third quartile, Q3) and low (first quartile, Q1) from a pair of variables (or risk factors, e.g., TBI total score + CAPS total score) were obtained by post hoc contrast tests from the model with interaction term. The point estimates for high/high, high/low, low/high, and low/low were used to illustrate the difference of differences. For example, when CAPS score is high (at the level of Q3), the impact of TBI on MMSE score was very minimal, with 28.06 (95% CI: 27.62, 28.51) versus 28.19 (95% CI: 27.74, 28.64) for TBI high (Q3) versus low (Q1), respectively. However, when CAPS score is low (at the level of Q1), the impact of TBI on MMSE score was stronger with 28.42 (95% CI: 27.87, 28.97) versus 29.18 (95% CI: 28.6, 29.76) for TBI high versus low respectively. Such a difference of differences was statistically significant with a p < 0.01 for the interaction test. The interaction effect was even larger after Wilcoxon ranking score transformation.
Risk factors and imaging markers
No statistically significant adjusted correlations were observed between the risk factors (PTSD, TBI, and combat exposure) and the imaging markers, including Aβ and tau PET, DTI, vascular imaging, and rs-fMRI metrics. Specifically, PTSD severity did not show statistically significant associations with Aβ burden or tau neurofibrillary tangles (as assessed by PET-SUVR). Similarly, no associations were found with WM integrity (measured by FA). No statistically significant association found with vascular burden (PVS volume fraction and WMH), or functional connectivity (examined via rs-fMRI of the DMN). Similarly, both TBI and Combat exposure scores showed no statistically significant correlations with these neuroimaging biomarkers (p > 0.05). Results on the relationship between cognition and PET markers are reported in the Supplemental Material.
Cognition and imaging markers of vascular health, functional connectivity, and white matter integrity
Finally, we investigated the relationships between cognitive performance (i.e., MMSE, CDR-SOB, and ADAS) and other imaging markers, specifically PVS and WMH for vascular health, rs-fMRI of DMN for brain connectivity, and FA for white matter integrity. We found no statistically significant associations between cognitive performance and any of the imaging markers of vascular health and brain function. Statistically significant associations were seen between ADAS and FA in the fornix (p < 0.01), the FA in the left cerebral peduncle and CDR-SOB (p < 0.05), and ADAS (p < 0.05). Such results did not survive FDR correction for multiple comparisons. Results were unchanged and the main findings remained consistent after accounting for scanner manufacturer.
Discussion
Our evaluation of the ADNI-DOD population imaging and clinical data showed significant associations between the risk factors, PTSD, and TBI, with the cognition performance. Worse cognitive function in people with higher PTSD symptoms and more severe TBI experiences was observed. As expected, we found that Aβ and tau were associated with cognitive scores, in particular CDR-SOB, ADAS and MMSE. However, there were no direct associations between factors such as TBI severity, level of combat exposure, and PTSD severity, with accumulation of the AD pathologies (i.e., Aβ and tau in the brain) in this dataset.
There was no association between any of the imaging vascular biomarkers or imaging structural or functional connectivity markers and cognitive functions. In addition, the severity of TBI, combat exposure, or PTSD did not correlate with any of the imaging vascular and structural or functional connectivity measures.
In our cohort of aging veterans composed mostly of cognitively normal individuals, we found PTSD symptom severity was associated with CDR-SOB, MMSE and the ADAS-Cog, while higher TBI severity only correlated with lower MMSE scores. This suggests PTSD might have a more detectable or profound effect on cognition compared to TBI in our dataset, where cases with cognitive impairment were initially excluded. This aligns with epidemiological evidence showing that PTSD alone and even more than TBI are risk factors for cognitive decline and progression to dementia among veterans. For example, a large longitudinal study of U.S. veterans demonstrated that PTSD increases the risk of dementia by nearly twofold, 8 while TBI has been associated with an approximately 60% increased risk of dementia diagnosis. 53 Such findings underscore the clinical relevance of trauma exposure in shaping cognitive trajectories during aging. The pathophysiological mechanisms underlying the associations between trauma-related risk factors and cognition are not completely understood. It may involve long-term neurobiological alterations such as low-grade neuroinflammation, disrupted neural connectivity, and diffuse microstructural injury, processes that can impair cognitive function without necessarily producing clear metabolic or diffusion abnormalities detectable by conventional MRI, rsfMRI, DTI, or PET.54,55
The results considering the interaction between TBI severity and PTSD symptoms showed a significant combined impact on cognitive performance, as reflected by MMSE scores. The effect of TBI on cognition depends on how severe the PTSD symptoms are. When PTSD symptoms and scores were high, it would hamper the effect of TBI on cognitive performance levels, while in cases of mild PTSD symptoms, those with more severe TBI showed lower MMSE scores. This means that TBI has a stronger impact on cognition when PTSD symptoms are mild, but when PTSD symptoms are already severe, they may mask the effects of TBI. Another consideration is that because PTSD symptoms commonly emerge following more severe injuries, these conditions may not be entirely independent, limiting the ability to detect their separate effects.
Among veterans, many of whom have complex medical and psychological histories, early Aβ accumulation could reduce cognitive reserve or interact with other brain vulnerabilities related to trauma, aging, or vascular burden. 56 Although the retrospective nature of the study limits causal inference, the associations of PTSD score and TBI severity with cognitive measures suggest that trauma-related experiences may contribute to cognitive vulnerability over time.8,53 This highlights the potential utility of incorporating trauma history into research frameworks and monitoring protocols in aging cohorts. Future prospective studies that examine whether early identification of trauma-related symptoms, such as post-concussive symptoms and PTSD, can help reduce the risk of progressive cognitive decline in trauma-exposed populations. 55
In this retrospective analysis, we investigated the relationships between key risk factors associated with military trauma and neuroimaging markers comprising WMH, PVS, rsfMRI, FA, and PET amyloid and tau. Despite prior literature suggesting that trauma-related exposures and PTSD can impact brain structure and function, 57 our findings indicate that, in this sample, exposure to TBI and combat stress earlier in life was not associated with increased Aβ or tau deposition, white matter microstructural damage, cerebrovascular pathology, or alterations in resting-state functional connectivity in later life. A potential explanation for the lack of association between trauma-related factors (TBI and PTSD) and amyloid and tau accumulation in this cohort might be survival bias given the substantial time lag between exposure to these risk factors and the collection of imaging biomarkers. Prior work has suggested that individuals with similar trauma histories may differ widely in neurobiological outcomes due to factors such as cognitive reserve, genetic predispositions, lifestyle factors, and effective neuroplastic compensatory mechanisms. 58 Such adaptive reorganization may mitigate the downstream effects of trauma on amyloid and tau deposition, reflecting a form of neural resilience that could mask direct associations between TBI severity and AD pathology and resulting in minimal detectable changes on vascular, connectivity or microstructural imaging measures.
Another consideration is that certain risk factors, such as TBI and PTSD, may influence the brain through pathways that are at least partly independent of classical AD pathology. AD is generally understood as being driven by Aβ and tau deposition, but TBI and PTSD may operate in parallel, triggering different biological processes that affect cognition and brain health without necessarily producing the hallmark AD changes, and engaging a second neural pathway. It is important to note that tau measurements in this cohort reflected AD-related tauopathy and did not capture other forms of tau pathology. Null results should be interpreted within the context of cohort-specific and methodological considerations. The neurobiological substrates implicated in trauma and stress-related disorders often involve limbic and paralimbic regions, and other components of the salience and fear circuitry. 59 These circuits are critically involved in emotional regulation and stress responses. Cognitive decline is predominantly associated with progressive pathology in medial temporal lobe structures (e.g., hippocampus, entorhinal cortex), posterior cortical regions, and functional networks such as the DMN. 60 Although there is some overlap, the distinct patterns of vulnerability may result in trauma-related risk factors not being strongly reflected in imaging markers primarily designed or sensitive to AD-related neurodegeneration or global cognitive impairment.
Methodological considerations inherent to retrospective analyses likely also contributed to our results. The ADNI-DOD population predominantly consists of older adults who are mostly cognitively normal, which can lead to a selection bias and limit the ability to detect associations that may be evident in individuals with more advanced cognitive impairment state. The timing between trauma exposure, PTSD onset, and neuroimaging acquisition complicates the detection of meaningful brain changes. The neural sequelae of TBI and PTSD may evolve dynamically over time, with initial alterations potentially stabilizing, recovering, or progressing in non-linear fashions. This variability in the trajectory of trauma-related brain changes poses a challenge for detecting consistent neurobiological patterns. Our data demonstrated substantial temporal heterogeneity in TBI events, which may have hindered the detection of associations with imaging biomarkers at the time of data acquisition. By the time imaging is conducted, some individuals may have undergone partial recovery or compensatory adaptation, while others may still be experiencing evolving alterations, resulting in heterogeneous imaging profiles that do not consistently align with clinical symptomatology or trauma exposure history. 61
Another important factor is the heterogeneity of trauma exposures and clinical presentations within the ADNI-DOD sample. Variability in TBI severity, timing, frequency, combat-related stressors, and PTSD symptom profiles introduces substantial noise that can obscure clear associations. Similarly, combat exposure and PTSD symptoms present with diverse intensities, symptom clusters, and durations, further complicating attempts to link these experiences with specific neural changes. Furthermore, resilience factors likely modulate brain outcomes and contribute to heterogeneity. 62 Such protective mechanisms may attenuate the neural features typically associated with TBI or PTSD, making it more difficult to detect group-level associations, particularly in individuals who retain cognitive function despite a history of trauma.
A central limitation of this study lies in the lack of detailed temporal information and contextual specificity regarding participants’ histories of TBI. While we accounted for TBI severity based on available records, many individuals in the ADNI-DOD cohort experienced one or more TBIs prior to study enrollment, sometimes by many years or even decades. The study population may be influenced by survival bias, as veterans with greater resilience to long-term effects of trauma may have been more likely to survive and participate, potentially leading to underrepresentation of individuals with more severe outcomes. Another limitation is a selection bias in our cohort due to the exclusion of participants with significant psychiatric or cognitive impairment, which may limit generalizability to more severely affected populations. Finally, the long interval between traumatic exposure and neuroimaging assessment may have reduced the ability to detect trauma-related effects due to recovery, compensation, or age-related changes over time. Therefore, the absence of significant associations in this study may, at least in part, be driven by these limitations, rather than indicating a true lack of long-term neural consequences of trauma. A key novelty of this study is the use of a new, cumulative TBI severity score that captures the total burden of brain injuries across a person's lifetime. By combining symptoms of LOC, amnesia, and brain fog from each injury, this score goes beyond traditional methods that often focus on a single event or measure. This allows for a more detailed and accurate assessment of how repeated TBIs might affect the brain over time. Using this approach improves our ability to identify subtle links between trauma history and brain changes, especially in groups where cognition is largely preserved. Overall, this new scoring system provides a valuable tool for studying the long-term effects of TBI in aging and neurodegenerative populations. Other TBI severity scoring criteria have been proposed with 4 pillars: a clinical pillar (full Glasgow Coma Scale and pupillary reactivity); a biomarker pillar (blood-based measures); an imaging pillar (pathoanatomical measures); and a modifier pillar (features influencing clinical presentation and outcome; CBI-M) 63 ; however, we do not have all those data in our cohort.
Given the extensive exploratory analyses conducted and the subsequent application of the Benjamini-Hochberg procedure to control the false discovery rate (FDR), the study may be subject to reduced statistical power. However, robust effect sizes remain detectable even under a penalized α. Specifically, for a conservative α of 0.01, our sample size is sufficient to achieve 80% power to detect a correlation coefficient of r ≥ 0.20. If the penalized α is further restricted to 0.002, 80% power is maintained for effect sizes of r ≥ 0.23. These calculations suggest that while the threshold for significance is high, the study remains well-powered to identify clinically meaningful associations.
In summary, greater TBI and PTSD severity were associated with poorer cognitive performance, which in turn correlated with cerebral Aβ and tau burden. However, after accounting for study limitations, we did not identify clear or statistically significant associations between TBI or PTSD severity and AD-related imaging biomarkers, including Aβ and tau PET, diffusion, functional connectivity, white matter hyperintensities, or dilated perivascular spaces. These findings suggest that the mechanisms underlying cognitive decline in individuals with TBI and PTSD remain incompletely understood.
This study underscores the challenges of assessing the long-term neural consequences of traumatic brain injury in aging populations. While the use of a cumulative TBI severity score and multimodal neuroimaging represents an important step toward capturing the complexity of repeated trauma, factors such as injury timing, survivor and selection biases, and relative cognitive preservation may have limited the ability to detect associations with AD biomarkers. Future studies incorporating longitudinal designs, trauma-specific biomarkers, and broader clinical spectra will be critical for clarifying how TBI and PTSD influence brain health across the life course and for refining their potential role in neurodegenerative processes.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261450973 - Supplemental material for Traumatic brain injury and post-traumatic stress disorder on brain imaging markers and cognition in a war veterans population
Supplemental material, sj-docx-1-alz-10.1177_13872877261450973 for Traumatic brain injury and post-traumatic stress disorder on brain imaging markers and cognition in a war veterans population by Francesca Sibilia, Maryam Fotouhi, Xiaomeng Lei, Ryan P. Cabeen, Steven Cen, Jeiran Choupan, Saman Hazany, Nasim Sheikh-Bahaei and in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Data collection and sharing for this project was funded by the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: Alzheimer's Association; Alzheimer's Drug Discovery Foundation; BioClinica, Inc.; Biogen Idec Inc.; Bristol-Myers Squibb Company; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; GE Healthcare; Innogenetics, N.V.; IXICO Ltd; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Medpace, Inc.; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Synarc Inc.; and Takeda Pharmaceutical Company. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Disease Cooperative Study at the University of California, San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. This research was also supported by NIH grants P30 AG010129 and K01 AG030514.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Disease Cooperative Study at the University of California, San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. This research was also supported by NIH grants P30 AG010129 and K01 AG030514.
Ethical considerations
As per ADNI protocols, all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. More details can be found at adni.loni.usc.edu.
Consent to participate
All ADNI and ADNI-DOD participants provided written informed consent at the time of enrollment for data collection and sharing. The consent process and study protocols were overseen by the Institutional Review Boards of each participating site.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Defense Grants: Effects of Traumatic Brain Injury (TBI) and Post-Traumatic Stress Disorder (PTSD) on Alzheimer's Disease (AD) in Veterans Using Imaging and Biomarkers in the (AD) Neuroimaging Initiative (ADNI), W81XWH-12-2-0012. Effects of Traumatic Brain Injury and Post-Traumatic Stress Disorder on Alzheimer's Disease (AD) in Veterans with Mild Cognitive Impairment (MCI) Using the Alzheimer's Disease Neuroimaging Initiative (ADNI), W81XWH-13-1-0259. Effects of Traumatic Brain Injury and Post-Traumatic Stress Disorder and Alzheimer's Disease on Brain Tau in Vietnam Veterans Using ADNI, W81XWH-14-1-0462.
Perivascular segmentation and diffusion metrics analyses were supported by the NIH grant R01NS100973_NINDS, awarded to Dr. Andrei Irimia.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The perivascular space mapping technology is part of a patent number US11908131B2 owned by JC. JC declares status as employee of the private company NeuroScope Inc (NY, USA). All other authors declare no financial or non-financial competing interests.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.