
Abstract
Background
The influence of lifestyle factors on cognitive health, particularly among middle-aged and older adults, has garnered significant attention in gerontology and cognitive neuroscience. Currently, over 55 million people worldwide are living with dementia, including Alzheimer's disease with nearly 10 million new cases annually. Although sedentary behavior has been associated with cognitive decline, these studies often treat sitting time as a homogeneous entity, without considering the specific nature of sedentary activities.
Objective
This systematic review aims to examine associations of individual sitting activities with cognitive function in middle-aged and older adults.
Methods
Data were searched using eight electronic databases (EMBASE, Web of Science, PsycINFO, CINAHL, Medline, SPORTDiscus, PubMed, and Scopus) from inception to September 2024. Qualitative studies, reviews, conference abstracts, theses, and book chapters were excluded. The methodological quality of included studies was assessed using the QualSyst tool.
Results
A total of 85 studies (n = 1,575,657) were included in this review. Of the 43 studies examining television viewing, 28 (65%) reported a negative association between prolonged television viewing and cognitive function. Conversely, among the 58 studies that included active sedentary activities, only five (8.6%) reported negative associations.
Conclusions
The cognitive effects of sedentary behavior depend on the type of activity performed. Promoting cognitively engaging sedentary activities may support healthy cognitive aging, while excessive passive behaviors may increase risk of cognitive decline and Alzheimer's disease. Future research should focus on further clarifying the mechanisms behind these associations and explore interventions to enhance cognitive health in aging populations.
Introduction
The global population is aging, such that by 2050, there will be 426 million people aged 80 years or older. 1 With this global aging population, cognitive health, particularly among middle-aged and older adults, has attracted growing interest in gerontology, cognitive neuroscience, and public health. Cognitive functioning encompasses the mental processes involved in acquiring knowledge and understanding, including several domains such as attention, language, executive functioning, learning, memory, intelligence quotient, and visuospatial abilities, essential for performing daily tasks and maintaining independence. 2 Cognitive abilities often exhibit a decline with aging. Declines in cognition beyond that due to aging may result in dementia. Dementia is an umbrella term that encompasses several conditions, with Alzheimer's disease (AD) being the most common. Dementia is characterized by a loss of cognitive functions such as thinking, remembering, and reasoning, 3 such that it impairs daily life. Although dementia is not a normal part of aging, the risk of developing it significantly increases with age. 3
Currently, more than 55 million people worldwide are living with dementia, with nearly 10 million new cases each year. 4 Dementia is the seventh leading cause of death globally and one of the leading causes of disability and dependency among older people worldwide. 5 The impact of dementia extends beyond individuals, affecting families and healthcare systems. In 2019, the global economic cost of dementia was estimated at US $1313.4 billion, involving 55.2 million individuals, equating to US $23,796 per person with dementia. 6 There is currently no cure for dementia, 6 making it critical to identify modifiable risk factors that can help prevent or delay cognitive decline and the onset of dementia. Several risk factors have been associated with the development of dementia. The 2024 Lancet Commission on dementia prevention, intervention, and care report has highlighted that approximately 45% of dementia cases can be prevented by targeting 14 modifiable risk factors throughout different life stages. 7 The early life stage factor is lower level of education (5%). The midlife stage factors are hearing loss (7%), elevated HDL cholesterol (7%), depression (3%), traumatic brain injury (3%), lack of physical activity (2%), diabetes (2%), smoking (2%), hypertension (2%), obesity (1%), and excessive alcohol consumption (1%). The late life stage factors are social isolation (5%), exposure to air pollution (3%), and untreated vision problems (2%). 7 Fifty-five percent of cases remain unclear, suggesting the need to investigate other risk factors.
In recent years, increasing time spent sedentary in mid-aged and older adults, has emerged as a crucial predictor of healthy aging.8–10 Sedentary time is defined as waking activities, while sitting or lying, with an energy expenditure of 1.5 metabolic equivalent tasks (MET) or less, such as watching television, working at a desk, and using a computer. 11 Researchers can investigate the impact of both total sedentary time and specific types of sedentary activities to better understand their associations with various health outcomes. Sedentary time is highly prevalent among older adults and tends to increase with age, often exacerbated by comorbidities and cognitive decline. 12 A meta-analysis involving 349,698 adults aged 60 years and older, encompassing 22 studies (10 national and one EU-wide), reported that older adults spend an average of 9.4 h per day in sedentary activities, accounting for 65–80% of their waking hours. 13
Numerous studies have established a link between sedentary activities and heightened rates of all-cause mortality, cardiovascular mortality, cancer mortality, and type 2 diabetes mellitus in older populations.14,15 However, the association between sedentary activities and cognitive function remains unclear. Recent studies have shown that prolonged sedentary activities, particularly passive ones like watching television, are linked to faster cognitive decline and poorer performance in global cognition, immediate memory, and verbal fluency,12,16,17 while positive impacts on processing speed and executive function have also been observed in reading and playing card games.18,19 Therefore, it is critical to consider the quality and context of these activities, as the impact of sedentary activities on cognitive health may vary depending on the nature of the activity.
Previous systematic reviews have often aggregated all forms of sedentary activities, potentially obscuring the distinct effects of specific activities health outcomes. Dillon et al. (2020)'s meta-analysis of 23 studies found that overall, total sedentary time had no significant association with cognitive function, while subgroup analyses showed that device-measured sedentary time had a significant negative association with cognitive function and self-reported sedentary time showed a positive association. 20 Olanrewaju et al. (2020) reviewed 18 studies and found mixed results in that some studies reported associations between higher sitting time and poorer cognitive outcomes, while others reported no significant association. 10 Copeland et al. (2017) suggested that cognitively engaging sedentary activities may benefit cognition function, while more passive activities could be detrimental. 21 Sedentary activities vary significantly in terms of cognitive engagement and an emerging body of research that have examined the impact of so called active and passive sedentary activities on depression. 22 Research suggests that activities requiring active thinking, problem-solving, and continuous learning can build cognitive reserve, thereby mitigating cognitive decline. For instance, a longitudinal study of a 1946 British birth cohort found that individuals with higher cognitive reserve, measured by educational attainment, occupational complexity, and social and leisure activity participation, performed better on cognitive tests at age 69. 23
Conversely, passive activities, particularly prolonged television viewing, have been linked to cognitive decline. A cross-sectional study by Guillot et al. (2012) demonstrated that regular computer use potentially helps to preserve cognitive function in older adults compared to television viewing. 24 The Wingood study on cognitively active versus passive sedentary activities in older adults found that cognitively demanding activities were associated with better performance in memory and executive function than passive activities. 25 Similarly, a longitudinal survey of healthy longevity in China found that playing card games or engaging in group activities provided social stimulation, reducing the risk of social isolation and its associated cognitive risks. 19 Additionally, earlier reviews have highlighted significant heterogeneity in study designs, including varying measures of sedentary behavior and cognitive outcomes. This variability can lead to inconsistent findings, complicating the ability to draw definitive conclusions about the relationship between sedentary activities and cognitive function. For example, a current systematic review and meta-analysis reported a weak association between total sedentary time and cognitive function and varied depending on the sedentary activities measure and the cognitive domain assessed. 20 Specifically, device-based measures of sedentary time showed a negative association with cognitive function, particularly with global cognitive function and processing speed, while self-reported measures showed a positive association with cognitive function, notably with processing speed. 20 Furthermore, previous reviews have generally not distinguished between the cognitive domains affected by sedentary behavior, as different sedentary activities may influence cognitive functions such as memory, executive function, or attention in diverse ways.
This study aimed to conduct a systematic review to describe the associations between individual sedentary activities and cognitive function in middle-aged and older adults. A key aim was to examine the relationships between various sedentary behaviors and different cognitive domains, such as executive function and memory. Specifically, we aim to determine whether differences exist in the relationship between active sedentary behaviors (e.g., reading or using a computer) and passive sedentary behaviors (e.g., watching television) in relation to cognitive performance.
Methods
The protocol for this systematic review is pre-registered with Prospero International Prospective Register of Systematic Reviews (registration number: CRD42018082384) - https://www.crd.york.ac.uk/prospero/display_record.php?ID = CRD42018082384). The present systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines. The PRISMA Checklist is displayed in Supplemental Table 1.
Search strategy
We comprehensively searched the following electronic databases from inception to September 2024: EMBASE, Web of Science, PsycINFO, CINAHL, Medline, SPORTDiscus, PubMed, and Scopus. The final search strategy and selection of search terms for each database were collaboratively determined by all contributing authors and encompassed three key dimensions: participants (i.e., middle-aged, and older adults), exposure (i.e., individual sedentary activities), and outcome of interest (i.e., cognitive function or cognitive status, e.g., dementia). Searches were conducted using search terms and free-text terms. Each database search was tailored to account for specific database requirements (see Supplemental Table 2 for detailed search strategies). We also included references identified through manual searches in the study team's libraries. The initial search was conducted in February 2024, with additional search and review of sources conducted in September 2024.
Types of participants
This review specifically focused on middle-aged and older adults, thus only studies with a population mean age of 40 years or older were included, with age referring to the timepoint at which participants were assessed for the analysis. Studies from all countries were considered. Studies including both healthy individuals and those with pre-existing conditions, such as mild cognitive impairment, were eligible for inclusion.
Types of exposure
The exposure of interest in this review is defined as time spent in individual sedentary activities, including watching television, reading, games and puzzles, driving, and using computer. Although one element of sedentary activity is defined by posture, i.e., sitting or lying, and with a low energy expenditure, 11 we included activities commonly deemed as sedentary even if posture or energy expenditure was not explicitly assessed. Sedentary activities are also classified into mental active sedentary activities (e.g., computer use, reading, driving, and playing games) and mentally passive sedentary activities (e.g., watching television). In this study, television viewing is the only sedentary behavior categorized as mentally passive, as it is typically associated with low cognitive engagement. 22 Other activities, such as reading, computer use, or playing games, are considered mentally active due to their higher cognitive demands. 22 In this review, different card games (poker games and mahjong) and puzzles are grouped together because while the specific content may vary, the cognitive engagement required for these activities is fundamentally similar, all involving problem-solving, memory, and strategic thinking, regardless of the exact nature of the game or puzzle. This is comparable to how people watch different types of content on TV—whether it's news, a movie, or a documentary—they are still engaging in the same passive activity of watching television. Measurement of these activities typically relies on self-report questionnaires or diaries, wherein participants document the duration and frequency of each activity. Studies were included in this review if they specifically reported the time spent on individual sedentary activities, such as the number of hours spent watching television, reading, games and puzzles, driving, or using a computer, either on a daily or weekly basis. Similarly, studies that reported the frequency of these activities (e.g., how often participants engaged in each sedentary activity) were also included. Therefore, any reference to ‘sedentary activities’ in this review refers to distinct and specific sedentary activities, unless otherwise specified.
Importantly, this review excluded studies that focused on cognitive training programs as part of sedentary behavior because such interventions have been reviewed in prior meta-analyses.26–28 The exclusion is based on the distinction between every day, non-structured sedentary activities, and structured, goal-oriented cognitive training, which aims to improve cognitive function directly. As our objective is to explore the effects of passive and mentally active sedentary activities on cognitive function in natural settings, studies that involved cognitive training programs were not suitable for this review. Studies that include composite measures of sedentary activities, combining multiple activities into a single exposure, were excluded because they do not allow for the isolation of the effects of individual sedentary activities on cognitive function, which is essential for the objectives of this review. Additionally, studies that reported only total sitting time or lack of physical activity, without distinguishing between specific sedentary activities, were excluded.
Types of outcome measure
Only studies that assessed cognitive function and/or cognitive impairment/decline (e.g., dementia or mild cognitive impairment [MCI]) were included. The cognitive outcomes were required to be assessed using recognized methods or standardized cognitive tests to ensure consistency and reliability across studies. Each study's cognitive outcomes were categorized according to the authors’ reported assessments of different cognitive domains. These cognitive domains were classified into one or more of the following domains: (1) processing speed, (2) episodic memory, (3) global cognitive function, (4) motor skills and construction, (5) executive function, (6) cognitive flexibility, and (7) working memory. For definitions of each cognitive domain and the acceptable cognitive tests, please refer to Supplemental Table 3. For inclusion, studies had to clearly specify the cognitive domain(s) they assessed, and the assessment tools had to be recognized in the literature as valid and reliable measures for those specific domains. Studies were excluded if they measured cognitive function as defined by brain volume or cerebral blood flow using magnetic resonance imaging (MRI) or if they provided only subjective self-reported assessments of cognitive functioning without any formal testing. In this systematic review, dementia and cognitive impairment were measured and categorized using standard clinical definitions and diagnostic tools. Dementia is classified as a significant decline in cognitive function that interferes with daily living, with AD representing a major subcategory. Cognitive impairment encompasses a broader spectrum of difficulties in thinking, learning, memory, judgment, and decision-making. This category includes subtypes such as MCI, subjective cognitive impairment, and cognitive complaints. For detailed definitions of dementia and cognitive impairment and the measurements, please refer to Supplemental Table 4.
Study selection
In addition to the aforementioned criteria, additional inclusion criteria for this analysis were studies that were (1) published in any year; (2) available in English language. The exclusion criteria include discussion articles, conference proceedings, book chapters, theses, or commentaries not presenting empirical research in a peer-reviewed journal. Two authors independently screened the titles and abstracts of the identified studies using the Covidence systematic review software, excluding studies that did not meet the inclusion criteria. Both authors then independently assessed the full texts to further identify studies that did not meet the criteria. At each stage of the screening process, any discrepancies between the authors were discussed, and consensus was reached to ensure consistency in selecting eligible studies. All additional articles identified through these alternative sources were evaluated using the same eligibility criteria and screening process as those retrieved from the electronic database searches.
Data extraction
Data extraction was conducted by one review author, with a second author verifying the accuracy of the extracted data on 10% of included studies. The extracted data are presented in a series of tables, each addressing specific aspects of the studies included in the review. Table 1 provides a summary of the general characteristics of the selected studies, including (1) the author and publication year, (2) the country where the study was conducted, (3) the study design, (4) sample size, (5) mean age of participants, and (6) the percentage of female participants. Tables 2, 3, 4, 5, and 6 focus on the relationship between passive and active sedentary activities and cognitive function separately, including: (1) the types of passive or active sedentary activities examined, (2) how these activities were measured, (3) the cognitive domains assessed, (4) the tools used to measure cognitive function, (5) the covariates included in the analysis, and (6) the main results of each study. Finally, Tables 7 and 8 summarize the findings from studies that investigated associations of sedentary activities with dementia and cognitive impairment. Additional information extracted but not included for reporting in Tables 1–8 included: (1) study objectives, (2) recruitment sources and methods, (3) inclusion and exclusion criteria, (4) data types for exposure and outcome variables, (5) statistical methods, (6) study conclusions, (7) limitations identified by the authors, and (8) disclosure of conflicts of interest.
Characteristics of included studies.
CS: Cross-Sectional; HIV: Human Immunodeficiency; LO: Longitudinal Observational; MCI: Mild Cognitive Impairment; N: Number.
Summary of association between watching television with cognitive function.
ADL: activities of daily living; BDI: Beck Depression Inventory; BMI: body mass index; B: beta-coefficient; β: standard beta-coefficient; CERAD: Consortium to Establish a Registry for Alzheimer's Disease; CES-D: Center for Epidemiologic Studies Depression; CI: confidence interval; CSI-D: Community Screening Instrument for Dementia; F: F-distribution; h/d hour/day; IADL: instrumental activities of daily living; LSI: Lifestyles Inventory; MET: Metabolic Equivalent of Task; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; OR: odds ratio; PA: physical activity; r: correlation coefficient; SE: standard error
*All the sedentary activities are measured by self-report.
Summary of association between reading with cognitive function.
ADL: activities of daily living; B: beta-coefficient; BDI: Beck Depression Inventory; BMI: body mass index; β: standard beta-coefficient; CES-D: Center for Epidemiologic Studies Depression Scale; CI: confidence interval; HR: hazard ratio; IADL: instrumental activities of daily living; MET: Metabolic Equivalent of Task; MMSE: Mini-Mental State Examination; OR: odds ratio; SD: standard deviation; SE: standard error; z: standard score
*All the sedentary activities are measured by self-report.
Summary of association between computer use with cognitive function.
ADL: activities of daily living; BDI: Beck's Depression Inventory; BMI: body mass index; B: beta-coefficient; CES-D: Center for Epidemiologic Studies Depression; CI: confidence interval; CDT: Center for Doctoral Training; FDR: false discovery rate; F: F-distribution; HR: hazard ratio; ICD-9: International Classification of disease 10th Revision; IADL: instrumental activities of daily living; MET: Metabolic Equivalent of Task; MMSE: Mini-Mental State Examination; M: mean; OR: odds ratio; r: correlation coefficient; SD: standard deviation; SES: socioeconomic status; TMT: Trail Making Test; z: standard score
*All the sedentary activities are measured by self-report, except one was measured by monitoring software. 32
Summary of association between playing games and puzzles with cognitive function.
ADL: activities of daily living; B: beta-coefficient; CI: confidence interval; HR: hazard ratio; IADL: instrumental activities of daily living; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; OR: odds ratio; SD: standard deviation; SE: standard error; TMT: Trail Making Test; WM: working memory; WMC: working memory capacity; z: standard score.
*All the sedentary activities are measured by self-report.
Summary of association between driving with cognitive function.
BMI: body mass index; B: beta-coefficient; CI: confidence interval; IADLs: instrumental activities of daily living; OR: odds ratio; SES: socioeconomic status
*All the sedentary activities are measured by self-report.
Summary of association between individual sedentary activities with dementia.
APOE: Apolipoprotein E; BMI: body mass index; RR: relative ratio; CERAD: Consortium to Establish a Registry for Alzheimer’s Disease; CSI-D: Community Screening Instrument for Dementia; CI: confidence interval; HR: hazard ratio; OR: odds ratio
*All sedentary activities are measured by self-report.
Summary of association between individual sedentary activities with cognitive impairment.
ADL: activities of daily living; APOE: Apolipoprotein E; CDR: Clinical Dementia Rating; CI: confidence interval; CSI-D: Community Screening Instrument for Dementia; HR: hazard ratio; MCI: mild cognitive impairment; MMSE, Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; OR: odds ratio
*All sedentary activities are measured by self-report.
Quality assessment
One reviewer independently evaluated the quality of each study using the QualSyst checklist developed by Maddocks et al. 29 with a second author cross-checking the accuracy of the quality assessment for 10% of the included studies. The QualSyst checklist was chosen because it is applicable to both observational and experimental studies, making it a suitable tool for assessing the diverse study designs included in this review. Each study was assessed on 14 criteria, with scores ranging from 0 (no) to 1 (partial) and 2 (yes). The total score for each study was then normalized by dividing it by the highest possible score. Any discrepancies between reviewers were resolved through discussion to ensure consensus. A QualSyst score of 80% or higher indicated strong quality, scores between 60% and 79% were deemed good quality, scores between 50% and 59% were rated as adequate quality, and scores of 50% or lower were classified as poor quality.
Data synthesis analysis
All relevant studies reporting on individual sedentary activities and cognitive functioning were synthesized into three pinwheels based on their sedentary activity types and cognition types. Pinwheels were used as a visual representation to effectively organize and present the data, allowing for a clearer comparison of findings across different study designs and cognitive domains. Additionally, this approach facilitated the identification of research gaps by highlighting areas where evidence is limited or inconsistent. The first pinwheel represents passive sedentary activities, such as watching television (see Figure 1), and the second one representing active sedentary activities, including reading, games and puzzles, driving, and using computer (see Figure 2). Within the first two pinwheels, studies were further categorized based on their research design (cross-sectional, longitudinal studies, and case-controlled studies). Positive and negative effects were also highlighted on the pinwheels to indicate the direction of the relationship. A positive effect on the pinwheel indicates that a particular sedentary activity is associated with improvements in a cognitive domain (e.g., more reading increasing episodic memory), while a negative effect reflects a decline in cognitive function associated with that activity (e.g., more television viewing decreasing attention). Additionally, we also synthesized studies exploring the relationship between different sedentary activities and cognitive disorders in pinwheel 3, including dementia and cognitive impairment (see Figure 3). In this cognitive disorder-specific pinwheel, a positive health outcome indicates that engaging in more of a particular sedentary activity is associated with a reduced risk of dementia or improved cognitive health. Cognitive functioning was systematically categorized into seven distinct cognitive domains, allowing for a nuanced examination of how different sedentary activities influence specific cognitive functions. Moreover, we used different cognitive functions as outcome variables to examine whether different sedentary activities have different effects on a particular cognitive domain, highlighting which sedentary activities are associated with improvements or declines in each specific cognitive function. Finally, in the current systematic review, a meta-analysis was deemed inappropriate due to the heterogeneity of the associations explored, e.g., different sedentary activities and different domains of cognitive function. As meta-analyses generally require a minimum of five studies addressing the same specific research question to ensure sufficient statistical power and comparability of data, with 10 or more studies being the ideal threshold, 30 a meta-analysis was not feasible.
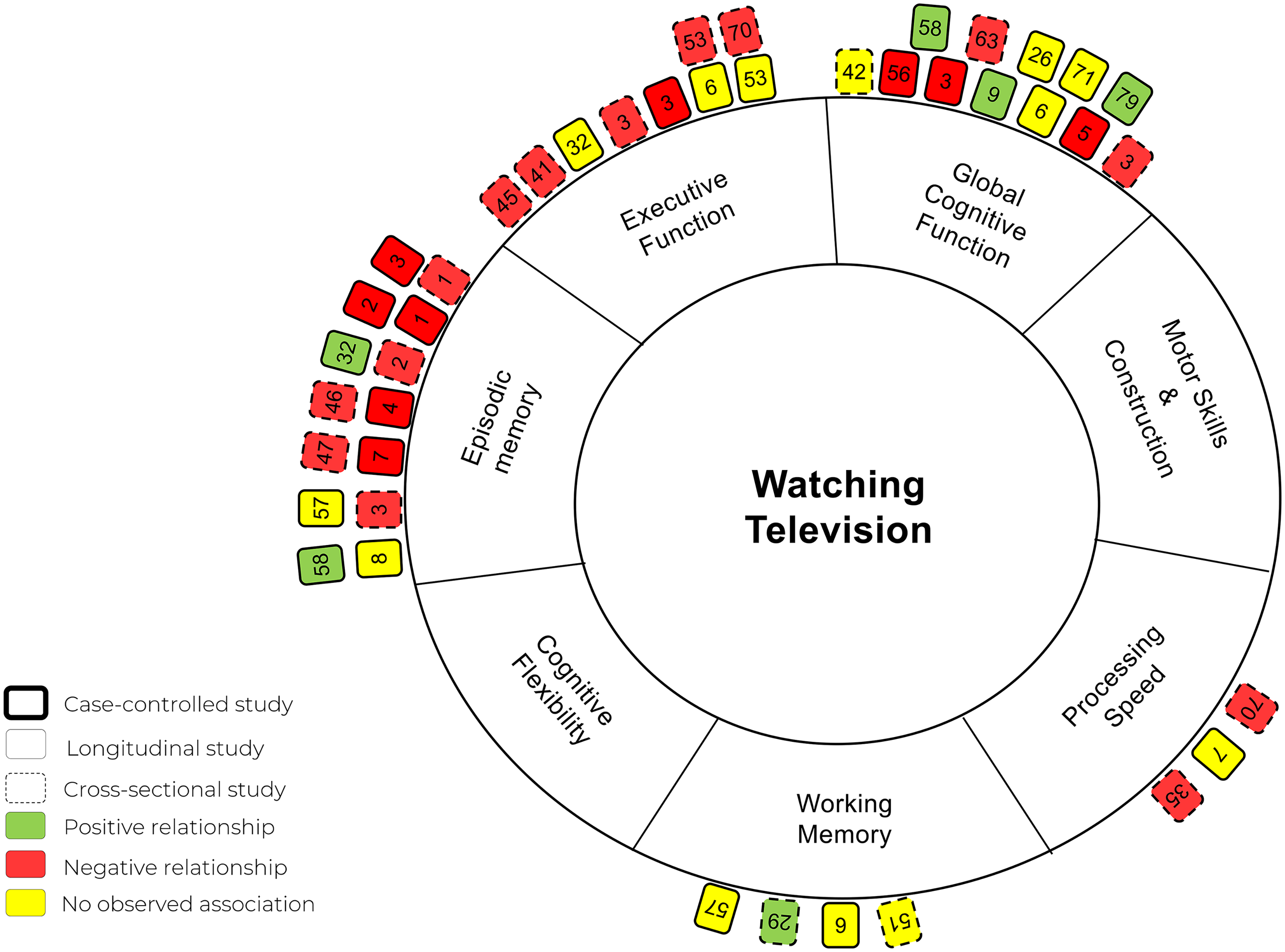
Pinwheel of all studies reporting association between watching television with seven cognitive domains.
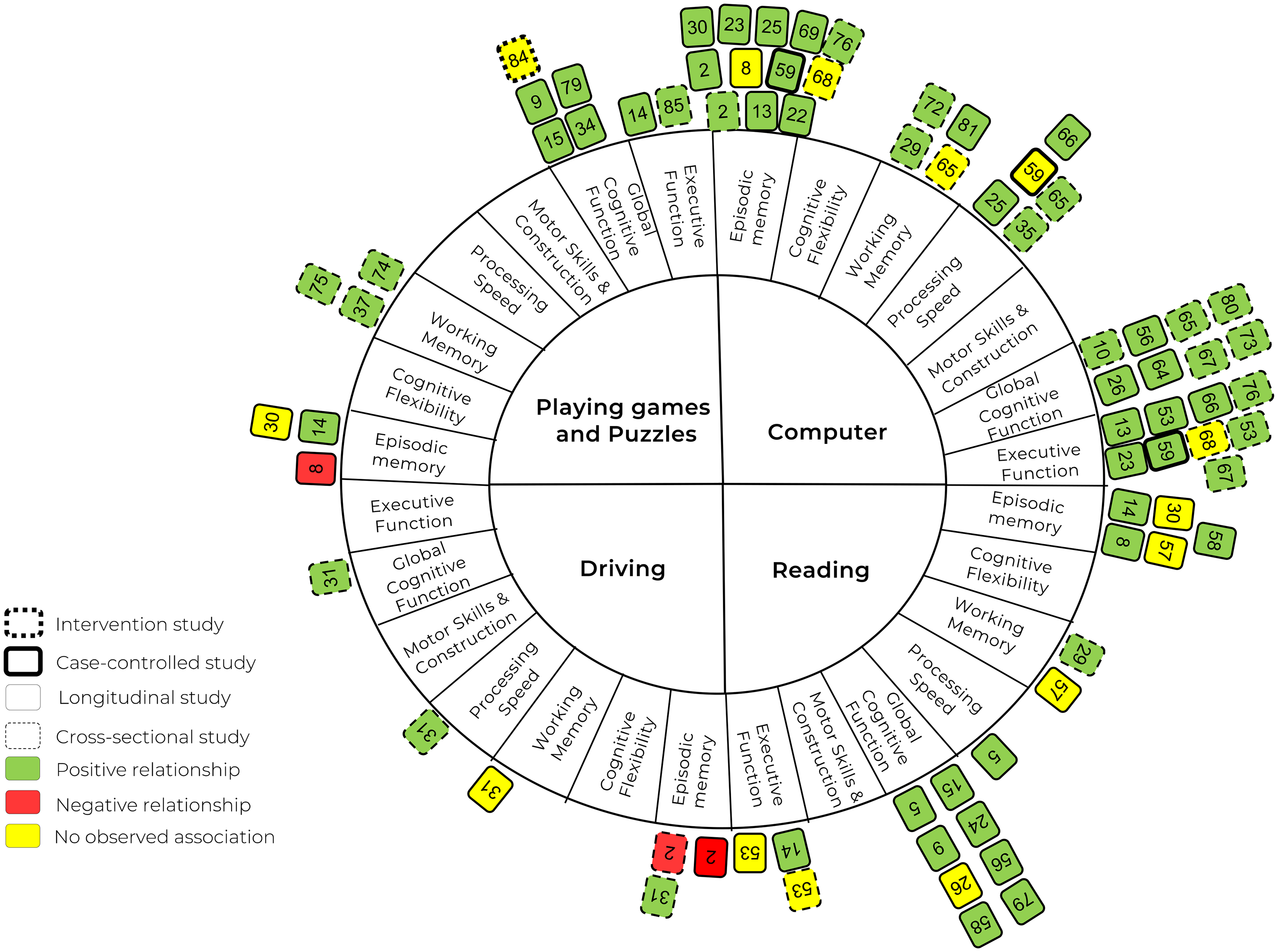
Pinwheel of all studies reporting association between Reading, computer use, playing games and puzzles, and driving with seven cognitive domains.
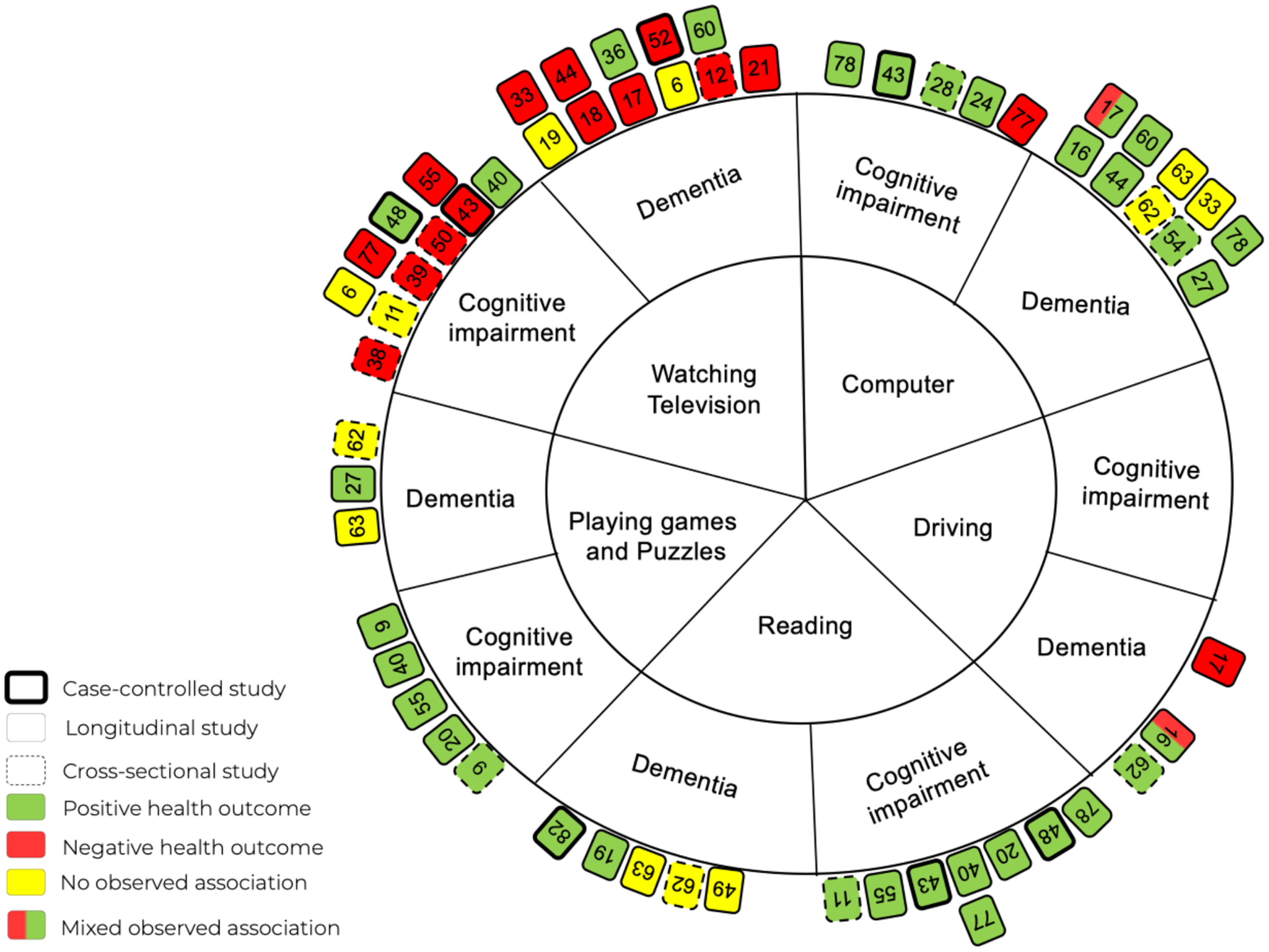
Pinwheel of all studies reporting association between individual sedentary activities with dementia and cognitive impairment.
Results
Search results and study characteristics
The initial electronic database search identified a total of 17912 papers. After removing 1316 duplicates, 16596 papers remained for title and abstract screening. During this stage, 16,148 studies were excluded, leaving 448 studies for full-text review. Following the full-text review, 363 papers were excluded for reasons like wrong exposure, wrong outcome, or wrong population, resulting in 85 studies that met the inclusion criteria (see Figure 4 for the PRISMA flow diagram). Among the 85 studies, 30 were cross-sectional studies,12,31–59 44 were longitudinal studies,12,16,17,25,39,58,60–97 five employed a case-controlled design,98–102 one study was an intervention study, 103 and five studies included both cross-sectional and longitudinal study data,10,24,55,104,105 (see Table 1). Overall, 49 studies included longitudinal analyses, exceeding the number of cross-sectional studies (n = 35), and thereby constituting the predominant study design. The length of follow-up for longitudinal studies ranges from two 104 to 25 years. 68 The publication years of these studies ranged from 2005 98 to 2024, with 10 studies published in 2024.25,35,37,48,56,60,72,73,94,106 Among the 85 studies reviewed, several cohorts were utilized multiple times, including the UK Biobank cohort (n = 12),31,51,56,72,83,86,87,92,93,95,97,105 the Chinese Longitudinal Healthy Longevity Study (CLHLS) cohort (n = 6),78,79,84,90,96,106 the Survey of Health, Ageing and Retirement in Europe (SHARE) cohort (n = 3),61,65,71 the English Longitudinal Study of Ageing (ELSA) cohort (n = 3),17,66,104 the National Health and Aging Trends Study (NHATS) cohort (n = 3),25,60,62 the Health and Retirement Study (HRS) cohort (n = 2),80,85 the German Ageing Survey (n = 2),80,81 and the Pentoxifylline to Protect the Preterm Brain (PROTECT) cohort (n = 2).34,107
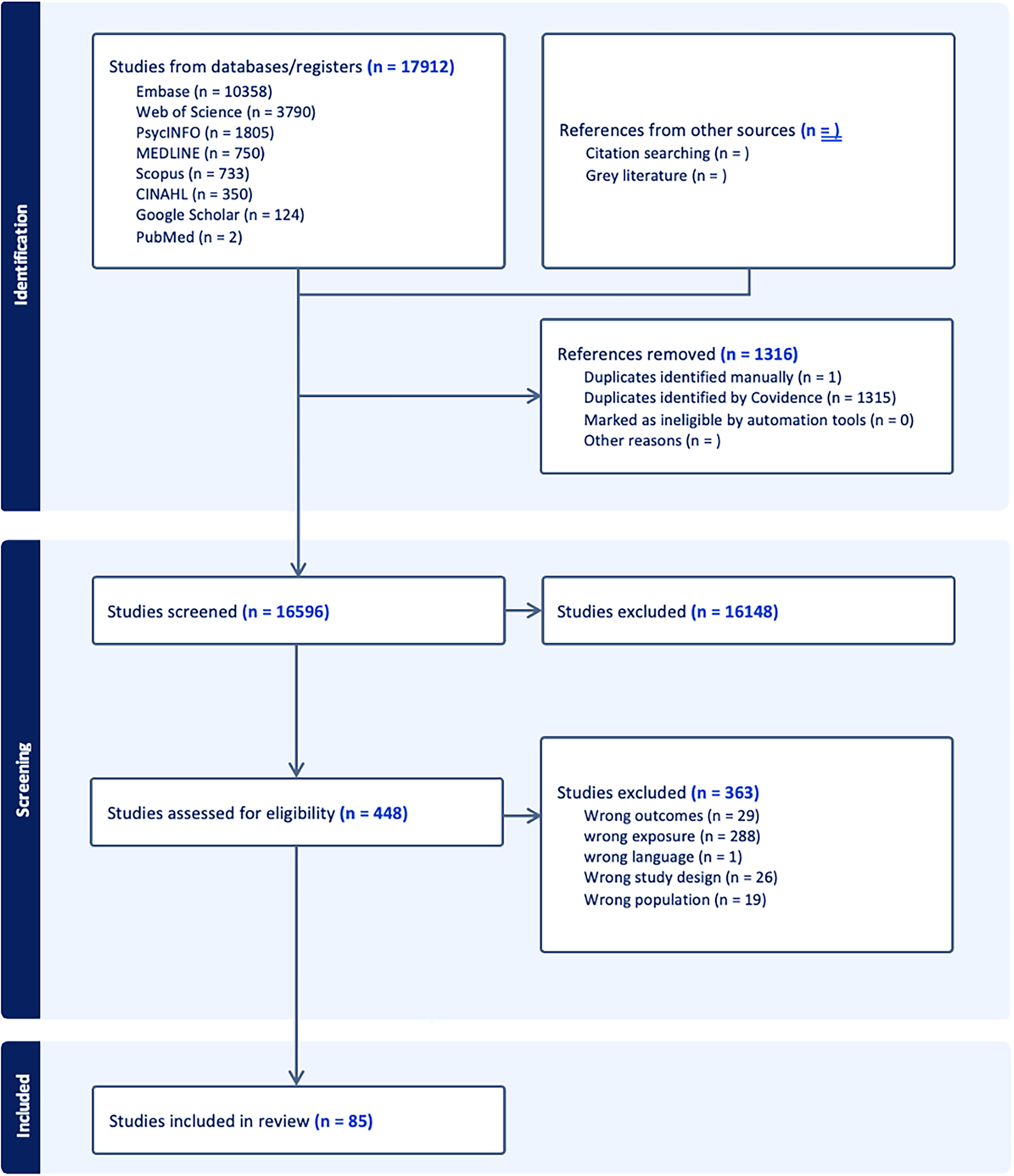
PRISMA flow diagram of the search and screening process in review of individual sedentary activities with cognitive function.
Study population
The total sample size across the 85 studies was 1,575,657 middle-aged and older adults. Where studies were from the same cohort, e.g., the UK Biobank, the largest sample size was included in the total sample size, rather than the participant number from each study from that cohort. Individual study sample sizes ranged from 29 45 to 851,307 64 participants. The mean ages of participants in the included studies ranged from 36.9 45 to 100 71 years old, with the average percentage of female participants being 55.84, ranging from 14.6% 100 to 100%. 64 The majority of the studies were conducted in the United Kingdom (n = 20),17,34,38,60,51,56,64,66,72,83,86,87,92–95,104,105,107,112 the United States (n = 18),16,25,32,33,37,43,48,52,60,62,67,68,74,80,85,98,100,113 and China (n = 14),53,55,59,79,42,78,84,89,90,96,100,101,106,109 with other countries represented, including Japan (n = 7),49,46,54,76,82,103,108 Australia (n = 2),47,91 Germany (n = 2),80,81 Ireland (n = 2),10,77 the Netherlands (n = 1), 88 Mexico (n = 1), 35 Singapore (n = 1), 50 South Korea (n = 2),44,45 Canada (n = 2),36,41 France (n = 2),24,58 Brazil (n = 1), 12 Greece (n = 1), 110 Iran (n = 1), 73 Spain (n = 1), 99 Switzerland (n = 1), 102 and Thailand (n = 1). 57 Four studies were conducted across multiple European countries.39,61,65,71
Exposure (individual sedentary activities)
Tables 2–8 provide a detailed summary of the type of individual sedentary activities examined in the included studies. Five primary individual sedentary activities were identified: watching television, computer use, playing card games, reading, and driving. Among these, only watching television was categorized as a passive sedentary activity, due to its low cognitive engagement compared to the other activities, which involve more active mental participation. 22 A total of 43 studies investigated the association between watching television and cognitive function, including both dementia and cognitive impairment.10,16,17,24,25,35,36,39,41–44,47,49,50,52,56,59,63,66,68,73,85,87,89–91,94,95,97–99,12,77,82,83,95,104,105,108–110,114 Twenty-five studies examined the impact of reading on cognitive function16,24,35,42,49,54,56,61,63,64,66,71,73,74,76,79,82,84,85,89,99,90,102,109,115. Thirty-five studies explored computer use.10,24,31,33,35,46–51,53,56–58,63,65–70,70–72,74–76,80,81,83,85,87,88,91,94–96,99,100,102,110 Seventeen studies assessed games and puzzles (including but not limited to mahjong, poker and puzzles), 34,38,54,55,61,71,78,79,84,85,89,90,92,103,106,107,111and six studies evaluated the impact of driving on cognitive function.48,54,56,86,95,105 Additionally, 29 studies investigated more than one sedentary activity.16,24,35,44,49,51,54,56,63,71,73,74,82–86,88–92,94,95,99,101,105,109 All sedentary activities across the included studies were assessed through self-reports or self-administered questionnaire, with the exception of one study that used monitoring software to assess computer use time. 32
Outcome (cognitive function)
Tables 2–8 present an overview of the various cognitive domains assessed in the included studies and summarize the tools used to measure cognitive function. Eleven studies assessed working memory,12,34,35,38,45,48,58,70,73,79,107 nine studies focused on processing speed,16,17,48,51,58,68,76,81,100 global cognition was evaluated in 22 studies,10,12,16,18,31,33,42,48,53,55,56,58,66,75,78,79,81,88,103,106,109,110 16 studies examined executive function,10,12,24,25,32,36,60,33,40,59,62,67,68,76,100 and 22 studies assessed episodic memory.10,17,25,31,41,43,4860–62,65,67,71,73,77,81,85,96,100,104,105,109 Additionally, 20 studies evaluating more than one cognitive domain.10,12,16,17,25,32,33,48,58,60–62,67,68,73,76,79,80,100,109 Episodic memory was measured using 14 different tools, with the most common being immediate and delayed recall tests (n = 10). Global cognition was assessed using 13 different measures, with the Mini-Mental State Examination (MMSE) being the most frequently used (n = 14). Working memory was assessed with eight different tools, executive function with 13, and processing speed with seven. Table 4 summarized the association between different individual sedentary activities with impaired cognition. Twenty-one studies focused on dementia as a cognitive outcome,12,54,56,57,63,64,72,74,82,83,86,87,91–95,97,98,102,108 and 11 studies assessed cognitive impairment.39,44,46,49,50,75,80,84,89,90,101 Hospital inpatient records were the most common tool for measuring dementia (n = 11), while the MMSE was the most frequently used tool for assessing cognitive impairment (n = 8).
Association of passive sedentary activities with cognitive function
The studies investigating the association between passive sedentary activities (television viewing) and cognitive function are summarized in Table 2 and illustrated in Figure 1. Four studies explored the relationship between television viewing and working memory,12,35,73,98 three studies examined its impact on processing speed,17,51,68 11 studies assessed global cognitive function,10,12,16,18,55,66,78,81,88,109,110 seven investigated executive function,10,12,17,25,36,59,68 and 11 studies focused on episodic memory.10,17,25,41,43,73,77,85,104,105,109 Overall, most studies reported a negative association, indicating that increased time spent watching television was linked to poorer cognitive function. However, five studies reported a positive association,25,35,55,78,109 suggesting that more television viewing was associated with better cognitive outcomes. The association between television viewing and global cognition yielded mixed findings. Among the 11 studies reviewed, four reported a negative effect,10,16,56,66 three identified a positive effect,55,78,109 and the remaining four found no significant effect on global cognition.12,47,88,110 Television viewing demonstrated a strong association with decreased episodic memory in the 11 studies reviewed. Among these, two studies reported positive effects, two found no significant effect, and the remainder consistently reported negative effects on episodic memory. A total of 11 cross-sectional studies reported a negative relationship between television viewing and cognitive function,10,24,36,41,43,51,59,68,97,104,105 while seven longitudinal studies similarly identified a negative association.10,16,17,66,77,104,105 In contrast, only one cross-sectional study reported a positive relationship, 35 compared to four longitudinal studies that observed a positive association25,55,78,109
Association of active sedentary activities with cognitive function
The studies examining the association between active sedentary activities (computer use, reading, playing card games, and driving) and cognitive function are summarized in Tables 3–6 and illustrated in Figure 2. Regarding reading (Table 3), five studies explored its relationship with episodic memory,36,71,73,85,109 two studies assessed its link with working memory,35,73 one study investigated its effect on processing speed, 16 eight studies evaluated global cognitive function,55,66,79,80,12,78,88,109 and two studies assessed executive function.24,61 Eleven studies investigated the relationship between computer use and episodic memory,32,60,62,65,67,71,81,85,96,100,105 four study assessed the link between computer use and working memory,35,45,70,76 five studies examined its association with processing speed,58,76,81,93,100 eight studies explored executive function,24,32,33,60,62,67,76,100 and eight studies investigated global cognitive function31,33,42,53,58,80,88,89 (see Table 4). Meanwhile, three studies examined the impact of games and puzzles on episodic memory,61,71,85 three examined working memory,34,38,107 five examine global cognition,55,78,79,103,106 and two examined executive function40,61 (see Table 5). For driving (Table 6), one study evaluated its association with global cognitive function, 48 processing speed, 48 and working memory. 48 Overall, most studies reported a positive association, indicating that increased engagement in these active sedentary activities was linked to better cognitive function. However, two studies identified a negative association with games and puzzles (8) and driving (2), and eight studies reported no significant effect.16,55,75,79,78,88,89,109 Computer use showed a particularly strong positive relationship with global cognition, executive function, and episodic memory. Among the 27 studies investigating computer use across these three cognitive domains, only four showed no effect,32,58,85,100 with the remaining studies all reporting positive effects. Similarly, reading was strongly associated with global cognition, as seven out of eight studies identified a positive association, with only one study reporting no effect. 88 There was no significant variation in the findings across the different study designs.
Association of sedentary activities with impaired cognitive function
The studies evaluating the association between individual sedentary activities and impaired cognitive function is summarized in Tables 7 and 8 and illustrated in Figure 3. Three studies assessed the relationship between playing card games and dementia,54,81,91 Four studies examined driving and dementia,54,56,63,74 seven studies evaluated reading and dementia,54,56,63,74,81,82,102 12 studies explored the link between television viewing and dementia.12,62,63,82,83,87,91,93–95,97,98 Regarding cognitive impairment, seven studies evaluated television viewing,39,44,49,50,89,90,99 six studies assessed reading,49,84,89,90,99,101 four studies examined playing card games,84,89,90,101 and three studies assessed computer use.46,75,99 Overall, most studies reported positive cognitive health outcomes associated with reading, playing card games, and computer use, while an increased amount of television viewing was generally associated with worse cognitive impairment. One study reported that very low (0 h/day) and high (≥2 h/day) levels of television viewing were associated with increased dementia risk compared to moderate viewing levels (>0 to <2 h/day). 95 Another non-linear relationship was observed for driving whereby individuals who did not drive at all had a significantly higher risk of dementia (HR = 1.41, 95% CI: 1.32–1.51, p < 0.001) compared to those who drove moderately (>0 to <2 h/day). 95 However, prolonged driving (≥2 h/day) was also associated with an increased risk (HR = 1.33, 95% CI: 1.22–1.44, p < 0.001). 95 Reading demonstrated a strong association with positive health outcomes, as among the 13 studies examining its relationship with dementia and cognitive impairment, only three reported no effect,54,56,64 while the remaining studies found positive outcomes. Similarly, playing card games showed a strong relationship with improved dementia and cognitive impairment, with only two of the seven studies reporting no effect.54,56 In this review, cross-sectional studies typically compared sedentary time between individuals with and without dementia, assessing differences in their current cognitive state, while longitudinal studies examined how sedentary activity earlier in life influences cognitive function over time.
Results from the UK Biobank studies showed different directions and strengths of associations in the relationships of each sedentary activity and cognition/dementia. This is demonstrated in the findings of studies examining the relationship of computer use with dementia. For example, Jia et al. (2024) found that frequent computer use was linked to a 19% lower risk of dementia (HR = 0.81, 95% CI: 0.69–0.94); 72 Xu et al. (2024) found no significant association between computer use and dementia risk (HR = 0.86, 95% CI: 0.66–1.12, p = 0.402); 94 and, results for Yang et al. (2023) found that moderate computer use (>0–<2 h/day) appears to be beneficial for dementia risk, whereas both no use (0 h/day) and excessive use (≥2 h/day) are associated with higher dementia risk. 114
Quality assessment score
The overall average quality score across the studies was 75.2%, with individual study scores ranging from 45.8% to 91.7% (as detailed in Supplemental Table 5). A total of 32 studies were classified as meeting the criteria for “good quality”,33,35,37,39–41,46,47,51,53,55–58,60,63–66,68,76,78,82–84,89,90,93,97,98,100,104 38 studies were identified as “strong quality”,10,12,16,17,24,25,31,32,43,44,48,49,52,54,59,62,67,72–75,77,80,81,85–88,91,94–96,101,105,106,108–110 indicating a high level of methodological rigor, seven studies were identified as “adequate quality”,32,34,38,45,50,102,107 and two studies were categorized as “poor quality”.42,103 Associations of sedentary activities with cognitive outcomes from studies categorized as of adequate quality32,34,38,45,50,102,107 were in the same direction as the majority of other studies in those sections of the pinwheel.32,86,90,100,101
Discussion
The purpose of this systematic review was to describe and synthesize existing evidence on the associations between different types of sedentary activities and cognitive outcomes. Specifically, this review aimed to identify how passive and active sedentary activities were differentially associated with key cognitive domains (e.g., episodic memory, executive function, and working memory) to elucidate the cognitive domains that are most susceptible to these activities. In addition, we explored the role of sedentary activities in cognitive decline or cognitive protection in older adults. Overall, the results of this systematic review highlight significant associations between different sedentary activities and cognitive function. Across study designs, the passive sedentary activities (e.g., watching television) were most consistently associated with negative cognitive outcomes, including increased risk of dementia and cognitive impairment, as evidenced by multiple studies with predominantly negative associations. In contrast, active sedentary activities (e.g., reading, playing card games, and using a computer) showed overwhelmingly positive associations with cognitive health, enhancing cognitive functions such as executive function, situational memory, and working memory. Importantly, longitudinal studies, which provide stronger evidence for causality, generally supported these patterns. Effect sizes typically were small in cross-sectional studies but small to medium for the longitudinal studies, underscoring the greater strength of the latter.
There was some preliminary evidence to suggest that the relationship between the sedentary activities of both driving and TV viewing with cognitive outcomes, particularly incident dementia, may not be linear. 95 Specifically, one large prospective cohort study reported U-shaped associations for TV-watching and driving time, and a reversed J-shaped association for nonoccupational computer use, with the lowest dementia risk observed at >0–<2 h/day for each behavior. These findings indicate that both inactivity (complete absence of an activity) and excessive engagement may increase dementia risk, highlighting a potential U-shaped or threshold effects. 95 This non-linearity underscores the need for further longitudinal research to determine whether specific sedentary activities have an optimal engagement level that minimizes cognitive risks and whether these effects vary across cognitive domains.
Passive sedentary activities
Our findings consistently show significant negative associations between passive sedentary behaviors (e.g., television viewing) and a variety of cognitive domains. Cross-sectional studies frequently identified negative associations, particularly with episodic memory, but these designs are limited by the inability to establish temporal direction. Importantly, longitudinal studies provide stronger support for these associations, with several showing that higher television viewing predicts greater risk of dementia and cognitive decline over time. The most significant association observed in our analyses was in episodic memory, with 10 of the 14 studies reporting a negative association between higher TV viewing time and situational memory performance. Taken together, the longitudinal evidence provides the most compelling case that prolonged television viewing may harm cognition, though further research is needed to clarify the role of program content, viewing patterns, and contextual factors.
One potential mechanism for this decline is that TV watching is often associated with continuous TV watching behavior (e.g., binge watching), and this pattern of sedentary behavior negatively impacts memory consolidation. 86 Memory consolidation is the process of converting short-term memories into long-term memories. 86 This process is designed to transfer memories from the hippocampus (the part of the brain associated with short-term gains and instincts) to the cerebral cortex (the part of the brain associated with rational/deeper thinking) and to build long-term memories by increasing the complexity, distribution, and connectivity of the cortex relative to the rest of the brain. 86 Continuous television viewing interferes with this process because it does not provide enough time for the formation and transfer of clear memories. This is further explained by the theory of temporal uniqueness, which suggests that memory recall can be enhanced when there is sufficient spacing between events. 116 However, it is unclear from our findings whether watching TV interrupts the consolidation of short-term memory from other periods of the day by preventing the successful transfer of memories to the cerebral cortex. This lack of “downtime” may disrupt the consolidation of neutral memories, preventing them from performing properly. 117 Thus, the same cognitive principles that apply to episodic memory formation in TV viewing can be generalized to other memory-related tasks. Whether individuals are engaging in educational activities, professional work, or personal learning, incorporating breaks, and allowing time for reflection between episodes is essential for effective memory consolidation. This reinforces the importance of spaced repetition techniques and underscores how passive, continuous exposure to information—without adequate intervals for reflection—can diminish long-term memory performance across different domains.
The negative effects of television viewing on executive functioning stem from the lack of cognitive engagement required for passive activities. Executive functioning refers to cognitive processes that rely on higher-order cognitive processing, such as planning, decision-making, and task-switching, which require frequent activation of the prefrontal cortex, the area of the brain responsible for higher-order thinking.118,119 In contrast, during television viewing, especially prolonged continuous television viewing, cognitive processes that typically rely on active engagement are underutilized, and in the absence of such cognitively engaged stimuli, neural pathways associated with executive functioning are weakened over time, leading to atrophy. 87 Simply put, just as a muscle weakens without exercise, the areas of the brain responsible for complex thinking deteriorate without active participation. Executive function requires constant use of these cognitive “muscles” through activities that require planning, problem solving, and quick thinking. Watching television provides little cognitive stimulation, leading to a decline in these functions, especially in older adults who are already facing natural cognitive aging.
While our review confirms much of the existing literature, it also highlights research gaps that warrant further exploration. Specifically, contextual factors, such as whether television programs are educational and whether individuals take regular breaks during viewing, have not been adequately studied. In addition to the lack of studies on television content and breaks during viewing, other contextual factors such as snacking may also influence cognitive outcomes. Snacking during television viewing could contribute to mindless eating, potentially affecting overall health and cognitive function indirectly through dietary patterns and weight gain, both of which are linked to cognitive decline.120,121 Addressing these factors may provide more comprehensive insights into how passive sedentary behavior affects cognitive function.
Active sedentary activities
Our data indicate that most studies demonstrate a positive correlation between active sedentary activities and cognitive functioning, which contrasts with the negative associations often observed in passive activities such as television viewing. Here again, longitudinal studies provide the strongest evidence: reading, computer use, and puzzle play were associated with better executive function, episodic memory, and overall cognition over time, even after accounting for baseline performance. Cross-sectional and case-control designs supported these benefits, reinforcing the robustness of these findings. The cognitive engagement required for these active activities appears to play a critical role in maintaining or even improving cognitive performance across multiple domains, including executive function, situational memory, and overall cognitive function. Reading is associated with positive outcomes in almost all cognitive domains. Studies have shown that reading is positively correlated with situational memory, executive functioning, and overall cognitive functioning, with no negative correlations observed. 122 This is because reading typically requires active participation through comprehension, memory recall, and mental visualization, challenging the brain to process complex narratives and ideas. 122
In addition, reading involves multiple regions of the brain, including the temporal lobe, Broca's area, and the angular gyrus, all of which are involved in language comprehension, memory recall, and mental visualization. 123 Reading also stimulates white matter pathways, enhancing the brain's ability to process information and form neural connections, which supports overall cognitive health and reduces the risk of cognitive decline. 123 Research shows that reading rewires your brain, creating new neural networks and strengthening white matter in the corpus callosum, which enhances communication between the two brain hemispheres. 124 These pathways improve overall cognitive function, which in turn improves your ability to actively recall information. The relationship between reading and reduced risk of cognitive decline may reflect the effects of education. 125 Previous research on early educational achievement and cognitive functioning in later life is controversial. Specifically, some studies supporting the cognitive reserve (CR) hypothesis suggest that higher levels of education provide a buffer against age-related cognitive decline and dementia. The CR hypothesis posits that individuals with higher education develop more robust neural networks, which allow them to better compensate for brain changes associated with aging, thus delaying the onset of dementia or cognitive impairment. 126 However, other research challenges this idea, suggesting while education is positively associated with cognitive performance at baseline, it does not appear to slow the rate of cognitive decline over time, meaning that education contributes to a higher starting point in cognitive abilities but does not alter the trajectory of cognitive aging. 127 However, although our data support the cognitive benefits of reading, this review did not consider stratified analyses for educational level; therefore, future research should explore the relationship between education and cognitive function more thoroughly to understand this link more clearly.
Similarly, data on playing games and puzzles show mostly positive associations with cognitive functioning. This is largely because card games involve strategic thinking, problem solving, and often social interaction. These games require the brain to switch rapidly between different cognitive tasks. To win or play well in the game, players need to coordinate and work with a variety of abilities, such as attention, observation, alertness, memory, recall, calculation, language, and communication, which, when used repeatedly in games, can improve and maintain cognitive functioning in older adults.19,128 Interpersonal interactions and emotional stimulation during play can further support the reactivation of neural circuits, positively affecting decision-making and cognitive health. 129 This dynamic mental stimulation may contribute to positive effects on executive function and memory, as these areas are closely linked to the brain's ability to adapt and multitask. In contrast to passive activities, playing card games provides sustained cognitive engagement that strengthens neural circuits related to decision-making, strategy development, and working memory. In addition, playing games and puzzles requires a certain amount of upper-limb physical activity in addition to rich emotional and environmental stimuli, which may increase cerebral blood flow, stimulate central nervous system excitation, improve brain tissue metabolism, and promote the establishment of brain neural networks, leading to adaptive changes in brain structure and function.130–132 Furthermore, playing games and puzzles helps to improve social support, reduce psychological stress, and protect stress-related neurons, all of which benefit cognitive function.132,133
The use of computers is another sedentary activity that is closely associated with cognitive benefits in the areas of executive function, overall cognitive function, and situational memory. Tasks performed on computers are often complex—whether for work, communication, or recreation—and typically require sustained attention, memory use and decision-making, all of which require cognitive abilities. Thus, this activity, although sedentary, can mobilize multiple cognitive processes simultaneously. Unlike passive activities, computer use encourages higher levels of cognitive engagement, such as problem solving and information processing, both of which contribute to better cognitive outcomes. 134 In addition, the use of computers and the Internet may provide older adults with opportunities to step out of their comfort zones and engage in more alternative activities, which in turn may stimulate cognitive functioning and provide cognitive benefits. 135 Computer use is also an interactive activity that poses special challenges for older adults, including increased psychomotor abilities when using a computer mouse, as well as sensory and cognitive abilities (e.g., speed of searching for icons), and problems with learning, memory, and executive functioning, all of which may be affected with age. Computer use may also have specific links to executive function. Neuroimaging has shown that older adults utilize prefrontal cortical areas during functional tasks and that middle aged and older adults with more computer experience have greater brain activation in frontal areas of the brain during Internet search tasks. 136
The cognitive advantages of driving may be related to processing speed and working memory. Driving is a complex activity with multitasking, spatial awareness, decision making, and problem solving, all of which require executive functions of the brain. 137 While driving, people must constantly process visual and auditory information, respond to environmental stimuli, and make split-second decisions that activate brain areas associated with attention, working memory, and cognitive flexibility. Longitudinal evidence provides mixed findings in this regard. One study reported that greater driving time was associated with small but significant improvements in visual-spatial and short-term numeric memory, suggesting that the cognitive demands of driving may help maintain cognitive flexibility and executive functioning.105,114 In contrast, two studies found that both no driving and higher levels of daily driving were linked to increased dementia risk, indicating a potentially non-linear relationship. 86 These inconsistent results highlight the complexity of driving as a cognitively stimulating activity, where benefits may depend on the level of engagement and individual context. Although fewer studies have focused on driving compared to other activities such as reading or computer use, the available evidence suggests that the cognitive demands of driving may help maintain cognitive flexibility and executive functioning, which are crucial for cognitive health in aging individuals. However, it is also important to consider the possibility of reverse causation in this relationship. It could be that individuals who continue to drive as they age are doing so because they already possess better cognitive function, rather than driving itself being the cause of maintained cognition. In other words, people with higher cognitive abilities may be more capable of continuing to drive, which makes it difficult to determine whether driving actively preserves cognitive function or simply reflects the individual's pre-existing cognitive status. Further research is needed to disentangle these effects and clarify whether driving directly supports cognitive health or is merely a marker of better cognition.
Differences in study results, particularly those from the UK Biobank studies, suggest that variations in sample characteristics, follow-up duration, and study design may influence findings. For example, some UK biobank studies included younger participants at baseline, whereas other studies primarily focused on older populations already at risk for cognitive decline. This age difference is critical, as cognitive impairment and dementia typically develop over long periods. Younger participants may not yet show cognitive deficits
Strengths and limitations of the review
This systematic evaluation has several significant strengths. First, it distinguishes between passive and active sedentary activities and examines in detail how individual sedentary activities are differentially associated with cognitive functioning in older adults. Second, the inclusion of different study designs—including cross-sectional, longitudinal, intervention, and case-control studies—increases the robustness and breadth of the findings. Longitudinal, case-control, and cross-sectional studies yielded consistent findings regarding active sedentary activities, indicating similar effects on cognition. However, the findings on the relationship of TV with cognitive function were more mixed across study types with more longitudinal studies demonstrating positive associations. Thirdly, several of the included longitudinal studies controlled for baseline cognitive function. This methodological feature helps reduce the risk of reverse causation, where early cognitive decline may lead individuals to disengage from cognitively stimulating activities and increase their engagement in passive behaviors such as television viewing. By adjusting for pre-existing cognitive status, these longitudinal designs provide stronger evidence for a potential causal relationship between sedentary activities and cognitive outcomes, thereby offering greater confidence in the observed associations compared to cross-sectional studies, where temporal ordering cannot be established. Importantly, the length of follow-up across these studies ranged from two to 25 years, allowing for both short-term and long-term trajectories of cognitive change to be examined. Another strength is the use of large population-based datasets from multiple countries and that we followed the PRISMA guideline. The use of the pinwheel also identified a lack of evidence that no studies have examined the impact of sedentary activities on motor skills and coordination or cognitive flexibility.
This systematic evaluation also has some concurrent limitations. While in this review, cognitive domains were assessed by several different measures, methods for assessing cognitive function in the included in the studies were all well validated which supports the robustness of our findings. Another limitation of this systematic review is the assessment of sedentary activities. Data were not available regarding posture, content of the activities, e.g., type of television program, and social interactions. A proposed taxonomy suggests also collecting data around choice and novelty which may provide further information on the mechanisms of the associations of sedentary activities with cognition. 138 The current literature precluded conducting a meta-analysis which may provide further evidence to quantify the relationships described in this review. Future research should focus on conducting meta-analyses to strengthen the evidence base and quantify these relationships more robustly, provided that a sufficient number of appropriate studies are available. Moreover, another limitation is the uncertainty regarding whether the effects of individual sedentary activities were adequately adjusted for other concurrent sedentary activities. We therefore do not know whether any of the active sedentary activities may confer protective benefits against the impacts on cognition of watching television. Furthermore, the studies were limited in adjusting for other risk factors for dementia listed in the Lancet Commission paper. Future studies should ensure that such adjustments are made to better understand the distinct effects of each sedentary activity.
In addition, many of the included studies, although prospective, relied on only one or two measurement time points, which makes it difficult to conclude whether the observed associations are predictive of cognitive decline or instead reflect early indicators of preclinical impairment. Sedentary activities may act as more sensitive markers than cognitive assessment tools, and although this review highlighted reverse causation primarily in relation to driving, it is also reasonable to consider that reverse causation may influence other sedentary activities, such as TV viewing or computer use, where early cognitive decline could alter participation patterns. 139 Taken together, while the long follow-up periods in some cohorts strengthen causal inference, the reliance on limited time points in others suggests that changes in behavior may sometimes be better interpreted as indicators of emerging impairment rather than causes of decline. Additionally, most of the studies in this review were from the UK (UK Million Women Study and UK Biobank cohort). Furthermore, all included studies were conducted in high-income countries, meaning that populations from low- and middle-income countries were not represented. This geographic limitation is important, as socioeconomic and cultural differences can influence both sedentary behavior patterns and cognitive health outcomes. The lack of studies from diverse regions restricts the applicability of the findings to global populations, highlighting the need for future research to explore these associations in underrepresented geographic areas and diverse socioeconomic contexts. The last limitation is that studies were only published in English.
Practical implications
The broader public health implications of these findings suggest that existing guidelines should be updated to reflect the cognitive risks associated with sedentary activities. However, current public health campaigns tend to focus on the physical health effects of sedentary activities, such as cardiovascular disease, cognitive effects are less emphasized. For example, during the World Health Organization's 2020 Guidelines on Physical Activity and Sedentary Behavior development process, the Guideline Development Group (GDG) identified all-cause mortality and cardiovascular mortality as the most critical outcomes to be addressed. 140 These were followed by other clinical outcomes, including falls, depression, cognition, and health-related quality of life. While cognition was included, it was not given the same priority as physical health outcomes, reflecting the broader tendency to focus on physical risks such as heart disease and mortality, rather than the cognitive consequences of sedentary activities. 140 With the trend towards 24-h movement behavior guidelines, such as the Canadian 24-Hour Movement Guidelines for adults and older adults, it is important to carefully consider which activities constitute the sedentary time component of the day. 141 Our findings suggest that it may not be beneficial to group television time and computer use together as “screen time,” given the differing associations with brain health. For instance, passive activities like television viewing are more strongly associated with cognitive decline, whereas active sedentary activities, such as computer use, may provide cognitive benefits. Therefore, future public health guidelines should place a greater emphasis on the cognitive health impacts of sedentary activities and distinguishing between passive and active sedentary activities. Additionally, given the growing trend of obsessive behaviors around television public health messages could emphasize the cognitive risks of prolonged time spent on television viewing and provide strategies to integrate more rest and cognitive engagement during these periods. For example, public health campaigns could recommend limiting daily television consumption and encouraging physical activity or cognitive activity during breaks, such as puzzles, social interactions, or brief exercise.
Research gaps and future directions
This systematic review reveals several key research gaps and opportunities for future research. First, the need for experimental studies is clear, as most studies to date have been observational, which limits our understanding of the causal relationship between sedentary activities and cognitive decline. Experimental designs can more rigorously test how interventions mitigate the deleterious effects of chronic passive activities. Another key area for further exploration is the intersection of physical and cognitive health. Sedentary behaviors often coincide with a lack of physical activity, and it is critical to understand how different levels of physical activity can mitigate the cognitive risks associated with sedentary lifestyles. Research should explore whether increased physical activity can counteract the negative cognitive consequences associated with passive behaviors, potentially identifying protective factors that maintain neuroplasticity and cognitive reserve. In addition to sedentary activities, the role of cognitive training deserves further attention. We excluded more than 200 studies on cognitive training, and these interventions have shown great potential to enhance cognitive functioning, particularly in the areas of executive function, memory, and attention.26–28 Future research should investigate whether cognitive training can be effectively combined with recommendations to reduce passive sedentary activities, resulting in a multifaceted approach to protecting cognitive health in older adults. Such integrated interventions could provide a more comprehensive solution to slowing or mitigating age-related cognitive decline. Another notable gap in the current literature is the lack of consensus regarding the distinction between active and passive sedentary activities, which can obscure the unique effects each type may have on cognitive and health outcomes. To address this, future research could benefit from investigating the cognitive load of different sedentary activities and developing consensus using a Delphi study methodology, where a panel of experts systematically classifies sedentary activities into active and passive categories.
Additionally, the review calls for more research on content-specific sedentary behaviors, particularly in the context of television viewing. While existing studies did not differentiate program type, it is plausible that more intellectually stimulating content (e.g., documentaries or educational programs) may confer different cognitive effects compared to purely entertainment-focused content. Examining these distinctions, along with the role of social interactions during viewing, will provide a more detailed understanding of how different contexts of sedentary activities contribute to or mitigate cognitive risk. Another important research gap is the role of social media use. Although not examined in the studies included in this review, social media represents a rapidly growing sedentary activity that may differ cognitively from both passive television viewing and active computer use. Future research should investigate whether the interactive features of social media confer cognitive benefits or, conversely, contribute to cognitive overload and distraction. Future research should also include the opportunity to explore these associations in individuals residing in aged care facilities. This population typically experiences more comorbidities, increased sedentary time, poorer cognition, and decreased physical activity, making them an important group for studying the cognitive impacts of sedentary behaviors. 142 Understanding these associations in such a vulnerable population could offer valuable insights into how sedentary behavior interventions might be tailored to improve cognitive outcomes and overall health in aged care settings. Future studies also need to examine the associations between sedentary activities and other cognitive domains, such as cognitive flexibility, which were not included in this review due to the lack of studies reporting outcomes in this area. Finally, only one of the included studies used a device to measure sedentary activities, the rest relied on self-reported data, which is prone to recall bias and inaccuracy. This is because older adults’ physical activity participation is often intermittent, sporadic, or unstructured, which makes recall extremely difficult, and older adults may inadvertently exaggerate their sedentary activities. Moreover, a previous review reported that studies that used devices to measure sedentary time showed a significant negative association with cognition, while studies relying on self-reporting found a positive association between sedentary time and cognitive function. 20 Therefore, future research on the association between sedentary activities and cognitive function should use both objective and subjective measures whenever possible, although using device is very difficult and expensive.
Conclusion
In conclusion, this systematic review comprehensively examined the differential impacts of passive and active sedentary activities on cognitive function in middle-aged and older adults. The findings indicate that passive sedentary activities (e.g., watching television) consistently correlates with negative cognitive outcomes, including cognitive decline and dementia risk. In contrast, active sedentary activities, such as reading, playing card games, and computer use relate to positive cognitive outcomes, particularly in preserving executive function, memory, and cognitive flexibility. These results suggest that public health guidelines should emphasize reducing time spent on passive sedentary activities and promoting cognitively stimulating activities to protect against cognitive decline. Additionally, future research should incorporate experimental studies to change sedentary activities, including cognitive training. These trials could also examine how physical activity might mitigate the cognitive risks associated with sedentary activities. Together, this body of research would provide evidence to gain a more comprehensive understanding of how to improve cognitive health in aging populations.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251394751 - Supplemental material for Individual sedentary activities and cognitive function in middle-aged and older adults: A systematic review
Supplemental material, sj-docx-1-alz-10.1177_13872877251394751 for Individual sedentary activities and cognitive function in middle-aged and older adults: A systematic review by Jiatong Chen, Kirsten Dillon-Rossiter, Lily Grigsby-Duffy, Anisa Morava, Adam Novic, Babac Salmani, Siobhan Smith, Harry Prapavessis and Paul A Gardiner in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Greta Vos assisted with developing the search strategy and conducting the search.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data can be obtained upon request from the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.