
Abstract
Background
Subjective cognitive decline (SCD), where older adults perceive a persistent decline of cognitive abilities without showing an objective cognitive impairment, may represent a preclinical stage of Alzheimer's disease (AD) in some individuals.
Objective
The complex characteristics of SCD cannot only be revealed by existing self-report questionnaires. Rather, it is necessary to involve individuals affected in the research process with methods like focus group discussions (FGDs).
Methods
Study conduction took place in three steps: telephone interview, neuropsychological assessment and questionnaires, four FGDs with 16 older adults (11 female, 5 male) affected by SCD. FGDs were analyzed with qualitative content analysis using an inductive - deductive code system.
Results
Although the neuropsychological assessments did not indicate a cognitive impairment, participants reported a decline for all cognitive domains within the FGDs, especially for the memory- and speech domain, with declining word-finding abilities as the most salient symptom. Participants reported strong concerns related to SCD and difficulties in social participation.
Conclusions
SCD seems to go beyond age-related cognitive changes, but as individuals do not show an objective cognitive impairment (yet), their symptoms are often not taken seriously enough. The FGDs revealed information that questionnaires or neuropsychological tests do not capture. The gained insight into SCD symptoms, related coping strategies and concerns is important to be able to develop measures for identifying individuals at risk for a transition to AD and to develop intervention measures that aim at delaying a further decline and increasing the quality of life of individuals affected.
Keywords
Introduction
Subjective cognitive decline (SCD) is a condition where individuals, especially older adults ≥60 years, perceive a persistent decline of their cognitive abilities, without showing an objective cognitive impairment. 1 Among others, SCD is associated with negative affective symptoms and a reduced quality of life,2,3 medical factors like diabetes and hypertension and also socioeconomic factors like poverty. 4 There are studies indicating that older adults with SCD are more likely to develop mild cognitive impairment (MCI) and Alzheimer's disease (AD) in the future: e.g., Mitchell et al. (2014) found that overall the risk of developing dementia is double in older people with subjective memory complaints compared to older people without; 5 Reisberg et al. (2010) found that 90 of 166 subjects with subjective cognitive impairment (54.2%) and only seven of 47 subjects without subjective cognitive impairment (14.9%) declined to MCI or dementia (p < 0.0001) during a 7-year mean follow-up interval. 6
Thus, SCD may represent a preclinical stage of AD in some individuals. 1 The pathophysiological process that underly the disease does not start with the diagnosis itself but years before. A therapeutic intervention during this preclinical stage of AD might be relevant for changing the course of disease. 7 Therefore, it is necessary to identify individuals with SCD at risk for a transition to MCI or dementia.
The Subjective Cognitive Decline Initiative (SCD-I) Working Group developed a conceptual framework for research on SCD in preclinical AD. According to this framework, the SCD criteria contains two main aspects: (1) Self-experienced persistent decline in cognitive capacity in comparison with a previously normal status and unrelated to an acute event; (2) Normal age-, gender-, and education-adjusted performance on standardized cognitive tests, which are used to classify MCI or prodromal AD (compare page 847 of 1 ). Furthermore, SCD should not be explained by a psychiatric or neurologic disease, medical disorder, medication or substance use. 1
In research, the self-experienced persistent decline of cognitive abilities is typically measured with self-report questionnaires. Yet these SCD measurements are heterogenous and vary in many aspects such as the number of items, the cognitive domains included, the referred time period and the response options. Due to this heterogeneity it is difficult to compare research findings and transfer them into clinical practice. 8 Many questionnaires quantify SCD, 8 however the complex characteristics and how SCD manifests in everyday life, as well as what are the concerns of individuals affected and how do they cope with their SCD symptoms often remains unclear.
Since the concept of SCD is about the subjective perception of cognitive decline, it is necessary to involve those affected in the research process through patient involvement methods like focus group discussions (FGDs). Thereby it is not just a matter of letting those affected participate in the research prosses but rather a prerequisite to conduct research on the perspectives of those involved, in order to gain understanding of the subjective perception of cognitive decline. A qualitative approach, with methods like FGDs, aims at gaining a deeper understanding of the experiences, perceptions and behavior of people and investigates a phenomenon in the natural context. 9 The qualitative analysis of FGDs in order to characterize SCD helps to reveal the first-person experience and to gather information about the SCD symptoms that are particularly burdensome for individuals affected. 8 Within the scope of a FGD, a comfortable environment is created for participants to share their thoughts on a specific topic with a small group of people. The moderator of a FGD is a professional that facilitates and guides group discussions to gather insights. Based on the discussions the researchers will be able to understand the feelings, thoughts and comments of participants. 10 In the present study, FGDs were conducted with older adults affected by SCD to answer the questions: How does SCD manifests in everyday life of older adults? Which symptoms are reported? How do individuals cope with SCD? What concerns individuals with SCD? This is another step towards characterizing SCD in older adults, which is important in order to be able to identify individuals at risk for a transition to MCI and dementia in the future. Gaining an insight into SCD symptoms and related coping strategies, as well as related concerns, is necessary in order to develop targeted intervention and prevention measures that aim at delaying a further cognitive decline and increasing the quality of life of affected individuals.
Methods
Study design
This study and further projects were preregistered with ‘The Open Science Framework’ on March 30, 2023 (registration DOI (digital object identifier): https://doi.org/10.17605/OSF.IO/PZXYG). The study was performed in accordance with the ethical standards of the Declaration of Helsinki. Ethical approval was granted by the medical ethics committee of the Carl von Ossietzky University of Oldenburg. Study conduction took place from April to September 2023 at the Carl von Ossietzky University of Oldenburg. Recruiting was done through advertisement in local newspapers and flyer distribution. Individuals interested in a study participation contacted author Franziska Kiene (FK) via telephone or email. Study conduction took place in three steps: (1) short telephone interview, (2) neuropsychological assessment at the University of Oldenburg, (3) FGDs at the University of Oldenburg. Participants received an information sheet in advance and any questions were clarified. All participants provided written informed consent. Individuals who took part in all appointments received a financial reimbursement of 20 euros. Participants received the money proportionally if they just took part in the telephone interview and neuropsychological assessment (mostly due to meeting an exclusion criterion within the neuropsychological assessment and therefore not participating in the FGD). The COREQ (COnsolidated criteria for REporting Qualitative research) guideline was used to report the data. 11
Participants
Exclusion and inclusion criteria of the present study are based on the SCD criteria established by the SCD-I Working Group, presented in the introduction. 1 In this study, the Mini-Mental State Examination (MMSE) 12 was used as a standardized cognitive test to rule out that participants already show clinically relevant cognitive impairment. The MMSE is a neuropsychological screening that covers orientation, memory, attention, ability to name, following verbal and written commands, writing a sentence spontaneously and copying a complex figure. A maximum of 30 points can be reached. The MMSE differentiates between people with and without cognitive impairment, although it cannot replace a comprehensive clinical assessment to get a final diagnosis. 12 Based on newer validation studies, the Memory Clinic Basel recommends a cut-off score of 27/30 (27 = healthy). 13 Therefore, we included participants with an MMSE score of 27 or higher and excluded participants with an MMSE score of 26 or lower.
The SCD-I Working Group also gathered and presented the SCD plus features that according to current literature increase the likelihood that the subjective feeling of cognitive decline is due to preclinical AD. 14 Based on these criteria, we included individuals aged 65 years or older with the persistent feeling of cognitive decline, compared to a previous normal personal status. We asked the people if they already sought help due to their SCD, although it was not an exclusion criterion if people stated that they have not consulted a professional yet.
Furthermore, the Hospital Anxiety and Depression Scale (HADS) 15 was conducted to screen for anxiety and depression. Participants with a score of 11 or higher (indicating probable presence (‘caseness’) of the mood disorder) 16 in one of the scales were excluded from the study. The German adaptation HADS-D was used 17 and German language proficiency was also an inclusion criterion.
Assessment procedure
Assessments were conducted by author FK (M.Sc.), who is a female PhD student at the Department of Psychology at the University of Oldenburg. FK is a PhD student since December 2022 and the PhD focuses on cognition in older adults. FK holds a master's degree in psychology with a focus on neuropsychology and has worked as a neuropsychologist in several clinics and practices. She had no relationship to the participants prior to study commencement. Participants knew that FK is doing the present and other related studies in the context of her PhD.
Telephone interview
A short telephone interview was conducted, using a self-developed interview guideline: the FAL (Fragebogen zur Ausgangslage) questionnaire Part one. Potential participants were informed that they can refuse their participation at any time and that they do not have to answer the questions. To check for the presence of SCD, the following questions were asked: ‘Do you feel that your cognitive abilities (e.g., perception, attention, memory, language, learning, orientation, problem solving, planning or organization) are persistently declining, compared to a previous normal personal status? If yes: Can your self-perceived decline of cognitive abilities be attributed to an acute event (e.g., stroke, accident)?’. People for whom it could not be ruled out that SCD was possibly due to an acute event, psychiatric or neurologic disease, further medical disorder, medication or substance use, were not included. If interested persons fulfilled the inclusion criteria, they were invited to a neuropsychological assessment.
Neuropsychological assessment
All participants of the FGDs underwent the neuropsychological assessment in advance. All neuropsychological assessments were conducted at the Department of Psychology at the University of Oldenburg by author FK. At the beginning of the approximately 60 min assessment, the further course of the study was explained. Participants filled out the second part of the self-designed questionnaire FAL Part two.
The already described MMSE neuropsychological screening was carried out as part of a comprehensive test battery, the CERAD neuropsychological assessment battery (Consortium to Establish a Registry for Alzheimer's Disease).18–20 In this study, the German CERAD was used in the CERAD-Plus version, 21 which contains two additional tests and assesses verbal fluency (category animals 22 and S-words 23 ); word-finding and visual perception (Boston Naming Test short version); 24 learning of new, unrelated verbal information and verbal episodic memory (wordlist learning and wordlist recall);25,26 visuo-construction and nonverbal memory (figure drawing and figure recall); 26 psychomotor speed and executive functioning (Trail Making Test A and B). 27 The evaluation of all tests was carried out using the evaluation program of the Memory Clinic Basel. 21 The Clock Drawing Test was conducted additionally. 28 Participants completed a number of questionnaires: the EuroQol (EQ)-5D-5L Paper Self-Complete with the subtest EQ VAS, which measures the health related quality of life 29 and the already described HADS to screen for anxiety and depression. Two questionnaires to examine SCD were conducted: the Juelich Questionnaire on Subjective Cognitive Decline (JQSCD-I) 30 and the German self- and informant-report version of the Measurement of Everyday Cognition (ECog),31,32 which will be analyzed in a further study. The participants underwent only one neuropsychological assessment, which therefore represents a current snapshot of the objective cognitive performance.
Focus group discussions
Participants who did not meet any exclusion criteria were invited to an approximately 90 min FGD at the University of Oldenburg conducted by author FK. An interview guideline and accompanying Power Point Presentation (not pilot tested) that gives an explanation on the definition and rules of a FGD was used. The interview guideline was developed in advance based on extensive literature research on SCD and early stages of AD with the help of author Helmut Hildebrandt (HH). It can be provided upon request. All participants were part of just one FGD. FGDs were recorded with two different voice recorders (Philips VoiceTracer and Olympus LS-P1 Recorder). Each FGD consisted of the interviewer and three to five participants. For the first two FGDs, a student assistant was present to make field notes. Student assistants were not available during the third and fourth FGD, which is why FK made notes during these FGDs herself. All FGDs lasted 90 min with only a few minutes of variation. The number of FGDs was not determined in advance. Rather, FGDs were conducted until data saturation was reached, 33 which means that no new aspects concerning the subjectively perceived decline in cognitive domains were reported. Data saturation criteria was discussed by author FK and author Mandy Roheger (MR).
Data analysis
Audio data of the FGDs was transcribed into text documents (anonymized) and then analyzed using a qualitative content analysis 34 with MAXQDA version 2024, a software for qualitative data analysis. The findings and transcribed text documents were not returned to participants for comments, as the text documents contain statements not only from themselves, but also from other participants of the respective FGD. Codes (thematic categories) were assigned to all text passages and in several rounds of coding further divided into subcodes (thematic subcategories) by author FK. In advance, an initial deductive code system was developed based on the used interview guideline, as the interview guideline was designed to ensure that the primary research questions were discussed within the focus groups. However, the guideline was rather open and participants could always bring up other topics that came to their mind and seemed important to them. Therefore, the initial deductive code system was just the basis and was extended by inductive codes that emerged from the data/ content of the focus groups. 34 Coding of the main category declining cognitive domains and corresponding subcategories was discussed with author MR until a consensus was reached. Initially in our preregistration we planned to conduct the content analysis independently by two researchers, however, due to personnel and time constraints we decided to conduct the content analysis by one reviewer (FK) with randomized parts checked by a second reviewer (MR). The coding tree can be provided upon request. Quantitative data was analyzed with R Project for Statistical Computing version 4.3.3.
Results
Sample characteristics
The initial sample consisted of 24 participants with SCD. A telephone interview was conducted with 23 participants, as one person dropped out due to time constraints. Four people dropped out after the telephone interview: one person withdrew due to lack of time; one person was excluded due to a borreliosis, which could be associated with the reported symptoms; one person was excluded due to a previous stroke and one person due to a previous traumatic brain injury. Nineteen participants (14 female, 5 male) were invited to the neuropsychological assessment at the University of Oldenburg. After the assessment, two more people had to be excluded as their MMSE scores were below 27. The remaining participants were invited and agreed to take part in one of the FGDs. One person canceled the participation on the respective date of the FGD due to a doctors’ appointment. In total N = 16 participants took part in the FGDs (11 female, 5 male).
10 of the 16 participants reported that sometimes also other people around them have the feeling that their cognitive abilities are declining. Two of the participants could not tell if other people also have this feeling. Nine participants stated that they already sought medical help due to SCD, e.g., with their general practitioner or a neurologist. Table 1 contains a description of the sample.
Description of the sample.
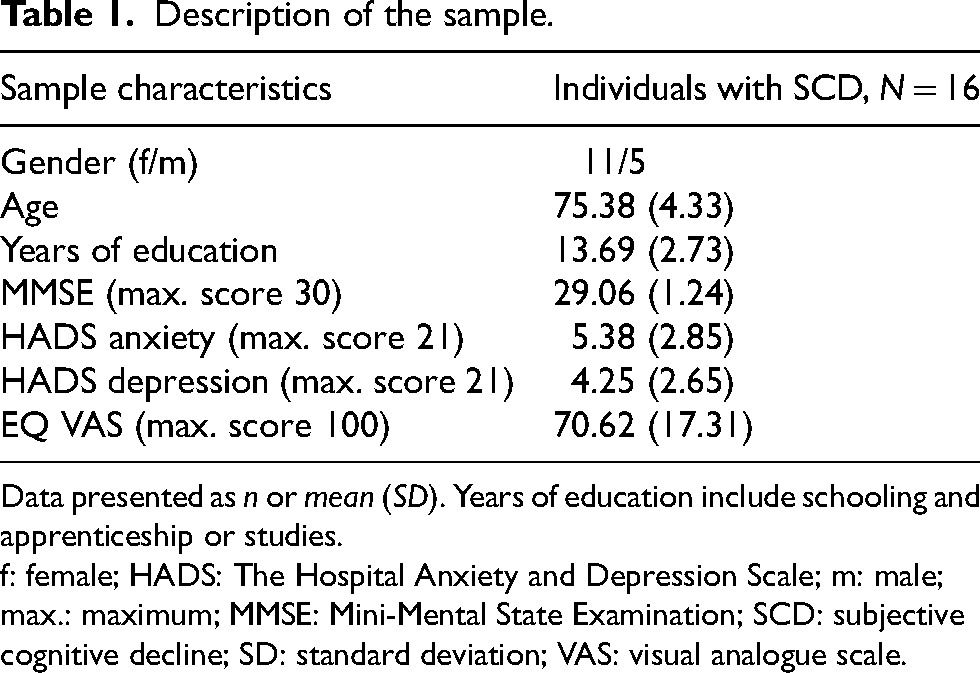
Data presented as n or mean (SD). Years of education include schooling and apprenticeship or studies.
f: female; HADS: The Hospital Anxiety and Depression Scale; m: male; max.: maximum; MMSE: Mini-Mental State Examination; SCD: subjective cognitive decline; SD: standard deviation; VAS: visual analogue scale.
Manifestation of SCD in everyday life of older adults
Neuropsychological assessment
Table 2 contains results of the subtests of the CERAD-Plus neuropsychological assessment. Age, education and sex corrected scores (z-scores) are within one standard deviation above or below the expected value. Only the mean of the TMT B z-score 1.06 (SD = 1.44) is slightly higher than one standard deviation above the expected value. The average neuropsychological test results do not indicate an objective cognitive impairment.
Neuropsychological test results.
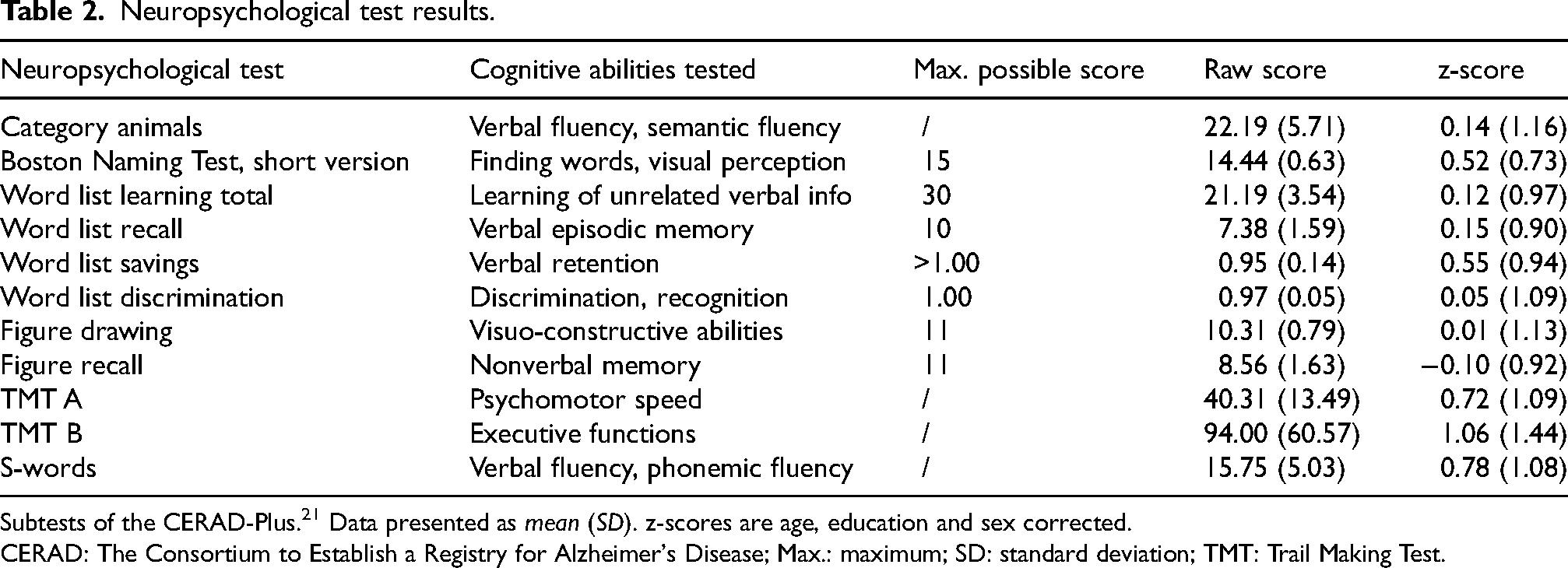
Subtests of the CERAD-Plus. 21 Data presented as mean (SD). z-scores are age, education and sex corrected.
CERAD: The Consortium to Establish a Registry for Alzheimer's Disease; Max.: maximum; SD: standard deviation; TMT: Trail Making Test.
Table 3 shows the JQSCD-I scores that assess self-reported SCD in five cognitive domains with 15 questions regarding cognitive functioning (three for each domain). 30 According to this instrument, participants are experiencing SCD mostly in the memory domain with a mean JQSCD-I score of 4.14 (SD = 1.79), followed by the motor domain with a mean JQSCD-I score of 3.94 (SD = 2.08).
Juelich questionnaire on subjective cognitive decline.
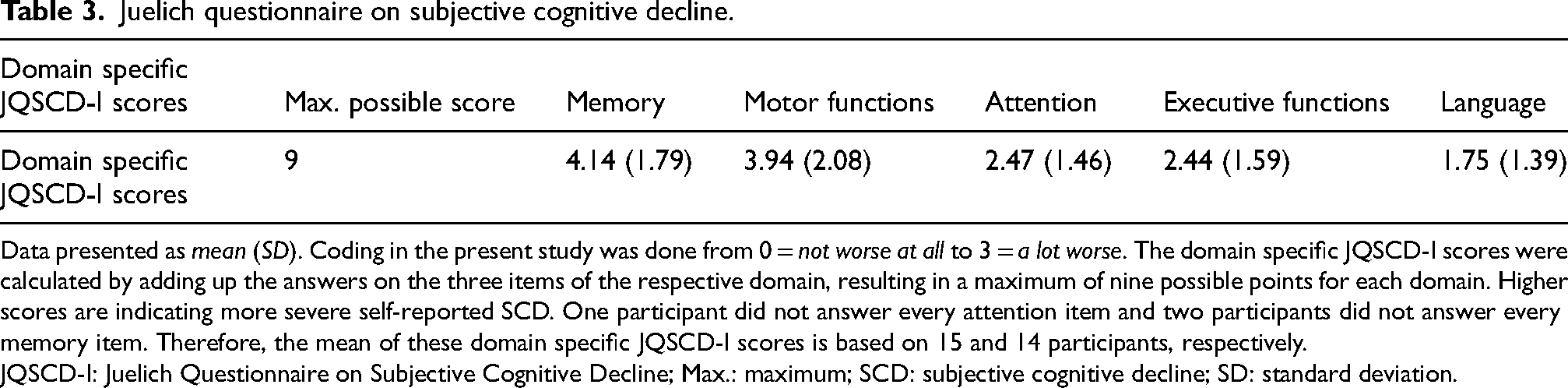
Data presented as mean (SD). Coding in the present study was done from 0 = not worse at all to 3 = a lot worse. The domain specific JQSCD-I scores were calculated by adding up the answers on the three items of the respective domain, resulting in a maximum of nine possible points for each domain. Higher scores are indicating more severe self-reported SCD. One participant did not answer every attention item and two participants did not answer every memory item. Therefore, the mean of these domain specific JQSCD-I scores is based on 15 and 14 participants, respectively.
JQSCD-I: Juelich Questionnaire on Subjective Cognitive Decline; Max.: maximum; SCD: subjective cognitive decline; SD: standard deviation.
SCD symptoms reported within the FGDs
A decline was reported for all cognitive domains within the FGDs. Text segments of the main category declining cognitive domains were further divided into subdomains. In order to get an overview of which SCD symptoms are particularly salient for the individuals affected and are frequently reported, it was counted how often a certain SCD related symptom was a subject of discussion within the FGDs. This should shed light on how SCD manifests in everyday life of older adults. Figures 1 and 2 show the amount of coded text segments over all FGDs, where participants reported a decline in cognitive domains and subdomains. Examples of translated statements from participants from different FGDs are shown below. Filler words (like ‘mh’) have been removed for better readability. The original German quotations of the presented examples can be provided upon request. Participants statements are just provided with the information in which FGD they took part, due to anonymization.
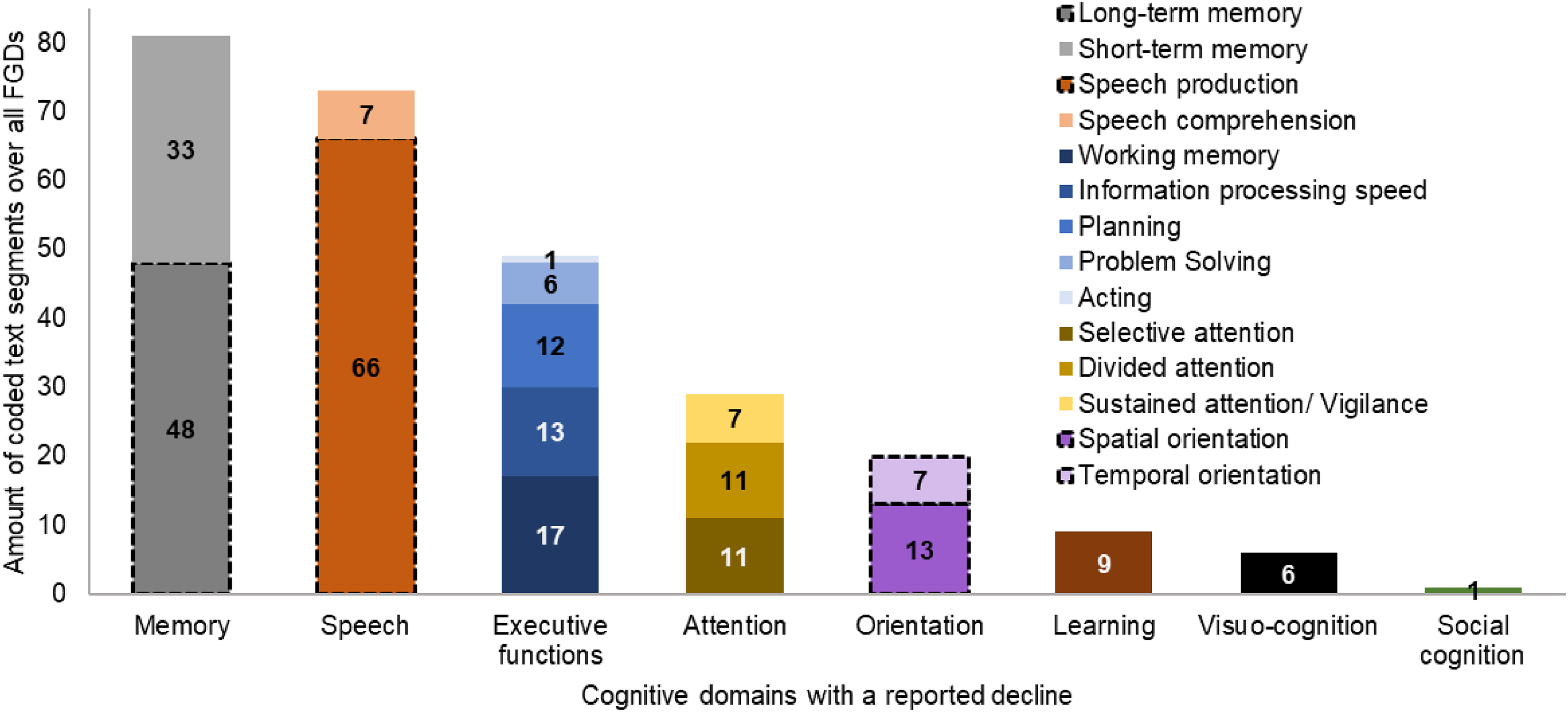
Cognitive domains with a reported decline. The x-axis contains the cognitive domains with a reported decline. Cognitive domains are further divided into subdomains. The y-axis contains the amount of coded text segments over all focus group discussions (number on bar). Cognitive domains that are typically impaired in Alzheimer's disease are framed in shaded black.
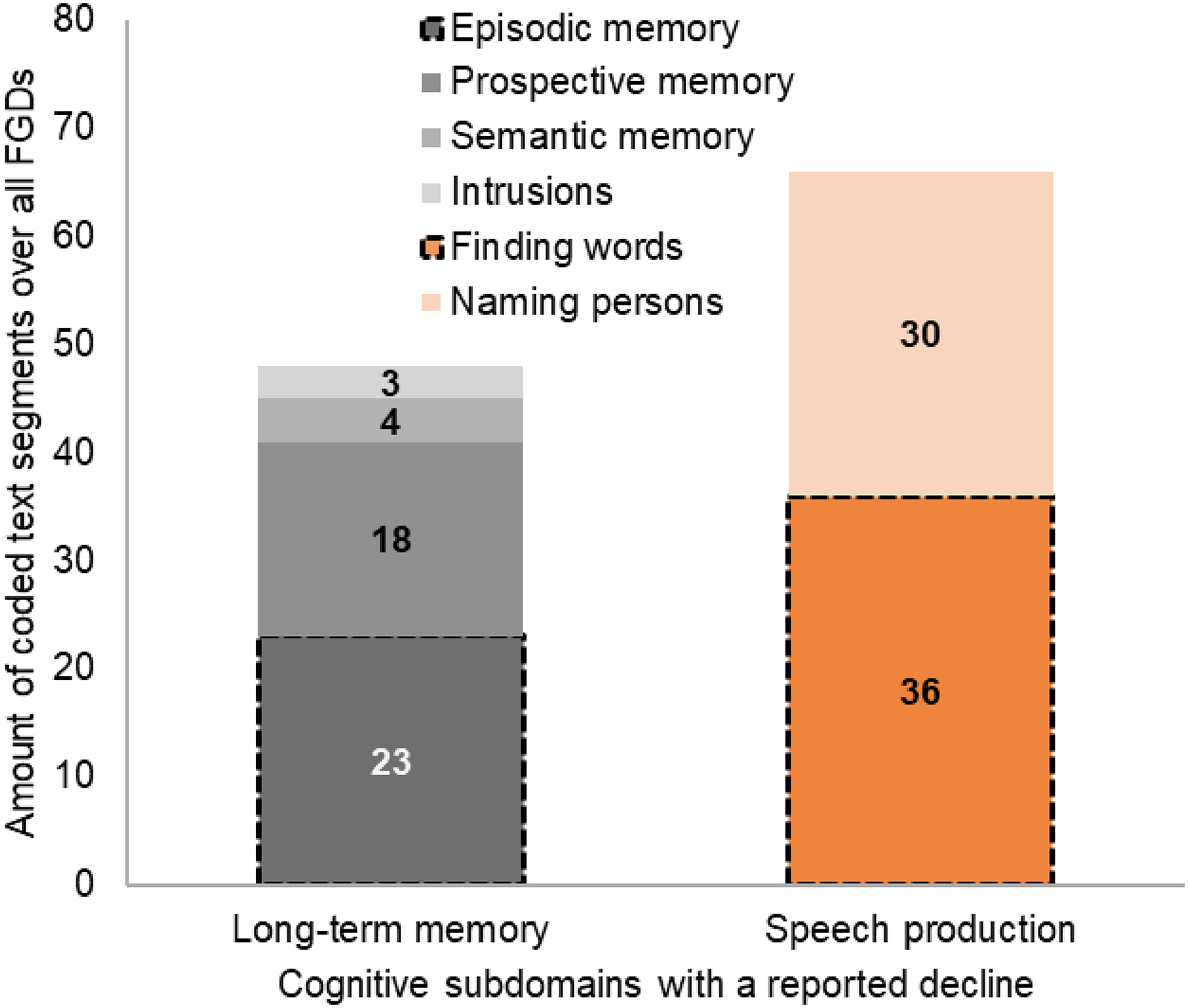
Cognitive subdomains with a reported decline. The x-axis contains the cognitive subdomains with a reported decline. The y-axis contains the amount of coded text segments over all focus group discussions (number on bar). Cognitive domains that are typically impaired in Alzheimer's disease are framed in shaded black.
Overall, a decline of the memory and speech domain was reported most frequently. Regarding the episodic memory (23 coded text segments), which is also often impaired in AD,
35
a participant described that sometimes things that happened are not stored and therefore are not available for retrieval. It's the same with me. So, the first time that my [child] did something new occupationally and I had completely forgotten about it. Also, what this job was called [shortened due to anonymization]. And I thought it's not stored. I don't have a trace of a memory [shortened due to anonymization]. (Individual with SCD, FGD 1, code: episodic memory) Yes, in the calendar, it's in the kitchen. So that's where I always come up with. In former times I didn't have to write it down. (Individual with SCD, FGD 1, codes: prospective memory, calendar) There is another problem with me, namely numbers. I am bad at memorizing numbers. When there are three that still works. But for example, when you buy something on the Internet and then getting a request concerning the numbers, this is getting so criminal. I write this down immediately as a first thing, because I cannot remember this five or four numbers at once. This is not working, this goes wrong and I write this down immediately. I can help myself with that but I think I was able to do this before […]. So, in any case especially this short-term memory, just what you have to remember for a moment in order to then type it in or something, becomes difficult. (Individual with SCD, FGD 3, code: short-term memory) Person 1: That hinders me. I like being in political discussions and then I want to say something, but then I can't remember the name. The name of the minister or the expression that matters now. Person 2: Yes, and then you block. Person 1: And then I'm standing there and that's why I don't even speak up for a discussion anymore and this is a huge hindrance. (Two individuals with SCD, FGD 4, codes: finding words, naming persons, less social participation) […] But what I observe in myself is that sometimes I'm in a conversation or in a discussion and I have a thought that I want to share and when it's my turn it is gone. (Individual with SCD, FGD 2, code: working memory) […] When I do something on the computer I can't do anything else. When my [partner] comes in and tells me something, that doesn't work, then I get confused. That wasn't the case before. (Individual with SCD, FGD 3, code: divided attention) My sense of orientation is very bad. I noticed that when I was here on [weekday], finding you here. And just now I was in front of this parking strip and then there was already [name of building], which are I guess 100 meters. (Individual with SCD, FGD 1, code: spatial orientation)
Concerns and worries related to SCD
Worries that were expressed during the FGDs are shown in Figure 3. Participants are especially worried of getting AD and a (further) cognitive decline.
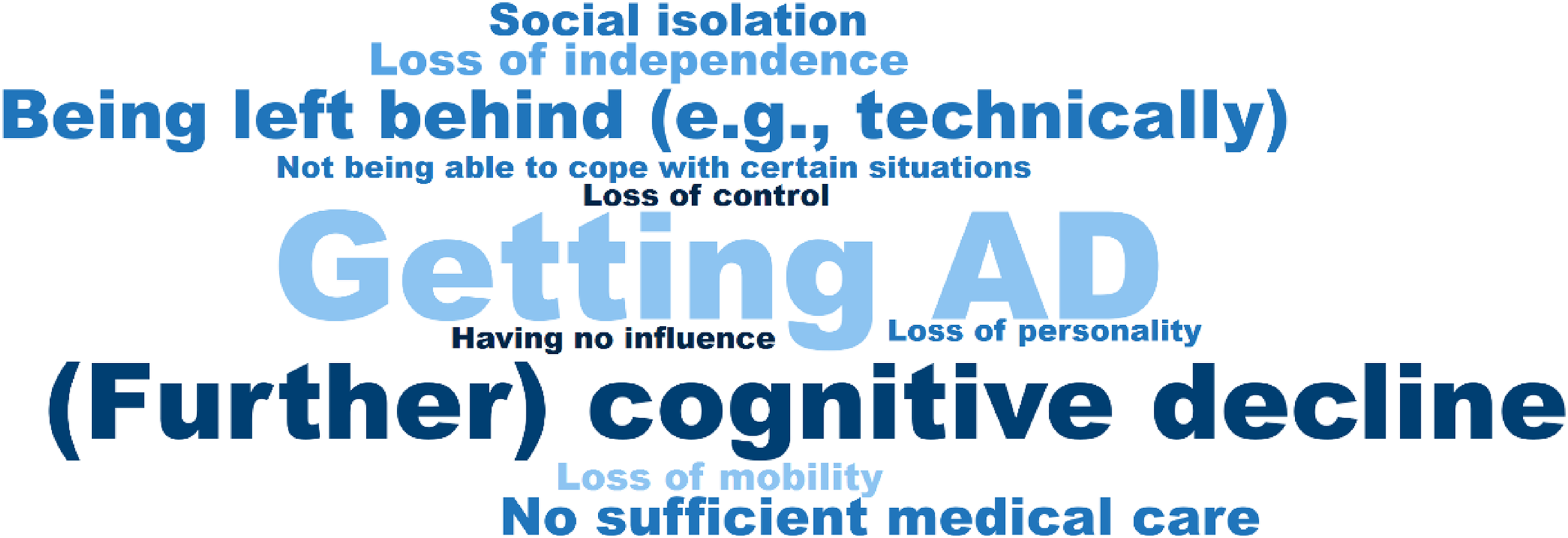
Worries of individuals with SCD. Worries that have a larger font size were discussed more frequently within the four focus groups.
SCD symptoms, like not knowing what to say in a conversation because one cannot remember the right words or names, are embarrassing for those individuals affected. This can lead to a social withdrawal and therefore to social isolation, which is also a concern of individuals with SCD. Can I go back to the first point you mentioned about this fear of stopping in a conversation and not knowing what to do next. There I am getting a very strong fear of isolation, that I withdraw because I'm afraid of such situations, that maybe others are no longer as interested because they know ‘I don't want to embarrass you like that’. This I have, yes. (Individual with SCD, FGD 2, codes: social isolation, anxious, embarrassed) […] And then I sometimes doubt myself, did I really not tell him that and so on. Everything like this, the overload. (Individual with SCD, FGD 4, codes: insecure, overwhelmed) Then I tend to be overwhelmed by such a simple thing [shortened due to anonymization] that I often do. […] (Individual with SCD, FGD 1, codes: overwhelmed) Person 1: [Shortened due to anonymization] and what scares me, I'm [age] now. That this is already starting for me. And that I think scares me. When I see how my mother was demented at the end and how I visited her […] and she didn't even know who I was anymore. Well, I think that's terrible and that's what scares me. And that's why I went to the neurologist and that's what interested me, what s*he asked there and then claimed afterwards, there's nothing wrong with her/him, what does s*he actually want here? So, I thought that it has to be different somehow, these questions. […] Person 2: This is where the big questionnaire is needed. Person 1: Exactly, something different than what the neurologists [are using]. […] (Individuals with SCD, FGD 4, codes: (further) cognitive decline, getting AD, (preliminary) examinations, new questionnaire) Person 1: With doctors, this is a topic for itself anyway these days. They don't really have time, sometimes they don't really want to, or they say what you have said: ‘what does s*he actually want here?’. Person 2: [The neurologist] didn't take me seriously at all. [The neurologist] thought: ‘what does s*he actually want here? S*he has nothing at all.’. (Two individuals with SCD, FGD 4, codes: (preliminary) examinations)
Strategies for coping with SCD symptoms
Participants reported that they often develop strategies for coping with their SCD symptoms. Figure 4 shows the ten most frequently reported strategies that were expressed during the four FGDs. Individuals with SCD use various different techniques for an active training of their cognitive abilities, e.g., cognitive exercises; crossword puzzles; riddles; quizzes; board games; card games and computer games; mental calculation; listing every country, city, river and plant that starts with a certain letter while on a walk; and purposely going shopping with leaving the shopping list at home. As another coping strategy, participants frequently write things down on a notepad/ memo in order to remember them. Furthermore, individuals with SCD reported that they try covering up/ circumvent weaknesses. For example, if they do not know the right name or word in a conversation, they smile or make a joke as a distraction that others will not notice their cognitive decline. Person 1: So, I'm still trying to cover it up […]. I think to myself, you don't have it anymore, you've forgotten. And then I smile at them and then they don't even know that I've forgotten it. Person 2: Yes, the same with names. Somehow you always get around it like that. (Two individuals with SCD, FGD 2, codes: covering up/ circumvent weaknesses, naming persons, short-term memory). One would like to prevent this with the help of some information so that the level of knowledge is a little higher. I mean that you have to do this or that in order to perhaps maintain your current level. Nothing will get better anyway, that's clear to me, we don't have to imagine this. But that you can somehow keep the level or at least that it becomes slower with forgetting and so on. Information is very important. […] (Individual with SCD, FGD 3, codes: confronting oneself with the topic SCD, (further) cognitive decline)
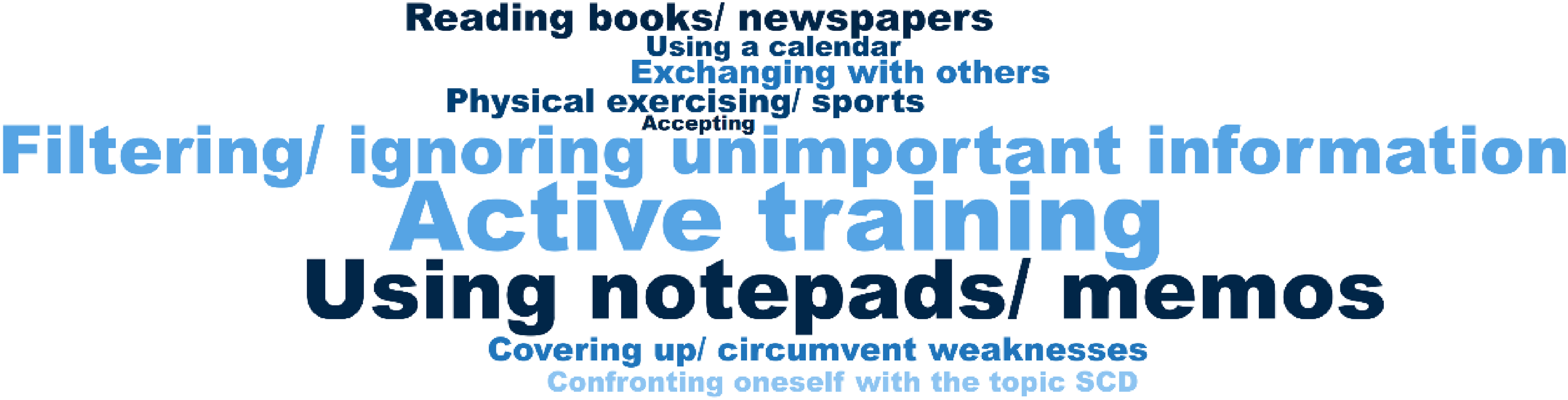
Strategies for coping with SCD symptoms. Strategies that have a larger font size were discussed more frequently within the four focus groups.
Discussion
We invited older adults with SCD to discuss their symptoms in FGDs, in order to reveal their first-person experience concerning the manifestation of SCD in everyday life. We also conducted questionnaires and neuropsychological assessments.
Individuals with SCD reported a decline in all cognitive domains within the FGDs, although the average neuropsychological test results do not indicate an objective impairment. Participants are experiencing a subtle cognitive decline from their own benchmark that the neuropsychological tests may not have captured. However, SCD describes a decline/ change of cognitive abilities, whereas neuropsychological tests measure a current state of cognitive performance. Hence, it may be more suitable to compare the change of objective cognitive performance over time with SCD reports in future studies. 30
Individuals with SCD might be more aware of age-related changes in their cognition than older adults without SCD, but most of the participants reported that other people have as well the feeling that their cognitive abilities are declining and many older adults with SCD even seek medical help. Within the FGDs it became clear that they have the feeling that their SCD symptoms go beyond the cognitive changes of healthy aging. In a review article, Sánchez-Izquierdo and Fernández-Ballesteros (2021) described that age-related changes of cognitive functions vary between individuals. Age-related decline can occur in some cognitive domains while others can remain stable or grow. 36 According to the authors, there is a continuous decline of cognitive performance after midlife on tasks involving processing speed, working memory and cognitive plasticity. 36 Processing speed and working memory were classified as executive functions within the present study. These cognitive abilities, associated with an age-related decline rather than an underlying pathology, came up as a topic within the FGDs but do not belong to the main symptoms of individuals with SCD and were not primarily discussed. SCD was rather reported for long-term memory (episodic- and prospective memory) and speech, with SCD related to name- and word-finding, which was also the most frequently discussed topic and particularly burdensome as it leads to problems in conversations and therefore to social withdrawal. Especially, problems with the episodic memory and finding words also often occur in patients with AD. 35 Nevertheless, a declining short-term memory with difficulties remembering a few numbers for a short period of time was also reported frequently during the FGDs. Buckley et al. (2015) reviewed qualitative studies concerning cognitive change in healthy older adults and those with MCI and AD. They found that older adults with MCI also reported problems with name- and word-finding and a poor contextualization of the memory. 37
According to the self-report questionnaire JQSCD-I, 30 participants are also experiencing SCD in all cognitive domains, especially in the memory domain with a mean JQSCD-I score of 4.14 (SD = 1.79). Within the FGDs, SCD was also reported primarily for the memory domain, followed by the speech domain. According to the JQSCD-I, the language domain declines the least with a mean JQSCD-I score of 1.75 (SD = 1.39). One explanation for this discrepancy could be that the JQSCD-I language domain includes the ability to understand written text. 30 During the FGDs participants reported a declining speech production, particularly a declining ability to find words and name persons, rather than a declining speech comprehension. The JQSCD-I language domain does only contain the ability of naming things but not naming persons. 30 Yet, as this is a frequent and burdensome symptom of individuals with SCD, a SCD assessment tool that captures all relevant aspects may be needed. Interestingly, according to the JQSCD-I, the motor domain was the second most affected domain with a mean score of 3.94 (SD = 2.08). Motor abilities of the JQSCD-I, like the ability to move quickly, 30 were not directly seen as cognitive abilities in the FGDs. Within the FGDs, mobility rather than motor functions was discussed. Participants reported that driving the car gets difficult due to parking issues and that riding the bicycle is not possible anymore with a certain age. The loss of mobility is a fear of some participants.
Participants developed strategies to cope with SCD symptoms in their everyday lives. Besides using notepads, active training like doing crossword puzzles and quizzes or playing mental challenging board games is a widely used strategy. Overall, active rather than passive strategies were discussed, showing that individuals want to do something themselves in order to keep their cognitive abilities at a certain level. This could imply an opportunity for possible prevention and intervention approaches: active cognitive training as early as possible might be feasible in order to delay the onset or progression of cognitive decline and enables those affected to take action themselves. Several SCD interventions are existing, yet, the effectiveness of SCD intervention approaches often still needs to be researched. 38
SCD is also often associated with negative affective symptoms and a reduced quality of life.2,3 In the present study, the mean EQ VAS score, which is an indicator for health related quality of life, 29 was 70.62 (SD = 17.31), which is somewhat lower than the mean EQ VAS score 71.59 (SD = 21.36) of a representative sample of the German general adult population (n = 4998). 39 Participants of this study are only showing a slightly reduced quality of life compared to the general adult population. We screened for anxiety and depressive symptoms with the HADS. 15 The average HADS scores were below eight points, which means ‘unremarkable’, indicating that although participants reported strong concerns related to their SCD, they are not showing clinically relevant symptoms of anxiety or depression. In future studies it could be useful to also assess personality traits of participants, as resilient personality traits like lower neuroticism and higher conscientiousness are associated with a reduced risk of a transition from SCD to a further objective cognitive impairment. 40
The evaluation of with SCD associated worries also increases the prognostic value of the SCD status for incident MCI. 41 Participants in this study were especially worried about getting AD and a (further) cognitive decline. Some participants are afraid to make mistakes, feel overwhelmed and insecure even in everyday situations. The fear of social isolation played a role in the FGDs. Participants are afraid that they cannot take part in social events anymore or that others do not want them to. These results are in line with those of Buckley et al. (2015), where the fear of participants concerning an exposure of their cognitive problems to others played an important role, as well as the fear of cognitive decline and a dementia diagnosis. 37 Less social participation was among the most salient and frequently discussed topics within the FGDs. To inform the society about SCD, MCI and AD might be helpful here. It is important that older adults with cognitive decline (subjective or objective) can continue to be a part of the society.
The main strength of this study is that it involves affected individuals in the research process, in order to reveal the complex characteristics of SCD and its manifestation in everyday life of older adults, which is important in order to be able to better identify individuals at risk for a transition to MCI or dementia in the future and develop intervention and prevention measures to delay a further cognitive decline. The FGDs revealed information that questionnaires or neuropsychological tests do not capture. This study also looked at concerns and coping strategies of individuals with SCD. This is important as one could start here to build supporting mechanisms for individuals affected and their families to reduce their burden in everyday life. The few male participants can be seen as a limitation and no AD biomarkers were assessed. The study reflects the situation in Germany and further studies have to investigate if the results are generalizable to other countries.
There are recent studies looking at sex differences in SCD that could help to explain the uneven female/male ratio in this sample. In a study of Schliep et al. (2022) 42 concerning overall and sex-specific risk factors for SCD, the representative sample of community-dwelling adults from the United States, aged 45 years or older, also consisted of more women (53.7%) than men. Nevertheless, the authors found that the prevalence of SCD was comparable between women and men (10.6% for women, 11.2% for men). Moreover, the important modifiable risk factors for SCD were the same for both: social isolation, depression, hypertension. 42 As these factors are modifiable, it highlights the importance of prevention and intervention measures for older adults in general. However, in another study it was found that females with SCD decline significantly faster than males with SCD in all cognitive domains, indicating that the presence of SCD may be a better predictor for future objective cognitive decline in females than in males. 43 Also, in another study with participants from the Hamburg City Health Study in Germany, participants with SCD (n = 3708) were more frequently female (54.2%). 44 One explanation why more women were interested in taking part in the FGDs may be that they are experiencing a faster cognitive decline from their personal baseline and therefore are especially worried about getting AD and a (further) cognitive decline. Also, more women have AD than men (2020 Alzheimer's disease facts and figures). 45 Nevertheless, the results from Schliep et al. (2022) 42 show that prevention and intervention measures to modify SCD risk factors should be targeted to both, women and men.
In summary, SCD in older adults is associated with impairments in their everyday lives, strong concerns and difficulties in social participation. Individuals with SCD have the feeling that doctors do not take their symptoms seriously enough, as they often do not show an objective cognitive impairment (yet). Hence, it is important to apply SCD assessments in clinical practice, in addition to the assessment of objective cognitive performance.
To the knowledge of the authors, there are no other studies with FGDs about SCD symptoms and related concerns of older adults. However, the present results are in line with findings from another qualitative study, investigating patients of memory clinics in the Netherlands, with and without a cognitive impairment. Gruters et al. (2021) 46 conducted four FGDs with 14 patients and their family about experiences concerning the neuropsychological assessment. Data was also analyzed with inductive and deductive content analysis. The authors identified three themes: ‘uncertainty’ (before, during and sometimes even after the diagnostic disclosure), ‘early diagnostic paradox’ (negative emotions, e.g., distress due to awareness of cognitive impairment; and positive emotions, e.g., relief after a diagnosis) and ‘knowledge utilization’ (inaccurate communication, problem of understanding and remembering information from the diagnostic disclosure). 46 The importance of an explanatory conversation with a health professional, in which patients are taken seriously and the high need for information concerning SCD and cognition also became clear in the FGDs of the present study. This seems to be necessary in order to reduce uncertainty and negative emotions, 46 which are also reported by participants from the present sample.
Results of this study will be used to develop a SCD assessment tool that captures all relevant aspects discussed in the FGDs. Further, an ambulatory assessment for smartphones that can be used in longitudinal studies to investigate SCD symptoms over time may be more advantageous than a single time point questionnaire, as the self-perceived cognitive decline can be measured without a retrospective bias and relations between cognition and other variables (e.g., stress) can be investigated. 47 Moreover, the evaluation of SCD consistency increases the prognostic value of SCD for future objective cognitive decline. 41 An ambulatory SCD assessment may provide an approach for an objective measurement of a subjective feeling, which can be applied in clinical practice. Of course, not all individuals with SCD will develop AD but some are at a higher risk. A comprehensive ambulatory SCD assessment allows to investigate the experienced symptoms in more detail and therefore may help to differentiate between individuals at risk for a transition to MCI and dementia and those experiencing mere age-related cognitive changes. This is important in order to be able to further examine older adults with a suspected underlying AD pathology and intervene as early as possible, and on the other hand to support individuals who are dealing with excessive worries due to mere age-related cognitive changes (e.g., with providing information on cognitive aging).
Footnotes
Acknowledgments
The authors acknowledge all the participants, who take part in the studies of our working group.
Ethical considerations
The study was performed in accordance with the ethical standards of the Declaration of Helsinki. Ethical approval was granted by the medical ethics committee of the Carl von Ossietzky University of Oldenburg.
Consent to participate
All participants provided written informed consent.
Author contributions
Franziska Kiene, Master of Science (Conceptualization; Formal analysis; Investigation; Methodology; Software; Visualization; Writing – original draft); Helmut Hildebrandt (Conceptualization; Investigation; Methodology; Validation; Writing – review & editing); Mandy Roheger (Conceptualization; Methodology; Project administration; Resources; Supervision; Validation; Writing – review & editing)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The FGD interview guideline, the coding tree of the qualitative content analysis and the original participants quotations of this article are available on request from the corresponding author.