
Abstract
Background
Alzheimer's disease and other dementias are major causes of disability and death among older adults. With an increasing number of older migrants in Italy, dementia prevalence in this group is expected to rise. However, little is known about their health outcomes.
Objective
This study aimed to analyze mortality in migrants with dementia in Lazio, Italy, as part of the ImmiDem project (GR-2021-12372081).
Methods
A cohort study was conducted on individuals aged ≥50 with dementia living in Lazio as of December 31, 2018, who were followed for 5 years. Migratory status was defined by country of birth: native Italians, migrants from High Migratory Pressure Countries (HMPCs), or Highly Developed Countries (HDCs). Age-standardized mortality proportion was calculated by migratory status, and time-to-event analysis was performed using Cox regression models.
Results
As of December 31, 2018, 38,380 individuals with dementia lived in Lazio, with 2.1% born in HMPCs and 0.9% in HDCs. The age-standardized mortality proportion was lower in migrants born in HPMCs (30.7%; 95% CI: 26.4–35.8) than among natives (36.8%; 95% CI: 35.4–38.4). The age- and sex-adjusted hazard ratio (HR) confirmed lower mortality in migrants (HMPCs HR = 0.91, 95% CI:0.82–1; HDCs HR = 0.79, 95% CI:0.68–0.91) than natives.
Conclusions
Migrants with dementia showed lower mortality than Italians, possibly due to health advantages, salmon bias, or migration dynamics. However, these findings may not accurately reflect better health status. Potential underdiagnosis of dementia and the use of country of birth as a proxy for migratory status may have influenced results and should be considered in future research.
Introduction
Dementia is the eighth leading cause of death globally, with an age-standardized mortality rate of 25.2 (uncertainty intervals [UIs] 6.4–65.6) per 100,000 people. 1 In Italy, the age-standardized mortality rate is slightly higher than the global estimate, reaching 29.8 (UIs 8.1–72.9) deaths per 100,000 individuals in 2021. 1 Dementia prevalence increases with age and, due to population aging, is expected to rise further in the coming decades. These projections apply to all population groups, including international migrants (i.e., people living in a country but born abroad), experiencing an unprecedented increase in their life expectancy. 2 However, they are growingly facing the burden of aging-related diseases, including cognitive disorders.3,4 Disaggregated data by migratory status are essential for understanding the impact of dementia on migrants and for informing targeted public health policies.
In 2019, nearly 475,000 dementia cases were estimated among migrants aged 65 or more living in Europe using population-based age- and sex-standardized prevalence rates. 5 The median proportion of dementia cases occurring in migrants was 7% (IQR 7.6%, ranging from 0.9% in the Czech Republic to 51.2% in Liechtenstein). 5 Nearly 26,000 cases were estimated in the migrant population in Italy, accounting for 2.3% of overall dementia cases. 5 Beyond these simulations, some national and international surveys have documented an increase in the number of migrants accessing dementia services due to cognitive disturbances.6,7
Previous studies have compared dementia prevalence between migrants and their native counterparts in host European countries. 8 Population-based surveys generally showed higher dementia prevalence in migrants compared to reference populations while most registry-based studies reported lower prevalence rates among migrants. We recently investigated dementia prevalence among older adults living in the Lazio region (Italy) based on health information systems. The age-standardized prevalence of dementia was 7 (95% CI 6.3–7.8) per 1000 among migrants who were born in Highly Developed Countries (HDCs) and 5.9 (95% CI 5.5–6.4) per 1000 among migrants from High-Migratory Pressure Countries (HMPCs). The prevalence was notably higher in Italian natives (9.2, 95% CI 9.1–9.3 per 1000). 9 Such a discrepancy between population-based and health record surveys has been interpreted as a combined result of poorer access to healthcare and a higher risk for dementia underdiagnosis in migrants.
Conversely, there is still a dearth of evidence concerning the health outcomes of migrants with dementia. Gaining insights into the health trajectories of this growing population of individuals is crucial for improving care provision and designing inclusive care pathways, with the ultimate goal of reducing health disparities. It may be hypothesized that migrants with dementia are exposed to a higher risk of unfavorable health outcomes (including mortality) due to lower access to healthcare resources and poorer social support.
Based on these premises, the present study aimed to investigate mortality in migrants living with dementia in the Lazio region relative to Italian-born patients. This analysis is part of the ImmiDem project, which seeks to explore the magnitude and challenges of dementia among migrants from clinical and public health perspectives 10 (GR-2021-12372081).
Methods
Study design and population
This study was conducted according to a population-based cohort design. The study protocol was approved by the Ethics Committee of the Italian National Institute of Health (Protocol 0017082; 6 April 2023). Individuals aged 50 years or older affected by dementia, living and residing in the Lazio Region, and receiving care from the Lazio Regional Health Service (RHS) on 31 December 2018 were included in the cohort. They were followed up for five years to study the association between migratory status and all-cause mortality. The follow-up was censored in cases of death (the event of interest), end of assistance by the Lazio RHS (considered lost to follow-up), or at the end of the study.
Setting
Lazio is a region in central Italy including the city of Rome. As of the end of 2018, it had a total population of 5,879,082 residents, of which 2,538,631 were aged 50 or older. The overall proportion of migrants was approximately 11.6%. For people aged 50 years or older, the proportion is 5.9%. 11
Variables of interest
The outcome variable was all-cause mortality. The primary exposure of interest was the migratory status, which was categorized according to the country of birth, regardless of legal status, reasons for migrations, and length of stay in Italy. 12 Based on this approach, participants were classified as i) native Italians, ii) migrants from HDCs: Western Europe, North America, Oceania, Israel, and Japan, and iii) migrants from HMPCs: Central and Eastern Europe, Central and South America, Northern Africa, Sub-Saharan Africa, Central and Western Asia (excluding Israel), and Eastern Asia (excluding Japan). 13 –15 A detailed classification of countries is reported in the Supplemental Material (Supplemental Table 1).
Demographic (age and sex) and clinical features (comorbidities and medication use) were included in the descriptive analyses and the adjusted models as potential confounders. Moreover, their role as effect modifiers was investigated.
Data sources
The primary data source for identifying the study population was the Regional Health Assistance database, which includes all individuals registered with a general practitioner and therefore covered by the RHS. Information about age, sex, country of birth, and the date of the last recorded assistance by the RHS (serving as right-censoring for those lost to follow-up) was obtained from this database.
To confirm eligibility for the study cohort, we established the diagnosis of dementia using a previously published and applied algorithm.9,16 Individuals were classified as affected by dementia if they met at least one of the following criteria: 1) at least one hospital discharge between 2014 and 2018 recorded in the Hospital Information System with a primary or secondary diagnosis of dementia, identified using codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM); 2) they received at least two consecutive prescriptions within one year for reversible acetylcholinesterase inhibitors and N-Methyl-D-Aspartate receptor antagonists during the previous five years, as reported in the Pharmaceutical Prescriptions Database using codes from the Anatomical Therapeutic Chemical (ATC codes); 3) they were entitled to an exemption from healthcare co-payment due to Alzheimer's disease or other dementia recorded in the Co-payment Exemption Registry before the enrolment date of December 31, 2018.
The presence of comorbidities was determined using data obtained from the Hospital Discharge Registry, covering the two years preceding the enrollment date (Supplemental Table 4).
Data on antidementia drugs and antipsychotics drugs, prescribed in the same two-year period, were also obtained, and categorized using the Pharmaceutical Prescriptions Database according to the ATC codes (Supplemental Table 5). Information about death for any cause was obtained from the regional mortality registry.
Finally, for individuals residing in Rome, the information regarding citizenship available in the registry archive of the Municipality of Rome was used to conduct a subgroup analysis in which migratory status was no longer assigned based on the country of birth but rather on citizenship.
Statistical analyses
The cohort was described using frequencies and percentages for variables such as country of birth, demographic characteristics (age and sex), and clinical features (comorbidities and medication use). These characteristics were analyzed both overall and stratified by migratory status to highlight potential differences between groups.
Comparisons across migratory status groups were performed using the chi-squared (χ²) test. This approach allowed assessment of the statistical significance of observed differences in categorical variables across groups.
To account for potential confounding by age and sex, logistic regression models were fitted to assess the association between migratory status and the prevalence of comorbidities and medication use. These models were adjusted for age and sex to isolate the effect of migration background on health-related variables.
Crude and age-standardized all-cause mortality proportions were calculated according to migratory status. The proportions were computed as the number of deaths during the follow-up period divided by the number of individuals at risk as of 31 December 2018, with age standardization based on the 2018 population structure of the Lazio region.
Time-to-event analyses were carried out to explore the association between migratory status and all-cause mortality. Kaplan-Meier survival curves were generated for the three migratory groups and compared using the log-rank test to assess differences in survival probabilities.
Subsequently, multivariate Cox proportional hazards models were developed to estimate hazard ratios (HRs) for mortality, adjusting for sex and age classes. These models helped quantify the relative risk of death associated with different migratory statuses while controlling for key demographic variables.
Censoring occurred at the earliest of three events: date of death, date of the last recorded health service assistance (indicating loss to follow-up), or the study end date (31 December 2023). Institutionalized individuals were included unless they had been institutionalized outside the region or abroad, as these cases would result in deregistration from the Regional Health Service (RHS).
Descriptive analyses were also performed for individuals lost to follow-up to understand their baseline characteristics. This helped evaluate the potential for attrition bias in the time-to-event analyses.
Finally, to assess whether the effects of migratory status varied by age or sex, interaction terms were included in the final regression model. Statistical significance of these interactions was tested to determine if stratified analyses were warranted.
Subgroup analysis
To give strength to the results and address the assignment of individuals to their respective migratory status categories, the analyses performed on the whole study population were repeated, focusing exclusively on the subgroup of individuals residing in Rome. For this subgroup, migratory status was assigned based on citizenship as recorded in the municipal registry of Rome rather than on country of birth.
Results
A total of 38,380 individuals aged 50 years or older living and receiving care in Lazio were identified as having dementia and considered for the present analysis. Among them, the majority were Italian natives (97%), 2.1% were migrants from HPMCs, and 0.9% were migrants from HDCs (Table 1).
Demographic and clinical characteristics of participants by migratory status (31 December 2018).
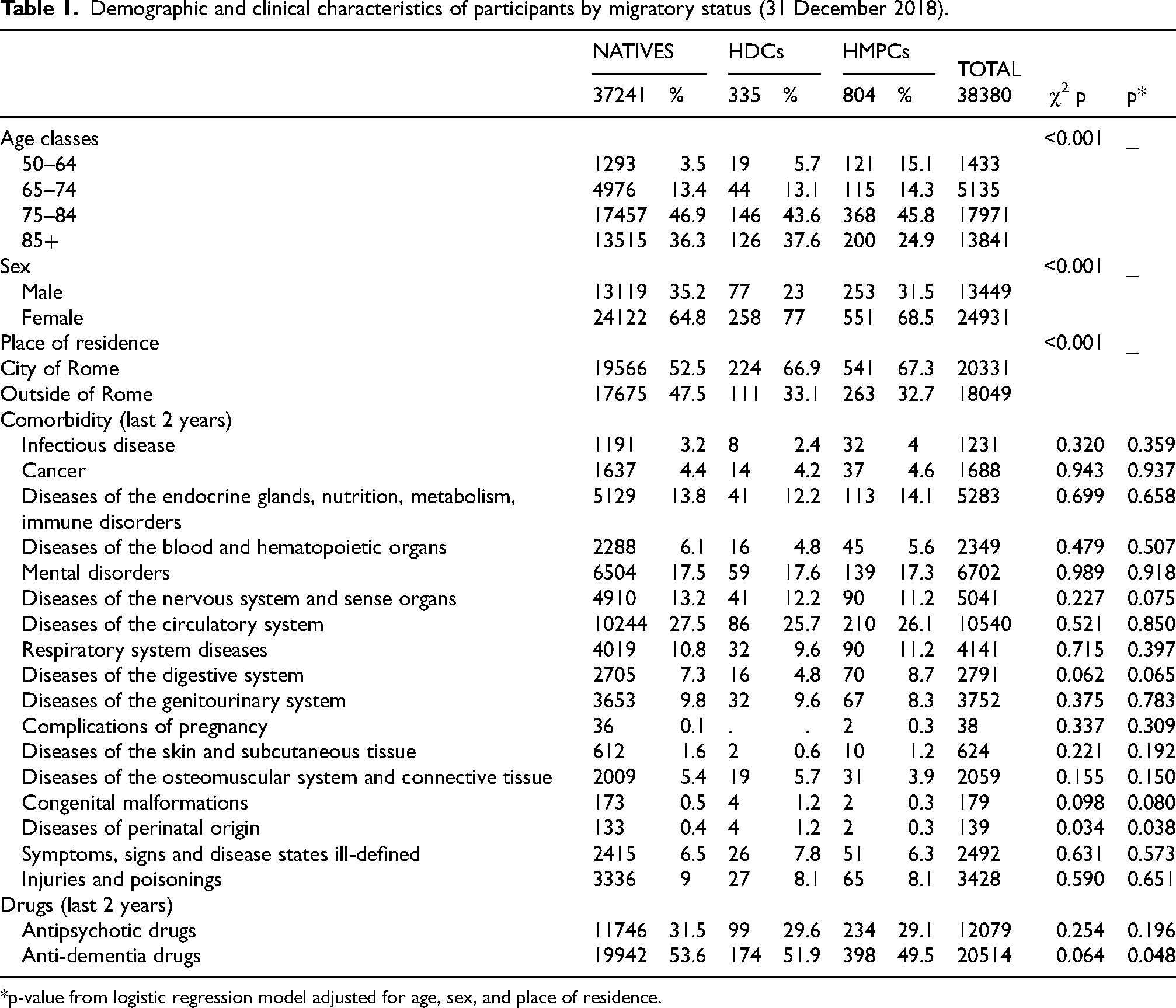
*p-value from logistic regression model adjusted for age, sex, and place of residence.
The majority of overall migrants living in Lazio were born in Romania, followed by the Philippines, Ukraine, and Libya (Figure 1(a)). Among migrants affected by dementia, the most represented countries of birth were Libya, Tunisia, and France (Figure 1(b)). Among migrants from HMPCs, the most common countries of birth were Libya, Tunisia, and Egypt, while those from HDCs primarily originated from France, Spain, and the United States (Figure 1(b)). Overall distributions are reported in the supplemental material (Supplemental Table 3).
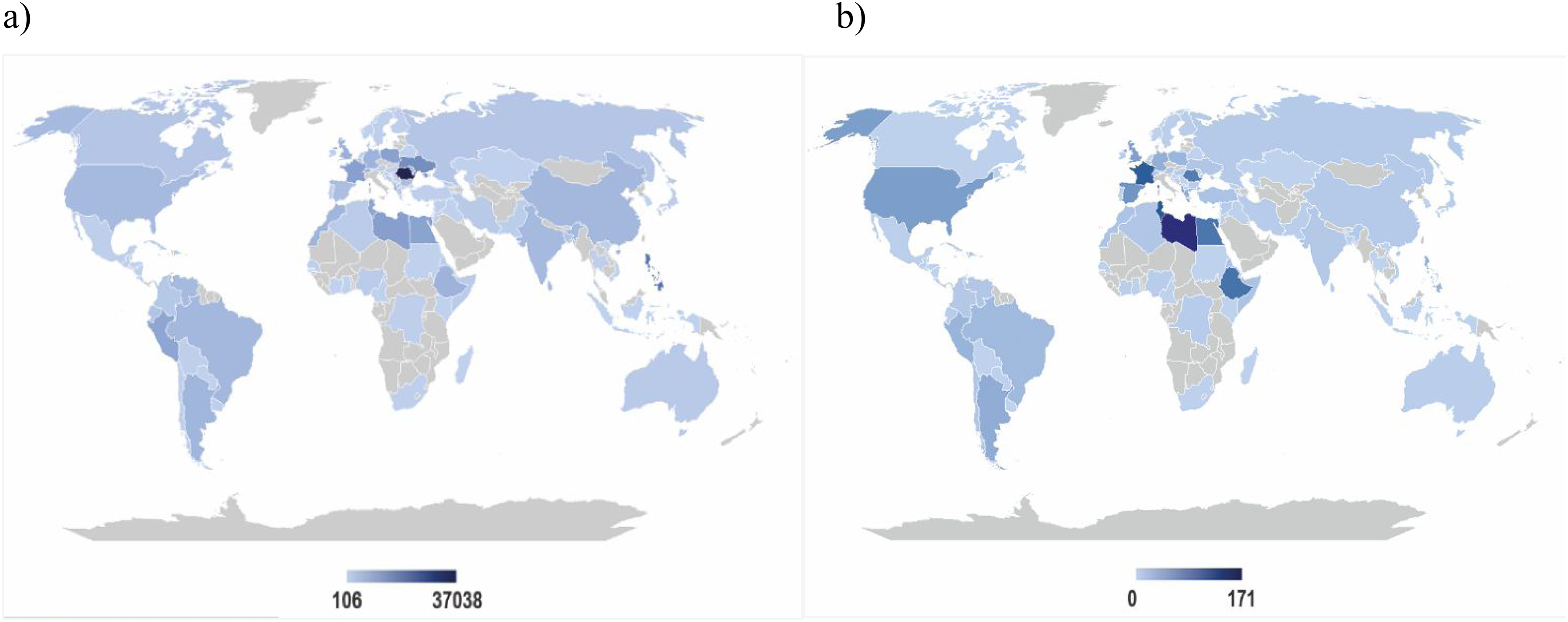
Case distribution maps by country of birth: a) all 50 + migrants living in Lazio and b) 50 + migrants with dementia living in Lazio (31 December 2018). Panel a shows the distribution (absolute frequency) of all migrants residing in Lazio by country of birth. Panel b shows the distribution (absolute frequency) of migrants with dementia residing in Lazio by country of birth. HDCs: Western Europe, North America, Oceania, Israel, and Japan; HMPCs: Central and Eastern Europe, Central and South America, Northern Africa, Sub-Saharan Africa, Central and Western Asia (excluding Israel), and Eastern Asia (excluding Japan).
In terms of demographic characteristics, a higher percentage of younger individuals and women were observed in migrants with dementia relative to natives. In addition, migrants exhibited a lower use of anti-dementia medications. No differences in comorbidities were observed among the three groups, except for diseases of perinatal origin (ICD-9 codes 760–779; p = 0.038). This difference may reflect variations in early-life diagnostic practices, neonatal survival, and health system reporting, rather than true differences in disease prevalence.
On the other hand, a statistically significant difference emerged in the use of anti-dementia drugs over the previous two years, with a higher percentage of use among natives compared to migrants (Table 1).
The age-standardized mortality proportion was higher among native Italians (36.8 per 1,000, 95% CI 35.4–38.4) and migrants from HDCs (38.5 per 1,000, 95% CI 22.2–67) compared to migrants from HMPCs (30.7 per 1,000, 95% CI 26.4–35.8), who exhibited a 17% lower 5-year mortality risk compared to native Italians (Table 2).
Crude, age-standardized mortality proportion and relative risk by migratory status (31st December 2023).
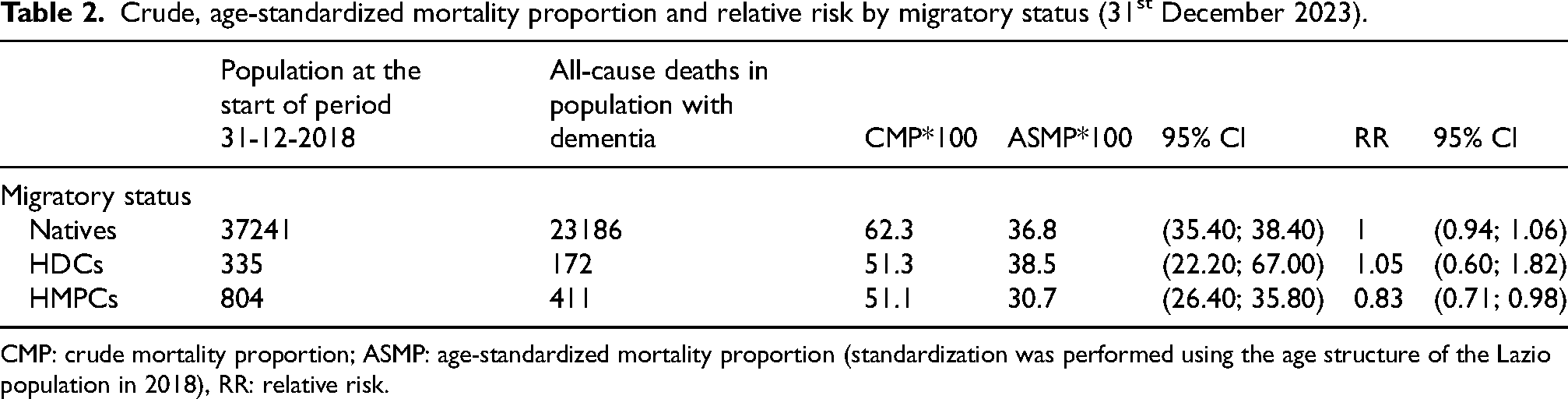
CMP: crude mortality proportion; ASMP: age-standardized mortality proportion (standardization was performed using the age structure of the Lazio population in 2018), RR: relative risk.
At the end of the study, 809 (2.2%) individuals were lost to follow-up, 787 (2.2%) among natives and 22 (2%) among migrants. Supplemental Table 6 shows descriptive characteristics of these study participants.
Lower mortality among migrants is graphically represented by the Kaplan-Meier curves (Figure 2) and confirmed by the multivariate Cox analysis, adjusted for sex and age group (Table 3).
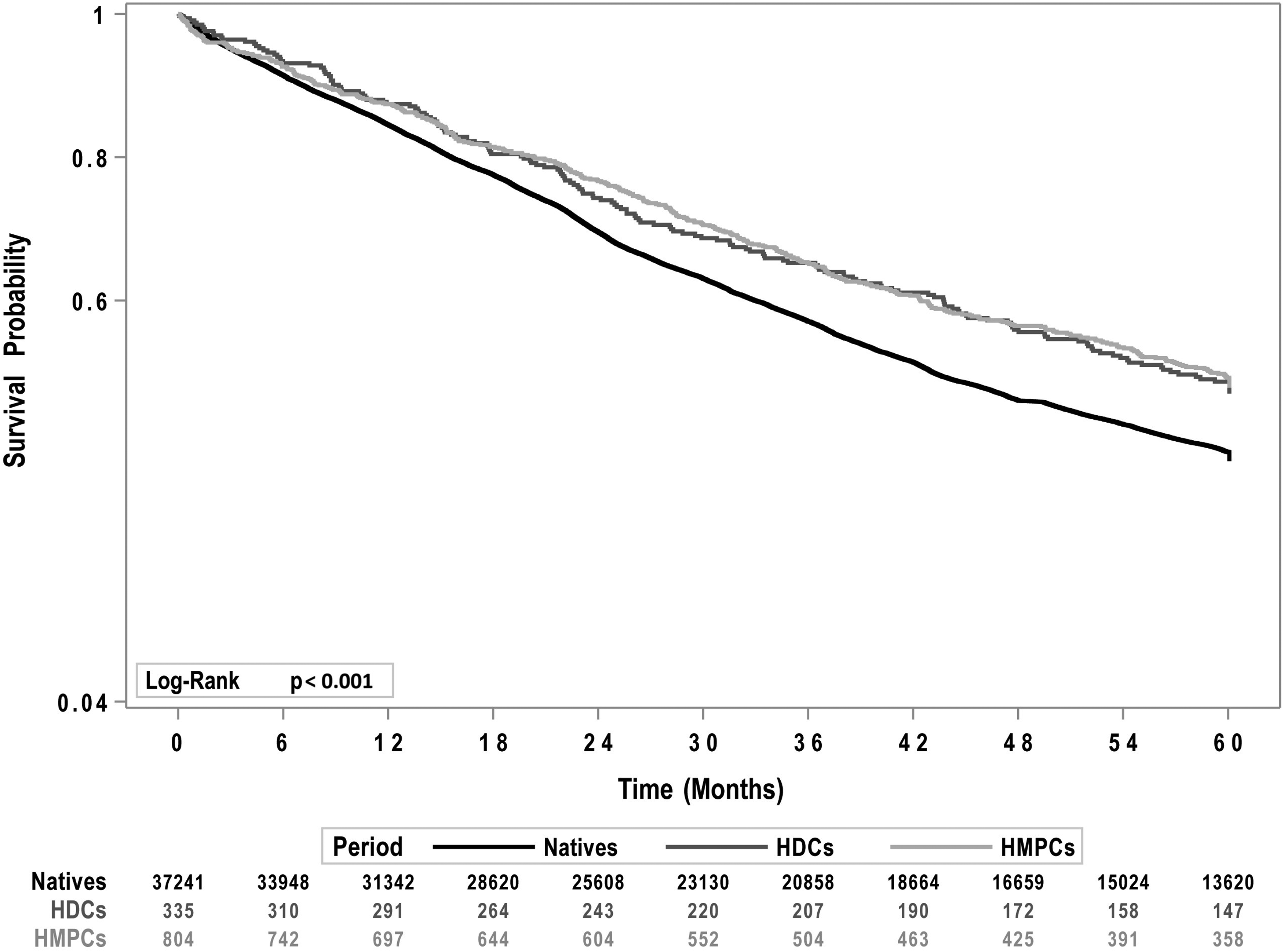
Kaplan-Meier curves by migratory status (31 December 2023).
Age and sex-adjusted cox regression analysis (31 December 2023).
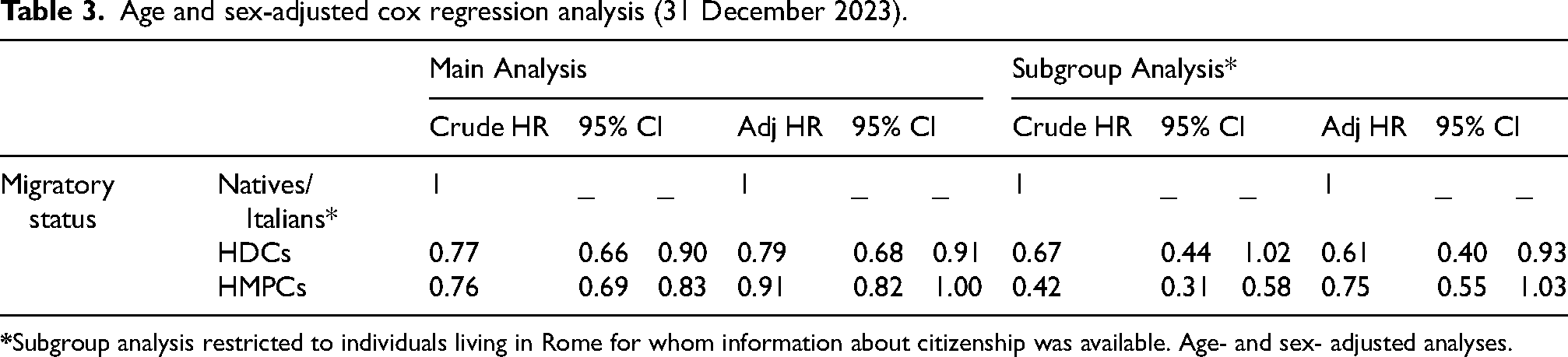
After controlling for age and sex as confounding factors, the Cox model showed that migrants had lower mortality compared to Italians: a 21% reduction (HR = 0.79, 95% CI: 0.68–0.91) for those from HDCs, and a 9% reduction (HR = 0.91, 95% CI: 0.82–1) for those from HMPCs (Table 3). Sex and age did not appear to be effect modifiers in the association between migratory status and mortality.
The subgroup analysis, restricted to individuals living in Rome for which information about citizenship was available, showed results similar to those from the main analyses (Table 3, Supplemental Tables 7 and 8, and Supplemental Figures 1 and 2).
Discussion
To investigate the relationship between migratory status and mortality in patients with dementia, we conducted a registry-based cohort study with a five-year follow-up of 38,380 older individuals living in the Lazio region. Our results indicated that migrants (defined as foreign-born individuals) had lower mortality compared to their native counterparts, even after adjusting for age and sex, seemingly disconfirming the original hypothesis of poorer health outcomes among migrants. These findings were further supported by subgroup analyses that focused on individuals living in Rome and used citizenship as a criterion to define migratory status.
To the best of our knowledge, the present study is the first attempt to explore mortality in migrants with dementia at a population level. Indeed, previous analyses on the topic have mostly focused on ethnic minorities, thus embracing migrants but also their descendants, who may or may not have been born in their current country of residence. Concerning European countries, a previous study of a nationwide cohort of 55,827 hospitalized patients in the Netherlands did not reveal any significant difference in short-term (1-year) and long-term (3-year) mortality between native Dutch and ethnic minority patients. 17 In the United Kingdom, two studies found that mortality rates in patients with dementia from ethnic minority groups (i.e., Asians and Non-Whites, respectively) were lower compared to those of White individuals.18,19 Conversely, a third UK-based study failed to confirm these results. 20 A meta-analysis of 17 studies conducted in the United States documented differences in overall survival and mortality among individuals with dementia from ethnic minority groups (i.e., Black/African Americans and Hispanic/Latino), who in some cases showed a survival advantage compared to non-Hispanic White individuals. 21 Overall, variations in settings, study designs, operationalizations of migratory/minority status, and ethnic composition of the study populations make it difficult to contextualize our findings within the body of available evidence.
In general, a migrant mortality advantage (MMA) (i.e., lower mortality among migrants as compared to the native population) has been frequently described in high-income countries and often referred to as a mortality paradox.17,22,23 Indeed, in contrast with this advantage, migrants generally have lower socioeconomic position, employment levels, and health literacy, limited social support, and reduced access to education and healthcare resources. Moreover, as confirmed in our study, they have a lower likelihood of receiving adequate therapeutic prescriptions. These factors are widely understood as determinants of poor health. To provide a tentative explanation for the MMA, the concept of a “Healthy Migrant Effect” has been proposed. This effect suggests that there may be a positive selection for health among migrants who move to highly developed countries. This phenomenon may be linked to various factors, including the motivations for migration (such as employment) and the differences in lifestyle behaviors in their countries of origin.17,24 However, this hypothesis is still debated in the scientific community17,24–26 and has not been consistently documented for dementia. Our study suggests that migrants did not exhibit a better health profile relative to natives based on comorbidities and concomitant pharmacological treatments, as shown in Table 1.
The mortality paradox might be explained by additional hypotheses, such as the “Salmon Bias”.22,26,27 This phenomenon describes the return migration selection, namely the tendency of migrants to return to their country of birth or to move to another region or country due to their illness, advancing age, or to rejoin relatives. This may contribute to the higher proportion of younger and healthier individuals among migrants and lead to an underestimation of mortality, as such events might occur outside the region under investigation and, therefore, go unrecorded. In this regard, a recent study conducted in the United States revealed that a diagnosis of dementia is associated with a marked increase in residential relocation within the country, likely reflecting the need for care support and proximity to family members or services. 28
Different studies have explored the return migration selection by comparing the mortality of migrants who returned to their country of birth to those who remained in the receiving countries.22,26,29 In the present study, the observation periods were right censored in cases of interruption of care in Lazio (e.g., when they were no longer listed among patients assisted by a General Practitioner in the Lazio region) to mitigate the impact of this phenomenon. However, it was still possible for individuals to move to another country while remaining on the assistance list, which may have contributed to an underestimation of mortality events. A previous Italian study by Di Napoli and colleagues (2011) compared age-specific all-cause mortality between Italians and immigrants, taking into account deaths occurring both in Italy and in immigrants’ countries of origin. The authors found that including deaths in the country of origin increased immigrant mortality rates, highlighting a potential underestimation using Italian Registries due to return migration and supporting the hypothesis that the salmon bias may partly explain the observed mortality paradox. Nevertheless, age-specific all-cause mortality remained higher among Italians even after accounting for deaths abroad, suggesting that additional factors may contribute to explaining the paradox. 22
A factor that could also influence our findings is the heightened risk of underdiagnosis of dementia among migrants as opposed to native populations. This issue may stem from two main reasons: first, migrants may have limited access to healthcare services or may be less willing to seek help; second, healthcare providers might encounter greater difficulties in delivering accurate dementia diagnoses to culturally and linguistically diverse groups.30–33 Indeed, our data showed a lower proportion of antidementia drugs used in migrant than in natives suggesting a reduced access to dementia treatment. According to a possible hypothesis, underdiagnosis in migrants, and not in natives, could be based on the migrant's health status. The likelihood of being identified as a person with dementia among migrants, and thus being included in the cohort, may also depend on overall health status, with individuals in better general health being more likely to access appropriate services. Dementia diagnosis relies primarily on cognitive and neuropsychological assessment. In a recent nationwide survey of Italian memory clinics, although the number of referred migrants affected by dementia was relevant and had increased over time, poor use of linguistically and culturally adapted tools was observed. Moreover, specialized healthcare professionals, such as professional interpreters and cultural mediators, were frequently lacking. 7
A point of consideration in the present study is the different performance of health information systems in capturing health phenomena, including dementia and other medical conditions, in migrants and natives. The identification of cases relies on individuals’ interactions with healthcare services, and consequently, greater access increases the likelihood of inclusion in disease cohorts. Additionally, the potential misclassification of migratory status resulting from using the proxy variable “country of birth” represents a limitation. As suggested by Figure 1 (different distribution by country of birth between all migrants living in Lazio (Figure 1(a)) and those affected by dementia (Figure 1(b))), some individuals classified as being born in HPMCs may have been born in those countries to Italian parents living in former colonies (e.g., Libia) and subsequently resided in Italy for most of their lives. While these individuals are categorized as migrants, their characteristics and health opportunities may closely resemble those of native Italians. Anyway, subgroup analyses conducted on individuals residing in Rome, alternatively using citizenship as a proxy, confirmed the results from the main analyses. The classification of countries of birth into two heterogeneous groups (HPMCs and HDCs) could present a limitation by combining migrants with varying migration histories and behaviors. In this study, we were unable to analyze individual ethnic groups or other alternative classifications due to the small number of migrants from Oceania, Asia, and North America (Supplemental Tables 2 and 3). With a larger sample size, and particularly a greater number of migrants from these regions, future research should investigate differences in mortality and health outcomes by geographic area of origin, thereby reducing the heterogeneity of the classification adopted in this study. Another characteristic of this study is that it included only migrants who are residents in Lazio and have healthcare assistance from the Regional Health Services. These individuals represent a selection of the healthier migrants living in the Lazio Region, with a higher possibility and capacity to access health care services. Furthermore, the absence of data on the severity of dementia, which would have enabled a more in-depth exploration of the differences in the health outcomes studied, could also represent a limitation. Finally, although in Italy reversible acetylcholinesterase inhibitors and N-Methyl-D-Aspartate receptor antagonists should be prescribed only for patients with mild to severe Alzheimer's dementia (according to Italian Medicines Agency note 85), 34 in clinical practice these drugs are also used in cases of mild cognitive impairment) or other neurological conditions. As a result, some individuals included in the study cohort may not have dementia. However, we do not expect this potential misclassification to differ between migrants and natives.
The present study also has valuable strengths. Firstly, to our knowledge, this is the first attempt to investigate mortality among migrants with dementia at a population level, offering a valuable contribution to the understanding of outcomes of a severely disabling disease in these populations. The findings become even more important since this phenomenon is expected to rise, given the aging of the migrant populations. A significant strength is the use of large administrative databases obtained by record linkage between different health information systems, which allows for the identification of individuals affected by dementia in the Italian and migrant resident population, and to follow up with them for many years. Health information systems collect health information at a population level and represent a reliable, standardized, and high-quality source of data. Moreover, the use of a validated algorithm to identify dementia cases in the Lazio population represents an additional key strength of this study. 16
In conclusion, the study found that migrants with dementia had lower mortality compared to native Italians, especially among those from HMPCs. These results may not accurately reflect the likelihood of better health status and improved outcomes among migrants. Various factors, behind a truly lower mortality, including a healthy migrant effect or data artifacts such as the salmon bias and described data limitation, could affect these findings. Researchers should carefully consider all these aspects when designing future studies on this topic.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251387134 - Supplemental material for Mortality in migrants with dementia living in Lazio, Italy: A 5-year cohort study
Supplemental material, sj-docx-1-alz-10.1177_13872877251387134 for Mortality in migrants with dementia living in Lazio, Italy: A 5-year cohort study by Anna Acampora, Laura Angelici, Laura Cacciani, Silvia Cascini, Marco Canevelli, Guido Bellomo, Benedetta Contoli, Ilaria Cova, Simone Pomati, Ilaria Bacigalupo, Nicola Vanacore, Nera Agabiti, Anna Maria Bargagli and ImmiDem Study Group in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We thank ImmiDem Study Group for the contribution to the discussion and interpretation of study results.
Ethical considerations
This study is conducted within the ImmiDem project (GR-2021-12372081). The study protocol was approved by the Ethics Committee of the Italian National Institute of Health (Protocol 0017082; 6 April 2023).
Consent to participate
The Department of Epidemiology of the Lazio Regional Health Service has complete access to anonymized health administrative databases. The data used in this study were analyzed anonymously, following a standardized methodology in accordance with national privacy laws. The results are reported in aggregate form, ensuring that individuals cannot be identified directly or through any identifiers. As a result, obtaining informed consent from participants was not necessary.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study and the whole ImmiDem project were funded by the Italian Ministry of Health (GR-2021-12372081). The funding sources played no role in the study's design and implementation, in the data collection, management, analysis, and interpretation, in the manuscript preparation, review, or approval, nor in the decision to submit the manuscript for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.