
Abstract
Stress is a known risk factor for Alzheimer's disease (AD), but religious stress coping practices, (e.g., prayer and attending religious services) may reduce this risk. We investigated the relation between religious stress coping and memory in cognitively-unimpaired individuals from the Colombian kindred with autosomal dominant AD. Additionally, we examined the link between religious stress coping and brain pathology. Religious coping was associated with lower entorhinal tau (p = 0.02) and better memory performance (p = 0.04) in Presenilin-1 E280A mutation carriers, but not in non-carriers. These findings suggest that religious coping may mitigate AD tau pathology and cognitive decline and warrant further investigation.
Introduction
Alzheimer's disease (AD) contributes to 60–70% of cases of dementia, and dementia is projected to afflict 139 million individuals by 2050.1,2 Identifying modifiable factors of risk is critical given increasing evidence that AD-related brain pathology (i.e., amyloid-β and neurofibrillary tau) accumulates years before dementia symptoms emerge.3–7 Chronic stress may elevate the risk of cognitive decline and dementia, with high stress linked to increased amyloid-β burden.8–12 Stress coping, defined as the ability to manage stressors or recover quickly from a stress response,13,14 can foster resilience against the harmful biological effects of stress and is associated with low tau deposition in older adults with increased AD risk.15,16 However, research examining specific stress coping strategies and brain pathology in those at increased risk of AD is non-existent. Effective stress coping strategies may provide resilience for those at greater risk of dementia and may point the way to the development of novel prevention interventions.
Religious stress coping (i.e., the use of religiosity for stress management) may be an effective coping strategy. Religious beliefs can inform cognitions and appraisal of stressors 17 and commonly foster mindfulness, compassion, acceptance, forgiveness, and higher meaning, which comprised a successful stress reduction intervention. 18 Studies also suggest that religious and spiritual activity may protect against cognitive decline. 19 For instance, Rajkumar 20 found that activities such as attending religious services and daily prayer relate to low dementia rates, independent of depression or social cohesion. In persons with AD, more religiosity is linked with slower cognitive decline and better functioning in multiple cognitive domains.21–23 These effects have been shown to vary based on racial background and gender, 24 which suggests that cultural and social identities may influence the relation between religiosity and cognition.
Despite positive cognitive outcomes associated with religiosity, the relation between religious stress coping and cognitive performance in the preclinical stage of AD has not been examined. Investigating this coping strategy in cognitively-unimpaired individuals with autosomal dominant AD (ADAD) could shed light on its role in preclinical AD. The Colombian kindred with the Presenilin-1 (PSEN-1) E280A mutation is an ideal study group, as it is the largest known ADAD cohort and features well-documented disease progression6,25 with a median age of onset for mild cognitive impairment (MCI) at 44 years (95% confidence interval [CI] 43–45) and for dementia at 49 years (95% CI 49–50). This population is predominantly religious, with most adults actively practicing their faith, 26 which may enhance the relevance of religious stress coping in their lives.
We examined whether religious stress coping could differentiate cognitively-unimpaired PSEN-1 mutation carriers from non-carrier family members, assessed the relation between religious stress coping and amyloid-β and tau accumulation, and examined associations between religious stress coping and cognitive performance. We hypothesized that there would be no differences in religious stress coping levels between groups given the ubiquity of religiosity among the population. 26 Based on literature linking better coping with lower pathology in individuals with elevated AD risk, 15 we predicted that greater religious stress coping would correlate with lower pathology in carriers but not non-carriers. Given evidence that religiosity may protect against cognitive decline, 19 we hypothesized that greater religious stress coping would be associated with better cognitive performance in carriers as they are predisposed to early cognitive dysfunction unlike non-carriers.
Methods
Participants
Participants included 40 PSEN-1 E280A mutation carriers (24 females) and 45 non-carrier family members (25 females) from the Colombia-Boston (COLBOS) Biomarker Study. The study was cross-sectional in design. Cognitive data was collected at participants’ baseline visit and neuroimaging was collected within 3 months of baseline. All participants were classified as cognitively unimpaired by a Functional Assessment Staging Test (FAST) 27 score of 2 or lower, a Mini-Mental State Examination (MMSE) 28 score of at least 26/30, and a performance of 1.5 standard deviations within the mean on the Spanish version of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) word list delayed recall test. 29 Individuals with major neurologic and psychiatric disorders were excluded.
Standard protocol approvals and participant consent
This study was approved by the institutional ethics review boards of Massachusetts General Hospital in Boston, Massachusetts, and the University of Antioquia in Medellin, Colombia. All participants provided signed informed consent. All measures were administered in Spanish by trained bilingual staff who were blind to the participants’ genetic status. Participants were also blind to their genetic status.
Measures of religious stress coping, cognition, and mood
Cognitive measures and questionnaires were administered at the University of Antioquia in Colombia. Religious stress coping was assessed using the Religious Coping subtotal of the Coping Strategies Questionnaire (CAE). 30 The CAE is a 42-item questionnaire in which participants respond to the question: “How have you habitually behaved in stressful situations?” Responses are scored on a 4 point scale (0 = Never, 1 = Rarely, 2 = Sometimes, 3 = Frequently, and 4 = Almost Always). Each of the seven subtotals, including the Religious Coping subtotal, consists of six questions (maximum score of 24). A higher score means the individual engages more in the coping strategy. The religious coping items are as follows: 1) “I attended church,” 2) “I asked a religious person (priest, etc.) for spiritual help,” 3) “I went to church to pray/ask for the problem to be resolved,” 4) “I had faith that God would remedy the situation,” 5) “I prayed,” and 6) “I went to church to place candles or pray.” Sandín and Chorot reported good internal consistency for the CAE's Religious Coping subtotal with a Cronbach's alpha of .86. 30 The Spanish version of the CERAD word list delayed recall test 29 was used as a measure of verbal memory. The 15-item Geriatric Depression Scale (GDS)31,32 was administered to assess for depression.
Brain imaging
A subsample of 34 participants completed neuroimaging in Boston. Details of MRI and PET acquisition parameters in this cohort have been described elsewhere. 33 (11)C-labeled Pittsburgh Compound-B (11C-PiB) PET data were expressed as the distribution volume ratio (DVR) with cerebellar gray matter as reference tissue; regional time-activity curves were used to compute regional DVRs for each region of interest (ROI) using the Logan graphical method. 34 Partial volume correction was applied using the extended Muller-Gartner method. 35 11C-PiB accumulation was assessed using a large cortical ROI aggregate that included frontal, lateral temporal, and retrosplenial cortices. 36 [F18] FTP-specific binding was expressed in FreeSurfer ROIs as the standardized uptake value ratio (SUVR) to cerebellar gray matter. 37 We selected FTP binding on the bilateral entorhinal cortex, an early site of tau accumulation in ADAD. 38 Whole-brain analyses of PiB and FTP followed approaches detailed in previous work for DVR and SUVR images.39,40
Statistical analysis
Data were complete for all analyses performed with no missing values for variables of interest. No missing data handling methods were required. Group differences were assessed using two-sample t-tests and chi-square tests. Effect sizes followed Cohen's criteria. 41 Pearson correlations were used to examine associations between religious stress coping and brain pathology. Linear regressions were used to estimate the effect of religious stress coping on cognition with MMSE total score and CERAD word list delayed recall as dependent variables and religious stress coping, age, and educational attainment as independent variables. Analyses were conducted using R v. 4.3.1, modeled separately for carriers and non-carriers.
For exploratory whole-brain analyses, Pearson correlations were used to assess the relation between religious stress coping and vertex-wise tau PET within carriers. Results were displayed as –log10(p), significant at cluster-wise p < 0.05 (minimum cluster extent = 100 mm^2). Correlations and visualizations were performed in R v. 4.0.3; clustering and multiple comparisons corrections were performed using FreeSurfer tools.
Results
Group demographics, neuropsychological, and AD pathology characteristics
Participant characteristics are summarized in Table 1. PSEN-1 E280A carriers were younger than non-carrier family members (t = 3.26, df = 83, p = 0.002, d = –0.71), but both groups had similar educational attainment (t = -0.23, df = 83, p = 0.82, d = 0.05). There was a comparable ratio of males to females in both groups (χ2(1, N = 85) = 0.17, p = 0.68, φ=–0.04). Carriers had lower scores on the MMSE than non-carriers (t = 3.33, df = 83, p = 0.001, d = -0.72) but similar CERAD word list delayed recall (t = 1.93, df = 83, p = 0.06, d = –0.42). The groups had comparable GDS scores. Mutation carriers had greater amyloid-β (t = –5.51, df = 12.5, p < 0.001, d = 2.45) and greater entorhinal tau (t = –3.21, df = 14.3, p = 0.006, d = 1.57) versus non-carriers.
Participant demographic, neuropsychological, and brain pathology characteristics and Pearson correlations between religious stress coping, demographics, and brain pathology.
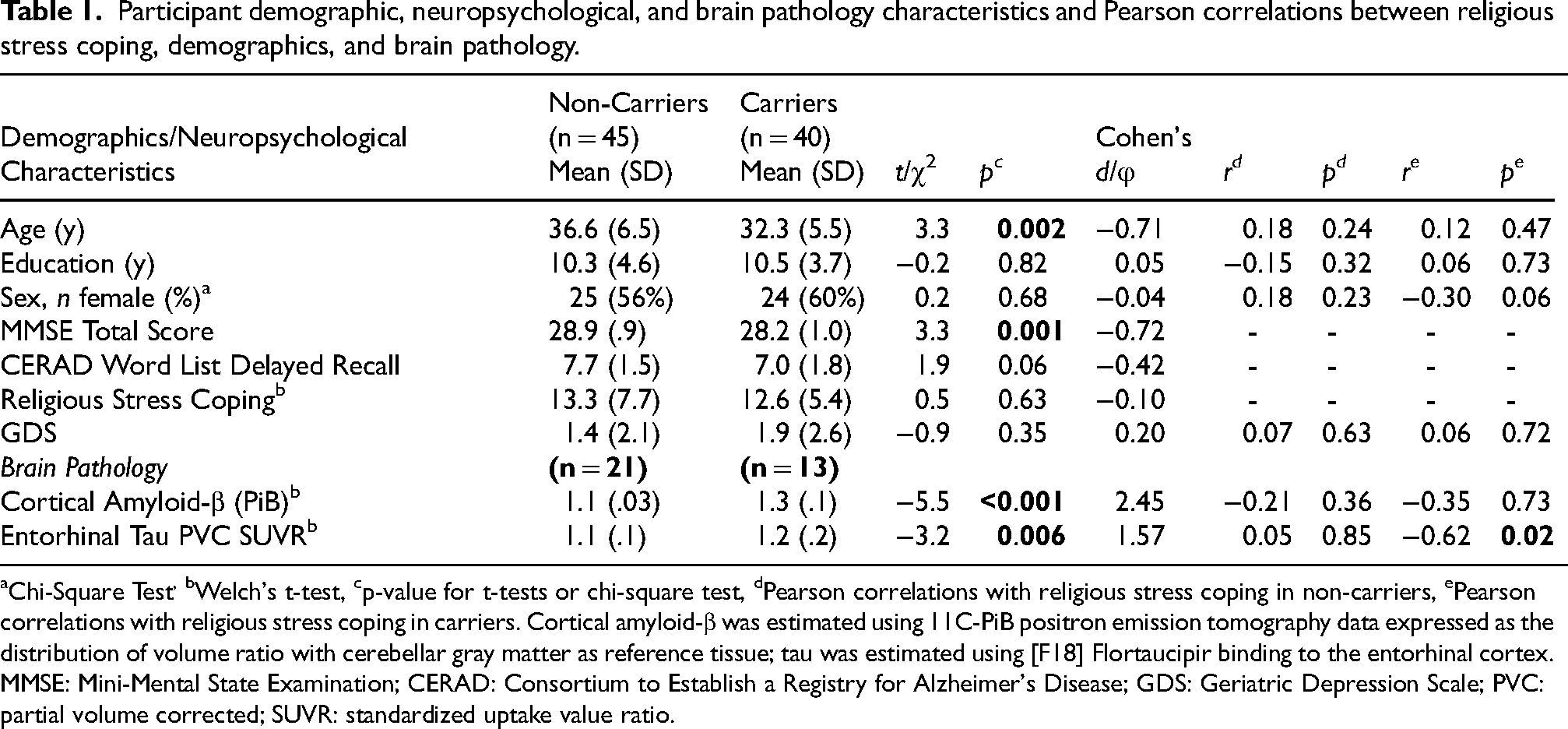
Chi-Square Test, bWelch's t-test, cp-value for t-tests or chi-square test, dPearson correlations with religious stress coping in non-carriers, ePearson correlations with religious stress coping in carriers. Cortical amyloid-β was estimated using 11C-PiB positron emission tomography data expressed as the distribution of volume ratio with cerebellar gray matter as reference tissue; tau was estimated using [F18] Flortaucipir binding to the entorhinal cortex. MMSE: Mini-Mental State Examination; CERAD: Consortium to Establish a Registry for Alzheimer's Disease; GDS: Geriatric Depression Scale; PVC: partial volume corrected; SUVR: standardized uptake value ratio.
Religious stress coping in mutation carriers and non-carriers
Carriers and non-carriers reported a similar amount of religious stress coping (see Table 1). In both groups, religious stress coping was not associated with age, educational attainment, GDS scores, nor sex.
Associations between religious stress coping and AD-related pathology
Associations between religious stress coping and AD-related pathology are summarized in Figure 1. Religious stress coping was not associated with cortical amyloid-β accumulation in carriers nor in non-carriers. Greater religious stress coping was associated with lower entorhinal tau (r = -0.62, p = 0.02) in carriers but not in non-carriers (r = 0.05, p = 0.85). In carriers, an exploratory whole-brain analysis of the association between tau binding and religious stress coping showed that greater religious stress coping was related to lower binding in the right temporal and parietal cortices (see Figure 2).
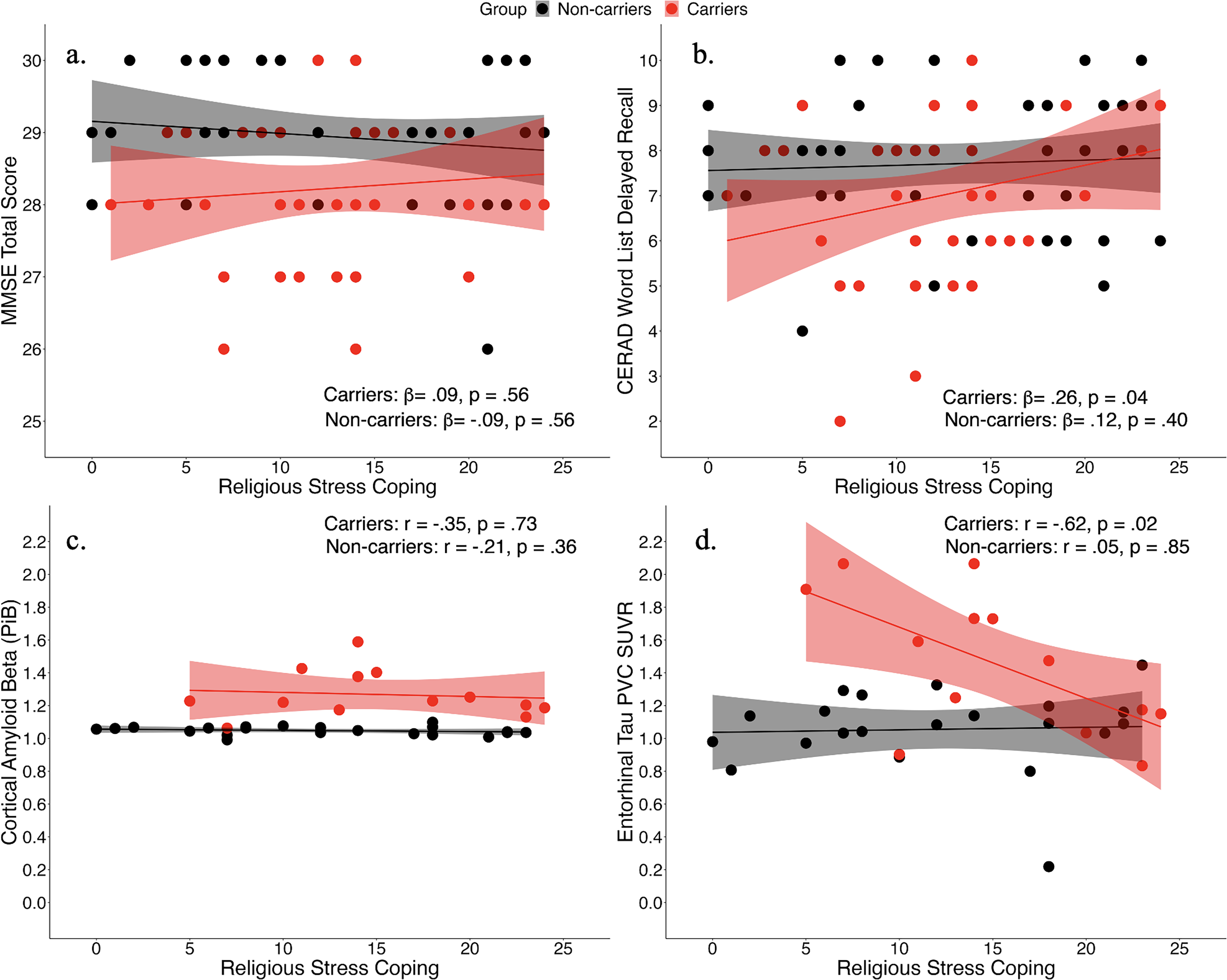
Associations between religious stress coping, cognitive performance, and Alzheimer's disease-related pathology.
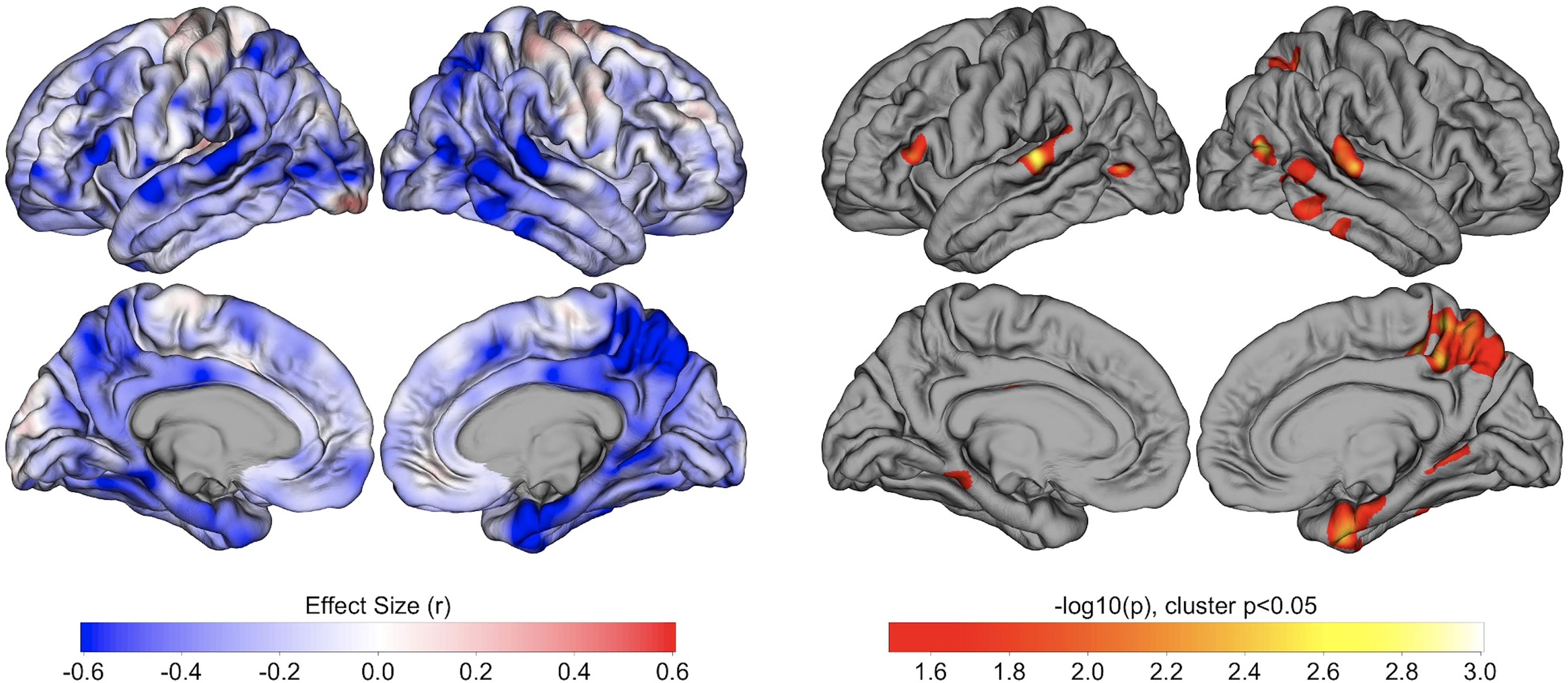
Whole-cortex analysis of tau PET versus religious stress coping.
Role of religious stress coping on global cognition and verbal episodic memory
In mutation carriers, more religious stress coping was related to better CERAD word list delayed recall (β=0.26, p = 0.04; Figure 1) but not MMSE performance after adjusting for age and educational attainment (β=0.09, p = 0.56). In non-carriers, religious stress coping was not related to MMSE performance nor CERAD word list delayed recall after age and educational attainment adjustments (see Figure 1). Regression results are detailed in Supplemental Table 1.
Discussion
Elevated stress has been linked to cognitive decline and increased risk for AD,8–12 while better stress coping and religiosity have been independently associated with reduced early AD-related brain pathology 15 and better cognitive outcomes.21–23 We investigated the impact of religious stress coping and its relation to AD biomarkers and cognition at the preclinical disease stage in cognitively unimpaired individuals with ADAD due to the PSEN-1 E280A mutation.
In PSEN-1 mutation carriers, greater religious stress coping was associated with lower tau in the entorhinal cortex, one of the earliest sites of tau accumulation,33,42–44 but not with cortical amyloid-β. This finding aligns with a previous study showing that better stress coping is related to lower entorhinal tau in cognitively unimpaired older adults. 15 The associations between tau uptake and religious stress coping were largely observed in the brain's right hemisphere, crucial for regulating the stress response and maintaining social bonds, 45 further implicating religiosity in stress management. Given the early median age of disease onset and the rate of tau accumulation in this kindred,6,25 our results suggest that better stress coping may provide some protection for those at increased risk for developing AD. Taken together with already-described genetic protective factors, 46 our results also suggest that protective factors can be multifactorial, environmental, or genetic, but longitudinal studies are needed. Future work might also explore whether religious coping interacts with amyloid on tau to further elucidate the relation of religious coping and AD pathology.
Despite similar levels of religious stress coping endorsed by mutation carriers and non-carrier family members, religious stress coping was associated with better memory performance in carriers only. This finding suggests that religious coping may be related to reduced cognitive load attributed to elevated stress47,48 and subsequently greater available resources for memory in those at increased AD risk. While our results support previous studies reporting that increased religiosity is associated with better cognitive outcomes,21–23 they differ from those that relied on measures of global cognition,21,22 which may be less sensitive to memory than domain-specific tests. When examined in this cohort, religious stress coping was not associated with global cognition. Notably, different elements of religiosity such as organizational versus non-organizational activities, social engagement, and its intersection with social identities may impact cognitive performance21,23,24,49–51 and should be explored further.
To our knowledge, this is the first study to examine the relation between religious stress coping, brain pathology, and cognitive performance in preclinical AD. Our study's strengths also include a unique sample of young and healthy adults with a well characterized clinical trajectory,6,25 and the use of PET imaging to assess AD-related pathology. Limitations include a small sample size occasioned by the fact that individuals with ADAD mutations are rare. The study's cross-sectional design prevents the deduction of a causal relation between our variables of interest and though age can be used as a proxy of disease progression in this cohort, a temporal sequence of events cannot be firmly concluded. Individuals may also underreport their religious stress coping due the low number of items on the CAE Religious Coping subscale. Though the results of the present study are consistent with studies in cognitively unimpaired older adults, 15 caution is advised in generalizing our findings to late-onset AD (LOAD). However, studying cognitively unimpaired ADAD mutation carriers with a well-characterized disease progression offers a unique opportunity to examine the preclinical AD stage, free from confounding comorbidities found in older age like cerebrovascular disease. Further, individuals with ADAD and LOAD share clinical and pathological phenotypes,6,52 making our findings relevant for LOAD.
Taken together, our findings provide support for religiosity as a potential protective factor against dementia. The present study highlights the value of considering religious coping when assessing the impact of stress on preclinical AD and developing interventions for those at increased dementia risk.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251331569 - Supplemental material for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease
Supplemental material, sj-docx-1-alz-10.1177_13872877251331569 for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease by Jairo E Martinez, Yamile Bocanegra, Ana Baena, Stephanie Langella, Averi Giudicessi, Justin S Sanchez, David Aguillon, Alice Cronin-Golomb and Yakeel T Quiroz in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-2-alz-10.1177_13872877251331569 - Supplemental material for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease
Supplemental material, sj-docx-2-alz-10.1177_13872877251331569 for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease by Jairo E Martinez, Yamile Bocanegra, Ana Baena, Stephanie Langella, Averi Giudicessi, Justin S Sanchez, David Aguillon, Alice Cronin-Golomb and Yakeel T Quiroz in Journal of Alzheimer's Disease
Supplemental Material
sj-pdf-3-alz-10.1177_13872877251331569 - Supplemental material for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease
Supplemental material, sj-pdf-3-alz-10.1177_13872877251331569 for Religious stress coping is associated with lower entorhinal tau pathology and better memory performance in autosomal dominant Alzheimer's disease by Jairo E Martinez, Yamile Bocanegra, Ana Baena, Stephanie Langella, Averi Giudicessi, Justin S Sanchez, David Aguillon, Alice Cronin-Golomb and Yakeel T Quiroz in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors thank the Colombian families with autosomal dominant Alzheimer's disease for contributing their valuable time and effort, without which this study would not have been possible. We also thank Francisco Piedrahita, Alex Navarro, and Claudia Ramos from Grupo de Neurociencias, Universidad de Antioquia in Medellin, Colombia, as well as Diana Munera, Daisy Noriega, Alex Badillo Cabrera, Crystal Castillo, Nikole Bonillas Felix, and Sofia Fabrega Ching from the Massachusetts General Hospital in Boston, MA for helping coordinate visits to Boston and assisting with data collection and processing. The authors would also like to recognize the late Dr. Francisco Lopera for his lifetime dedication to studying Alzheimer's disease and other dementias, as well as his invaluable contributions to the COLBOS Biomarker Study during his time as coordinator of the Grupo de Neurociencias, Universidad de Antioquia in Medellin, Colombia.
ORCID iDs
Ethical considerations
This study was approved by the institutional ethics review boards of Massachusetts General Hospital in Boston, Massachusetts, and the University of Antioquia in Medellin, Colombia.
Consent to participate
All participants provided written informed consent.
Author contributions
Jairo Enrique Martinez (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing); Yamile Bocanegra (Data curation; Formal analysis; Writing – review & editing); Ana Baena (Data curation; Formal analysis; Writing – review & editing); Stephanie Langella (Data curation; Formal analysis; Writing – review & editing); Averi Giudicessi (Data curation; Formal analysis; Writing – review & editing); Justin S Sanchez (Data curation; Formal analysis; Writing – review & editing); David Aguillon (Data curation; Investigation; Project administration; Writing – review & editing); Alice Cronin-Golomb (Conceptualization; Investigation; Project administration; Supervision; Writing – review & editing); Yakeel T Quiroz (Conceptualization; Data curation; Funding acquisition; Investigation; Project administration; Resources; Supervision; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Langella was supported by an Alzheimer's Association Research Fellowship. Dr. Quiroz was supported by grants from the NIA (R01 AG054671, RF1AG077627, R01AG066823), the Alzheimer's Association, and Massachusetts General Hospital ECOR. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Quiroz serves as consultant for Biogen. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Anonymized clinical, cognitive and genetic data are available upon request, subject to an internal review by D.A. and Y.T.Q. to ensure that participant confidentiality and PSEN1 E280A carrier or non-carrier status are protected, completion of a data sharing agreement, and in accordance with the University of Antioquia's and MGH's Institutional Review Board and institutional guidelines. Please submit requests for participant-related data to Y.T.Q. (yquiroz@mgh.harvard.edu).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.