
Abstract
Background
Young-onset dementia (YOD), diagnosed before age 65, most often appears as Alzheimer's disease (AD) or frontotemporal dementia (FTD). Compared to late-onset dementia (LOD), YOD poses distinct caregiving, emotional, and social challenges. While research has expanded, it has largely centered on spouses and children, leaving the experiences of parents caring for an adult child with YOD underexplored and in need of greater scholarly attention
Objective
This study aims to investigate the unique experiences of parents caring for an adult child diagnosed with YOD.
Methods
Qualitative semi-structured interviews were conducted with 12 Hebrew-speaking Jewish Israeli parents who provided informal care to an adult child diagnosed with YOD. The sample included cases of FTD and dementia with Lewy bodies (DLB). Participants were recruited through purposive sampling, and the data were analyzed using thematic analysis.
Results
Thematic analysis revealed three themes. The first, “The Diagnosis,” captured parents’ descriptions of the long and complex diagnostic process, from initial recognition of symptoms to the formal diagnosis. The second, “Parent-Child Relationship,” reflected experiences of loss and shifting dynamics within the relationship. The third, “Assimilation Into the Caregiver Role,” highlighted significant changes in personal identity alongside emotional, and practical caregiving challenges.
Conclusions
Caring for an adult child with YOD involves a profound sense of loss and presents substantial challenges to parental identity, particularly as parents themselves age. These findings highlight the critical need for tailored interventions, improved communication, and strengthened support within healthcare and mental health systems to effectively address the unique needs of parent caregivers.
Introduction
Dementia is a broad term encompassing several progressive disorders that impair memory, cognition, and the ability to perform daily activities. 1 While dementia is predominantly associated with aging, growing evidence highlights the increasing incidence of young-onset dementia (YOD), defined as dementia diagnosed before the age of 65. 2 Common types of YOD include Alzheimer's disease (AD), frontotemporal dementia (FTD), dementia with Lewy bodies (DLB), vascular dementia and medical disorders such as Huntington's disease and Parkinson's disease. 3
YOD presents with a wide range of behavioral, cognitive, psychiatric, and neurological symptoms, making diagnosis particularly challenging and often delayed. 4 Early symptoms are usually subtle and ambiguous, further complicating timely detection. 5 When a definitive diagnosis is finally received, families often experience acute shock and devastation, not only due to the individual's relatively young age, but also because of the realization that their lives will be permanently changed. 6 As the disease progresses, care increasingly relies on both formal and informal support systems. While formal support is provided by paid professionals, such as home care workers, informal support is typically offered by family members or close friends.7,8 In most cases, family members, particularly spouses and adult children, assume the primary caregiving responsibilities. 9
The period following diagnosis marks a complex transition, as caregivers must adapt to evolving responsibilities and assume multidimensional compensatory roles while managing their existing commitments. 10 Research has illuminated the complex realities faced by caregivers of individuals with YOD, emphasizing both the profound loss of emotional intimacy and the increasing burden of care as the disease advances.11,12 These challenges are especially pronounced due to the progressive impairments in behavior, personality, and cognition associated with YOD. 13 As these changes occur, caregivers frequently grapple with ambiguous loss, a phenomenon in which the individual with YOD remains physically present, yet their memories and sense of identity gradually deteriorate.14,15
Caregivers of individuals with YOD may also experience anticipatory grief, characterized by sorrow and a sense of impending loss due to the progressive nature of the disease. 16 Recent research highlights a strong positive correlation between caregiver burden and anticipatory grief among primary caregivers of individuals with YOD, underscoring the profound emotional toll of prolonged caregiving. 17 For parents caring for an adult child with a chronic illness, anticipatory grief is intensified by the child's diminishing autonomy and the parents’ own loss of independence. This experience, termed “perpetual parenthood,” extends caregiving beyond the expected life stage, disrupting the natural trajectory of parental roles and imposing a significant emotional burden.18,19 Such challenges are shaped not only by personal circumstances but also by broader social expectations, particularly in cultures that place high value on parental devotion and responsibility. 20 In Israel, for example, pro-natalist cultural values position the family as a central institution, magnifying both the sense of duty and the emotional weight carried by parental caregivers, often more so than in many other industrialized societies. 21
To better conceptualize these challenges, researchers have turned to the Dementia Grief Model (DGM), which frames dementia-related grief as a normative yet uniquely complex process. Unlike traditional models of bereavement, the DGM situates grief as a normative, though uniquely complex, process shaped by the progressive and recurrent losses characteristic of dementia. The model delineates three interrelated psychological states, separation, liminality, and re-emergence, each marked by a specific experiential quality and propelled by dynamic mechanisms that facilitate adaptation. When these mechanisms fail to operate effectively, caregivers may become trapped in cycles of unresolved grief, leading to heightened emotional distress and diminished coping capacity. 22 Importantly, however, the grief trajectory is not uniform across caregivers. Factors such as gender and relational role, such as spouse, adult child, or parent, influence how pre-death grief is experienced and expressed. 23
Against this backdrop, existing scholarship has focused predominantly on the experiences of spousal and child caregivers,24–29 leaving the voices of parents of adult children with YOD largely absent from the literature.30,31 This group occupies a distinct and understudied position within the caregiving spectrum, as their experiences are shaped by the dual realities of maintaining a lifelong parental role while simultaneously meeting the intensive demands of daily care for an adult child. Consequently, there is a pressing need to examine more closely the unique challenges and unmet needs of these parents, particularly those serving as primary caregivers. Such inquiry is essential not only for illuminating their lived realities but also for identifying the forms of targeted support and intervention required to sustain their caregiving role. Accordingly, the aim of this study was to explore the experiences of parents caring for an adult child with YOD. The guiding research question was “What are the experiences of parents serving as informal caregivers for an adult child with YOD?”
Methods
Study design
The aim of this study was to examine the experiences of parents caring for an adult child with YOD. A qualitative design using semi-structured interviews was chosen, as this approach is well suited to capturing the depth, nuance, and subjectivity of complex caregiving experiences that cannot be meaningfully conveyed through quantitative measures. Thematic analysis was used to identify patterns within participants’ narratives while allowing flexibility to account for diverse individual perspectives. 32 This method facilitated the exploration of both shared challenges and unique variations in parents’ accounts, providing a rich, contextually grounded understanding of caregiving in the context of YOD.
Sample
Participants were recruited through purposive sampling. Advertisements were posted on internet forums and Facebook groups with group administrator approval. These forums included the following: “Families Dealing with FTD,” “Alzheimer Dementia—Daily Activities,” and “Amda Group—An Association for Alzheimer's Dementia Patients and Similar Diseases in Israel.” Members of these group were family and friends of individuals diagnosed with YOD. Candidates were provided with full information regarding the study when they made contact via email or phone, as soon as their compatibility with the inclusion criteria was ascertained. The inclusion criteria were as follows: (a) Have a child diagnosed with dementia before age of 65; (b) providing informal care for at least one year since the diagnosis; and (c) Jewish Israeli and Hebrew-speaking. Informal caregivers were defined as non-professional individuals who provided the majority of assistance and supervision necessary to meet the basic needs of persons with any form of dementia. 8 In all cases, the caregiver-care recipient relationship was biological.
A total of twelve participants met all inclusion criteria and were interviewed: six men and six women, ranging in age from 71 to 82 (see Table 1, for participant characteristics). The study's sample size is consistent with other studies employing thematic analysis to achieve data saturation. 33 No eligible participant declined participation, and none withdrew during the study. Most participants were married and cohabiting with their spouses. None of the parents lived with their adult child diagnosed with YOD. Among the adult children with YOD, three were divorce and nine were married, though none were living with their spouses at the time of data collection. All adult children received some form of formal caregiving support, in addition to care provided by their parents, who served as the primary informal caregivers in all cases. The types of dementia represented in the sample included FTD and DLB.
Participant characteristics.
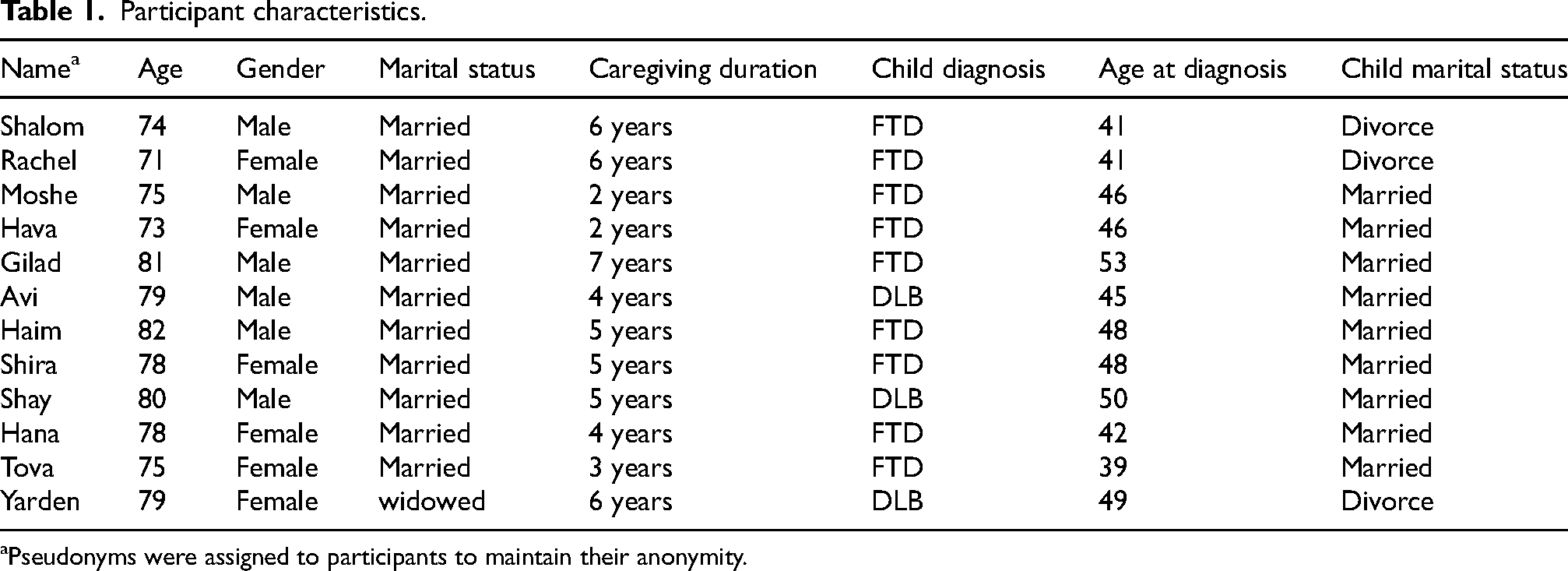
Pseudonyms were assigned to participants to maintain their anonymity.
Data collection
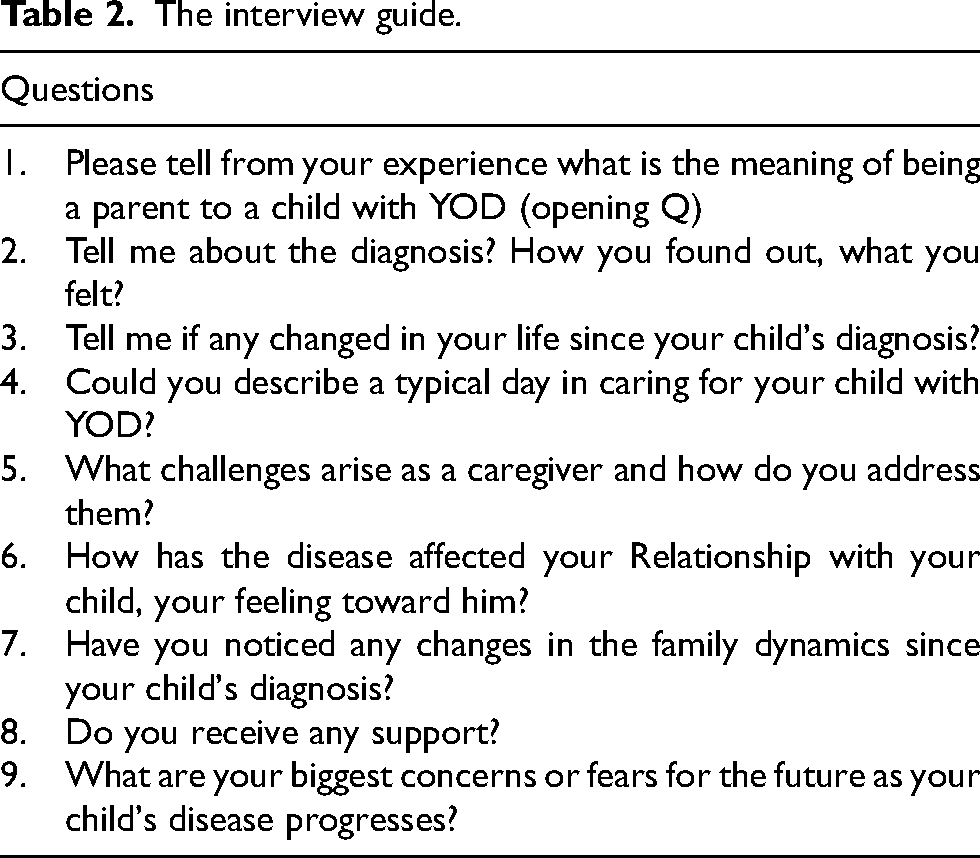
Data were collected through in-depth, semi-structured interviews conducted between July and November 2024. The interview protocol provided systematic and consistent data collection while maintaining flexibility to elicit spontaneous, detailed accounts and preserve a conversational tone. Questions focused on experiences across the trajectory of YOD, perceived challenges and sources of distress, and supports that had, or could have, been helpful (see Table 2, for interview guide). The interview guide was developed based on multiple sources, with key concepts and domains of exploration identified through a review of the published literature,34–36 which informed the structure and thematic focus of the guide.
The interview guide.
All interviews were conducted face to face by the first author, a female graduate student in medical psychology with prior experience in qualitative interviewing and analysis. At the beginning of each interview, participants were informed of the study's objectives and invited to ask questions. Written informed consent was obtained prior to participation, followed by the completion of a brief demographic questionnaire. Interviews were conducted in Hebrew, lasted between 45 and 60 min (average 50 min), and took place in participants’ homes across the Lowland region, Jerusalem District, and Central District of Israel. With participants’ consent, all interviews were audio-recorded in their entirety and subsequently transcribed verbatim in Hebrew by the first author. To ensure confidentiality, all identifying information was removed from the transcripts, and all study materials were stored securely under password protection.
Each interview began with a broad, open-ended question intended to elicit personal narratives: “Please tell from your experience what is the meaning of being a parent to a child with YOD.” This was followed by a series of follow-up, exploratory, and open-ended questions, including: “Tell me about the diagnosis? How you found out, what you felt?”; “What challenges arise as a caregiver and how do you address them?”; and “Have you noticed any changes in the family dynamics since your child's diagnosis?”
Data analysis
The interviews were transcribed verbatim in Hebrew by the first author, who also conducted the interviews. Data analysis was carried out on the original transcripts, and only the selected quotations were translated into English after the analytic process was completed. A reflexive thematic approach guided the analysis, following Braun and Clarke's six-phase process of data familiarization, coding, theme development, and refinement.37,38 This method provided a systematic yet flexible framework for identifying and interpreting patterns within qualitative data, enabling the construction of meanings and conceptualizations grounded in participants’ lived experiences and subjective realities.37,39
Both authors, each with experience in qualitative research, participated in the analytic process. Each transcript was read and re-read multiple times to ensure deep familiarization, during which preliminary ideas and impressions were recorded. Initial codes and categories were generated from each individual transcript. Transcripts were systematically coded, and codes were then grouped together into elevated categories, based on either being too similar or by virtue of conceptually belonging to the same area. Codes were sorted into themes and overarching themes. This involved grouping some of the categories and generating new themes to better define and accommodate the scope of the categories. The themes were reviewed and discussed by all authors to determine whether any should be combined, refined, or discarded. To enhance the trustworthiness of the analysis, 40 the coding process and thematic refinements were jointly reviewed by the two authors. Disagreements were resolved through discussion and by explicitly considering potential researcher bias. The most vivid, compelling, and descriptive extracts were selected from each transcript upon unanimous agreement among the researchers regarding each theme. Ambiguities or discrepancies in interpretation were addressed collaboratively until consensus was reached. Data saturation was considered achieved when no new themes or insights emerged from subsequent interviews. 41
Researcher reflexivity
The first author is a medical psychology graduate student, and an adult child of a parent diagnosed with YOD. To minimize potential bias, she employed a transparent approach by openly acknowledging her dual role to the research supervisor, the second author. Additionally, the authors discussed the thematic analyses with each other throughout the study. Any disagreements on themes and excerpts were resolved through discussion and exploration of alternative explanations for both data and conclusions.
Results
The experiences of parents caring for an adult child with YOD were categorized into three central themes: “The Diagnosis,” “Parent-Child Relationship,” and “Assimilation Into the Caregiver Role.” These themes illustrate the progression from the initial impact of receiving the diagnosis, through shifts in the dynamics of the parent-child relationship, to a significant transformation in parental identity as caregiving responsibilities become integral to their sense of self.
The diagnosis
This theme examines the lengthy and complex diagnostic journey experienced by parents caring for an adult child with YOD, from the initial recognition of symptoms to the formal diagnosis.
A long journey to diagnosis
All parents described the period between first noticing changes in their child and receiving a formal diagnosis as lengthy and emotionally exhausting. “Several years passed before we finally received a diagnosis… I watched my son suffering… I felt helpless” (Rachel). This period was further marked by a gradual recognition of cognitive and behavioral changes, including memory impairment, aggression, mood instability, impulsivity, and disorientation. “He used to ride his bike every Friday… he told me he could no longer find his way back home” (Shira). Some parents emphasized the profound familial repercussions of undiagnosed dementia: “He was disrespectful to others, stubborn, violent, inconsiderate. As a grandfather, it was painful to see his children frightened and unable to understand what was happening to their father” (Gilad).
Challenges in providing a diagnosis
Parents described the difficulty of interpreting the initial symptoms, which were often vague and ambiguous. “I was sure his extreme behavioral change pointed to a mental illness. I urged him to see a psychiatrist” (Rachel). Others overlooked early warning signs: “For years, I noticed unusual behavioral changes, but I attributed them to the everyday challenges… I was afraid that seeking counseling would reveal an unsettling truth” (Haim). Diagnostic delays were also attributed to healthcare professionals’ limited familiarity with YOD: “We met a neurologist who was surprised by his condition. He suspected early dementia but hesitated to pursue that direction because of my son's young age and his own lack of experience” (Hanna).
Reactions to diagnosis
Several parents described experiencing a complex mix of emotions when their child's symptoms were finally explained, oscillating between shock and denial on one hand, and relief and understanding on the other. “It was a moment of shock and confusion… I felt like I had entered a whirlwind of uncertainty and anxiety” (Gilad). For many, accepting the diagnosis was fraught with resistance: “I wasn’t familiar with this disease in young adults… I told the doctors they must have made a mistake” (Tove). However, others found solace in finally having an explanation: “Receiving the diagnosis after a prolonged period of uncertainty brought a sense of relief, as it provided an explanation for my son's atypical behaviors” (Moshe).
Uncertain future
Many parents reported overwhelming feelings of hopelessness, worry, frustration, and anxiety as they grappled with escalating care demands and an uncertain future. “I’m afraid I won’t be able to cope with the physical and emotional challenges that may arise in the future” (Gilad). Financial strain compounded these burdens: “We also face financial concerns about being able to cover all the care he will require in the years ahead” (Moshe). The demands of intensive caregiving, particularly as parents themselves aged, emerged as a significant source of concern: “What is clear to us is that he must die before we do… because there will be no one to care for him after we’re gone” (Shalom).
Parent-child relationship
This theme examines the evolving parent-child dynamics in the context of YOD, emphasizing the emotional and practical challenges of prolonged caregiving. Parents’ reflections on loss reveal a narrative marked by emotional complexity, changes in communication and connection, and the profound impact of dementia on multiple aspects of their relationship.
Change in relationship. Parents described their pre-diagnosis relationship with warmth and admiration. “He was my right hand… Now I have to face my struggles alone, while also taking care of him” (Shalom). The disease reshaped these bonds, often arousing negative emotions. “Now, when I see him yelling violently at his children, I feel disgusted and afraid” (Shira). Despite these changes, several parents described efforts to maintain a sense of normalcy and continuity in their relationship. “We used to sit for hours and talk… and that's still what I do with him today” (Shay). Others used symbolic activities to maintain their emotional connection: “Sometimes we read him stories he used to love, even though it's not always clear if he understands” (Avi).
The parents’ perception of the child
Parents expressed a strong commitment to preserving their child's identity. “I feel it's my duty to mention that my son was a devoted father… he earned admiration wherever he went… Maintaining his honor is deeply important to me” (Haim). For some, focusing on their child's former self provided a sense of continuity: “That's how I preserve who he was, by keeping his former self present in our lives” (Moshe). Yet for others, reminiscing about their child's past identity evoked profound emotional distress. “It's hard, painful and heartbreaking to remember the amazing person he once was” (Yarden).
Perception of the relationship: “lifelong parenting”
All parents reported a transition from parenting an autonomous adult to caring for a dependent adult child. Many likened this transition to early parenthood: “I never imagined I’d be a mother caring for a child for so many years. Today, it feels like I’m caring for a six years old, and I fear that soon, it will feel like raising an infant” (Tove). This transformation evoked complex emotions, with five parents viewing caregiving as an imposed obligation. Rachel described feeling “chained” to her caregiving duty, while Shay expressed the burden of a responsibility he did not choose: “I am a lifelong parent… Despite all the love I have for my son, it's incredibly difficult… I didn’t ask for this.” Additionally, parents emphasized the profound sacrifice involved: “It's frustrating to raise a child with the hope that they’ll become independent, only to find yourself continually supporting them… It feels like a constant sacrifice, of my life, my desires, my dreams and my plans” (Hava).
Assimilation into the caregiver role
This theme examined how parents assimilated into the caregiver role following a YOD diagnosis, highlighting significant shifts in their personal identities as well as the profound emotional and practical challenges associated with caregiving.
Carers’ impact
As caregiving responsibilities intensified, parents became increasingly aware of the overwhelming physical and emotional weight of their role. Many neglected their own health, experienced chronic stress, and faced compounding burdens, especially in old age. As Shira shared, “I don’t find the time to take care of myself.” Similarly, another parent shared, “Unfortunately, I was diagnosed with chronic arthritis as a result of physical strain from caring for my son” (Moshe). The burden often extended to marital relationships: “My relationship with my husband has changed… We only talk about our son, it feels like we have lost our relationship” (Hava). Others emphasized chronic stress and social isolation: “I found myself increasingly stressed and isolated from those around me… unable to share what I’m experiencing with others” (Shay).
New needs
Parents expressed a strong need for accurate and accessible information. “From the first moment we received the diagnosis until today, I’ve felt that I don’t have enough knowledge about the disease… I know this affects my ability to provide my child the care he deserves” (Gilad). While all parents emphasized the importance of formal caregiving support, some experienced emotional conflict when seeking help. “I searched for a formal caregiver to assist with the physical care. It was difficult for me to let someone else share my caregiving responsibilities… It felt like I had failed as a mother” (Yarden). Additionally, many identified emotional support as a critical yet unmet need: “I feel like I’m going crazy… Sometimes I just want to call someone who's been through the same thing, just to unload and hear that I’ll be okay” (Shira).
A prolonged experience of grief
Parents described a profound and ongoing sense of loss as they watched the disease progress. “This disease progresses so slowly, every day, I witness a small change… every day I feel the sadness of that loss all over again” (Gilad). The complexity of their grief stemmed from mourning a child who was still physically present: “I’m constantly in conflict with myself, I feel like I’m mourning my son, but there's no space for that grief… He's still physically here, but he's no longer the son I once knew” (Shira). Shay compared the experience to witnessing a loved one's death: “It's like watching someone die and being completely powerless.” For some, this sense of loss led to profound disconnection. As Shalom reflected, “He is sitting there in his chair, and I realize this is no longer the son I raised… I only see his body sitting there.”
Adjusting to the caregiver role: who am I today?
Caregiving prompted parents to deeply reflect on their sense of self as parents. “I feel a tremendous sense of responsibility, accompanied by the feeling that I am fulfilling my purpose” (Haim). Similarly, other parent shared, “I feel that this is my calling, especially in the moments when he is calm” (Avi). For some, caregiving also revealed inner strengths: “I’ve discovered strengths I never knew I had” (Moshe). However, for several mothers, caregiving profoundly disrupted their sense of maternal identity. “I take care of my son, and I feel intense emotions such as disgust, disappointment, frustration, and anger directed at him. Then I think, what kind of mother am I?” (Hava). Rachel echoed these struggles: “I feel ashamed and guilty that I have no patience or compassion left for my son… Sometimes I think I don’t deserve to be called a mother.” In contrast, for others, caregiving reinforced and deepened their sense of maternal identity. “From childhood, I knew I would feel complete as a mother… I feel a deep sense of fulfillment and satisfaction when I’m able to help” (Hanna).
Discussion
In the present study, participants were Israeli parents of an adult child diagnosed with YOD. The progressive nature of the disease was evident in the parents’ narratives, highlighting the evolving dynamics of their experiences. The first theme, “The Diagnosis,” served as the foundation upon which their experience of loss was constructed. The second theme, “Parent-Child Relationship,” highlights the profound shifts in emotional connection and identity that shape parents’ evolving experience of loss. The third theme, “Assimilation Into the Caregiver Role,” represented the ongoing nature of loss and the process of adapting to altered form of parenthood.
Eternal parenthood
The extraordinary circumstances surrounding YOD caregiving evoked profound emotional strain among parents. As their child's condition worsened, parents faced overwhelming feelings of confusion, grief, and frustration, often intensified by a pervasive sense of powerlessness in the face of their child's suffering. These findings are consistent with existing literature, which indicates that the prolonged trajectory of dementia, progressive cognitive decline, and heightened emotional distress significantly contribute to caregiver burden. 42 While such emotional responses are common among dementia caregivers, recent studies highlight the value of cognitive coping strategies, such as reframing negative thoughts and focusing on small positive moments-in reducing psychological distress. 43
The emotional burden experienced by parents was further compounded by the ways in which caregiving for an adult child with YOD challenged traditional conceptions of parenting. Traditionally, parenthood is framed within the context of raising young children, with the expectation that as children grow older, they mature, assume responsibility, and become independent.44,45 In parallel, parents age and eventually retire from active caregiving roles. However, for parents in this study, this normative trajectory was fundamentally disrupted. Rather than witnessing the sustained independence typically associated with midlife, parents observed a regression in their child's autonomy as a consequence of the disease. Their adult child became progressively more dependent on them, emotionally, cognitively, and physically.
This reversal aligns with the concept of the “eternal parents”, 46 wherein the parental role extends indefinitely and often intensifies over time. This shift profoundly impacted daily life, as parents found themselves engaging in routines reminiscent of early parenthood, providing constant supervision, emotional support, and hands-on care. Unlike early parenthood, which is typically marked by growth and a gradual reduction in care requirements, this experience was characterized by ongoing deterioration and escalating demands, resulting in a persistent and challenging caregiving reality.
Within this reality, some parents construed caregiving as an inherent extension of their parental responsibilities, framing devotion to family as a central component of their identity. For these individuals, the fulfillment of such obligations often engendered a sense of pride, continuity, and belonging, allowing them to reinterpret the caregiving role as meaningful despite its inherent challenges. Simultaneously, however, they recognized the profound personal costs associated with caregiving, including reduced social engagement, financial strain, and the deterioration of their own physical and emotional well-being. For others, adherence to ideals of parental self-sacrifice intensified a sense of ambivalence, as these ideals not only sustained commitment but also amplified guilt and perceived inadequacy when patience, compassion, or physical endurance faltered under the cumulative pressures of caregiving.
This sense of ambivalence must be understood within the broader sociocultural context of Jewish Israeli society, which integrates elements of modern Western individualism with enduring traditional, religious, and cultural commitments to family life. Within this cultural framework, parenthood is not only associated with the responsibility of providing care but is also closely linked to personal achievement, marital fulfillment, and the preservation of lineage.47–49 Although Jewish Israelis place significant value on independence and individual self-realization, paralleling patterns characteristic of American middle-class culture, 50 these ideals coexist with deeply embedded collectivist norms that elevate loyalty, devotion, and self-sacrifice within the family unit. Consequently, the parents in this study were required to negotiate their caregiving within a field of competing cultural imperatives. On the one hand, as older adults they aspired to autonomy and to the cultivation of a normative life stage associated with later life, which is conventionally perceived as free from the obligations of active parenting. On the other hand, they remained bound by a profound moral commitment to provide continuous and selfless care for their children.
Caregiving dissonance
The caregiving role often created profound tension for parents, as their unconditional love and commitment to their child coexisted with feelings of sorrow, frustration, and at times, even disgust, particularly as they witnessed the disorienting erosion of their child's identity. This emotional conflict exemplifies the concept of ambivalence, the simultaneous experience of opposing feelings, as highlighted in caregiving literature. 51 Ambivalence was further intensified by the perception that caregiving was an imposed obligation rather than a choice. One parent described feeling “chained” to these duties, a metaphor that captures the confining and inescapable nature of their daily reality.
As the disease progressed, parents experienced the unique pain of mourning someone who remained physically present but was no longer emotionally or cognitively accessible. This experience, known as ambiguous loss, leaves caregivers suspended in a state of unresolved grief. 14 This ambiguous loss erodes shared memories and weakens emotional bonds, 52 making it difficult for parents to reconcile their child's current state with memories of who they once were. In response, parents adopted coping strategies aimed at preserving continuity and connection. Some maintained shared routines or revisited meaningful activities from the past, while others focused on emphasizing their child's pre-illness traits and values to sustain a sense of emotional closeness. These findings align with research suggesting that maintaining a positive narrative about the person with dementia can support caregivers and help reduce emotional strain. 53
Through the development and application of coping strategies, many parents cultivated a distinct caregiver identity characterized by resilience, competence, and emotional fulfillment. For these individuals, caring for an adult child with YOD was not perceived merely as a set of burdensome obligations, but rather as a meaningful role that provided purpose and reaffirmed their capacity to express love, protection, and commitment. Within their narratives, caregiving was frequently represented as an opportunity to embody deeply held values of devotion, responsibility, and moral duty, resonating with cultural ideals such as filial piety. This reframing underscores how the caregiving relationship, despite its considerable demands, could simultaneously nurture a strengthened sense of self and affirm the moral worth of caregivers’ actions. Similar positive dimensions of caregiving within family contexts have been identified in several studies conducted in Western societies. 54 Although such perspectives remain relatively underrepresented, they offer valuable insight into the multidimensional character of parental caregiving in YOD, drawing attention to its capacity to encompass affirming as well as challenging experiences. Acknowledging these voices is crucial, as their scarcity may reflect not only the lived complexities of caregiving but also the impact of social and cultural norms that discourage open expression of its positive dimensions.55,56
Nevertheless, this positive adaptation was not shared by all parents. For some mothers, the unremitting demands of caregiving for an adult child with YOD generated a profound rupture in their maternal identity. In these cases, traditional ideals of motherhood, emphasizing patience, compassion, and emotional availability, were continually strained by the psychological and physical burden of attending to a child whose personality had become unfamiliar and unrecognizable. Within this context, the caregiving role frequently elicited intense negative emotions, including anger, frustration, and even aversion. When directed toward their child, these affective responses often provoked feelings of guilt, shame, and self-doubt, leading mothers to critically question their moral adequacy as caregivers. These findings resonate with existing research suggesting that individuals prone to shame are more likely to engage in harsh self-criticism and to internalize a sense of personal defectiveness, thereby impeding the development of self-compassion and self-acceptance. 57 Over time, such cycles of self-directed negativity may intensify psychological distress. 58
These struggles highlight the precariousness of maternal identity when deeply ingrained cultural expectations collide with the lived realities of dementia caregiving. Importantly, the findings must be situated within the broader sociocultural discourse of “good mothering,” which remains particularly salient in Israeli society while also reflecting dominant ideals across many Western contexts. 59 Within this cultural framework, maternal identity is frequently equated with self-sacrifice, unconditional giving, and the prioritization of children's needs above personal well-being. Consequently, the mothers in this study were burdened not only by the emotional and practical challenges of caregiving but also by the internalized imperative to embody the ideal of the ever-giving mother, even when such enactment entailed profound personal costs. This enduring tension can be understood through the lens of identity non-verification, wherein distress arises when role-related behaviors are perceived as inconsistent with one's internalized self-concept, thereby generating emotional instability, identity strain, and, in some cases, transformations in self-definition. 60
Dementia grief model
The experiences of parents can be conceptualized as comprising two interrelated processes: the loss of the child they once knew and the subsequent transformation of their parental identity. These processes are well captured by the DGM. 22 The “separation” state began when parents first recognized changes in their child's personality and cognitive functioning. This recognition marked a pivotal turning point, initiating a gradual and painful process of losing the child they once knew. For some parents, receiving a formal diagnosis provided clarity and validation, enabling them to begin confronting and acknowledging the depth of their loss. Others, however, responded with denial and resistance, defensive reactions that risked stalling their progress in this state and hindering their ability to fully acknowledge the loss.
The “liminality” state emerged as the disease progressed and caregiving demands intensified. During this phase, parents grappled with the stark contrast between their child's pre-illness identity and their current condition, a reflection that extended to the shifting dynamics of the parent-child relationship. Parents endured profound uncertainty and ambiguity, caught between their former parental role and the evolving demands of caregiving. This ambiguity often gave rise to emotional ambivalence, as parents oscillated between unconditional love for their child and the difficult emotions elicited by caregiving and the symptoms of the disease. Nevertheless, by acknowledging and articulating these complex emotions, some parents demonstrated a willingness to confront their loss, which enabled the grieving process to unfold.
Finally, the “re-emergence” state marked a period of adaptation and acceptance for some parents. Several parents began to recognize their own limitations, particularly those related to aging, and sought external support to address their child's changing needs. Some demonstrated resilience by tolerating and processing the emotional challenges of caregiving, which facilitated the reconstruction of a renewed parental identity through psychological adaptation. However, others remained anchored in rigid self-concepts, which contributed to a fragmented sense of identity and unresolved questions about their new role as parents.
Applying the DGM to the parental experience of YOD highlights the need for interventions that address parents’ evolving psychological challenges throughout dementia-related grief. To effectively address these challenges, healthcare professionals should prioritize early diagnosis and provide clear information and practical guidance to reduce confusion and distress, enabling parents to better support their child and develop adaptive coping strategies. Mental health professionals should provide empathetic, individualized therapy that acknowledges caregivers’ unique needs and helps challenge unhelpful internalized beliefs. When caregivers struggle with maladaptive narratives rooted in guilt or self-blame, therapeutic interventions should focus on reshaping these narratives to foster a healthier self-concept. As Montgomery and Kosloski 61 suggest, cultivating present-focused awareness can enable caregivers process ongoing losses, reconstruct meaning, and adapt their identities. In addition, Given the rarity of this caregiver group, tailored support groups are especially valuable. These groups enhance knowledge, well-being, and caregiving skills, while fostering a sense of community and reducing isolation.62,63 Group therapy, therefore, offers essential solidarity and practical support for parents navigating the unique complexities of caregiving.
This study offers a distinctive scholarly contribution by examining the experiences of parents providing care for an adult child with YOD in Israel, thereby addressing a caregiving population that has been largely neglected in existing research. While prior studies have predominantly concentrated on spouses, children, and siblings, the unique challenges encountered by parents of adult children with YOD have remained comparatively overlooked. By foregrounding this group, the study confronts a critical research gap and extends the conceptual boundaries of informal caregiving scholarship. The findings challenge the prevailing assumption that parental responsibilities diminish or cease once children reach adulthood, demonstrating instead that YOD disrupts normative life-course trajectories and reimposes intensive parenting obligations at a late stage in life. Interpreted through the theoretical lenses of ambiguous loss, dementia grief models, and identity strain, these findings illuminate the complex processes through which parental caregiving is reframed under conditions of chronic illness. In doing so, the study underscores the urgent need for policies and interventions that address the vulnerabilities of aging parents, who must navigate the dual burden of supporting the regression of an adult child with YOD while simultaneously coping with their own aging. This underexplored dynamic highlights the importance of developing culturally sensitive, intergenerational approaches to dementia care.
Building upon these contributions, the study also carries broader implications for theory, practice, and policy. The findings suggest that existing models of dementia-related grief require refinement to more fully capture variations across caregiver roles and life stages. From a practical perspective, the results emphasize the necessity of interventions specifically tailored to the circumstances of older parents, including psychoeducational programs, support groups, and therapeutic approaches that directly address the prolonged parental role, identity disruption, and the compounded strain of caregiving in later life. At the policy level, the study underscores the importance of formally recognizing non-normative caregiver populations within health and welfare systems, and of expanding support services, respite opportunities, and financial assistance for parents of dependent adult children. More broadly, the findings point to the need for culturally sensitive frameworks that acknowledge the pervasive influence of familial devotion and parental sacrifice in shaping caregiving experiences in Israel and comparable societies. Taken together, these insights call for a more inclusive conceptualization of dementia caregiving, offering critical direction for future research, clinical interventions, and policymaking.
The present study should be considered within the context of its limitations. First, the participant sample comprised solely parents of adult children diagnosed with YOD, specifically within the clinical subtypes of FTD and DLB. As a result, the study does not capture the broader spectrum of caregiving experiences associated with other forms of YOD or neurodegenerative conditions. The distinct cognitive and behavioral manifestations characteristic of FTD and DLB may have shaped parental caregiving experiences in ways that are not generalizable to caregivers of individuals with other dementia etiologies. Second, the interview guide did not include a direct question about positive caregiving experiences, which may have limited the opportunity for such themes to surface. The scarcity of positive narratives may also reflect social desirability bias or broader cultural taboos surrounding open discussion of dementia care. Future studies would therefore benefit from incorporating interview prompts that intentionally elicit both affirmative and challenging dimensions of the caregiving experience.
Additionally, the study did not examine potential gender-based differences in caregiving, which could have provided important insights into variations in burden, coping strategies, and relational dynamics. A further limitation pertains to the recruitment strategy, which relied heavily on internet forums. This method may have disproportionately excluded caregivers who are older, less technologically connected, or less active on digital platforms. Consequently, the sample may not adequately represent the full diversity of caregiving perspectives, thus narrowing the generalizability of the findings. Future research should therefore employ more diversified recruitment strategies, such as outreach through healthcare providers, community centers, and caregiver organizations, in order to broaden participation and enhance representativeness. Finally, further investigation is warranted to design, implement, and evaluate therapeutic interventions specifically tailored to the distinctive challenges of parental caregivers.
Conclusion
The present study highlights the multifaceted challenges faced by parents who provide care for an adult child diagnosed with YOD, underscoring the profound emotional, physical, and relational repercussions of this role. Findings indicate that these parents endure a prolonged and evolving sense of loss as the disease advances, often marked by the gradual dissolution, and, at times, renegotiation, of parental identity. By foregrounding the narratives of parents of adult children with YOD, the study brings visibility to a population largely neglected within the existing body of dementia caregiving scholarship. In documenting how older parents contend with the enduring continuation of parental responsibilities, disruptions to self-concept, and the burden of culturally embedded ideals of parenthood, the research addresses a critical empirical and theoretical gap. It further contributes to broader discussions on ambiguous loss, dementia-related grief, and identity strain. Crucially, the findings underscore the pressing need for tailored psychosocial interventions and culturally responsive support systems designed for this specific caregiving group. Future research should continue to prioritize their perspectives while also advancing public and institutional recognition of their distinct challenges, thereby informing therapeutic, social, and policy frameworks that more effectively meet their multidimensional needs.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The study received ethical approval from the institutional review board of the institution with which it is affiliated (number: 272).
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.