
Abstract
Background
Young-onset dementia (YOD) affects the lives of people living with the condition and family carers, such as partners and children, creating complex situations and unique needs. These needs are likely to differ across dementia subtype, disease phase, and living setting, yet, a comprehensive overview of distinct needs is currently lacking.
Objective
This scoping review aims to identify needs of people with YOD and family carers in relation to dementia subtype, disease phase, and living setting.
Methods
Literature was systematically searched in PubMed, CINAHL, Embase, and APA PsycINFO up to October 2024. After screening by two independent researchers, 140 articles were included.
Results
Four main themes of needs emerged: support-, care-, interpersonal-, and personal needs. Needs varied per target group, dementia subtype, living setting, and disease phase. Prominent support needs included practical assistance, and emotional and psychological support. Information on diagnosis and prognosis, and active involvement of healthcare professionals were highlighted within care needs. Interpersonal needs often referred to companionship and togetherness, as well as empathy, understanding, and acceptance. Finally, security and safety, and time for oneself were emphasized as personal needs. Overall, the majority of current evidence pertained to Alzheimer's disease, the post-diagnostic phase, and living at home.
Conclusions
YOD-needs vary widely, requiring flexible, person- and family-centered care and support. Future research should address underrepresented areas, including the needs of dyads, families, and YOD care home residents. Additionally, it should address needs related to rarer YOD subtypes and specific disease phases to better capture the diversity of these needs.
Introduction
When dementia affects individuals before the age of 65, it is referred to as young-onset dementia (YOD). 1 The worldwide prevalence of YOD is estimated at 3.9 million. 2 YOD not only impacts those with the condition, but also family carers, which include spouses, children, and other family members. The far-reaching impact of YOD can lead to various psychosocial challenges such as changes in family dynamics, as well as difficulties in employment, finances, and relationships. 3
To manage the impact of the condition, psychosocial support plays a crucial role for people living with YOD and family carers. For example, YOD support groups can positively impact acceptance of cognitive impairment, promote self-help strategies, and stimulate meaningful activities and resilience. 4 However, available support and psychosocial interventions are generally designed for individuals with late-onset dementia (LOD), which means most services may not fully meet the needs of people living with YOD and family carers.5–7
YOD leads to unique needs and challenges for those living with the disease as well as family carers, as they are often still employed and actively engaged in social activities, compared to people living with LOD.8,9 Some reviews have examined the impact of YOD, and needs related to YOD. For instance, Wiggins et al. 10 reviewed the impact of YOD, focusing on experiences of relatives, but did not explicitly explore needs. In addition, O’Malley et al. 11 conducted a literature review about the lived experiences of people affected by YOD, with a focus on the diagnostic process. Another review 12 presented an overview of needs of people living with YOD and family carers, focusing specifically on service use. Moreover, Svanberg et al. 13 reviewed the impact of a YOD diagnosis on individuals and families, but without providing detailed information regarding the phase in the disease process or the living setting. However, specification of needs by dementia diagnosis, disease phase and living setting is important, as needs may vary accordingly.14,15
First, YOD can express itself in many ways due to the 251 unique YOD subtypes identified in a recent integrative review. 1 For example, in young-onset Alzheimer's disease (AD), multiple variants exist which can lead to cognitive, visual, language and/or behavioural symptoms. 16 Each YOD etiology has its own specific set of symptoms, leading to subtype-dependent needs for people with YOD and family carers. 15 Second, needs of people living with YOD and family carers may evolve and vary during the disease process. 17 For example, around diagnosis, people living with YOD might still be employed, often requiring support in managing work-related challenges and maintaining social connections. 18 This phase can differ from a later phase in the disease process where more support with activities of daily living and managing complex care tasks might be needed. 9 Simultaneously, family carers also experience changing needs over time, as their role evolves during the disease process 19 and their priorities may change as time progresses. Third, the living setting of the person with YOD can influence the needs of people living with YOD and family carers. The living setting refers to the physical environment in which the person with YOD primary resides and receives care. This setting can include the persons own home, assisted living facilities, nursing homes, or even specialized dementia care units. People with YOD tend to live at home for a longer period of time compared to those with LOD. 20 However, caring for a person with dementia at home poses extra challenges on family carers, who may already have demanding social and professional responsibilities. On a dementia care unit, it is also important to understand and adjust to the needs of people living with YOD, as long-term care facilities are generally targeted at older adults while people with YOD regard themselves as distinct from older people with dementia. 21
Acknowledging and understanding the specific challenges faced by individuals with YOD and family carers is crucial for the development of appropriate support and care. Although there is growing recognition of these challenges, the literature remains limited in its exploration of YOD needs. Currently, there is a lack of in-depth understanding of YOD needs and how these needs differ across subtypes of dementia, phases in the disease process, and living settings. To address this gap and extend existing knowledge, this scoping review aims to answer the following research question: What are the needs of people living with YOD and their family carers, as specified by subtype of dementia, phase in the disease process, and living setting? The outcome of this review will provide a foundation for developing targeted, person-centered support and interventions for people with YOD and family carers. Ensuring alignment between identified needs and available interventions is essential for enhancing quality of life and sustainability of YOD interventions.
Methods
This study is part of the YOD-INCLUDED project. This is a Dutch research consortium, aimed at improving early recognition and diagnosis, studying (hereditary) causes, and providing appropriate care and psychosocial support to people with YOD and their families. In this study, a scoping review was conducted to provide a comprehensive overview of the existing literature regarding the diverse needs of individuals with YOD and family carers. A scoping review uses an expansive approach to answer broad research questions, making this design suitable for the present study. 22 This study followed the methodology of Arksey and O’Malley 23 with five consecutive steps: (1) identification of the research question, (2) identification of relevant studies, (3) selection of studies, (4) charting the data, and (5) collating, summarizing, and reporting the results. In addition, the results were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist. 24 The scoping review protocol was pre-registered within Open Science Framework: https://doi.org/10.17605/OSF.IO/U4KVB. No ethical approval was required, as this study is a scoping review that does not involve experiments on human or animal subjects.
Search strategy
The systematic literature search was conducted in PubMed, CINAHL, Embase, and APA PsycINFO, in August 2023, to identify relevant publications. The search was updated in October 2024. The search strategy consists of three blocks: (1) young-onset, (2) dementia, and (3) needs. The complete search strategy can be found in Supplemental Tables 1–4. In addition, reference lists of included articles were searched for additional relevant papers.
Eligibility criteria
The inclusion criteria for this review encompassed studies that: (a) specifically address needs or experiences of people living with YOD and family carers, including spouses, children, dyads, and families. The definition of a need was conceptualized as an implicitly expressed felt state of deprivation, an explicit desire for something, or as a solution to fulfill this state of deprivation;25,26 (b) include one or more of the following dementia subtypes: AD, frontotemporal dementia (FTD), Lewy body dementia (LBD), vascular dementia (VaD), Parkinson dementia, posterior cortical atrophy (PCA), primary progressive aphasia (PPA), corticobasal degeneration, and cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL); (c) incorporate original data; (d) are peer-reviewed; and (e) published in English or Dutch. Studies were excluded if they: (i) made no clear distinction between experiences of people affected by YOD and LOD; (ii) included one or more of the following dementia subtypes, namely HIV/AIDS dementia, Down syndrome dementia, Creutzfeldt-Jakob, or Huntington; or (iii) used YOD diagnosis purely as an outcome measure, such as identification or prediction of dementia, instead of exploring the needs and experiences of persons with dementia.
Study selection
After the removal of duplicates, two researchers (MR and KP) executed the screening process, using the online tool ‘Rayyan’. 27 A sample of 100 titles and abstracts were screened by two researchers (MR and KP) and resulted in a Cohen's Kappa of 0.62 which stands for a substantial agreement between researchers. 28 Hereafter, all articles were screened based on title and abstract by MR and KP. One researcher (MR) performed the full-text screening of the remaining articles, and another researcher (KP) performed a check on these articles. If no consensus was reached on a decision to in- or exclude an article, a meeting with a third researcher (MdV) was held to decide.
Data extraction
An initial data extraction form was developed in Excel and comprised: (1) general data (e.g., authors, title, country, aim); and (2) study characteristics (e.g., study design, methodology, participant characteristics). An additional data extraction form was developed in Excel to derive (3) needs and additional details on dementia subtype, phase in the disease process, and living setting. An initial data extraction on 13 full-text articles was performed by two reviewers (MR and KP) to critically evaluate the data extraction forms and make any necessary adjustments. Data from the remaining full text articles were extracted by one researcher (MR). A second and third researcher (KP and SLB) verified the extracted data of these articles. In case of disagreements between researchers, a meeting with other researchers was held (MdV and CB) to reach consensus. If data was missing or unclear, the researchers contacted the study author(s) and requested data or clarification.
Data analysis and synthesis
Initially, extracted data from the included articles was inductively analysed and discussed by two researchers (MR and SLB) to decide on the interpretation and identification of specific needs. In cases where consensus was not reached between these researchers, a consensus meeting was conducted with the complete research team (MR, SLB, MdV, CB). After consensus was reached on all needs, themes and subthemes were created. The creation of themes and subthemes was deductively inspired by two key frameworks. The first framework, The Domains of Quality of Life in Dementia, proposed by Schölzel-Dorenbos et al., 29 incorporates categories of needs in dementia, including biological and physiological needs, safety needs, belongingness and love needs, esteem needs, and self-actualization. The second framework, Themes on Objectives and Needs Met by Positive Services for People with YOD outlined by Stamou et al., 30 is specifically focused on people with YOD and consists of three themes: maintaining autonomy, being myself, and a sense of togetherness. When previously identified needs did not align with the concepts of these frameworks, additional themes and subthemes were developed inductively. The final categorization structure was primarily guided by the extracted data from the included articles, allowing for the inclusion of all relevant qualitative findings while using the existing frameworks as a helpful foundation rather than a limiting structure. Ultimately, the research team (MR, SLB, MdV, CB) collaboratively deliberated on the definitive categorization of identified unique needs into themes and subthemes.
Results
Review process
In July 2023, 2715 unique articles were identified in Pubmed, CINAHL, Embase, and APA PsycINFO. After title-, abstract-, and full-text screening, 117 studies were included in this review. In October 2024, 23 additional articles were included by means of snowballing reference lists and by performing an update of the search. This ultimately resulted in a total of 140 included articles that met the inclusion criteria. The PRISMA flow diagram in Figure 1 illustrates the study selection process. When referred to the studies extracted by the literature search in the results section below, a Vancouver parentheses numbering referencing style was used, alongside a Vancouver superscript referencing style for all other references. This follows the referencing approach of Bartels et al. 31 The reference list of the 140 included studies can be found in the Supplemental Material.
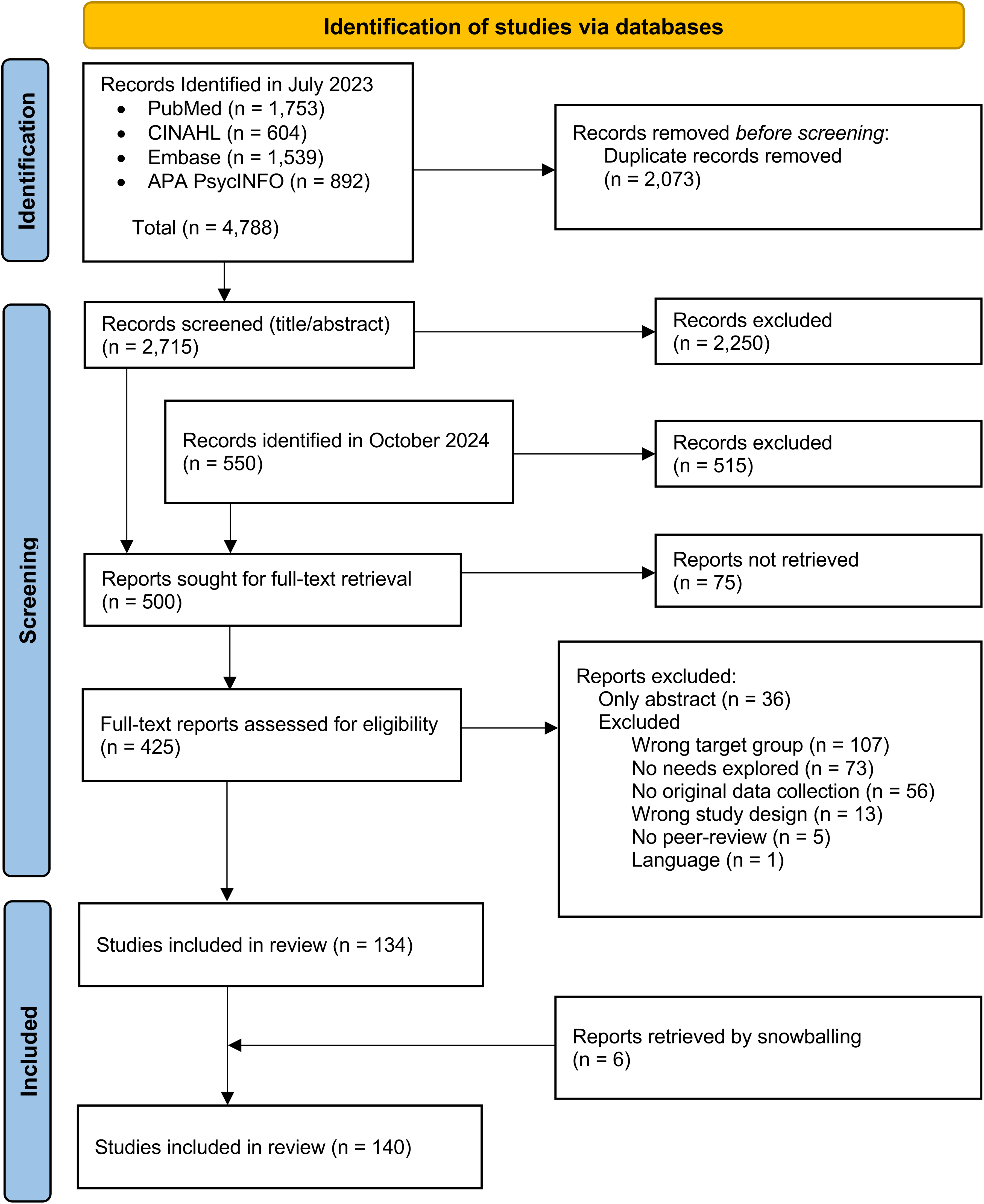
PRISMA flow diagram.
General study characteristics
Included studies were published between 1994 and 2024. Most studies were conducted in Europe (n = 92), followed by North and South America (n = 28), Oceania (n = 13), and Asia (n = 7). Primarily, qualitative research methods were employed (n = 124), with fewer studies using quantitative approaches (n = 7) or mixed methods (n = 9).
Target groups varied across studies: 69 articles explored the needs of individuals with YOD, while 88 articles focused on the needs of family carers (including spouses, children, and siblings). Additionally, 19 articles highlighted the specific needs of couples, and 8 articles examined the needs of families (including individuals with YOD, spouses, children, and siblings). Furthermore, 32 studies included multiple target groups from those mentioned above.
Overall, 28 articles focused on specific dementia subtypes, with AD being the most frequently studied (n = 16). Moreover, 99 articles addressed needs associated with specific phases of the disease process. In 79 articles, needs were explored in a specific living setting, with most studies focusing on persons with YOD living at home (n = 76). Thirteen articles mentioned needs in relation to the person with YOD living in a care home. An overview of all study characteristics can be found in Supplemental Table 5.
Identification of main themes and subthemes related to needs
Four main themes were identified when synthesizing the extracted data of the included articles: (i) support needs, (ii) care needs, (iii) interpersonal needs, and (iv) personal needs. Each of these main themes include four to five subthemes, representing various aspects of the corresponding main themes. In total, 90 unique needs were identified from the included references. Figure 2 comprises a visual representation of all main- and subthemes including details regarding dementia subtype, disease phase, and living setting, based on the available evidence. In the following sections each main theme will be examined in detail, along with its corresponding specific needs, in the context of dementia subtype, disease phase, and living setting.
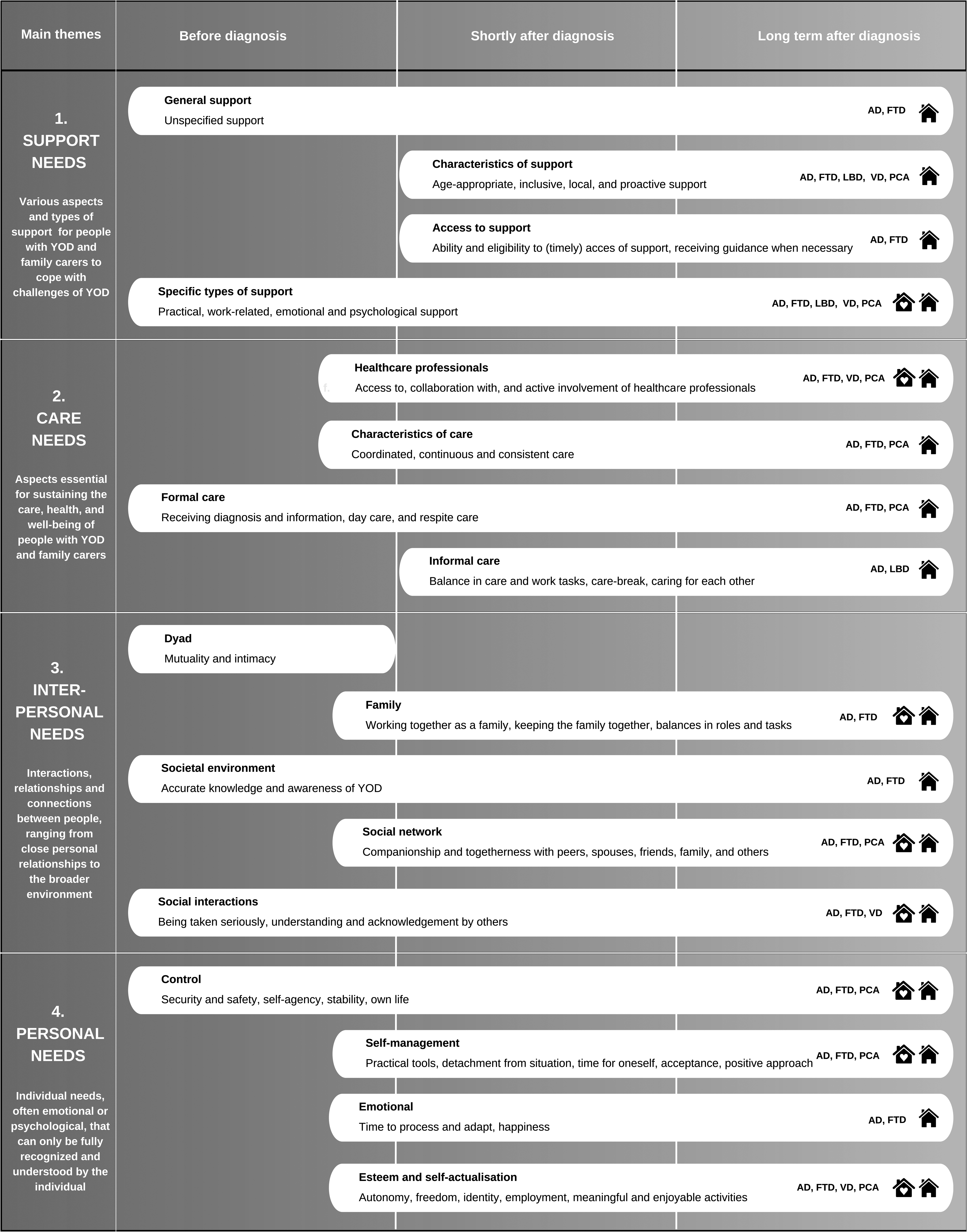
Main and subthemes with detailed information on dementia subtype, disease phase, and living setting based on available evidence. AD: Alzheimer's disease; FTD: Frontotemporal dementia; LBD: Lewy body dementia; PCA: Posterior cortical atrophy; VD: Vascular dementia. The house icon represents a home setting, while the house icon with a heart represents a care home setting.
Theme 1: Support needs
‘Support needs’ is the first main theme that will be discussed and refers to the various forms of assistance and support required to help people with YOD and family carers to cope with the challenges of the disease. Within this main theme, four subthemes were identified (Table 1): general support, reflecting broad, unspecified support needs; characteristics of support, emphasizing tailored, flexible, and inclusive assistance; access to support, addressing eligibility, guidance, and timely help; and specific types of support, covering financial, social, psychological, and practical aid.
Support needs of persons with YOD and family carers including subthemes, specific needs, and clarifications.
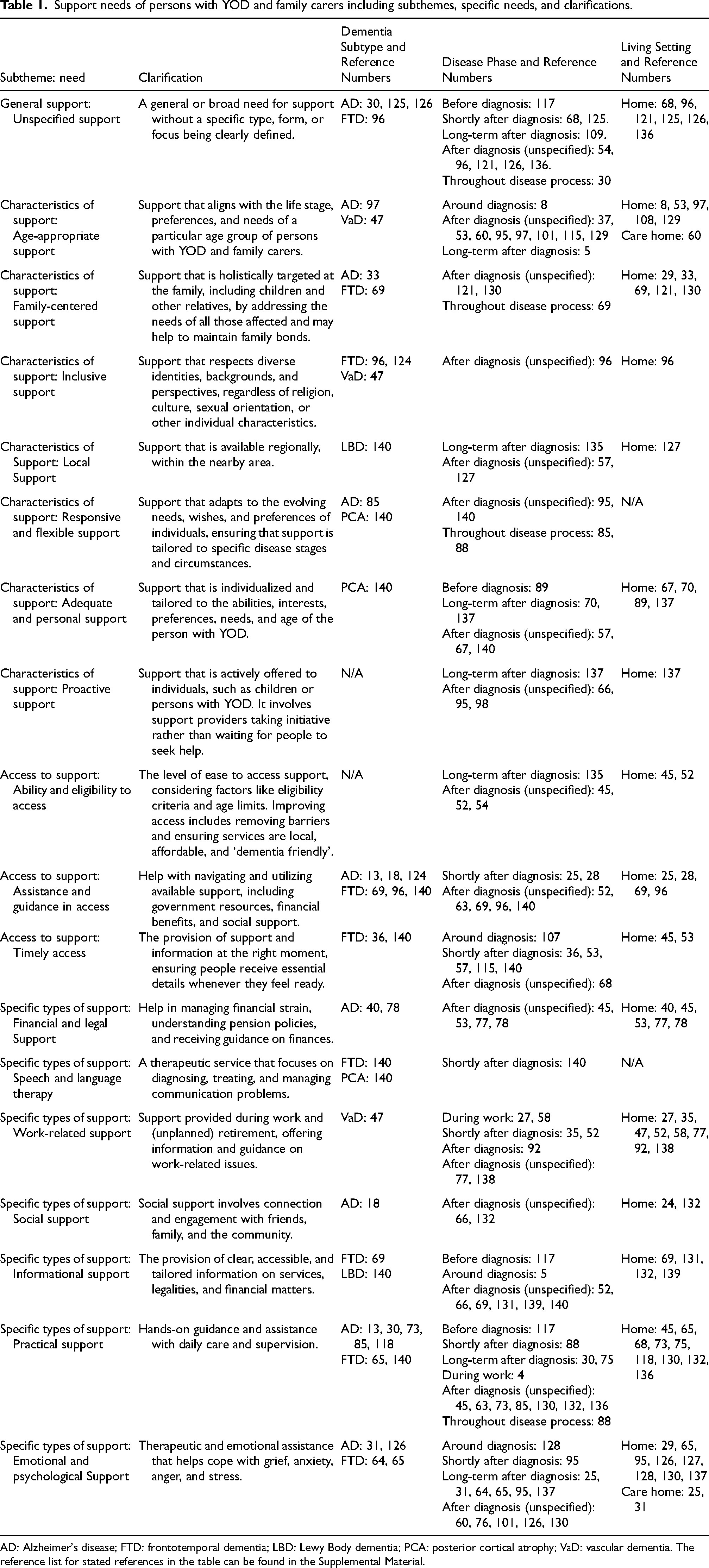
AD: Alzheimer's disease; FTD: frontotemporal dementia; LBD: Lewy Body dementia; PCA: posterior cortical atrophy; VaD: vascular dementia. The reference list for stated references in the table can be found in the Supplemental Material.
Characteristics of support needs by dementia subtype
People with AD, FTD, VaD, and PCA expressed a need for support in general (unspecified support), age-appropriate support and inclusive support. Inclusive support referred to the consideration of topics such as religion, culture, and sexual orientation (Supplemental reference 96). More specifically, a need for speech and language therapy was highlighted by individuals with FTD and PCA, given the communication difficulties that can be associated with these dementia subtypes (Supplemental reference 140).
A need for assistance and guidance in accessing support, as well as a need for practical support, was mentioned by family carers, spouses specifically, of persons with AD and FTD. Practical support included both support in developing (self-)care skills (Supplemental reference 13) and guidance in communication strategies (Supplemental reference 140). Spouses of persons with AD and FTD also mentioned a need for emotional and psychological support from family carers (Supplemental reference 126) and health- and social care professionals (Supplemental reference 65), to share their story with others and process the situation.
Specific patterns of support needs by disease phase
Shortly after diagnosis, family carers expressed a need for timely access to support, while persons with YOD emphasized a need for age-appropriate and practical support throughout the post-diagnostic phase. Since the onset of YOD is often before retirement age, work-related support was particularly emphasized when people with YOD were still employed. Such support can range from open communication with the employer regarding the situation (Supplemental reference 92) to suitable work-place adjustments (Supplemental reference 138). In the period following diagnosis, children primarily indicated a need for proactive support, as well as assistance and guidance in accessing resources. Proactive outreach by support services can improve awareness and accessibility of available resources (Supplemental references 66, 98).
Throughout the disease trajectory, persons with YOD, family carers, and spouses expressed a need for emotional and psychological support. This ranged from having a supportive family member present during the disclosure of the diagnosis (Supplemental reference 128) to one-on-one therapeutic conversations to process the diagnosis and its impact (Supplemental reference 130). Additionally, family carers emphasized the importance of ongoing informational support throughout the disease trajectory.
Distinctions in support needs by living setting
Independent of the living setting, spouses and other family members reported a need for emotional and psychological support. This need is particularly important during the transition from living at home to moving into a care home (Supplemental reference 25), which can help in coping with the emotional impact that this change brings in people's lives.
In the home setting, key needs mentioned by people with YOD were work-related and practical support, including home care services or support to manage daily activities (Supplemental reference 132). Family carers express a need for adequate and personal support tailored to the person with YOD, while children specifically mention a need for family-centered support.
Theme 2: Care needs
‘Care needs’ refers to the second main theme which covers aspects essential for sustaining the care, health, and well-being of individuals YOD and their family carers. This main theme consists of four subthemes (Table 2): health- and social care professionals, focusing on medical and specialist support; characteristics of care, highlighting personalized and coordinated care; formal care, covering professional services; and informal care, recognizing the role of family and community support in care.
Care needs of persons with YOD and family carers including subthemes, specific needs, and clarifications.
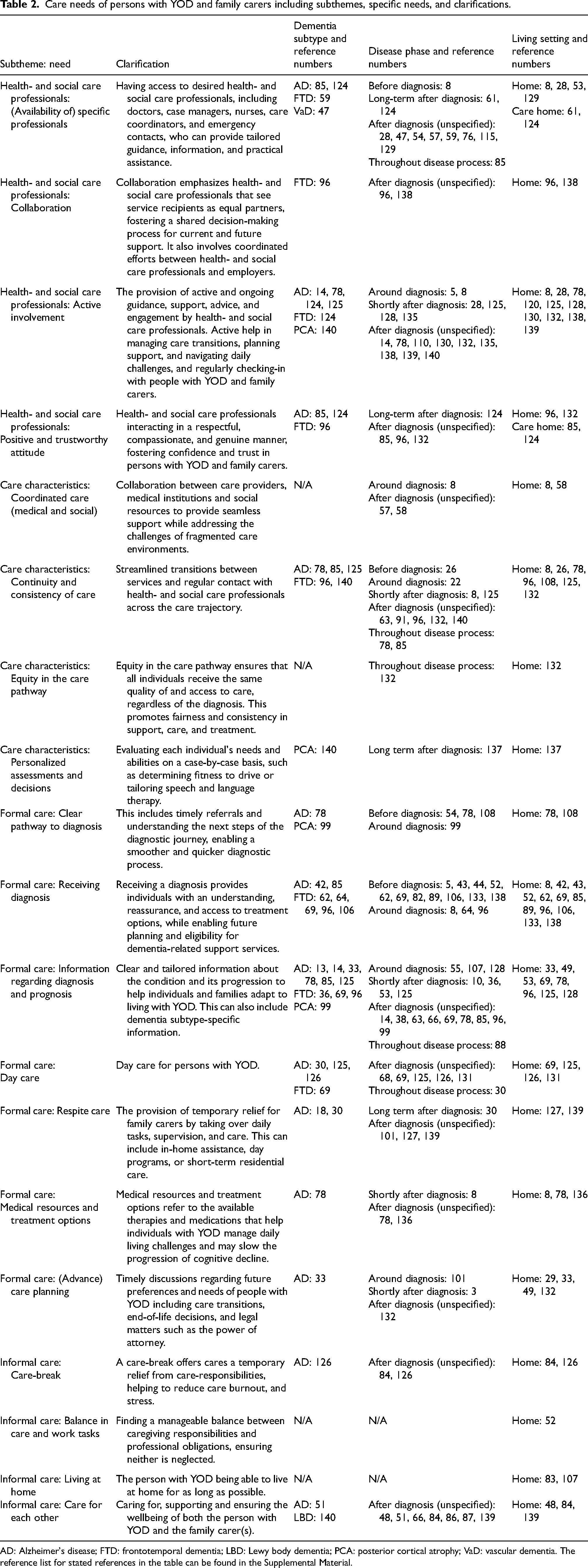
AD: Alzheimer's disease; FTD: frontotemporal dementia; LBD: Lewy body dementia; PCA: posterior cortical atrophy; VaD: vascular dementia. The reference list for stated references in the table can be found in the Supplemental Material.
Characteristics of care needs by dementia subtype
A need for continuity and consistency of care was emphasized across AD, FTD, and PCA, where it was also deemed important for spouses of persons with AD and FTD that health- and social care professionals stayed actively involved. Lastly, an overarching need for information regarding diagnosis and prognosis was mentioned by people with YOD, family carers, and dyads. In relation to AD, FTD, and PCA, specific subtype information was sometimes perceived as lacking or inaccessible (Supplemental reference 33).
Specific patterns of care needs by disease phase
In the pre-diagnostic phase, family carers highlight the importance of receiving reassurance that symptoms are attributable to dementia and that a diagnosis can be identified by specialized healthcare professionals (Supplemental reference 43), implying the need for a timely diagnosis.
After receiving the diagnosis, persons with YOD emphasized the need for active involvement and a positive and trustworthy attitude from health- and social care professionals. Access to specific professionals was also deemed important, including a designated point of contact to call in need (Supplemental reference 115), professionals facilitating (online) support groups (Supplemental reference 129), and speech- and language therapists (Supplemental reference 140). More specifically, both spouses and children mentioned a need for active involvement from health- and social care professionals with YOD expertise. Children wished to be actively involved by health- and social care professionals in the communication regarding the illness of their parent (Supplemental reference 63).
Throughout the disease trajectory, all subgroups expressed a need for information regarding diagnosis and prognosis, ideally including guidance on what to expect and how to manage behavioral challenges (Supplemental references 53, 85). Spouses often emphasized the importance of having access to, for instance, physicians throughout the disease process (Supplemental references 8, 124).
Distinctions in care needs by living setting
When living at home, day care was a recurring need for persons with YOD and family carers as this can positively impact the quality of life of persons with YOD (Supplemental reference 125) and provide relief and respite for family members responsible for care at home (Supplemental references 125, 131). Furthermore, individuals with YOD often expressed a desire for advanced care planning, driven by the wish to remain actively involved in decisions about their future care. In the early stages of dementia, while still living at home, individuals are most likely able to communicate preferences and actively participate in advanced care planning (Supplemental references 33, 49).
In care home settings, it was important for family carers to feel at ease with health- and social care professionals and trusting them in taking over their loved one's care (Supplemental reference 85), especially in care home settings. Therefore, family carers emphasized the need for a positive and trustworthy attitude from health- and social care professionals.
Theme 3: Interpersonal needs
The third main theme, ‘interpersonal needs’, reflects interactions, relationships, and connections between people. Different levels of connection are addressed, ranging from close personal relationships to the broader social environment. This main theme consists of five subthemes (Table 3): dyad, emphasizing mutuality, reciprocity, and intimacy in spousal relationships; family, addressing needs within the family setting; social environment, highlighting the need for accurate knowledge and awareness in the general public; social network, underscoring the importance of companionship and togetherness with others; and social interactions, which encompasses interactions between people.
Interpersonal needs of persons with YOD and family carers including subthemes, specific needs, and clarifications.
AD: Alzheimer's disease; FTD: frontotemporal dementia; LBD: Lewy body dementia; PCA: posterior cortical atrophy; VaD: vascular dementia. The reference list for stated references in the table can be found in the Supplemental Material.
Characteristics of interpersonal needs by dementia subtype
The overall need for companionship and togetherness was frequently highlighted by both family carers and individuals living with AD, FTD, and PCA. Companionship and togetherness with peers were deemed valuable by family carers, especially spouses, as sharing experiences and receiving guidance from others in similar situations can help reduce feelings of isolation while fostering a sense of belonging and normalcy (Supplemental reference 124). Additionally, dyads expressed a desire for companionship and togetherness with others, as they often experience isolation both from their environment and from each other. Individuals with AD and FTD also emphasized a need for empathy, understanding, and acceptance from others. People with YOD stressed the importance of raising awareness that certain behaviors are a consequence of the condition rather than intentional actions, to increase understanding in others (Supplemental references 2, 47).
Specific patterns of interpersonal needs by disease phase
Before diagnosis, the prominent need to be taken seriously was voiced by family carers. Some family carers felt dismissed by general practitioners when raising concerns about changes in behavior of their relative, which, in their view, ultimately delayed the diagnostic process (Supplemental references 26, 89, 138).
In the post-diagnostic phase, people with YOD, family carers, specifically spouses and children, emphasized the need for companionship and togetherness with friends, family members and peers. Family carers particularly valued working together as a family, as open discussions about the diagnosis and supporting each other fostered closer bonds and provided them with renewed energy (Supplemental references 62, 84). Within the family context, children expressed a desire for quality time and a meaningful relationship with their parent with YOD. This need remained important in later stages to maintain the bond between parent and child for as long as possible (Supplemental reference 119). Furthermore, spouses highlighted the importance of approval, validation, and appreciation. Recognition from others for their caregiving efforts served as a crucial motivator, helping them to sustain their role despite the challenges of the disease (Supplemental reference 51).
Throughout the disease trajectory, individuals with YOD desired to be taken seriously. Many persons with YOD experienced frustration when others did not believe their diagnosis, as this invalidation can undermine their experiences and struggles (Supplemental reference 136). Similarly, spouses consistently emphasized the need for empathy, understanding, and acceptance as the disease progressed.
Distinctions in interpersonal needs by living setting
In the home setting, persons with YOD and family carers mentioned a need for balance of roles and tasks within the family, as family members navigate their roles in the caregiving process, responsibilities often shift and require adjustment to reach a new balance (Supplemental references 85, 125). For spouses, maintaining companionship and togetherness with their partner was particularly important in this setting. Dementia can alter the relationship and lead to a loss of intimacy, making it important to foster closeness in other ways, such as taking daily evening walks while holding hands (Supplemental references 73, 118).
During the transition from living at home to living in a care home, a need to collaborate as a family in providing care was particularly emphasized by spouses. This collaboration as a family during this period can lessen the overall burden of making difficult decisions associated with the transition (Supplemental reference 124).
People with YOD living in a care home often missed peers of a similar age (Supplemental references 70, 71). For this reason, companionship and togetherness with peers was expressed as a prominent need by people with YOD.
Theme 4: Personal needs
The fourth main theme, ‘personal needs’, encompasses individual needs, often emotional or psychological, that can only be fully recognized and understood by the individual. This main theme consists of four subthemes (Table 4): control, covering needs such as security, self-agency, and clarity; self-management, referring to individual coping strategies; emotional, such as finding happiness; esteem and self-actualization, encompassing self-belief and identity.
Personal needs of persons with YOD and family carers including subthemes, specific needs, and clarifications.
AD: Alzheimer's disease; FTD: frontotemporal dementia; LBD: Lewy body dementia; PCA: posterior cortical atrophy; VaD: vascular dementia. The reference list for stated references in the table can be found in the Supplemental Material.
Characteristics of personal needs by dementia subtype
Family carers, and particularly spouses, of individuals with AD and FTD emphasized the need for acceptance for both the situation and external support. Another prominent need mentioned in relation to these subtypes was the desire to have time for oneself, as many spouses felt heavily tied to their caregiving responsibilities, leaving little opportunity for solitude or personal interests (Supplemental reference 65). Focusing on people living with AD and FTD, a positive and empowering approach is desired which focuses on the positive aspects of life and seizing the day to cope with the diagnosis (Supplemental references 2, 27, 125). Among people living with AD specifically, the need for meaningful and enjoyable activities, along with a sense of self-agency (having a sense of control and competency over making own decisions), was most frequently highlighted.
Specific patterns of personal needs by disease phase
Families emphasized the need to receive the dementia diagnosis in a secure and private setting (Supplemental reference 128), underscoring the importance of security and safety around the time of diagnosis.
After diagnosis, a strong desire to continue working emerged for people with YOD, as work often provided a meaningful role and a sense of purpose, which can be challenging to maintain after the diagnosis (Supplemental references 4, 71). In addition, also meaningful and enjoyable activities were valued by persons with YOD and family carers. Meanwhile, spouses longed for personal time, allowing them to temporarily detach from caregiving responsibilities and finding some time to relax (Supplemental references 59, 67), while children mention a need for personal time which extends beyond finding time to relax and is focused on maintaining their own lives. This includes pursuing personal dreams, attending college, and starting a family (Supplemental reference 66).
In later stages of the disease, the importance of security and safety increased, with a strong emphasis on balancing the independence of the person with YOD while effectively managing risks (Supplemental reference 109). Family carers emphasized the need for acceptance throughout the disease process. In hindsight, many family carers recognized the importance of accepting additional support, particularly in the early phase after diagnosis when caregiving responsibilities often felt overwhelming (Supplemental reference 87). For children specifically, it was important to emotionally and physically detach at times to process emotions, cope with the diagnosis, and protect their own well-being (Supplemental references 88, 139).
Distinctions in personal needs by living setting
In both the home and care home settings, people with YOD emphasized the importance of staying engaged throughout the day through meaningful and enjoyable activities, such as physical, creative, and social activities (Supplemental references 33, 120, 125). The need for security and safety differed per living setting. At home, it was deemed important that the person with YOD was safe when left alone (Supplemental reference 131). In a care home, it was emphasized that the person with YOD must be safe in an unfamiliar setting and surrounded by others (Supplemental reference 124).
In the home setting specifically, people with YOD highlighted the need for a positive and empowering approach, and a sense of purpose, while spouses stressed the importance of having personal time. Spouses noted that living at home with a person with YOD primarily meant continuous caregiving, as much of their time was occupied with care tasks necessary to maintain daily life, often at the expense of their own time (Supplemental reference 69). Children, on the other hand faced different challenges in the home environment and often used different coping strategies. They often felt the need to distance themselves from the situation, particularly when confronted with dementia-related difficulties at home. Some children explained that in such moments, they would leave the home to avoid confrontations and difficult discussions (Supplemental reference 88).
Discussion
Summary of key findings
This scoping review aimed at providing an overview of the needs of people living with YOD and their family carers. The systematic search resulted in the synthesis of evidence from 140 articles. Findings reveal that needs are multi-facetted and vary depending on the target group. Needs also appear to differ based on dementia subtype, phase of the disease, and living setting of the person with YOD. Most needs documented in the current literature relate to AD and FTD, the post-diagnostic phase, and individuals with YOD living at home.
Four main themes of needs were identified: support needs, care needs, interpersonal needs, and personal needs, including specific subthemes (Figure 2 and Tables 1–4). Within the theme ‘support needs’, practical support and emotional- and psychological support were frequently mentioned. In the ‘care needs’ theme, a strong emphasis was placed on information regarding diagnosis and prognosis as well as active involvement of health- and social care professionals. The ‘interpersonal needs’ theme highlighted the importance of companionship and togetherness with peers, friends, family, spouses, and others, along with a desire for empathy, understanding, and acceptance from others. Lastly, in the theme ‘personal needs’, the need for security and safety, mostly focused on the person with YOD, was underscored multiple times, while family carers, especially spouses, frequently mentioned the need for time for oneself.
Definition, expression, categorization, and comparison of needs
Needs, as defined in this review, were interpreted according to the conceptualization of needs of Kotler 25 and refer to a felt state of deprivation or deficiency. As evident in this synthesis, these states can be explicitly expressed, for example when family carers mentioned frustration over the lack of gratitude from their relative with dementia (Supplemental reference 12), or feeling isolated in their struggles (Supplemental reference 17). Moreover, a need could also be expressed as a preference or desire, like the expressed benefit of talking to friends as a useful outlet (Supplemental reference 36). A specific solution to address a deficiency is also closely related to needs, for example the proposed solution of regular interactions with health- and social care professionals every six weeks (Supplemental reference 8) to fulfill the need for continuity and consistency of care. These distinctions highlight the diverse ways in which needs were expressed in the various studies, sometimes making it challenging to identify a potentially underlying need, especially when mentioned implicitly. This challenge was compounded by the nature of the included studies, which were primarily focused on lived experiences rather than systematically inventorying needs.
Needs are shaped by an individual's personal interests, culture, and intrinsic motivators,32,33 which means needs are not static or universal. They evolve over time and vary across different stages as the dementia progresses. The variability of needs challenges the idea of universal solutions and emphasizes the importance of personalized, context-sensitive, and adaptive care and support. Moreover, the aims and topics of the included studies may have influenced the findings, as researchers often prioritize interview excerpts that align with their focus. This could lead to underrepresentation of other needs or participant reflections. Certain needs may also go unaddressed or unspoken due to a delayed acceptance and acknowledgment of the situation. An example of this is the ‘caregiver paradox’. 34 This paradox suggests that family carers may initially downplay or fail to acknowledge their own needs, especially in the early caregiving phase. Time is needed to process and accept the situation before carers are able to acknowledge their early-stage needs and accept support. Societal expectations and stigma may also discourage carers from voicing their challenges, further perpetuating a lack of visibility for unmet needs. 35 Understanding this dynamic is critical to ensure that evolving needs are identified and addressed over time. While this dynamic is commonly seen in carers, it likely applies to the broader family context as well. However, there is still limited research on how this unfolds within the family.
The categorization of the extracted needs was guided by the frameworks of Schölzel-Dorenbos et al. 29 and Stamou et al. 30 yet, not limited to these frameworks to allow for the identified evidence to shape the synthesis. Schölzel-Dorenbos et al. 29 proposed a hierarchy of needs in dementia, which includes biological and physiological needs, safety needs, belongingness and love needs, esteem needs, and self-actualization, ordered by their importance. In this review, extracted needs were identified across all these domains, however, needs in the biological and physiological domain were mentioned less often. This contrasts with the emphasis placed on this domain by Schölzel-Dorenbos et al. 29 A possible explanation for this discrepancy is that these needs, which include basic physical requirements such as sleep and nutrition, may be less emphasized, as individuals with YOD generally experience a better overall health compared to persons with LOD. 36 To enhance comprehensiveness, two additional categories, namely ‘support needs’ and ‘care needs’, were introduced in this review, addressing aspects that were not captured in the original framework.
The framework of Stamou et al., 30 specifically focused on the needs of persons with YOD, also informed the categorization in this study. This framework consists of three themes: maintaining autonomy, being myself, and a sense of togetherness. The findings of this review overlapped with all themes mentioned in this framework. However, additional needs that were not explicitly outlined in the framework of Stamou et al. 30 were also identified. These included the need for empathy, understanding, and acceptance, as well as a need for time to process and adjust to the diagnosis of YOD. This scoping review also incorporated the perspectives of family carers, dyads, and families, hereby highlighting the crucial role of the family unit in coping with YOD. This family-oriented approach adds to the framework of Stamou et al., 30 which primarily focuses on the perspective of the individual with YOD. Finally, the distinction between the individual and social environment, as outlined in the social health framework, 37 was reflected in the themes of interpersonal and personal needs, highlighting the social aspects of health and well-being. Overall, the categorization in this review provides added value to the previously mentioned frameworks by incorporating multiple perspectives and contexts, as dementia subtype, disease phase, and living setting were also considered. This scoping review provides a comprehensive overview of various needs which reflects the evolving nature of needs depending on the context.
Van der Roest et al. 26 identified the need for coping strategies, coming to terms with the disease, social contact, and information about disease progression of dementia. However, their study did not specifically focus on YOD, but rather on dementia in general. These needs correspond to the categories of self-management, acceptance, companionship and togetherness, and information regarding diagnosis and prognosis as outlined in this study. Our review adds the specific contexts in which these needs are most prominent and how the focus of needs shifts across different contexts. For example, the need for security and safety was found to be relevant throughout the disease trajectory and in various settings, with the focus shifting depending on the context. On the other hand, the need to be taken seriously was mentioned less frequently and was most prominent in the phase before- and shortly after the diagnosis. In addition, Carvacho et al. 38 observed that individuals with YOD often express ‘internal’ needs, such as a sense of purpose and identity, while family carers focus more on ‘external’ needs, like specific types of support and care. This disparity may stem from the fact that family carers are not affected by dementia in the same way and may not perceive a significant deficiency in ‘internal’ needs but have to deal with the implications of YOD on a more practical level. Our findings support this distinction: people with YOD frequently emphasized autonomy and having a purpose, while family carers primarily highlighted external and practical needs, such as receiving a diagnosis and collaborating as a family.
Strengths and limitations
A key strength of this scoping review is the inclusion of multiple perspectives, incorporating the needs of persons with YOD, family carers, spouses, children, dyads and families. The needs of these different groups were analyzed separately, as they can differ depending on the perspective. However, it is important to note that these needs are often intertwined, especially when a dyadic or family-based perspective was considered. Additionally, this review also actively considered the context in which these needs emerged, including dementia subtype, disease phase, and living setting. This approach provides a comprehensive overview of these context-specific needs, which allows for a more contextual understanding of how needs vary across different circumstances. Another strength is the inclusive selection process, with no restrictions on publication year. This approach ensured that all relevant studies, regardless of publication date, were considered, allowing for a thorough and extensive analysis of needs.
However, the present review of needs should not be considered exhaustive. The absence of certain needs, or their lack of association with specific dementia subtypes, disease phases, or living settings, does not imply these needs do not exist. Rather, they may not have been captured in the included articles or may not have emerged during the original data collection of the included articles. Additionally, needs are often expressed implicitly in qualitative articles, which requires careful interpretation. To reduce potential bias, interpretations of needs were discussed among the wider research team. Additionally, due to the qualitative nature of most of the included articles, it was challenging to connect needs to a specific disease phase and living setting, as participants often referred to a mix of past and present experiences. To maintain accuracy, phases and living settings were only extracted when they were explicitly mentioned in relation to a need. Finally, only articles published in English were included, thus, additional evidence may be available but not synthesized. As a result, context-specific needs, which may vary by country and culture, could have been overlooked.
Gaps in the field and implications for further research
A subset (n = 129) of all included articles mentioned at least one need that could be linked to dementia subtype, disease phase, and/or living setting. Eleven articles (Supplemental references 32, 41, 46, 56, 74, 81, 90, 100, 103, 104, 105) did not provide detailed information on these aspects in connection to needs. Notably, the expressed needs of dyads and families often lacked specific details regarding dementia subtype, disease phase, and living setting. Overall, articles commonly included needs associated with AD, FTD, and PCA, whereas the specific challenges and needs of people with LBD and VaD were explored less often. Additionally, no studies explicitly mentioned needs of people with other rare forms of YOD such as PPA. Including rarer forms of dementia is essential, as they are often overshadowed by a more generalized understanding of dementia, which can differ significantly. Insufficient attention to these rarer subtypes can lead to an underrepresentation of the unique needs of individuals with these forms of dementia. 39 Articles frequently presented needs within the post-diagnostic phase, though often without clearly defined time frames. Furthermore, the needs of individuals with YOD residing in care home settings were reported less frequently compared to those of individuals living at home.
These gaps in the literature highlight key areas for further research. Future studies should examine needs within the interconnected and evolving context of dyads and families, as well as the experiences of individuals with rarer dementia subtypes and those residing in care homes. Additionally, while needs are most frequently discussed in relation to the broad post-diagnostic period (Figure 2), there is a lack of evidence addressing specific disease phases. Further research should explore how needs evolve across different stages of the disease, as this understanding is essential for developing targeted interventions that adapt to changing needs. Lastly, the included literature may reflect biases, such as overgeneralizing needs or focusing on specific populations, especially those in Western contexts (n = 133). Considering intersectional factors such as age, sexuality, gender, comorbidities, poverty, religion, and disabilities 40 next to the dementia subtype, disease phase, and living setting was beyond the scope of the present review but requires further investigation in the future.
Conclusion
Needs related to YOD vary depending on the target group, dementia subtype, phase in the disease process, and living setting, reflecting the dynamic and evolving nature of these needs. This scoping review offers a broad yet detailed overview, highlighting that no single need applies universally across all individuals, contexts, or stages. These findings also emphasize the importance of adopting a family-centered approach, which considers the differing, yet equally important, perspectives and needs of individuals with YOD and their families. Building on these insights, the authors will develop a needs-oriented taxonomy of interventions to identify key areas for the (further) development of YOD interventions. Nonetheless, it remains essential to engage directly with persons with YOD and family carers to ensure that interventions are tailored to unique circumstances.
This review underscores the importance of adopting a flexible and person-centered approach to care and support that acknowledges the diversity, complexity, and intertwined nature of needs and continuously adapts to the changing circumstances of people affected by YOD. Ultimately, care provision and intervention development should focus on identifying what works, for whom, in which situation, and at what time, to enhance the quality of life of individuals with YOD and their loved ones.
Footnotes
Acknowledgements
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is part of the project YOD-INCLUDED (project no. 10510032120002) of the Dutch Dementia Research Programme, which is financed by ZonMw.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.