
Abstract
Background
Receiving a diagnosis of a major neurocognitive disorder due to Alzheimer's disease (AD) brings with it the need to adjust to a new life situation. People with AD seek to (1) maintain emotionally positive goals in their current lives, and (2) use positive experiences from the past to create continuity in their lives, with the aim of maintaining their quality of life and gaining a sense of hope.
Objective
This research aims to explore the coping strategies and processes used following diagnosis.
Method
An exploratory qualitative design was implemented to study the different coping strategies used by ten people with AD, via semi-structured interviews. The transcribed data was subject to an interpretative phenomenological analysis.
Results
All participants experienced unpleasant emotions following their diagnosis. Their coping process following two different trajectories: (1) adaptive coping strategies to gain resilience and hope to maintain meaning in their current lives; (2) less adaptive coping strategies essentially resulting in the denial of the diagnosis and withdrawal from social life.
Conclusions
This research makes it possible to identify possible intervention paths adapted to an individual's needs to help them move towards adaptive coping strategies.
Keywords
Introduction
Diagnoses of a major neurocognitive disorder (MND) are steadily increasing, and estimates indicate that by 2050, the number of people affected worldwide will triple to 131.5 million. 1 Up to 75% of these diagnoses are expected to be MND due to Alzheimer's disease (AD).2,3 This dramatic increase is mainly due to the aging of the global population, since age is the primary risk factor for MND-AD.4,5
Even though longevity is steadily increasing, remaining life expectancy shortens as people age. An individual's remaining life expectancy significantly influences their perceptions of the goals they wish to achieve. According to the socioemotional selectivity theory (SST), older adults tend to prioritize goals that are emotionally meaningful and relevant to their present lives over those oriented towards a distant future.6,7 By realizing that they have less time to live, older adults tend to memorize more emotionally positive events to make sense of their lives, while also making use of their past experiences. 6 Several authors argue for the existence of a positivity effect in older individuals who draw on distant positive memories retrieved through their autobiographical memory.8,9 According to one of them, this positivity effect continues to exist in people with AD. 10 The author suggests that although these individuals quickly lose their temporal bearings in the early stages of the disease, they continue to be aware of their impending finitude, which contributes to maintaining the positivity effect. Consequently, people with AD adopt coping strategies similar to those observed in the healthy aging population to deal with the changes. They are more inclined to seek positive emotions and regulate unwanted emotions (emotion-focused coping) rather than searching for practical solutions to manage and resolve a specific problem (problem-focused coping). 11 People with AD prioritize positive experiences and emotional closeness in their interpersonal relationships, much like the healthy aging population. 10
The premise of SST complements that of the continuity theory, 12 which asserts that the recollection of positive events supports the present experience to enhance an individual's ability to adapt to a new situation, thereby maintaining external and internal stability in their lived experience. A research team recently confirmed the proposition of continuity theory with people with mild AD, contrary to the initial statement of the theory which clearly excludes people living with MND. 13 Positive memories retrieved via autobiographical memory allow them to create continuity and stability in their self-awareness despite the changes in their lives. Furthermore, according to the results of a meta-analysis, reminiscence based on nostalgic thoughts positively impacts the social connectedness and the self-esteem of people with AD; they increase meaning in life, a sense of self-continuity, optimism, and positive affects. 14
In line with these two theories, people with AD seem to tend to retain hope, particularly with regard to their well-being, autonomy and the continuity of their self-awareness. 15 These authors suggest that for people with AD, hope is aimed more towards general (societal) rather than individual goals (recovery), enabling them to preserve their values and maintain self-awareness. The aim is to preserve their well-being, or perceived quality of life (QoL) which is based on the subjective evaluation of the gap between an individual's expectations and their actual experience (i.e. chronical illness). 16 These authors found that the individual seeks to adapt to their new reality and assigns meaning to it to balance their live. Therefore, this represents a dynamic process, changing over the course of a major life event, such as the diagnosis of MND-AD. In addition, some research has highlighted the difference between the self-assessment and caregiver rating: people with AD evaluated their OoL better than their caregivers.17–19 These results suggest the need to better understand MND-AD, which is essentially based on medical and neurological models. 20 According to this author, an individual and existential approach would make it possible to adapt interventions, in particularly to preserve the humanity of people with AD. He added, when the connection to the world is maintained, it is possible for people with AD to establish continuity in their existence instead of confining them to a state of “living death”. Consequently, this would enable people with AD to maintain a better perception of their QoL, in particular by adjusting their expectations to their current experience 16 and recovering a sense of self-determination. 21 This seems to be possible by recalling positive memories and experiences from their past.13,14
This research is divided into two parts. The first part aimed to describe the subjective experience of people with AD following diagnosis, as well as the resulting consequences. The results showed that (1) all the participants experienced incomprehension, particularly in terms of the way healthcare professionals communicated at the time of diagnosis, (2) they engaged in an oscillatory movement of connection-disconnection, drawing on past experiences in particular, and (3) this movement ultimately enabled them to re-establish a sense of control and self-determination in their lives. Detailed results have been published elsewhere. 22 The present article relates to the second part of the research and aims to carry out an in-depth exploration of the coping strategies used by people with mild AD disease shortly after diagnosis, in order to gain a new understanding of the processes involved.
Methods
The present research had two objectives: (1) to explore the subjective experience of people living with MND-AD after diagnosis, 22 and (2) to better understand the coping strategies mobilized to deal with it. Interviews were conducted only once with each participant, allowing an interpretative phenomenological analysis (IPA) to address each of the objectives. 23 The interviews were conducted from a humanistic and intersubjective perspective of co-construction of meaning.24,25 The first objective was embedded in Heideggerian phenomenology, 26 and the second in continuity theory 12 and SST.6,7,9 The methodology reported below describes the process for the latter; details for the former can be found in another publication. 22
Participants
Participants were recruited in collaboration with a university-affiliated cognitive clinic located in a large urban area and serving a primarily francophone population. Ethical approval for this research was given by two local Research Ethics Committees (research center and university).
Participants were formally diagnosed with MND-AD based on DSM-5 criteria. 27 Since we sought to obtain a homogeneous sample, 28 two important criteria were required: (1) diagnosis was given less than three months ago, and (2) the disease progressed at a mild stage (Clinical Dementia Rating [CDR] = 0.5–1). To be eligible, the inclusion criteria were: (1) participants had to be at least 70 years old; (2) they had no protection mandate; (3) they were able to speak and understand French; and (4) they were able and eager to talk about their experience. In order to limit some influences in the speech of the participants about their emotional experience after diagnosis, some exclusion criteria were determined: (1) high vascular burden; (2) early-onset diagnosis of MND-AD; and (3) other physical or psychological disabilities or illnesses. For the purposes of this research, the decision was made to create a homogeneous group to better explore the phenomenon. An individual's subjective experience can be influenced by various factors, such as the existence of another chronical disease or a psychological disorder. Consequently, it is no longer clear whether the subjective experience reported by the person relates to the announcement of the diagnosis of MND-AD and the coping strategies they have mobilized to deal with it. Moreover, people who have received an early diagnosis do not necessarily experience the same reality as older adults.
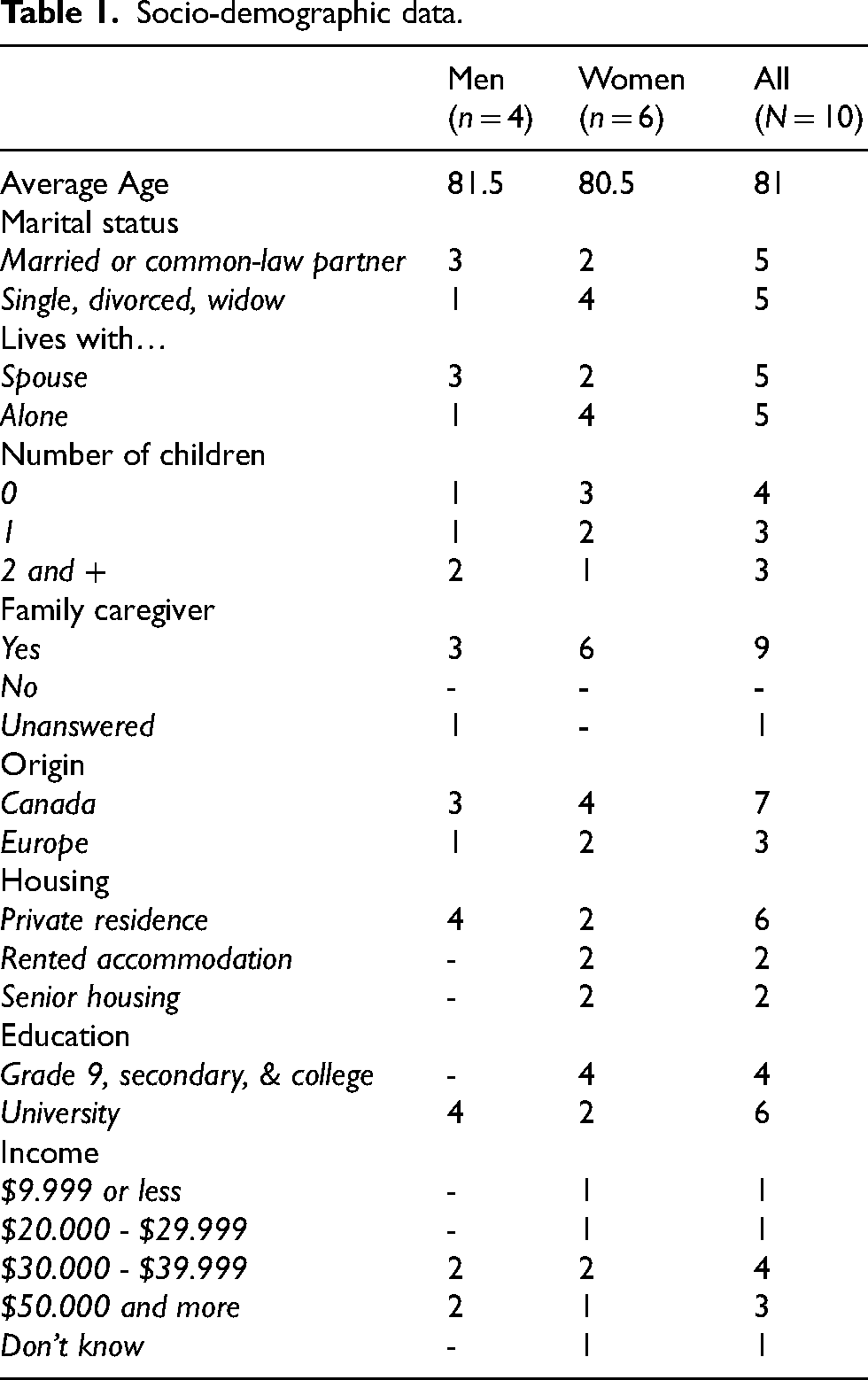
At the same time, we were looking for socio-demographic variation in the sample to explore the phenomenon from different perspectives. Given the complexity and individuality involved in a diagnosis of MND-AD and the fact that this population had not been questioned often in the past, we aimed a small sample which was nevertheless able to provide rich data.23,29 Ten community-living participants were recruited: six women and four men, aged on average of 81 years (R = 72–92 years). Half of them lived with their spouses and they all benefited on support from a relative or friend (Table 1).
Socio-demographic data.
Interviews
All semi-structured individual interviews (N = 10) were conducted by the first author with an average duration of 61 min (R = 45–100). To achieve this, a humanistic and intersubjective approach was used with the aim of exploring the individual resources of each participant to cope with the changes in their life.24,25 In fact, even if the person's narrative does not necessarily seem perfectly coherent, they communicate their way of understanding the diagnosis.30,31 Through an intersubjective approach, a co-construction of meaning is possible where each individual contributes in a different way to the construction of a common understanding. 24 One by sharing their experience, the other by interpreting the words and the understanding shared with them, thus accessing a double hermeneutic. According to the intersubjective approach, it is possible to re-establish contact with oneself through one's relationship with others.24,25 This way to conduct interviews created a high degree of proximity with the participants, enriching corpus data throughout the process. 32 Given the COVID-19 pandemic, most of the interviews were conducted by telephone (n = 5) or via videoconference (n = 2); only three participants were interviewed at their home as initially planned. The interviews were digitally audio-recorded, transcribed verbatim and checked for accuracy. 33 After obtaining the participant's verbal consent (audio-recorded), the interviewer guided the participant to explore through reflection, active listening, and an empathetic posture. 34 The aim was to get the participant to express his or her personnel experience after diagnosis and to co-construct meaning. 32 The interviewer paid attention to the particular needs during the interviews, for instance by expecting breaks and moments of reminiscence. 35 Even though the interviews were conducted remotely, the authentic, non-judgmental interest in the participants’ experiences allowed for an in-depth exploration of their coping strategies. 25 The interview ended by questioning the experience of each participant about the process and his or her actual feelings. Indeed, it was important to conclude in a way that allowed the participant to feel balanced. It was therefore necessary to ensure that the person did not have any unpleasant emotions or feelings which may have emerged during the interview.
Data analysis
The data was analyzed from the perspective of IPA. 23 Unlike a classical phenomenological approach, the IPA is part of a double hermeneutic which enables the researcher to interpret the meaning reported by the participants as they try to make sense of their experience bringing out a common understanding. This interpretive element is particularly suitable for an in-depth understanding of the subjective and emotional experience of people with AD.36,37 It made it possible to go beyond the cognitive self, particularly affected in MND-AD, to co-construct the meaning of lived experience based on the experimental self which is less affected by the disease.37–39
The analysis was conducted following the steps suggested in IPA: first, the immersion in the corpus data and the draft of exploratory notes; then, the development of themes and their combination to link them to the research question; and finally, the repetition of these steps with each participant to understand the recurrence through all analysis. Details of analyses can be found in the first published part of our research. 22
Criteria for rigor
The data analysis was governed by several rigorous criteria to obtain reliable results. Throughout the process a special emphasis was placed on authenticity, through the identical and ontological treatment of each participant's experience. 32 Reflexivity was documented by regular notetaking, which made visible the influence of the researcher's thoughts on the analysis process. Information power was another important criterion for rigor. This is defined by the size and specificity of the sample, the quality of the interviews, the rigor of the analyses, as well as the theoretical contributions. 40 Regular discussion of results within the research team and reflexivity based on the field notes has increased their trustworthiness. 32
Finally, transferability and naturalistic generalization were targeted.29,32 The in-depth description of each individual experience and its interpretation allow caregivers, professionals or policy makers to transfer the results of this research as per their understanding and to adapt them to their environment and reality. 39
Results
Participants experienced unpleasant emotions and feelings following the diagnosis of MND-AD (M = 2.35 months from diagnosis). To begin with, these emotions and feelings are described and illustrated. Then, will follow the description of the engagement in a coping process in which they required different strategies. Finally, the converging and individual goals of this process are illustrated. The coping process following the diagnosis does not appear as a linear progression or as a chronological sequence. Participants seemed to navigate back and forth between the experienced emotions and feelings and the adjustment of the coping strategies used (Figure 1).
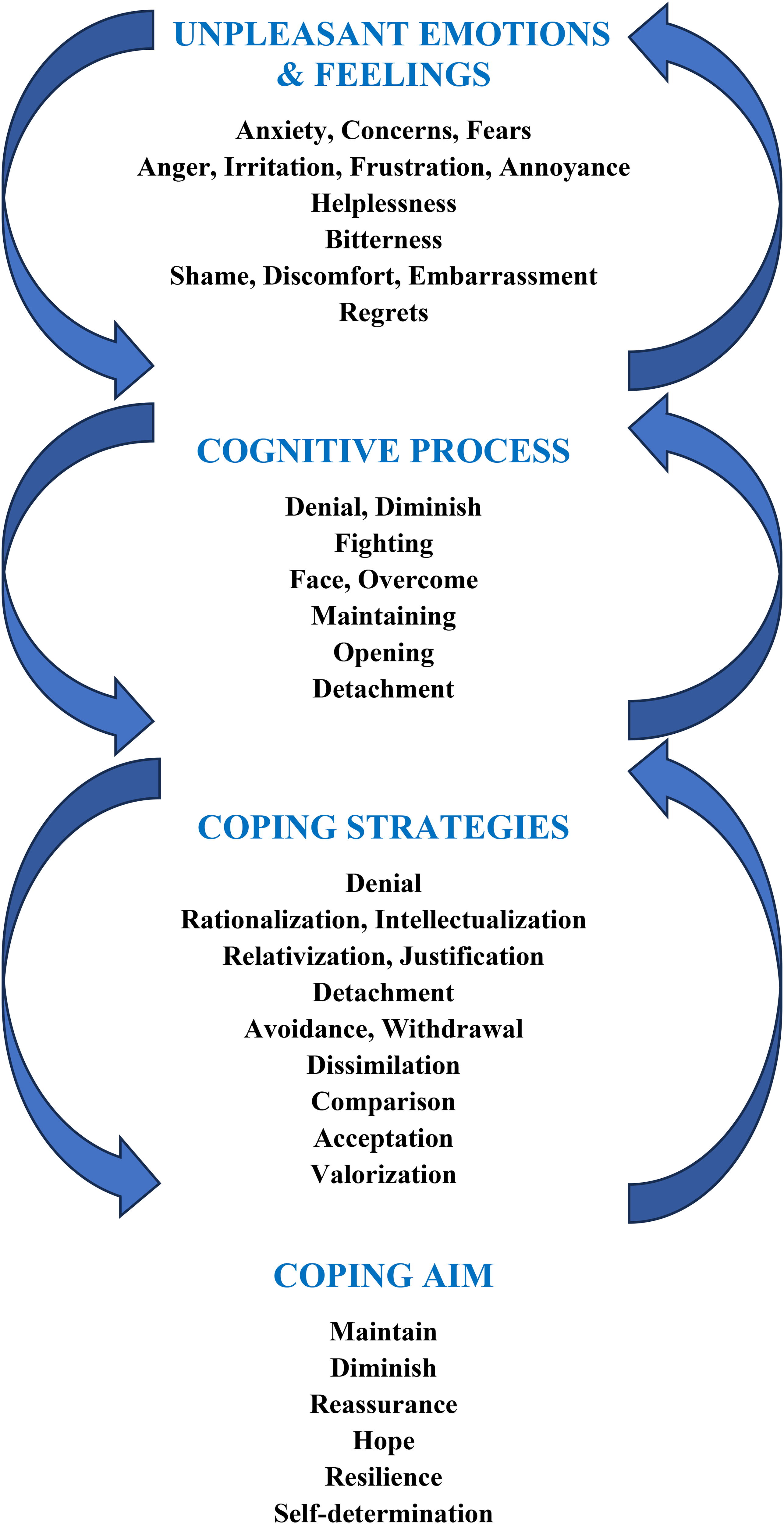
The schematic representation of the coping process following MND-AD diagnosis.
“Just to say that I wish it were otherwise, because I know very well that it cannot be otherwise”: Unpleasant emotions and feelings following the diagnosis
A diagnosis of MND-AD caused many unpleasant emotions and feelings for the participants such as anxiety, worry, fear, but also frustration, irritation, and anger. Feelings such as helplessness and insecurity, bitterness, shame, embarrassment, and regret were also noted.
The anxiety experienced was often linked to symptoms that the person had noticed in themselves for some time or that had been raised during the medical assessment, as illustrated by Phillip
i
:
That examination revealed a certain number of things to me [clears throat] – not fundamental issues – but indeed a number of weaknesses in terms of memory problems, ultimately.
ii
The observed symptoms were memory and word loss, as well as a perception of diminished autonomy in everyday life. In several cases, the decrease in cognitive and physical abilities led to the withdrawal of driver's licenses, an experience often perceived by participants as a deprivation of their freedom and independence. Moreover, the participants were worried about the development of the disease; they particularly feared a decline, which represented a risk of self-loss for them, and a decrease in their ability to manage their lives independently: Over time and with the years, with all of those things you’re completely lost as a person. Now I am… you know, I've forgotten. Until a year ago, I didn’t have any problems. (Pierre)
In other words, participants were aware of the risk of becoming dependent on their loved ones. This made them more fearful about how their loved ones would see them and how they might be judged, especially if they don’t feel like doing a certain task or simply don’t feel capable:
My famous friend who keeps an eye on me and who is there for me would like me to write everything down, all the time. Well, I can’t do that. (Ursula)
This participant frequently experienced frustration and irritation, especially when it came to how she felt about the loss of her abilities, particularly in terms of communication. These were crucial for maintaining connections with others and expressing her thoughts, emotions, and needs:
What irritates me the most is when I'm looking for words and can't find them. I need to find a way to explain to the other person what I mean. This is what is most different in my life.
Monique felt frustrated with her loss of memory, which she felt reduced her ability to communicate and connect with others:
For example, there are names that I sometimes miss. If I experience something — I know who, I know what. But names are perhaps the most difficult. People's names.
For her, a sense of powerlessness manifested as a consequence of concerns about the future and frustrations stemming from perceived loss:
Well, I try. I live today, so I try not to hurt myself too much with the past. I can't change it. I can't do anything about it. I can't do anything anymore. Why can't I do anything?
Some participants, like Mathilda, felt more discomfort about having to rely on the assistance of others instead of being able to help others as she had been accustomed to doing before. She always tells me: “If you need anything, call me”, but I'm a person who doesn't like… to call someone for small things.
Her current condition and feelings meant she was unable to take care of herself independently. Many participants had regrets about their past, both socially and professionally. They seemed to have lost their sense of purpose which had allowed them to define themselves individually, both in their personal lives and as members of society. Their sense of worthlessness and the feeling of being sidelined from society gave them bitter thoughts. These mainly revolved around their specific disease-related condition, but also around aging and their loss of status in the active world:
I’ve let go of many of my connections… I had lots of contacts from colleges that specialized in my field, with my research center that I created. This is less and less the case. (Gérard)
This feeling of being sidelined and withdrawn gave Gérard a heightened sense of loneliness:
We go for walks or go cycling, but… you’re alone [laughs]. […] It's boring, but you’re alone [laughs].
To learn to live with their unpleasant emotions and feelings, and eventually cope with them, a cognitive process was engaged in all participants. This appeared to support their lived experience and help create meaning despite their negative emotions and feelings, to maintain self-awareness and identity.
“I hope so, but it's true that we lose on an intellectual level”: Cognitive process
When participants were confronted with unpleasant emotions and feelings, their cognitive processes moved in different directions. They sometimes seemed to be triggered consciously, and in other cases, unconsciously. Some participants were in denial of their diagnosis and others tended to diminish the importance that the diagnosis and related symptoms could have on their lives, for example, they attributed their difficulties to other, often physical, causes:
My doctor sent me to hospital, and I had a magnetic resonance imaging scan. He told me that my brain was affected a little and because of that, I have been a bit… I was going to forget things. (Mathilda)
For others, to lessen or eliminate their suffering, they ascribed the reasons for their current condition to a normal aging process. This was a noticeable process in Josée: You experience fewer things, including old age… Which is not necessarily negative… I look at myself and I can't complain. I’m lucky.
Some thought processes appeared to be more active and conscious, including the efforts made by some participants to fight their condition to overcome it, even if they were aware of certain difficulties: I don’t hide my… what I no longer know how to do or what I no longer want to do or what I think is not correct or that I don't agree with. But no, I haven’t reached that point, I haven’t reached… But it's true that sometimes it takes me some time to find my glasses. (Ursula)
Other participants turned to openness and detachment to continue living and so as not to sink into despair, fear, and worry. Gérard illustrates his understanding of the diagnosis and related symptoms, which then allowed him to focus on finding solutions to compensate for his difficulties: It didn't surprise me because at my age it's not unusual except you must compensate. You have to write down what you have to do… on paper to make sure you have it somewhere… You have to compensate, but by compensating, it's corrected and that's good.
Monique clearly illustrates her willingness to live in the moment by accepting her diagnosis and her disease while detaching herself from the seriousness she feels, as well as the worries and fears. She attempts to live in the present by integrating her new living conditions and its limitations:
I have trees, so that's all I can see. It's a pleasure to see all these trees every day, that's it. So, despite everything, I don't think I'm that bad. I'm quite proud of myself, of how I react. I don't want to fight anymore: it's not perfect but that's how it is.
A cognitive process had been triggered in all participants which allowed them to get through the period following the diagnosis of MND-AD, a period fraught with unpleasant emotions and feelings. They were able to move towards coping strategies that led them to integrate this new reality into their lives.
“I feel it, especially other peoples’ reactions […], but I have to accept it”: Coping strategies
Participants used different coping strategies, described in this section, to cope with the diagnosis and the disease. Most participants used minimization, rationalization, and justification strategies which allowed them to relativize their experience, making it more bearable. They often tried to explain the difficulties they were experiencing as having physical causes, such as falls or head injuries:
I hit my head and face and bam. (…) Yes, it hit my brain and that's why I’m doing all this. (Mathilda)
For others, like Ursula, the disease started in an insidious, barely perceptible way:
So, I was falling because I lost my balance. Because [I was] always falling on my head, an illness gradually developed. It took years.
Most often, participants minimized their difficulties and symptoms to reassure themselves and to demonstrate that their functionality was maintained to those around them, but also to themselves:
That's how my memory works, written down. In fact, it's been like this for quite a while. (Phillip)
Minimization became apparent as participants sought to regulate their grieving process regarding various activities that were no longer within reach, including driving, professional recognition, and maintaining their social circle and specific relationships.
It wasn't very dramatic at all, because anyway my wife drove most of the time before and now, she drives all the time [laughs]. (Gérard)
This strategy enabled them to maintain or create positive thoughts and emotions associated with their current experience. To create this positive outlook, participants drew upon pleasant and rewarding memories from their past to reinforce their sense of purpose and well-being in the present. Memories of pleasant social relationships or enjoyable activities helped establish meaning and continuity in their lives. On the other hand, some participants were more likely to use distancing, detachment, avoidance, or withdrawal strategies, hindering them from confronting their new reality: I've [clears throat] seen it happen before. And the way the world is heading, I don't know if I'm interested in living in this world… or maybe because I'm too old, or perhaps I was never interested anyway. (Josée)
To maintain a sense of self and preserve their identity awareness, participants can resort to comparison, either in a general sense to standards and stereotypes.:
Because there are many people – artists, painters – who have worked until they’re 90. Imagine it wasn’t perfect anywhere… the judgment was… […] The judgment is there, you understand, creativity remained, only the memory and the power… (Pierre)
This can be in relation to the people around them, especially if they felt confronted with their own finitude:
[My mother] passed away, I think she was 83-84. So, I think about it, but… I think I'm better than she was at my age. But you don't know what's going to happen [laughs]. (Ursula)
Some participants, like Monique, were going through a process that resulted in the acceptance of her current condition, which seemed to lessen her suffering and set a new standard for preserving her QoL:
I had a good memory; so, finding that out was quite something. So, I cried for two days and after that – well, I have no choice; I have to take it on board [laughs] – I have to accept it, I try to live my life the best way possible; then we'll see because…
Acceptance also served the purpose of maintaining the person's identity, even if they were aware of changes in their current life, particularly in relation to their ability to perform daily tasks:
And it doesn't irritate me at all, it doesn't change me in any way. What has changed is that I am much slower. I live my life quietly [laughs]. I'm not in a hurry anymore: that's the difference. It takes me longer to put my things away. (Ursula)
Another strategy for maintaining a good self-image and preserving identity was to place value on the capabilities which remained. Participants seemed to place greater emphasis on achievements than the loss of certain abilities:
I can remember things in the past, as I told you. My long-term memory isn’t any worse. But for the present, that's it [awkward laugh]. (Monique)
Coping strategies that allowed participants to establish continuity in their lives and maintain a positive self-image appeared to promote an emergence of resilience. Resilient attitudes helped to give their lives new meaning, to re-establish a sense of purpose and thus to find positive aspects in their lives: My children are careful… They no longer ask me about things I used to do. They come and bring my groceries and things like that but for example, every Sunday evening, I tell the grandchildren tales and that is becoming more and more important, it's very pleasant. (Gérard)
The coping strategies used to deal with unpleasant emotions and feelings aligned with individual goals which provided participants with a sense of adaptability to their new reality. These strategies allowed them to maintain a sense of usefulness, give meaning to their identity to continue finding purpose in life, preserve their autonomy, and uphold an acceptable QoL.
“I try to live my life the best way possible”: Objectives of coping strategies
There were diverse underlying objectives for implementing coping strategies among the participants. They aimed to maintain normalcy and create continuity in each participant's life. For some participants, it seemed crucial to live with the hope of retaining the ability to preserve their autonomy, independence, and a sense of usefulness in their existence. This gave them the feeling of maintaining control and power over their lives, specifically accessing a sense of self-determination. Thus, they could adjust their expectations realistically and feel reassured, fostering the emergence of hope.
For several participants, it was essential to maintain their autonomy and abilities to manage their daily lives while remaining open and willing to seek or accept help from others for certain tasks that were more difficult or inaccessible:
I try to handle my stuff on my own because I'm that kind of person, but if I need help, there are people; they’re happy to give me a hand. What more could you want? (Ursula)
Although asking for support for certain tasks seemed necessary, Paule illustrates the importance of balancing the help she received and carrying out certain tasks on her own to maintain her autonomy and thus maintain a sense of usefulness and pride:
We have a cleaner. But for the rest, I manage: I make food then…. It's okay as it is, I don't want any more.
Gérard stressed the importance of finding tools that help him function better in his daily life. Compensation strategies were widespread and useful to participants; for example, most of them had gotten into the habit of taking notes or keeping a diary:
Sometimes I forget to make a note [laughs], but it's important to do so, you must compensate. It's important for older people to find a way to maintain autonomy by compensating for the losses we experience, whether it be in terms of memory or physical abilities.
Furthermore, Monique recalled the importance of living in the moment to make it possible to appreciate her life as it is now, despite the diagnosis of MND-AD, and so reduce her suffering:
I try to take it one day at a time [laughs]… yeah one day at a time. Sometimes it's just an hour at a time [laughing].
Conversely, some participants used avoidance and withdrawal strategies to retreat from their social lives. Their goal was to maintain the balance of their current lives, without having to confront their difficulties related to the diagnosis and symptoms of the disease. I prefer to stay at home and be on my own because I live alone and… that's how it is. It isn’t easy. (Mathilda)
Through withdrawal and avoidance strategies, these participants appeared to have some stability in their current lives—but they did not feel that they had control over their lives or were able to act in a self-determined manner. They lived more with a sense of failure, hopelessness, and loss of control. Lisette refers to the lack of social contact and limited activities in her day, such as reading the newspaper or watching television. She experienced her situation as an inevitability, which she constantly illustrated in the following way:
One day at a time, we can't change that.
To summarize the aims of coping for the participants, they all showed a kind of fight against unpleasant emotions, feelings and the heaviness of the diagnosis using individual coping strategies. Sometimes, participants accepted the diagnosis, and were then able to face their illness, showing a better ability to cope with their difficulties and accessed to resilience. On the other hand, participants with more denial or refusing behavior and thinking seemed living with more distress and were less able to develop adapted coping strategies to face their difficulties and to maintain a good QoL.
Discussion
The objective of the second part of our research was to obtain a better understanding of the coping strategies mobilized by people with AD to deal with their diagnosis, especially by exploring the adaptation processes deployed (results of the first part can be found in another publication 22 ). The present findings made it possible to describe and differentiate these strategies to establish trajectories that appear to be more adaptive. The unpleasant emotions and feelings experienced by participants following their MND-AD diagnosis were apparent, ranging from anger to shame to anxiety. Participants engaged in a cognitive process that led them to coping strategies to deal with these unpleasant emotions and feelings to adapt to their new reality. Each participant used their own individual strategies. Some seemed more adaptive than others, giving way to resilience among other things. Adaptive trajectories contributed to the maintenance of a good QoL which was based on a sense of self-determination and maintaining or regaining control over their lives. The results of this research are in line with those reported by a research team suggesting that self-determination and control over one's life are associated with the well-being of people with AD. 30
Through adaptive coping strategies, it was possible to observe a positivity effect in the participants.6,10 This positivity bias allowed participants to assign new meaning to their current experience based on positive memories of their past. 13 According to the SST, in order to maintain this positivity bias, some negative information is eliminated.6,7 It is possible that this “sorting” of information may have been part of a sort of denial for some participants. Several of them claimed that they had not been informed of their diagnosis. Although this is possible, this omission could also be explained by the presence of anosognosia specifically related to the diagnosis and/or by the influence of positivity bias in the triggering of denial cognitions. Anosognosia, like denial, refers to a poor awareness and loss of insight. 41 The psychological concept of denial describes a mechanism that enables the individual to adapt to a threat to his identity.42,43 For the time being, there are no models or measures that can diagnose anosognosia or clearly explain its neurological origin or to differentiate it from denial.41,44–46 A research team reported that the presence of anosognosia is linked to a poor ability to adapt compared to individuals without anosognosia.41,47 A similar observation was made in the current research: participants who deployed more coping strategies related to the denial of diagnosis and withdrawal from social life reported greater difficulty in completing tasks in their daily lives, while tending to overestimate their current abilities. The results from one study suggest that, individuals with anosognosia have a better QoL. 41 In contrast to these statements, our participants who lived in denial of their diagnosis communicated a worse QoL than participants who were aware of it. This seemed to be related to a tendency to withdraw from social life and a sense of loss of control and hope that they experienced. It is essential to clarify these two concepts and to better understand the role they play in helping people with AD adapt to the diagnosis, and to offer them the support they need.
However, regardless of whether they were in denial or coping with their disease, participants recalled past experiences to adjust to their reality and make sense of their current lives. This allowed them to create continuity in their existence and identity. The results are in line with those reported by Robertson (p. 538): “The accomplishment of a ‘good’ quality of life involves looking backwards to sustain continuity with the past and looking forwards to maintain momentum and keep going". 48 Looking to the past allows people with AD to create continuity in their present and give meaning to their current and future lives. Contrary to the continuity theory 12 which argues that people with AD are not able to use their experience (memory loss), needed to make sense of their present (internal change), the findings of the present research suggest the opposite. Indeed, it seems that people with AD can continue to find meaning in their lives by recalling and relying on their experiences. This would allow them to maintain a sense of identity and thus continuity in their existence, as suggested by the continuity theory. Despite their cognitive and mnemonic losses, people with AD seemed to be able to create continuity, by giving a sense to their present and future by relying on their past experiences.
These results provide avenues for improving interventions for people with AD as described in the next section.
Implications for practice
People with AD who used adaptive coping strategies, gained access to a form of resilience and hope that allowed them to regain control over their lives. As discussed, the positivity bias 6 as well as the need for continuity in their lives 13 seem to have influenced their trajectory thus facilitating the adaptation to their new life reality. By referring to these coping trajectories, it is possible to support people who use less adaptive coping strategies, to help them improve and develop better ones. At the same time, it is important to maintain or even improve those of people who are already using adaptive coping strategies. Communication-based interventions could help trigger cognition related to positivity bias, for example by raising the positive consequences of a planned action along with an individual's strengths and resilience—based on positive experiences in the past—as seen in Gérard or Monique. By allowing people with AD to regain a sense of control over their lives and by promoting self-determination, adaptive behaviors could emerge that allow them to develop resilience and hope.
To support people with AD at the beginning of the disease, the results of a meta-analysis emphasize the importance of nostalgic reminiscence, which appears as an adapted intervention possibility. 14 Participants are guided to retrieve positive memories to decrease their psychological distress and increase their perceived QoL. Several research teams suggest that this form of therapy may be effective with people with AD as their cognitive abilities improved, their depressive symptoms decreased, and their satisfaction with life increased (i.e., subjectively perceived QoL).14,49–51 They would maintain continuity in their lives 13 through positive memories, which appears in line with the positivity bias 10 and that could even be enhanced. That way, people with AD would maintain or regain a sense of purpose and self-determination. This could enable them to improve their self-esteem and, consequently, feel better in their lives, which would regain its meaning. 14
Furthermore, results of a research have proposed that instrumental reminiscence therapy could be beneficial for older individuals, enhancing their adaptive coping strategies when confronted with the challenges of aging. 52 This therapy specifically targets the retrieval of effective coping strategies used in difficult situations in the past. The researchers point to the emergence of a sense of self-determination and regained life control among participants, which had improved their perceived QoL and fostered the emergence of resilience and hope. However, this research was conducted with older adults without cognitive loss. Nevertheless, participants in the present research reported a better QoL when they were able to regain control over their lives, in particular by relying on coping strategies that had worked for them in the past. In future research, it would be interesting to evaluate the efficacy of instrumental reminiscence therapy to improve adaptive coping strategies in people with mild AD.
Strengths
This research sheds light on different coping strategies used by people with AD shortly after being diagnosed. It was possible to delve into each individual experience without generalizing. These findings highlight the importance of listening to the life-history of the concerned people, mostly their emotional experience to offer them an intervention focused on their individual needs.
In addition, different teams of researchers have raised the importance of maintaining a sense of continuity based on positive memories by strengthening self-determination in people with AD.10,13,48 One research team, using The Thinking about Life Experiences Scale (TALE), assessed the role of autobiographical memory support in relation to a sense of self-continuity. 13 Another author specifically investigated the existence of the positivity bias in MND-AD to allow people with AD to adapt more based on their emotional experience. 10 Finally, a third one proposed an interesting case study with a single person with AD in which she suggested the importance of using past memories to make sense of an individual's present. 48 However, the research that focuses directly on the experiences of people with AD is rare and uses different methodologies. This second part of the research, using semi-structured in-depth interviews, provided an in-depth and individual understanding of the coping strategies used by people with AD. In doing so, it sheds new light on a largely understudied field of research.
Recruiting people with AD is challenging. During the research, the first contact often needed to be with caregivers who feel unsure about the involvement of their unwell loved one. Persistent stereotypes about the ability of people with AD to participate in interviews that require some communication skills and a good insight and awareness of the self were often conveyed, both by loved ones and by the person themselves. 37 This research challenges these stereotypes or false beliefs; it has been shown that it is possible to conduct in-depth interviews with people with AD and to obtain a discourse that allows us to better understand what they are experiencing. More research like this is needed to better understand the emotional experience of people with AD after diagnosis, but also during the progression of the disease. With better understanding of these elements, it would be possible to grasp and support the emergence of coping strategies to be able to offer help that better targets the specific needs of each individual.
Research limitations
As part of this research, ten Francophone people were interviewed. They all lived in an urban environment in Quebec, Canada. The results obtained are descriptive and individual; they are not representative of other populations in a different context who are living with MND-AD (e.g., institutionalized or from other cultures) or people who have been diagnosed with MND differently from AD.
Most of the interviews were conducted by telephone due to the Covid-19 pandemic, which represented an obstacle to build a relationship of confidence with the participants, enabling them to explore and share their experiences. However, active, authentic listening and a sincere interest in each individual helped to establish the necessary emotional closeness between the interviewer and each participant.24,25,37 Moreover, analysis had to be carried out without access to the participants’ environment, which represents a valuable loss of material. In future research, it would be interesting to add these observations to provide additional information.
For this part of the research, participants were met only once; the reported results illustrate a specific moment in their lives. Further longitudinal studies are needed to better understand the fluctuations and evolution of coping strategies used according to the daily challenges encountered in relation to the symptoms of the disease or modifying according to the different stages of the disease.
Conclusion
This research sheds important light on the coping strategies used by people with AD following their diagnosis; interviews were conducted with them to co-construct meaning and to give them back their voices. It takes a fresh look at their subjective experience and the coping strategies used to deal with a recent MND-AD diagnosis that inevitably changes their lives.
Footnotes
Acknowledgments
First of all, we would like to express a huge thank you to all participants for their involvement, openness, and authenticity; we were truly touched by your stories and experiences!
Furthermore, we thank Manon Fleurent and Dr Nancy Vasil (IUGM) who facilitated the recruitment of participants. We would like to express our gratitude to Catherine Dupuis-Fortier and Lina Boyer for their involvement in interview transcripts.
Ethical considerations
Ethical approval for the research was given by two local Research Ethics Committees: (1) Ethical committee, CRIUGM: CER VN 19-20-26, October 15, 2019; (2) Ethical committee in psychology, University of Montréal: CEREP-19-114-R, October 22, 2019.
Consent to participate
All participant's gave an informed verbal consent (audio-recorded) to their participation in the research.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by the Advisory Committee for Clinical Research (CAREC), IUGM Research Centre under Grant # UA300287. The first author was supported by the Alzheimer Society Research Program (ASRP) Doctoral Award, Alzheimer Society of Canada under QoL Regular Grant #20-11. Dr Sébastien Grenier is supported by an FRQS Senior salary award.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.