
Abstract
Background
A cognition bolt-on version for EQ-5D is needed to comprehensively assess health states of the general population.
Objective
To experimentally evaluate the valuation methods of the EQ-5D-5L bolt-ons using scaling factor and conventional models, we used the cognition bolt-on version of the Japanese EQ-5D-5L (EQ-5D-5L + C) and two previously developed cognition dimensions Remembering things and Thinking clearly.
Methods
Eligible participants, recruited from the general Japanese population, included adults living in three cities. Interviews were conducted from June to August 2023. Participants were randomized to Arms 1 (EQ-5D-5L + C), 2 (EQ-5D-5L + Remembering things), and 3 (EQ-5D-5L + Thinking clearly). Preferences were collected using a composite time trade-off (cTTO). The “1-cTTO” data were modeled using the scaling factor model, with EQ-5D-5L disutility weights estimated from the existing value sets. We also fitted the data into the conventional main-effects additive model. Both models used a tobit model and maximum likelihood estimation. Model performance was assessed using indices of fit.
Results
Overall, 864 individuals participated in the study. Addition of cognition dimensions to EQ-5D-5L expanded the scaling factor model coefficients in all arms. The observed mean and predicted “1-cTTO” values of the scaling factor model were not largely different in all three arms. The mean absolute errors of the scaling factor and conventional models were 0.0720 and 0.1305, 0.0748 and 0.0885, and 0.0985 and 0.0685 in Arms 1, 2, and 3, respectively.
Conclusions
The performance of the two models did not appear greatly different. Further experimental valuation studies using the scaling factor model and cognition items are warranted.
Keywords
Introduction
The EQ-5D is a widely used generic preference-based instrument to assess health-related quality of life based on five dimensions: mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD). 1 The standard EQ-5D classification system provides a generic measure of health, and to better capture disability caused by specific health conditions, the need for adding new or multiple dimensions to the EQ-5D has been proposed. Among various conditions,2–5 a cognition bolt-on for the EQ-5D and its five level response version (EQ-5D-5L) has been shown to improve the ability to evaluate health states.6,7 In countries such as Japan where dementia is prevalent and is projected to increase, 8 a cognition bolt-on version of the EQ-5D that comprehensively assesses the health states of the general population is urgently needed.
Developing a new value set incorporating a bolt-on dimension using the standard EuroQol Valuation Technology (EQ-VT) protocol, however, raises some challenges. The standard approach requires a full-scale valuation study with a large general population sample, which has cost implications. Additionally, value sets generated from newly conducted, stand-alone valuation studies may become inconsistent with existing ones, and the rank order after bolt-on may change due to sampling methods and/or interviewer effects. 9 To overcome these challenges, Yang et al. 9 recently proposed an approach for developing bolt-on value sets based on existing EQ-5D value sets. This approach uses a modified main-effects model (hereafter, the scaling factor model).
Applying this scaling factor model and a conventional approach using existing Japanese value sets,10,11 this study aimed to experimentally evaluate the valuation methods of the EQ-5D-5L bolt-ons by using three cognition dimensions, added to the EQ-5D-5L. As one of the cognition dimension (CO), we used the linguistically and psychometrically validated cognition dimension which is an experimental bolt-on, added to the Japanese EQ-5D-5L (EQ-5D-5L + C).7,12 For the other two, as “cognition” is not a simple concept, the cognition dimensions experimentally developed by Finch et al. 5 (hereafter, Remembering things and Thinking clearly) were also used for comparison purposes.
Methods
Study design
The present study examined health state values collected from the general population in Japan using the composite time trade-off (cTTO) method. The use of EQ-5D-5L cognition bolt-on version was granted by the EuroQol group (Rotterdam, Netherlands). This study was part of the research “Efficiency and Optimization of Care in Nursing Homes from the Perspectives of QOL and Medical Economics”, which was approved by the ethics committee of the Graduate School of Pharmaceutical Sciences, The University of Tokyo. The study was conducted following the local Ethical Guidelines for Medical and Biological Research Involving Human Subjects.
Study population and recruitment
To capture societal values on health states, participants were recruited from the general population in Japan, in line with standard valuation study methodologies. Eligible participants were adults aged ≥18 years, living in Tokyo, Osaka, or Kumamoto, and capable of providing written consent and comprehending Japanese. No exclusion criteria were applied. Potential participants, coordinated by INTAGE Healthcare Inc., were recruited using snow-ball sampling. Among those who showed interest in participating in personal interviews, eligibility was screened. Those confirmed to be eligible were invited to participate in the interview. The target sample size was 810 individuals. This sample size was determined on the basis of the number of target cities considering large- and small-sized cities, population demographics, equal sample sizes across arms and cities, and feasibility. Participants were randomized into three arms (Arm 1, EQ-5D-5L + C; Arm 2, Remembering things; and Arm 3, Thinking clearly; the cognition dimensions are described in the following section), with 270 individuals each (90 per city). Allocation was guided by the population composition by sex and age in Japan. 13
Study procedure
Cognition bolt-ons
As stated above, for the EQ-5D-5L + C, the linguistically and psychometrically validated Japanese cognition dimension 12 was used. The translated EQ-5D-5L + C uses a label “Cognition (e.g.,: memory [forgetfulness], comprehension, concentration, thinking)” and the descriptions included “I have no problems with cognition” (Supplemental Table 1a). For the other two experimentally developed cognition dimensions Remembering things 5 and Thinking clearly, 5 Japanese versions were unavailable. Their translations were prepared according to the following three-step process: 1) forward translation by two individuals, 2) back translations by a native English speaker, and 3) finalization. Final descriptions are provided in Supplemental Table 1b and 1c. The two versions of the cognition dimensions used a label “Cognition” and their descriptions included “I have no problems with remembering things/in thinking clearly”. The permission to modify the EQ-5D versions (Japanese EQ-5D-5L) by adding the Japanese-translated cognition dimensions5,7,12 was granted by the EuroQol office.
Data collection
Preferences were collected through face-to-face, one-on-one interviews conducted by nine trained interviewers using the cTTO valuation method,14–16 following the EQ-VT protocol (EQ-VT version 2.7.2). For health state valuation, we employed a 6*5 orthogonal design following Yang et al. 17 The orthogonal array contained six columns, each representing a dimension, and could therefore be utilized to represent the states of the EQ-5D and a cognition dimension. The selected orthogonal array contained the worst possible health state 555555 (pits state), with the most plausible states. All five mildest states were included in the design manually. 17 Therefore, in total we selected 31 health states (i.e., 25 states + one pits state + five mildest states). Each participant valued a randomly selected block of ten health states and the worst possible health state (555555). Following the quality control (QC) measure provided by the EuroQol office, responses were reviewed on the basis including the time interviewers spent for explanation, the time interviewees required to complete responses, and response patterns (e.g., whether selecting the same option for all questions).
Before starting the interviews, informed consent was obtained from each participant. Participants were free to withdraw their consent at any time up to one week following the interview. Each interview was expected to take approximately one hour to complete. The participants who completed the survey received incentive payment. The interviews were conducted from June 27 to August 7, 2023.
Statistical analysis
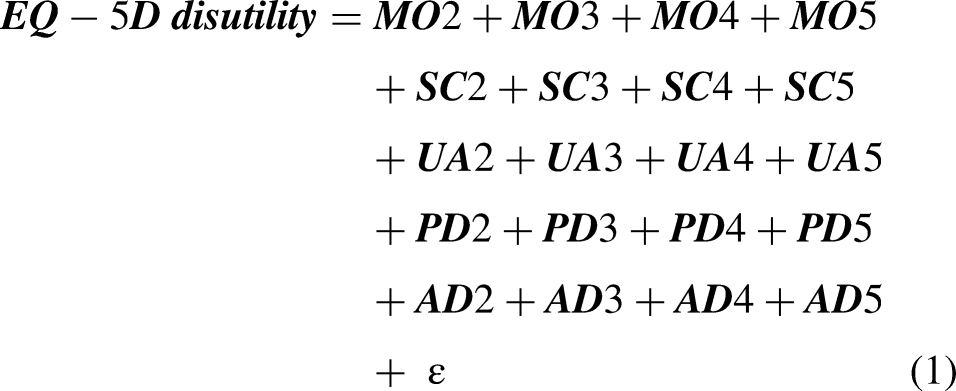
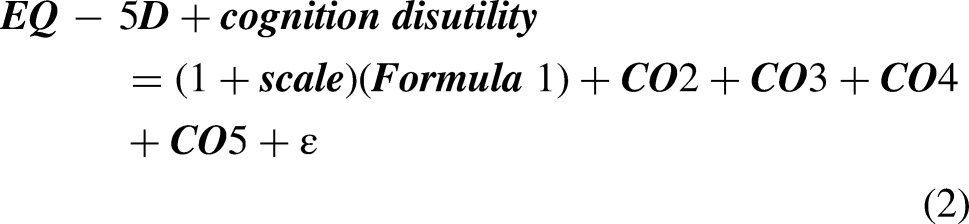
The “1-cTTO” values were modeled for each arm independently using the scaling factor model,
9
with EQ-5D-5L disutility weights estimated from the existing Japanese value sets (Formulae 1 and 2).10,11 The scaling factor model therefore estimated only 1 + scale and four coefficients for each cognition dimension (i.e., CO2, CO3, CO4, and CO5). We also fitted the “1-cTTO” values into the 24-parameter conventional additive model with main-effects using an approach similar to Formula 1.
Both the scaling factor model and conventional main-effects model used a tobit model and maximum likelihood estimation. Model prediction accuracy was assessed using the following indices of fit: mean absolute errors (MAEs), root mean square error (RMSE), Pearson's correlation coefficient, and concordance correlation coefficient (CCC). Both the errors (MAE and RMSE) and correlations (Pearson's correlation and CCC) were calculated using the predicted values and observed means. Lower MAE and RMSE values indicate higher prediction accuracy. Statistical analysis was performed in SAS release 9.4 (SAS Institute, Cary, NY, USA) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
A total of 864 individuals from the general population participated in this study (Tokyo, n = 287; Osaka, n = 288; and Kumamoto, n = 289). Among them, 287, 289, and 288 participants were randomized to Arms 1, 2, and 3, respectively. The distribution of sex and age was similar across the three arms (Table 1). Half of the participants in all three arms were working full-time (Arm1, 52.6%; Arm 2, 55.0%; and Arm 3, 51.7%), followed by those working part-time (Arm1, 16.0%; Arm 2, 15.9%; and Arm 3, 20.1%). Other characteristics were similar across the three arms. Of the 864 participants, one participant in Arm 3 was excluded due to operation errors found by an interviewer; data of 863 participants were analyzed further.
Participant demographic characteristics.
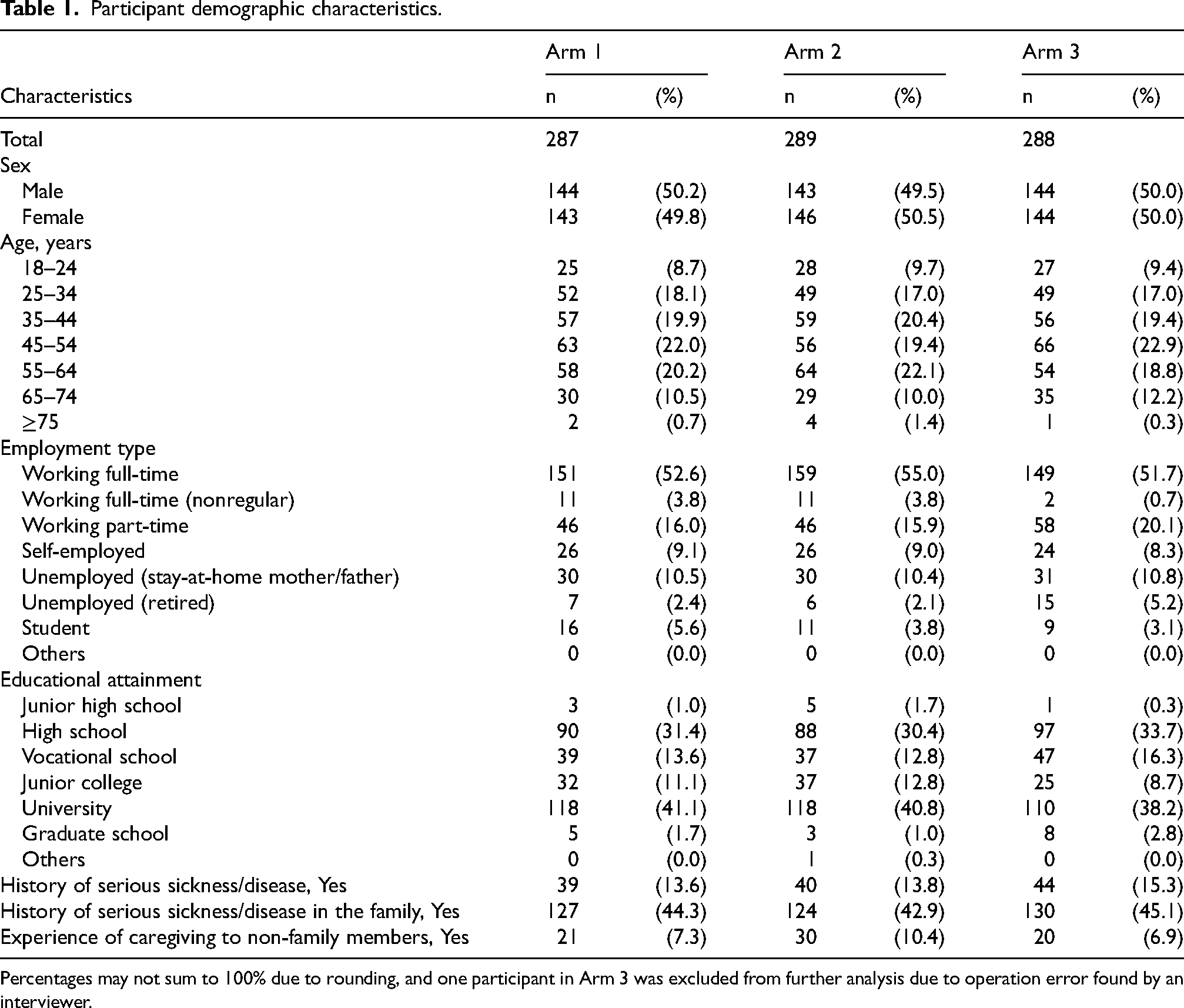
Percentages may not sum to 100% due to rounding, and one participant in Arm 3 was excluded from further analysis due to operation error found by an interviewer.
Scaling factor model and conventional additive model
Addition of the cognition dimension to the existing EQ-5D-5L resulted in the expansion of the scaling factor model coefficients in all arms (i.e., > 1) (Table 2). The estimated scaling factors were 1.3667, 1.3991, and 1.4201 for Arms 1, 2, and 3, respectively. The coefficients of cognition dimension estimated using the scaling factor model showed monotonicity in all three arms. While a similar monotonic pattern was observed for the coefficients of the three cognition dimensions in the conventional additive model, the rank order of the two core dimensions (SC4/SC5 and UA4/UA5) was reversed for Arm 1, but not for the other two arms. The coefficients of CO5 ranked 2nd or 3rd among the severity level 5 across dimensions (i.e., MO5, SC5, UA5, PD5, AD5, and CO5) in all three conventional additive models.
Coefficients of scaling factor model and conventional additive model.
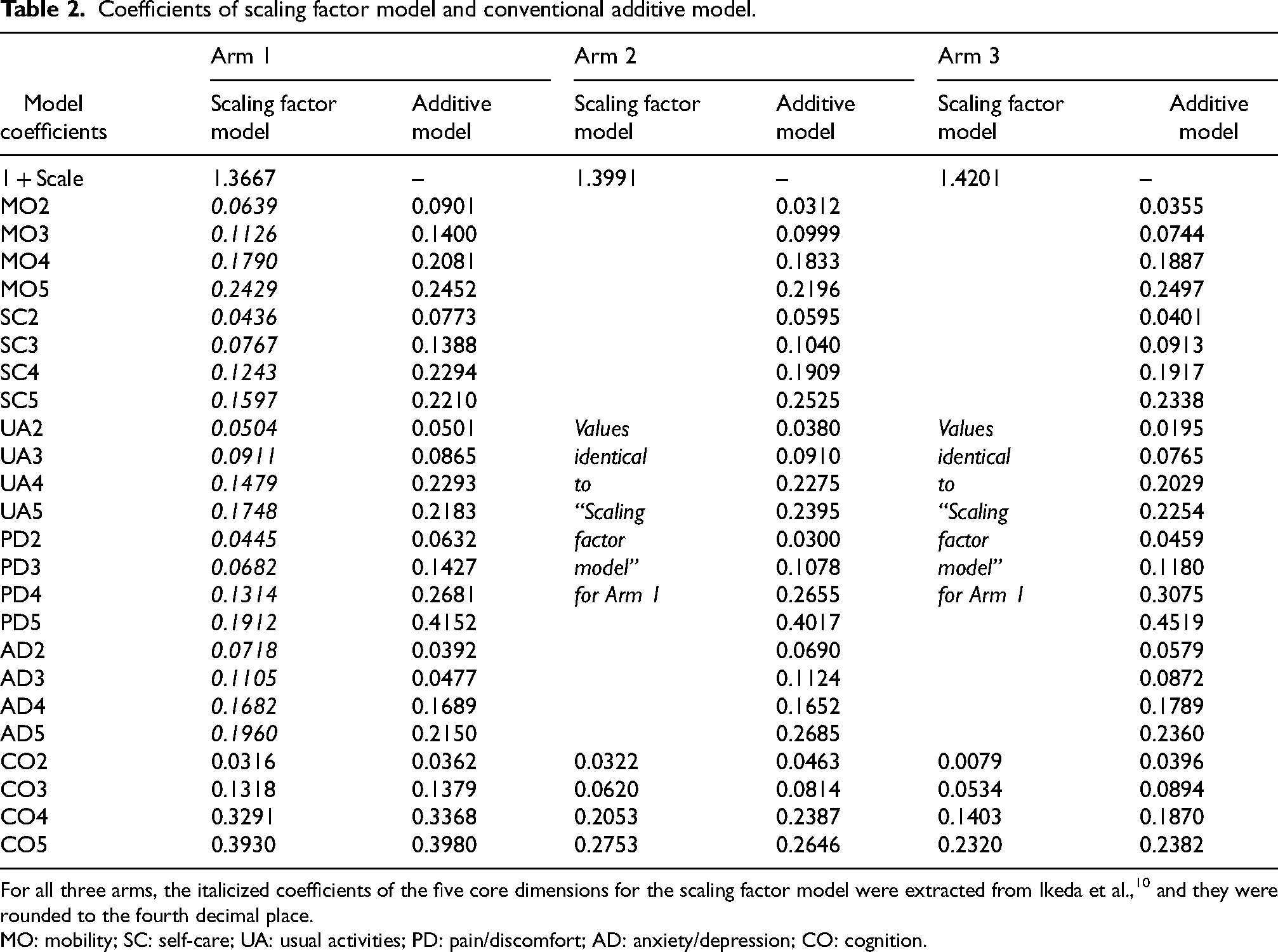
For all three arms, the italicized coefficients of the five core dimensions for the scaling factor model were extracted from Ikeda et al., 10 and they were rounded to the fourth decimal place.
MO: mobility; SC: self-care; UA: usual activities; PD: pain/discomfort; AD: anxiety/depression; CO: cognition.
The observed mean and predicted “1-cTTO” values were slightly discrepant, but no large discrepancies were observed in all three arms (Figure 1). The prediction accuracies of the two models did not appear greatly different in all three arms. The MAEs of the scaling factor model and conventional model were 0.0720 and 0.1305 in Arm 1, 0.0748 and 0.0885 in Arm 2, and 0.0985 and 0.0685 in Arm 3 (Table 3). Pearson's correlation coefficients of both the scaling factor model and conventional additive models exceeded 0.9 in all three arms. The value sets estimated from the present experimental analyses using the scaling factor model are provided in Supplemental Table 2.
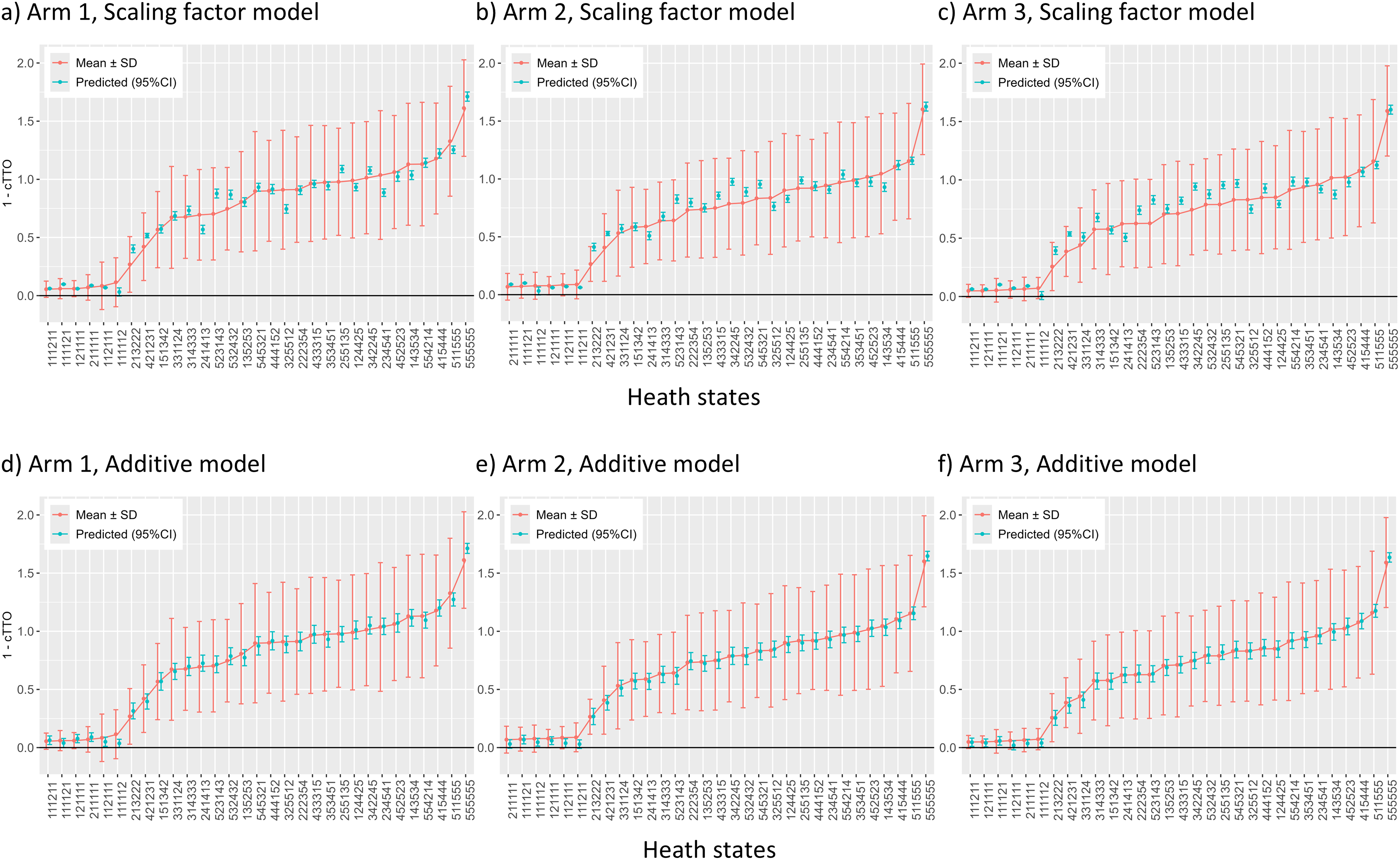
The observed mean and predicted cTTO values for 31 health states. cTTO: composite time trade-off.
Model prediction accuracy.
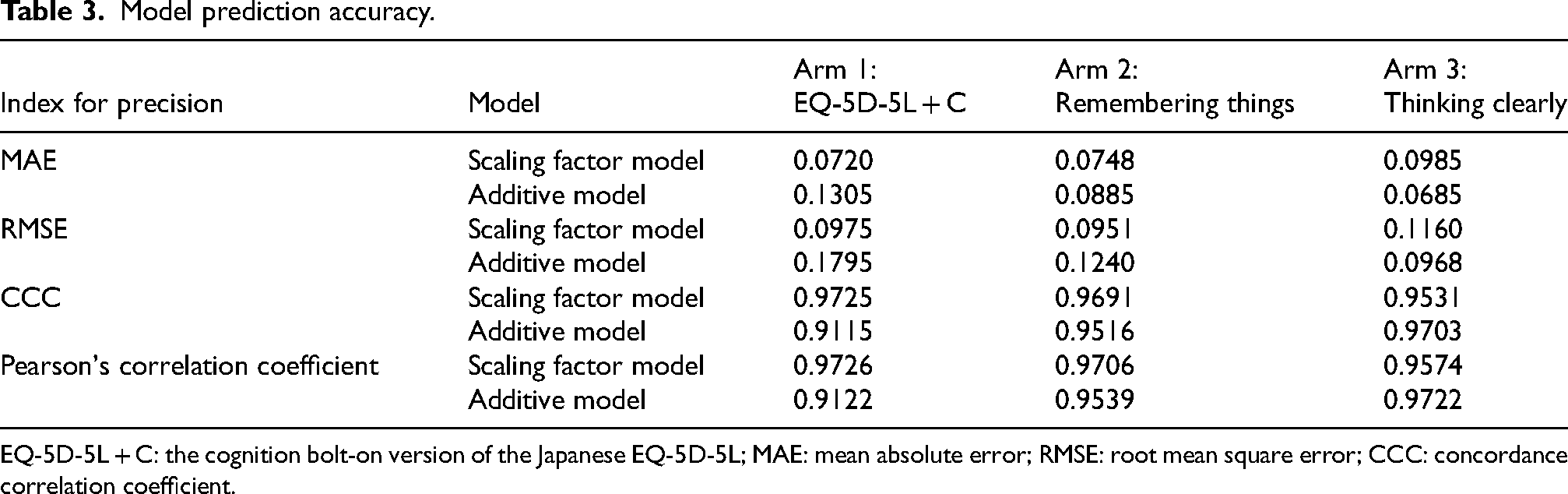
EQ-5D-5L + C: the cognition bolt-on version of the Japanese EQ-5D-5L; MAE: mean absolute error; RMSE: root mean square error; CCC: concordance correlation coefficient.
Discussion
This experimental study evaluated the valuation methods of three cognition bolt-ons for the EQ-5D-5L, EQ-5D-5L + C,7,12 Remembering things, 5 and Thinking clearly, 5 by using the scaling factor model and conventional approach. Background characteristics were similar among the three arms, demonstrating that randomization effectively balanced the groups. The prediction accuracies of the scaling factor model and conventional additive model did not appear greatly different in all three arms.
Despite the comparable prediction accuracies of the scaling factor model and conventional additive model, it is important to acknowledge that a direct comparison between them may not be entirely fair due to differences in their parameterization and the limitations of the study's sample size. The conventional additive model, which has a considerably larger number of parameters, is inherently more demanding in terms of sample size required for robust estimates. This discrepancy likely biases the results against the conventional additive model in this study. However, this observation also highlights a key advantage of the scaling factor model: it allows for the development of bolt-on value sets using smaller and more feasible sample sizes while maintaining predictive accuracy. This characteristic makes the scaling factor model a pragmatic choice for generating value sets in resource-limited settings or when large-scale data collection is impractical.
Among the five core dimensions and the cognition dimension, the rank order of CO2, CO3, and CO4 from the conventional additive model varied within each severity level (e.g., CO2 ranked 6th among MO2, SC2, UA2, PD2, AD2, and CO2 in Arm 1, and CO2 ranked 3rd and 4th in Arms 2 and 3, respectively). In contrast, CO5 ranked 2nd or 3rd in the severity level 5 in all three arms. Based on previous findings, cognition appears to be an important dimension. Previously, Krabbe et al. 6 suggested the potential importance of including a cognition dimension into EQ-5D. Another study by Finch et al. 5 examined five bolt-on dimensions (cognition, hearing, sleep, energy, and relationships), and the authors concluded that hearing and cognition had the largest impact on preferences collected from the UK general population. Other bolt-on dimensions that have been examined include sleep, 3 vision, hearing, and tiredness, 4 and psoriasis. 18
Additionally, in a conventional model, adding a cognition bolt-on resulted in the rank order changes in the two core dimensions (SC4/SC5 and UA4/UA5 in Arm 1). Although this change was only observed in Arm 1, there are several potential explanations for these findings. First, the observed reversal may be related to the lead-time TTO (LT-TTO) valuation, which involves valuing health states as worse than death (WTD). The formal QC process provided by EuroQol revealed that, during their practice interviews, some participants may not have fully understood the concept of WTD. Therefore, this concept was carefully explained to participants. Second, the preferences of the general Japanese population for health states may have been shifted over time. Approximately ten years have passed since the previous valuation studies were conducted.10,11 Third, the relatively small sample size in our study may have led to our findings. Alternatively, it is also possible that structural differences in our study with cognition bolt-ons and the previous study with five dimensions10,11 may have contributed to the rank order changes. Thus, the bolt-on dimensions may have an interaction with five core dimensions. We however used conventional additive models, assuming that no significant interaction exists between the bolt-on dimensions and the EQ-5D core dimensions. Further evaluations are warranted.
The inclusion of a cognition bolt-on in the EQ-5D-5L descriptive system has notable implications for the sensitivity to cognitive health conditions. Specifically, the addition of this bolt-on results in lower health utility values across all health states compared with the original EQ-5D-5L value set. This adjustment enhances the system's ability to reflect the impact of cognitive impairments on health-related quality of life. Consequently, in cost-utility analyses, interventions targeting cognitive problems that result in significant improvements or resolution of these conditions would yield larger changes in utility. This, in turn, could improve the incremental cost-effectiveness ratios of such interventions, reinforcing the relevance of the cognition bolt-on in capturing the health benefits derived from interventions addressing cognitive issues. These findings highlight the potential utility of bolt-ons for tailoring generic preference-based measures to better capture the nuances of specific health domains. The utility of bolt-ons, including descriptions of cognition dimensions, is an area for further research.
Although further discussion regarding the above discrepancies and the methodologies is required, the use of the former model as a method to estimate bolt-on value sets presents a comparable approach as well as a novel and resource-efficient approach. The standard approach requires a full-scale valuation study with a large general population sample. Additionally, value sets generated from the standard stand-alone approach may become inconsistent with existing ones, and the rank order after bolt-on may change due to sampling methods or interviewer effects.17,19 In contrast, the scaling factor model builds upon existing EQ-5D value sets, preserving the dominance relationships among five core dimensions. 9
Limitations
This study has limitations in addition to those discussed above. Generalizability of the results may be limited. There may be some bias in the selection of the general Japanese public, as the interviews were conducted with residents of only three cities. We selected the two largest cities (Tokyo and Osaka) and one small-sized city (Kumamoto), considering geographic and demographic perspectives to minimize selection bias as much as possible. However, rural populations were not included. As aforementioned, a direct comparison between the scaling factor model and conventional model in terms of prediction accuracy may not be entirely fair due to differences in their parameterization and the study's sample size. Additionally, the existing value set was obtained using a previous version of the EQ-VT protocol, whereas our study used the updated version 2.1. Due to the changes in cTTO tasks, 16 there may be some issues in applying the scaling factor model.
Conclusions
This experimental study examined valuation methods for creating value sets for the Japanese population. The results suggest that a scaling factor model may offer a comparable method to the conventional modelling approach, and the scaling factor model could be used to calculate “bolt-on” QOL scores. Further experimental valuation studies using the scaling factor model and cognition items are warranted.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251365548 - Supplemental material for Valuation of cognition bolt-ons for EQ-5D-5L in Japan: A comparative analysis of scaling factor and conventional models
Supplemental material, sj-docx-1-alz-10.1177_13872877251365548 for Valuation of cognition bolt-ons for EQ-5D-5L in Japan: A comparative analysis of scaling factor and conventional models by Ataru Igarashi, Aureliano Paolo Finch, Zhihao Yang, Yukinori Sakata, Mie Azuma-Kasai, Kiyoyuki Tomita, Mika Ishii and Manabu Ikeda in Journal of Alzheimer's Disease
Supplemental Material
sj-xlsx-2-alz-10.1177_13872877251365548 - Supplemental material for Valuation of cognition bolt-ons for EQ-5D-5L in Japan: A comparative analysis of scaling factor and conventional models
Supplemental material, sj-xlsx-2-alz-10.1177_13872877251365548 for Valuation of cognition bolt-ons for EQ-5D-5L in Japan: A comparative analysis of scaling factor and conventional models by Ataru Igarashi, Aureliano Paolo Finch, Zhihao Yang, Yukinori Sakata, Mie Azuma-Kasai, Kiyoyuki Tomita, Mika Ishii and Manabu Ikeda in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We appreciate Dr. Kim Rand from Maths in Health for his support in data analysis and Clinical Study Support, Inc. for their support in project planning, administration, data collection, statistical analysis, and medical writing. We also thank INTAGE Healthcare Inc. and interviewers for their contribution in data collection. All the contributions were funded by Eisai Co., Ltd. and Biogen Inc. A part of the abstract was presented at the ISPOR Europe 2024 conference in Barcelona, Spain.
Ethical considerations
The use of EQ-5D-5L cognition bolt-on version was granted by the EuroQol group (Rotterdam, Netherlands). This study was part of the research “Efficiency and Optimization of Care in Nursing Homes from the Perspectives of QOL and Medical Economics”, which was approved by the ethics committee of the Graduate School of Pharmaceutical Sciences, The University of Tokyo. The study was conducted following the local Ethical Guidelines for Medical and Biological Research Involving Human Subjects.
Consent to participate
Before starting the interview, the written informed consent was obtained from each participant. Participants were free to withdraw their consent at any time up to one week following the interview.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Eisai Co., Ltd. and Biogen Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A Igarashi received research funding from Eisai Co., Ltd.; and advisory fees from Eli Lilly Japan K.K., Novartis Pharma K.K., Janssen Pharmaceutical K.K., Ono Pharmaceutical Co., Ltd., and Chugai Pharmaceutical Co., Ltd.
AP Finch is employed by the EuroQol Research Foundation and is a member of the EuroQol Group.
Z Yang received grant from the EuroQol Research Foundation in supporting this study and is a member of the EuroQol Group.
Y Sakata, M Azuma-Kasai, K Tomita, and M Ishii are employees of Eisai Co., Ltd.
M Ikeda received advisory board fees from Eisai Co., Ltd., Eli Lilly Japan K.K., Otsuka Pharmaceutical Co., Ltd., Ono Pharmaceutical Company Limited, Chugai Pharmaceutical Co., Ltd., Novo Nordisk Pharma Ltd., Shionogi & Co., Ltd., and Takeda Pharmaceutical Company Limited; honoraria from Sumitomo Pharma Co., Ltd., Eisai Co., Ltd., Nihon Medi-Physics Co., Ltd., Otsuka Pharmaceutical Co., Ltd., FUJIFILM Toyama Chemical Co., Ltd., Janssen Pharmaceutical K.K., and Shionogi & Co., Ltd.; and grants from Sumitomo Pharma Co., Ltd., Eisai Co., Ltd., and Otsuka Pharmaceutical Co., Ltd.
Data availability statement
The data used in this study are not publicly available due to privacy and ethical reasons.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.