
Abstract
Background
Detecting life disability is crucial in diagnosing dementia; however, early detection has proven challenging with previous assessment scales. This study focused on an individual's ability to use household appliances as a means of detecting life disability.
Objective
The objectives of this study are threefold: (1) to compare the ability to use household appliances between the non-dementia and dementia groups, (2) to determine whether the level of life disability based on the ability to use appliances is at the level of diagnosed dementia or non-dementia, and (3) to explore the impact of age and gender on the ability to use appliances.
Methods
We selected 13 essential household appliances for elderly individuals and proposed an instrumental activities of daily living (IADL) assessment tool to evaluate their usage. Our sample consisted of 98 patients with cognitive impairment, divided into a non-dementia group (N = 34) and a dementia group (N = 64). Most participants in the dementia group had Alzheimer's disease or related conditions. Through multiple logistic regression, the model equation aimed to determine whether a subject's functional disability indicated a potential dementia diagnosis.
Results
The optimal model equation identified the microwave oven and air conditioner as key factors, achieving an area under the curve (AUC) of 0.78. Additionally, analysis by age and gender enhanced the discriminative power of the results.
Conclusions
Our proposed scoring system can efficiently determine the degree of life disability by assessing appliance usage, demonstrating comparable discriminatory ability to existing scales.
Keywords
Introduction
The clinical phase of mild cognitive impairment (MCI) represents an intermediate state between normal aging and early dementia. MCI can be defined as a condition where pathological changes have already progressed, resulting in objective memory impairment beyond what is expected for a certain age while maintaining activities of daily living.1–3 As the disease progresses, cognitive disorders lead to impairments in everyday functioning, with dementia being diagnosed when individuals demonstrate substantial impairment in cognitive performance that directly impacts their independence in daily activities. Unlike dementia, MCI is characterized by the absence of impairment in activities of daily living (ADL). 4 However, recent reports have shown that individuals with MCI may experience difficulties in daily living, especially in instrumental ADL (IADL).4–6
IADL refer to a set of complex daily activities performed by the elderly, including meal preparation, household chores, shopping, and financial management,7–9 that are more susceptible to the effects of early cognitive decline compared to basic ADL (BADL), such as eating, dressing, walking, bathing, using the toilet, and personal hygiene. 8
Given that MCI is characterized by minimal impairments in IADL, evaluating these activities is critical for distinguishing between dementia and MCI. Additionally, assessing IADL remains essential even after a dementia diagnosis, as these impairments significantly influence the daily lives of both patients and caregivers and are, thus, essential for planning care needs, legal matters, and financial decisions. 8 In summary, the assessment of IADL is important for both diagnostic purposes and follow-up care management.
The Lawton IADL scale, developed in 1969, 7 remains a widely used tool by clinicians and researchers. This informant-based questionnaire provides valuable insights into the functional skills necessary for individuals to live independently within their community. 10 The scale comprises eight items: telephoning, shopping, food preparation, housekeeping, laundering, use of transportation, use of medicine, and financial behavior. 8 The IADL items form an eight-point scale for females and a five-point scale for males, as certain tasks in the scale, such as food preparation, housekeeping, and laundering, are deemed exclusive to females. However, there is a growing consensus among experts such as Fessler et al. that the IADL scale requires updating to accurately reflect modern-day functional abilities to continue being used as a valid tool in clinical and research practice. 11 The increased reliance on electrical devices today has altered the skills needed to perform daily activities compared to when the Lawton IADL scale was first introduced. Therefore, the scale must be revised to align with current functional expectations.
While several dementia detection scales focus on an individual's ability to use electronic devices, such as the AD8, there are limitations to consider. For instance, one of the eight items in the AD8 is the following yes/no question about daily activities: “Having difficulty learning how to use tools, appliances, and gadgets (e.g., VCR, computer, microwave oven, remote control)”.12,13 However, we believe that this scale is insufficient because (a) the questionnaire evaluates the use of electronic devices altogether rather than asking about the ability to use each item and (b) it rates the patients’ abilities on only two levels, which is not considered accurate for individuals with MCI or mild dementia.
Furthermore, the Alzheimer's Disease Cooperative Study/Activities of Daily Living scale for MCI patients (ADCS/MCI/ADL) is a functional evaluation scale designed for MCI patients due to Alzheimer's disease (AD). This scale has been used in numerous studies and clinical trials to monitor the evolution of patients with MCI. 14 One notable feature of this scale is its inclusion of an item related to household appliances based on information provided by an informant/carer. Within this scale, informants are asked to choose from the following four choices regarding the patient's abilities to operate one or two commonly used appliances: (a) without help, and operated all necessary controls; (b) without help, but operated only on/off controls; (c) with supervision (e.g., instructions), but no physical help; and (d) with physical help. 15 While this questionnaire offers a more detailed assessment of appliance use, it is not sufficient to assess the use of each appliance individually, as informants are only asked to choose one or two most frequently used appliances. In modern society, many daily activities, both at home and in the community, involve the skilled management of everyday technology (ET), such as household appliances and information and communication technologies. However, due to its complexity and changeability, ET has been shown to present greater challenges for people with MCI and dementia compared to older adults without these disorders. 11 Consequently, there has been a growing emphasis on evaluating the ability to use ET devices such as remote controllers, microwave ovens, and cell phones when assessing IADL. 11
Recently, two major questionnaires/scales were developed that focused on the use of ET. One of these, the Everyday Technology Use Questionnaire (ETUQ), was designed to investigate the ability of individuals with cognitive limitations to utilize ET effectively. 16 The ETUQ consists of 86 items, including activities not commonly performed in daily life by the majority of elderly individuals, particularly those aged 70–80 years old, such as internet banking, automated airport check-in, and sewing machines. This comprehensive questionnaire covers a wide range of ET. Previous studies utilizing the ETUQ revealed that both older adults with MCI and mild-stage AD perceive themselves as less capable of using ET, actually using fewer ETs compared to older adults without known cognitive impairments.17–19 The second questionnaire, the Amsterdam IADL Questionnaire, is an informant-based computerized questionnaire aimed at detecting the early stages of dementia. 20 It has been proven to be a reliable and valid instrument in the evaluation of dementia.21,22 This questionnaire, which is administered using a web survey-based internet tool, consists of 70 items, including some items unfamiliar to elderly individuals, such as driving, managing finances, and using computers and smartphones. While these two scales provide a comprehensive assessment with 70–80 questions, they can be time-consuming to administer and may not be easy to use in a busy dementia outpatient setting.
Nygard et al. pointed out that the use of ET in IADL may be more sensitive to cognitive impairment than other activities, making it a crucial aspect of social function that warrants further in-depth investigation. 19 Therefore, we hypothesized that by focusing on essential ETs for the elderly, we could accurately evaluate their daily living abilities.
Although many activities involve the management of ET, we limited our survey to appliances considered essential for use by most elderly people in their daily lives. The primary objectives of this study are to (1) compare the ability of elderly individuals with and without dementia to use household appliances, (2) determine whether the level of life disability based on the ability to use appliances is at the level of diagnosed dementia or non-dementia, and (3) explore the impact of age and gender on the ability to use household appliances.
The IADL survey in this study, which focuses on the use of home appliances that are a necessity in the lives of the elderly, may contribute to the diagnosis of dementia by detecting lifestyle disabilities through a simple and unified scale.
Methods
Subjects
The study included outpatient participants who sought treatment at the Memory Clinic with their caregivers at Kyoto University Hospital between April 2022 and June 2023 or the Center of Neurological and Cerebrovascular Diseases, Koseikai Takeda Hospital, between January and March 2023. The sample consisted of 98 community-dwelling patients experiencing subjective or objective cognitive impairment.
Patients diagnosed with dementia or MCI were evaluated by board-certified neurologists specializing in AD and related disorders. The diagnoses were based on the National Institute on Aging-Alzheimer's Association (NIAAA) workgroup diagnostic criteria/Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria, and Petersen's criteria. Various cognitive tests, such as the Mini Mental State Examination (MMSE), Alzheimer's Disease Assessment Scale (ADAS), Trail Making Test (TMT), and Clock Drawing Test (CDT), were used as reference findings, along with the logical memory subtest of the Wechsler Memory Scale (WMS) to detect detailed memory impairment. Subjective cognitive decline (SCD) was defined as a self-reported decline in cognitive functions, especially memory, without formal deficits on neuropsychological testing. Patients with amnestic MCI were selected as it is considered an earlier stage of AD.
In this study, the participants were divided into two groups based on their medical diagnosis: the non-dementia group (SCD–MCI) and the dementia group.
The exclusion criteria included the following: (1) patients with severe ADL impairment requiring constant care in their daily activities and (2) patients without caregivers knowledgeable about their daily activities.
Procedure
To evaluate the patients’ abilities in using household appliances, we created a new assessment tool named Kyoto-IADL, an informant-based digital questionnaire that can be completed on a tablet. The operational interface of the questionnaire is presented in Supplemental Figure 1. Family caregivers familiar with the patients’ daily routines were tasked with entering information into the Kyoto-IADL at an outpatient memory clinic.
The Kyoto-IADL questionnaire comprises queries regarding the participants’ ability to operate 13 household appliances, including a landline telephone, mobile phone, microwave oven, gas stove / induction cooktop, rice cooker, air conditioner, heating equipment, electric fan, electric light, washing machine, vacuum cleaner, television, and automatic water heater for a bathtub. We selected appliances considered truly essential for the daily lives of elderly individuals. Notably, the Kyoto-IADL excludes items that have been investigated in previous studies, such as automated airport check-in, sewing machines, irons, and computers.
The Kyoto-IADL questionnaire is structured to include three types of questions for each of the 13 appliances: (a) whether the patient owns the appliance, (b) whether the patient uses the appliance himself/herself, and (c) to what extent the patient can use the appliance. If the patient answers “yes” to question (b), they are prompted to indicate their level of usage in question (c).
The ability to use each item is rated on a four-point scale ranging from 0 to 3, where 3 indicates that the patient can use the appliances appropriately by himself/herself and a score of 2 denotes that the patient can use the device on their own only for some simple operations. Moreover, a score of 1 denotes that the patient uses the device with help or under the supervision of a caregiver, and a score of 0 indicates that the patient cannot use the device at all. Thus, the total score for the Kyoto-IADL ranges from a minimum of 0 points to a maximum of 39 points. In question (b), if the respondent (usually a caregiver) indicates that the patient does not use the appliance, they are prompted to specify whether the patient cannot use the appliance because they do not know how to use it, do not try to use it by themselves, or if it is simply not a habit for them.
The questions and response options for each appliance were developed according to the aforementioned criteria and can be found in Supplemental Table 1. During the administration of the Kyoto-IADL, a study investigator was present to assist as needed. The completion of the questionnaire required 5–10 min.
In addition to the Kyoto-IADL assessment, basic patient information such as age, gender, diagnosis, and MMSE scores were obtained from the medical records.
Statistical analyses
We conducted statistical analyses to compare factors such as age and gender between the non-dementia and dementia groups using Wilcoxon's rank sum test and Pearson's chi-squared test, respectively. Additionally, Wilcoxon's rank sum test was employed to compare the Kyoto-IADL scores (i.e., the total score and the score for each appliance) between the groups.
A logistic regression analysis was performed using the scores of each household appliance as predictor variables to determine whether the subject's life disability was at a level that warranted diagnosis as dementia.
The receiver operating characteristic (ROC) analysis was then employed to identify optimal cutoff points for each household appliance, with subsequent calculations of their sensitivities, specificities, and positive and negative predictive values. The Youden index was used to determine the optimal cutoff point. The diagnostic accuracy of each electric device was calculated using the area under the curve (AUC).
As reasons for deviations in the survey of usage capability, responses such as “do not own this item” or “not in the habit of using this item” could be collected. However, if these responses were treated as missing, the cases would be excluded from the analysis population. To avoid overestimation, these responses were assigned a score of 0. Multiple logistic regression analysis was then performed on all 98 cases.
Subsequently, multiple logistic regression analysis was conducted to identify predictors of more accurate discriminant ability, using the Kyoto-IADL total score (i.e., the total score for all appliances) and the combination of multiple scores for each appliance as predictor variables. A stepwise method based on the Akaike Information Criteria (AIC) was employed to select factors for inclusion in the optimal model equation.
Moreover, the variance inflation factor (VIF) value was computed to confirm the absence of collinearity in the final equation. The general rule of thumb states that a VIF exceeding 4 warrants further investigation, while a VIF exceeding 10 indicates serious multicollinearity that requires correction.
To evaluate the internal validity of the AUC, resampling using the bootstrap method was performed. A total of 1000 resamples were drawn from the dataset to estimate the bootstrap AUC and the bootstrap 95% confidence intervals. The analysis was conducted using the “boot” and “pROC” packages in R software.
Statistical analyses were performed using JMP Pro (version 17.0.0, SAS Institute Inc., Cary NC USA) and R statistical package (version 4.4.1, R Foundation for Statistical Computing, Vienna, Austria). Two-sided P values of less than 0.05 were deemed statistically significant.
Ethical approval
The study protocol was approved by the Ethics Committee of Kyoto University Hospital (R1243) and the Center of Neurological and Cerebrovascular Diseases, Koseikai Takeda Hospital (R3258).
Oral and written informed consent was obtained from participants and their caregivers, with the understanding that they were free to withdraw from the study at any time.
Results
Participants’ demographic characteristics
In total, 98 patients with cognitive impairment, with the median age being 82 years (IQR: 78–85), participated in this study. The characteristics of the subjects are shown in Table 1. The non-dementia (SCD–MCI) group consisted of 34 subjects (34.7%), while the dementia group included 64 subjects (65.3%). They comprised four cases of subjective cognitive decline (SCD), 30 cases of MCI (presumably due to AD), 53 cases of AD, two cases of dementia with Lewy bodies (DLB), and nine patients with mixed dementia (AD plus cerebral small vessel disease).
Demographic characteristics of the participants.
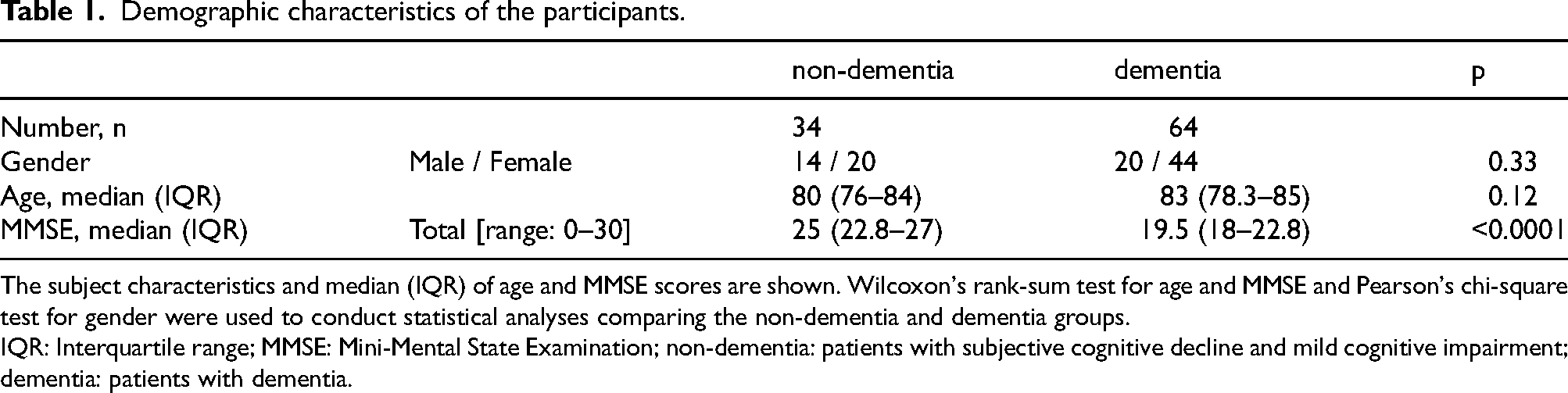
The subject characteristics and median (IQR) of age and MMSE scores are shown. Wilcoxon's rank-sum test for age and MMSE and Pearson's chi-square test for gender were used to conduct statistical analyses comparing the non-dementia and dementia groups.
IQR: Interquartile range; MMSE: Mini-Mental State Examination; non-dementia: patients with subjective cognitive decline and mild cognitive impairment; dementia: patients with dementia.
The mean age did not reveal any significant differences between the non-dementia and dementia groups (Z = –1.57, p = 0.12). Additionally, there were no significant variations in gender distribution between the two groups (χ2 = 0.97, p = 0.33). The study population comprised 34 males (34.7%) and 64 females (65.3%). The male had a median age of 82.5 years (IQR: 78.8–84.3) and a mean MMSE score of 22.3 (SD = 5.1), with 14 non-dementia and 20 dementia cases. On the other hand, female had a median age of 81.5 years (IQR: 78–85) and a mean MMSE score of 20.7 (SD = 4.6), with 20 non-dementia and 44 dementia cases.
Ability to use each household appliance
Regarding questions (a) (“whether the patient owns the appliance”) and (b) (“Does the subject use the appliance?”), the percentages of respondents indicating “not owning this item” and having “no habit of using this item” are presented in Table 2. Moreover, the responses “not owning this item” and “no habit of using this item” are considered missing values in the usability survey. The sum of the percentages of these two responses is presented as the missing data rate in Table 2.
Missing data rate and the score of Kyoto-IADL in non-dementia and dementia groups.
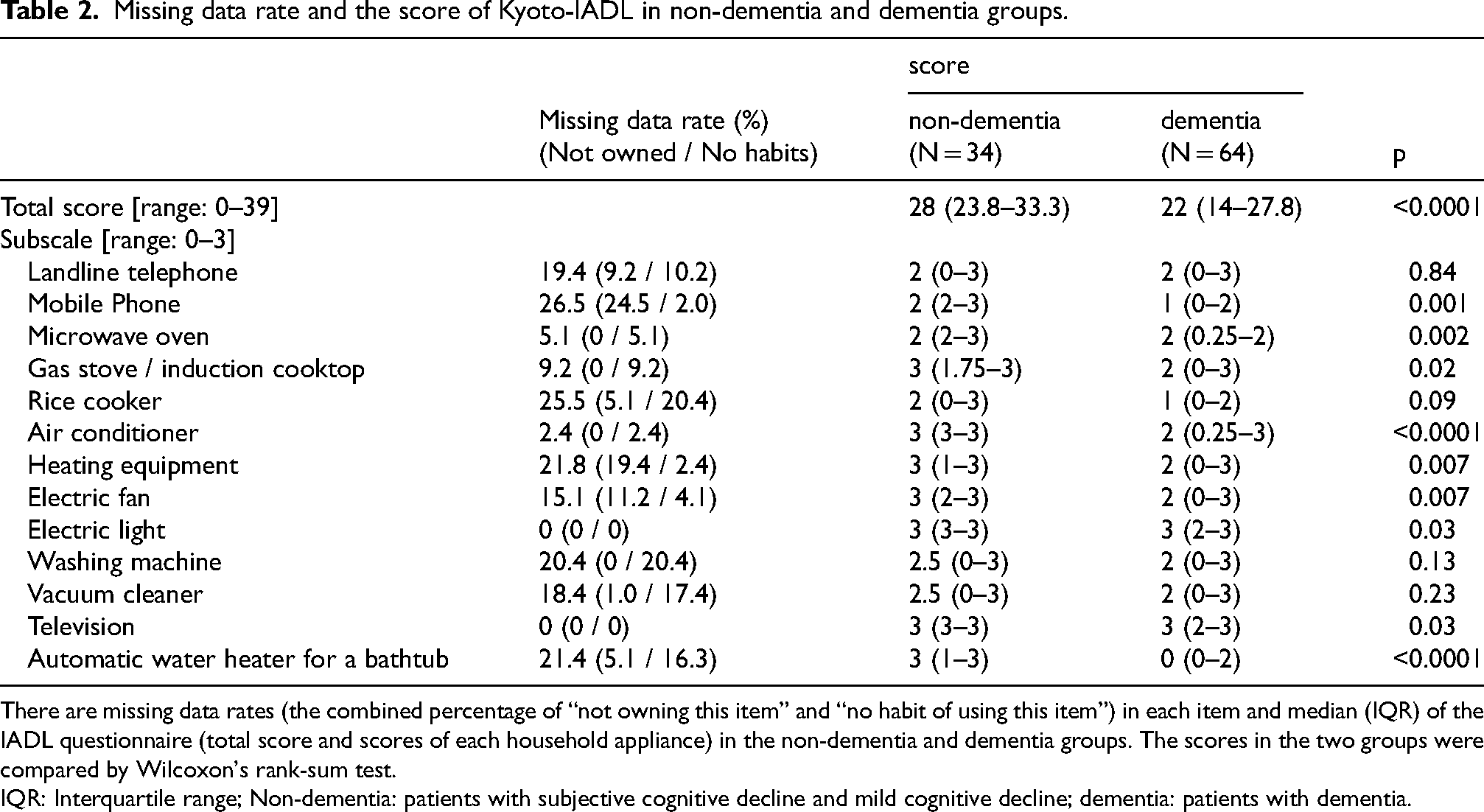
There are missing data rates (the combined percentage of “not owning this item” and “no habit of using this item”) in each item and median (IQR) of the IADL questionnaire (total score and scores of each household appliance) in the non-dementia and dementia groups. The scores in the two groups were compared by Wilcoxon's rank-sum test.
IQR: Interquartile range; Non-dementia: patients with subjective cognitive decline and mild cognitive decline; dementia: patients with dementia.
Further, Table 3 exhibits the missing data rate (i.e., the sum of the rates of “not owning this item” and “no habit of using this item”) for the respective appliances, categorized by gender and age (under/over 82 years, which is the median age of this study).
Percentage of not owning each item and no habit of using each item in the group of males/females and those under 82 years and those over 82 years.
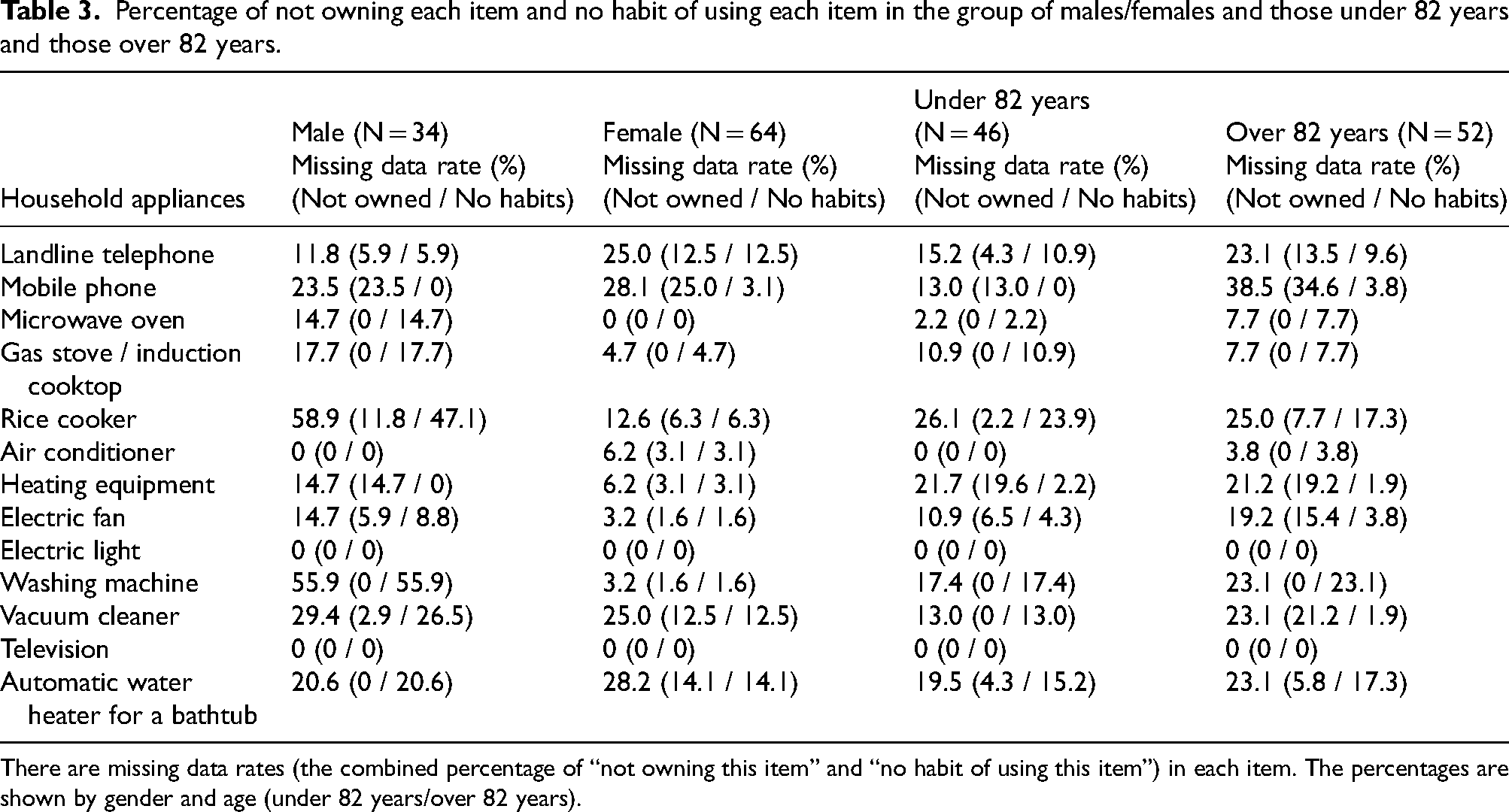
There are missing data rates (the combined percentage of “not owning this item” and “no habit of using this item”) in each item. The percentages are shown by gender and age (under 82 years/over 82 years).
The percentage of Kyoto-IADL responses in both the non-dementia and dementia groups is depicted in Figure 1. The Kyoto-IADL questionnaire required family caregivers to rate the subject's use of home appliances on a four-point scale. Additionally, the percentages of subjects “not owning this item” and “no habit of using this item” are also shown in Figure 1. In Figure 1A, the percentage of responses in the non-dementia group is displayed. The sum of the percentages of responses for 3 points (can be used appropriately by oneself) and 2 points (can use only some functions by oneself) exceeded 50% for all items. Notably, the sum of the percentages of “not owning this item” and “no habit of using this item” was high for the following three appliances: landline telephone (29%), rice cooker (27%), and washing machine (21%). Conversely, the percentage of 0 points was significantly higher in the dementia group, as shown in Figure 1B, compared to the non-dementia group. Specifically, the percentage of 0 points was particularly high for the gas stove/induction cooktop (23%), rice cooker (23%), air conditioner (22%), washing machine (23%), and automatic water heater for a bathtub (22%). However, even among the dementia group, electric light (66%) and television (63%) received high scores of 3 points. The sum of the percentages of “not owning this item” and “no habit of using this item” was high for the mobile phone (34%), automatic water heater for a bathtub (31%), rice cooker (25%), heating equipment (25%), vacuum cleaner (25%), electric fan (20%), and washing machine (20%).
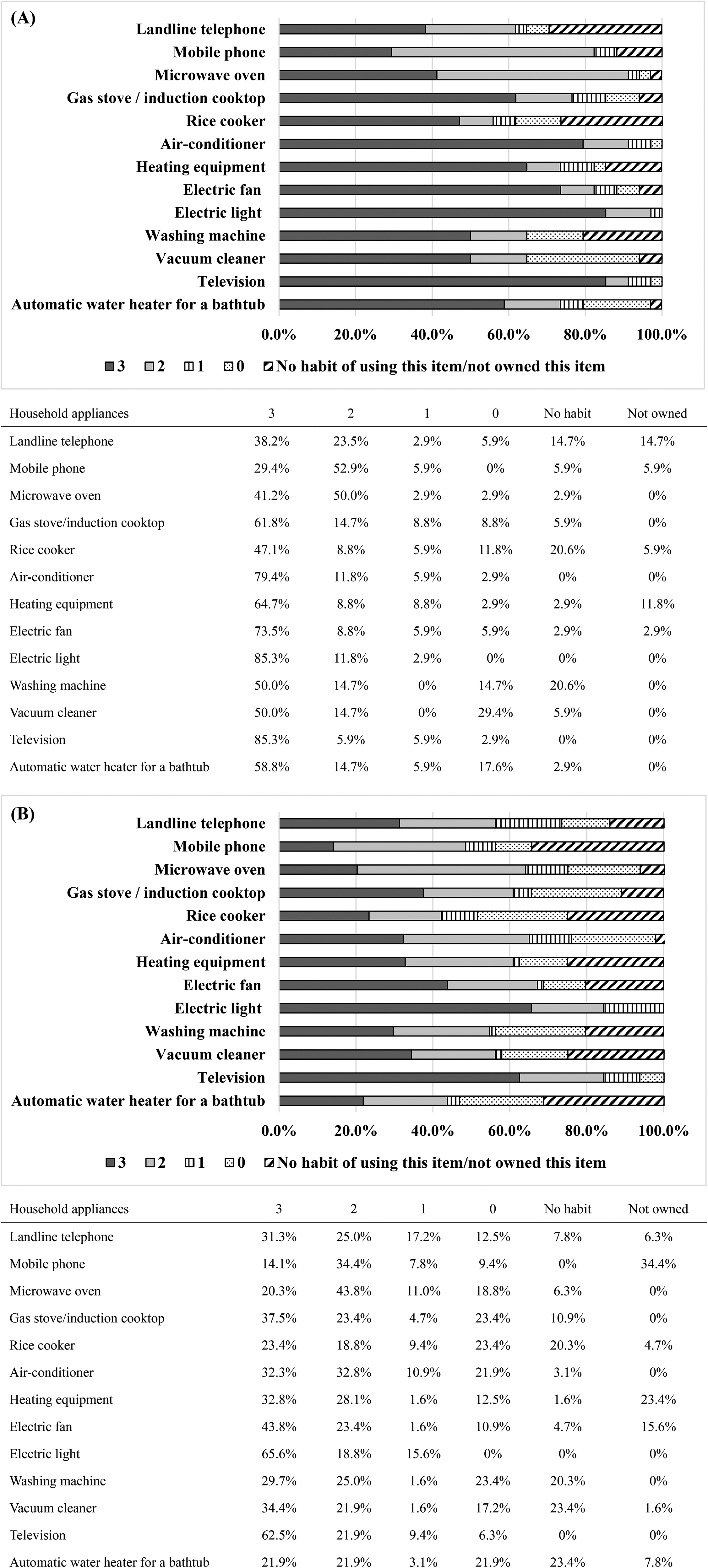
Ability to use each household appliance in non-dementia and dementia groups. Panel A shows the percentage of responses in the non-dementia group, while Panel B illustrates the percentage of responses in the dementia group. The ability to use each item is rated on a four-point scale from 0 to 3, where 3 indicates that the patient can use the appliances appropriately by himself/herself, 2 indicates that the patient can use the device on their own only for some simple operations, 1 indicates that the patient uses the device with help or under the supervision of a caregiver, and 0 indicates that the patient is unable to use the device at all. (A) Non-dementia group. (B) Dementia group.
Comparison of Kyoto-IADL scores between non-dementia and dementia groups
The scores of the Kyoto-IADL in the non-dementia and dementia groups are presented in Table 2. A comparison was made between the scores of these two groups. For many electric appliances, the scores of the dementia group were significantly lower than those of the non-dementia group. However, no significant difference was found in the scores for four items: landline telephone, rice cooker, washing machine, and vacuum cleaner (Table 2).
The total score for the dementia group (21.2 points) was significantly lower than that of the non-dementia group (28.4 points, S = 2163.5, Z = 3.59, p = 0.0003). Thus, it was found that there was a significant difference between the dementia and non-dementia groups across all appliances (except for the four listed above) and in the overall total score.
Discrimination ability in each household appliance
An attempt was made to discriminate whether patients had a life disability at a level that could be diagnosed as dementia, based on their ability to use these appliances. An ROC curve analysis was conducted using the score of each appliance as the predictor variable. The AUC, cutoff point, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) are shown in Table 4. The air conditioner demonstrated the highest discrimination power (AUC = 0.75), while the landline telephone had the lowest (AUC = 0.51).
The AUC, cutoff point, sensitivity, specificity, PPV, and NPV for each household appliance.
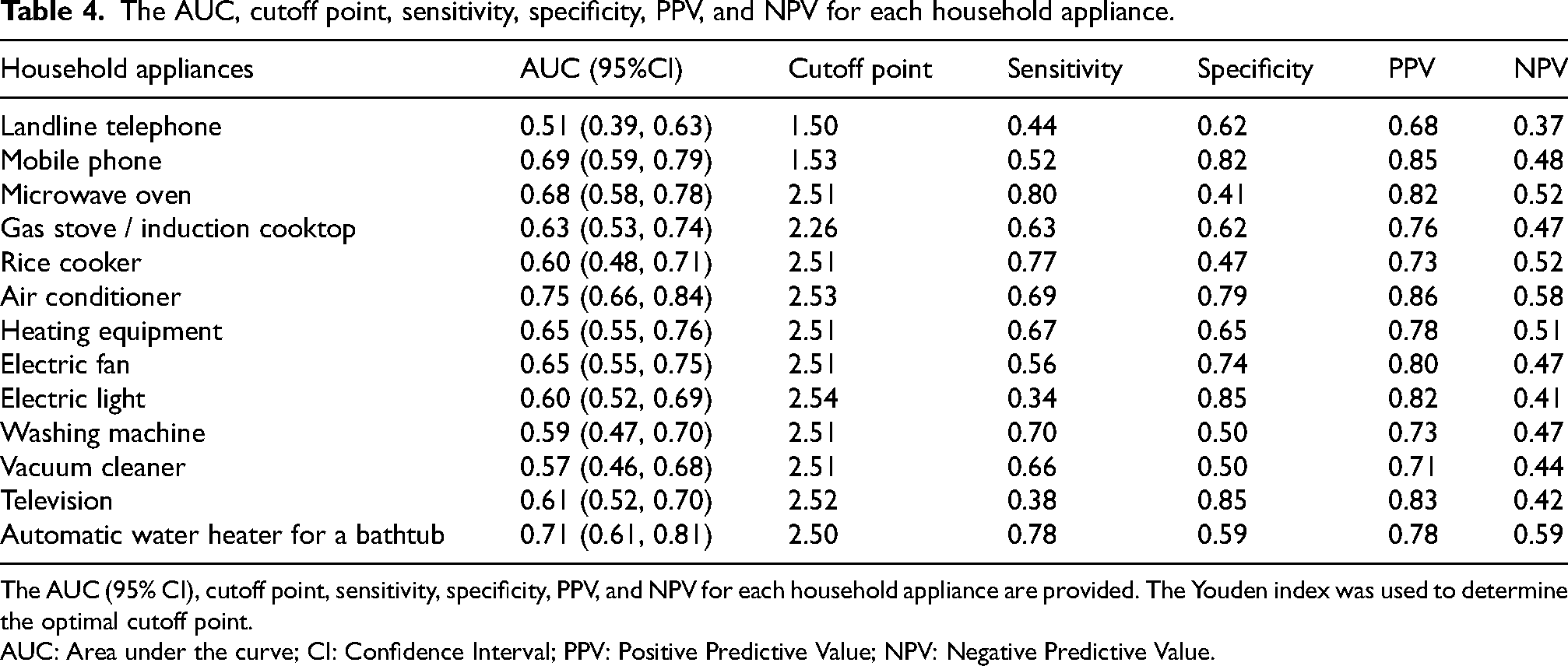
The AUC (95% CI), cutoff point, sensitivity, specificity, PPV, and NPV for each household appliance are provided. The Youden index was used to determine the optimal cutoff point.
AUC: Area under the curve; CI: Confidence Interval; PPV: Positive Predictive Value; NPV: Negative Predictive Value.
Calculation of a model equation to estimate the level of life disability based on the ability to use household appliances
The aforementioned logistic regression analysis was conducted using the score of each appliance as the predictor variable. Next, a logistic regression analysis was conducted using the total score and scores of multiple appliances as predictor variables to identify more accurate predictors of discriminant ability.
Initially, ROC curve analysis was performed using the total score of the Kyoto-IADL as a predictor, resulting in an AUC of 0.72. This value was slightly lower than the air conditioner's AUC of 0.75, which was the highest among the individual appliance analyses (Table 4).
A multiple logistic regression analysis was then conducted using the scores of several appliances as predictor variables. In this analysis, eight items were utilized as predictor variables, excluding five items with a missing data rate of 20% or more (i.e., mobile phone, rice cooker, washing machine, vacuum cleaner, automatic water heater for a bathtub). This decision was made because, in this study, the absence of ownership or lack of usage habit for these items was imputed with a score of 0, potentially biasing the results toward a score of 0. Through the stepwise method, the two factors of the microwave oven and air conditioner were adopted as factors in the optimal model equation, yielding an AUC of 0.78 (as shown in Table 5), which was slightly higher than that of the air conditioner alone (AUC = 0.75). The VIF value was 1.12, indicating no concerns regarding multicollinearity. The probability of the logistic regression model for all cases with the intercept of the logistic regression model β0 = 3.83, log odds ratio of the air conditioner β1 = -0.97 at the Kyoto-IADL score x1, log odds ratio of the microwave oven β2 = -0.50 at the Kyoto-IADL score x2 is given by
The or and AUC for optimal model equations in determining life disability for (a) all cases, (b) males, (c) females, (d) under 82 years, (e) over 82 years.
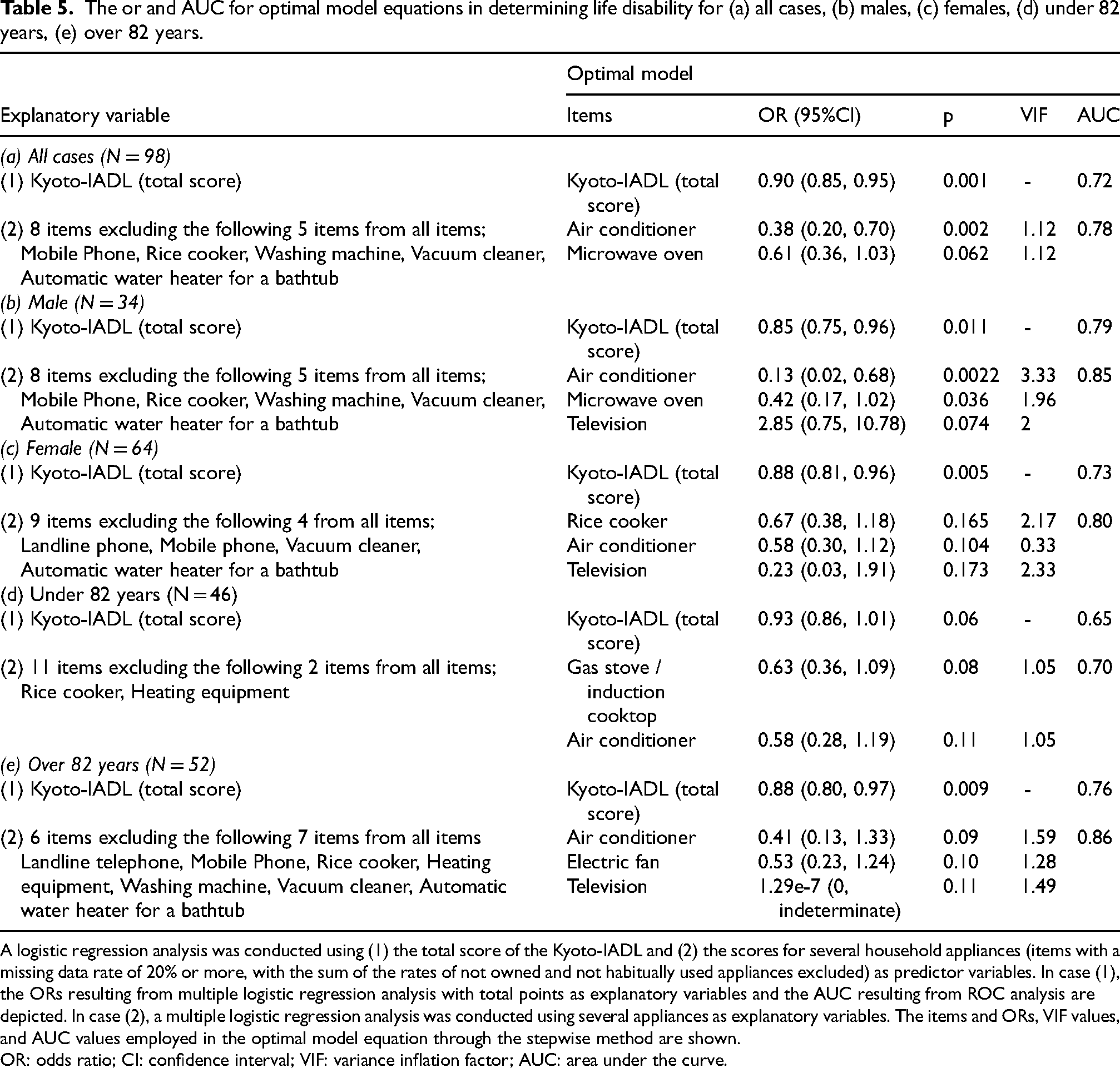
A logistic regression analysis was conducted using (1) the total score of the Kyoto-IADL and (2) the scores for several household appliances (items with a missing data rate of 20% or more, with the sum of the rates of not owned and not habitually used appliances excluded) as predictor variables. In case (1), the ORs resulting from multiple logistic regression analysis with total points as explanatory variables and the AUC resulting from ROC analysis are depicted. In case (2), a multiple logistic regression analysis was conducted using several appliances as explanatory variables. The items and ORs, VIF values, and AUC values employed in the optimal model equation through the stepwise method are shown.
OR: odds ratio; CI: confidence interval; VIF: variance inflation factor; AUC: area under the curve.
The ROC curve for this model (a) is shown in Figure 2.
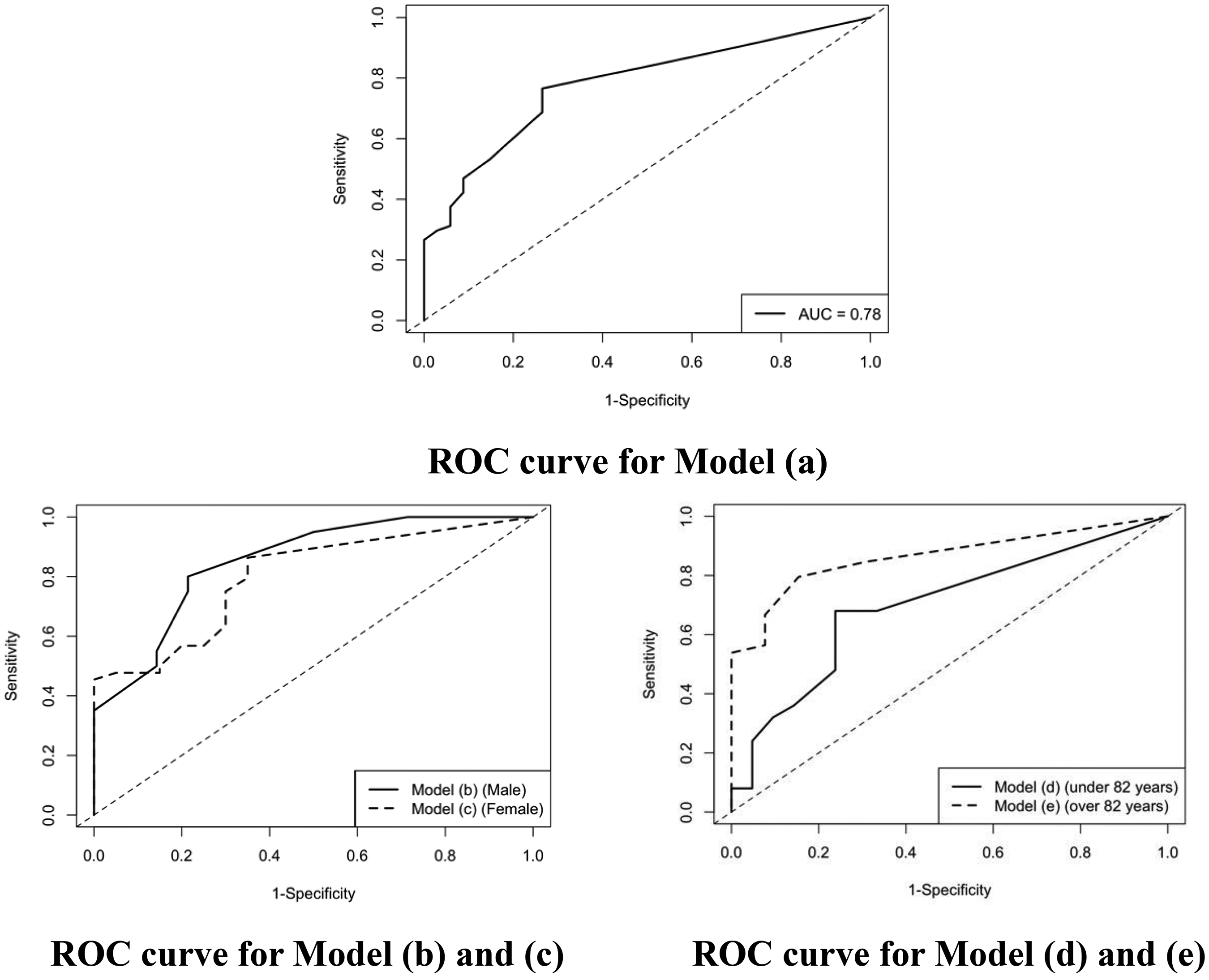
ROC curve for each model. The ROC curve for model (a) – all cases: the AUC is 0.78. The ROC curve for model (b) –male and (c) –female: the AUC for model (b) is 0.85 and model (c) is 0.80. The ROC curve for model (d) – under 82 years and (e) – over 82 years: the AUC for model (d) is 0.70 and model (e) is 0.86. ROC curve: receiver operating characteristic curves; AUC: area under the curve.
Comparison of Kyoto-IADL results by gender
An examination was conducted to determine if there were any gender differences in the use of home appliances by comparing the results of the Kyoto-IADL by gender. No significant differences in age (S = 1720, Z = 0.27, p = 0.78) and MMSE scores (S = 1884.5, Z = 1.51, p = 0.13) were observed between genders.
The missing data rates (the sum of the rates of “not owning this item” and “no habit of using this item”) for male and female participants are detailed in Table 3. For males, the items with a missing data rate of 20% or more were rice cooker (58.9%), washing machine (55.9%), vacuum cleaner (29.4%), mobile phone (23.5%), and automatic water heater for a bathtub (20.6%). On the other hand, for females, the items with a missing data rate of 20% or more were automatic water heater for a bathtub (28.2%), mobile phone (28.1%), landline phone (25.0%), and vacuum cleaner (25.0%).
The mean total score of the Kyoto-IADL was 20.4 (SD = 8.4) for males and 25.4 (SD = 9.1) for females, indicating a significant gender difference (S = 1302.5, p = 0.0045).
We obtained the optimal model equation for assessing life disability using the Kyoto-IADL (total score) as a predictor variable for males and females separately. Further, the value of AUC was 0.79 for males and 0.73 for females (shown in Table 5).
Subsequently, a multiple logistic regression analysis was conducted using eight items as predictor variables, excluding the five items (i.e., mobile phone, rice cooker, washing machine, vacuum cleaner, automatic water heater for a bathtub) with a missing data rate of 20% or more for males. Using the stepwise method, the microwave oven, air conditioner, and television were adopted as factors in the optimal model equation, resulting in an AUC of 0.85 (Table 5). The probability of the logistic regression model for male cases with the intercept of the logistic regression model β0 = 4.25, log odds ratio for the air conditioner β1 = −2.06 at the score x1, log odds ratio of the microwave oven β2 = −0.87 at the Kyoto-IADL score x2, and log odds ratio of the television β3 = 1.05 at the Kyoto-IADL score x3 is given by

The ROC curves for the models (b) and (c) are shown in Figure 2.
Comparison of Kyoto-IADL results by age
The median age of the participants was 82 years (IQR: 78–85). Age is a factor believed to influence the use of home appliances, prompting the division of all subjects into those under 82 and those over 82 to examine the effect of age on appliance usage.
The group under 82 (N = 46) comprised 14 males and 32 females, with a mean MMSE score of 22.4 (SD = 4.7), while the group over 82 (N = 52) consisted of 20 males and 32 females, with a mean MMSE score of 20.3 (SD = 4.7). There were no significant differences in gender (χ2 = 0.69, p = 0.40) between the two groups. The MMSE score of the group under 82 was significantly higher than that of the group over 82 (S = 2590, Z = 2.23, p = 0.03). The missing data rate (the sum of the rates of “not owning this item” and “no habit of using this item”) for the two groups is shown in Table 3.
For the group under 82, the items with a missing data rate of 20% or more were the rice cooker (26.1%) and heating equipment (21.7%), whereas for the group over 82, the items with a missing data rate of 20% or more were the mobile phone (38.5%), rice cooker (25.0%), vacuum cleaner (23.1%), automatic water heater for a bathtub (23.1%), washing machine (23.1%), landline telephone (23.1%), and heating equipment (21.2%). The total score of the Kyoto-IADL was significantly higher in the under 82 group, amounting to 26.7, compared to the over 82 group, which came to 21.1, indicating higher life disability in older individuals (S = 2687.5, Z = 2.92, p = 0.004).
We obtained the optimal model equation for determining life disability using the Kyoto-IADL (total scores) as predictor variables for each of the two age-based groups. The AUC was 0.65 for those under 82 and 0.76 for those over 82.
Afterward, multiple logistic regression analysis was conducted using 11 items as predictor variables, excluding rice cooker and heating equipment due to a missing data rate of 20% or more for those under 82. Using the stepwise method, a gas stove/induction cooktop and air conditioner were identified as relevant factors in the optimal model equation, resulting in an AUC of 0.70 (Table 5). The probability of the logistic regression model for patients under 82 with the intercept of the logistic regression model β0 = 2.49, log odds ratio of the gas stove/induction cooktop β1 = −0.46 at the Kyoto-IADL score x1, and log odds ratio of the air conditioner β2 = −0.55 at the Kyoto-IADL score x2 is given by

Thus, the items adopted in the optimal model equation differed according to the two age-based groups.
Internal validation of the AUC
The results of the internal validity of the AUC using bootstrap resampling (Iteration = 1000) are presented below.
Model (a): ROC-AUC: 0.78 / Bootstrap AUC: 0.78 / Bootstrap 95%CI: [0.69, 0.87] Model (b): ROC-AUC: 0.85 / Bootstrap AUC: 0.87 / Bootstrap 95%CI: [0.73, 0.97] Model (c): ROC-AUC: 0.80 / Bootstrap AUC: 0.78 / Bootstrap 95%CI: [0.71, 0.92] Model (d): ROC-AUC: 0.70 / Bootstrap AUC: 0.67 / Bootstrap 95%CI: [0.53, 0.81] Model (e): ROC-AUC: 0.86 / Bootstrap AUC: 0.86 / Bootstrap 95%CI: [0.76, 0.95]
All ROC-AUCs fell within the Bootstrap 95% confidence intervals, indicating a low likelihood of model overfitting and suggesting high internal validity of the models.
Discussion
Detecting life disability is crucial in the diagnosis of dementia; however, it has been challenging to detect early life disability using previous scales. To address this issue, our study focused on the practical ability to use household appliances to determine whether it is possible to detect life disability. We selected 13 essential household appliances commonly used by the elderly and created a scale, named the Kyoto-IADL to assess their ability to use them. Based on these results, a model equation was constructed to determine whether a subject's level of life disability is sufficient for a level that would be diagnosed as dementia or not. The Kyoto-IADL is a simple observational rating scale administered by caregivers to assess daily life disability based on the patient's ability to use everyday household appliances. This scale plays a significant role in clinical settings, as the presence or absence of daily life disability is crucial in differentiating between MCI and dementia.
Comparison of the ability between dementia and non-dementia cases
A comparison of the Kyoto-IADL scores of the two groups (the non-dementia and dementia groups) revealed that, as anticipated, the dementia group's scores were significantly lower, indicating a decreased ability to operate home appliances. Interestingly, of the 13 items surveyed, four appliances (i.e., landline phone, rice cooker, washing machine, and vacuum cleaner) demonstrated no significant differences between the two groups, suggesting that a high percentage of respondents were not accustomed to using these appliances regularly. Furthermore, for these four items, a decline in scores was observed in the non-dementia group, with minimal divergence in scores between the two groups. This phenomenon was attributed to individuals who were not in the habit of using these appliances receiving a score of 0.
Determining the degree of life disability based on the ability to use household appliances
Initially, a logistic regression analysis was conducted using the scores of each home appliance as predictor variables. The results revealed that air conditioners had the highest AUC values in ROC curve analysis, indicating their superior ability to distinguish the degree of life disability compared to other household appliances.
Calculation of a model equation to determine dementia/non-dementia by comprehensively evaluating the ability to use household appliances
First, a logistic regression analysis was conducted using the total score of the Kyoto-IADL as a predictor. The AUC value (Table 5) obtained in ROC curve analysis, indicating discriminatory ability, was lower than the maximum values achieved in the analysis for individual home appliances, which is presented in Table 4.
Next, a logistic regression analysis was conducted using the scores of multiple appliances as predictor variables. The optimal model equation for all cases, determined through the stepwise method, included the microwave oven and air conditioner as key factors. The AUC values for this model equation were higher than those for each individual appliance, with no concerns of multicollinearity based on VIF values. Although the items employed in the optimal model equation included some non-significant items based on the p value, a higher discriminative power was obtained due to the inclusion of these items. This suggests that a more accurate evaluation can be achieved by focusing on the aforementioned two factors rather than evaluating each home appliance separately.
Impact of gender differences
Compared to females, a higher percentage of males answered positively to “no habit of using this item” for household-related products, such as rice cookers, vacuum cleaners, and washing machines. The model equation used to assess life disability, calculated separately for males and females, revealed that focus should vary based on gender. The AUC values were higher when using model equations (b) and (c) for males and females, respectively, compared to using model equation (a) for all patients. These results suggest that differences in experience with household appliances between males and females should be considered when assessing daily living disability. The disparity in housework experience between males and females in this generation is not surprising, as a study from the 1990s described tasks like cooking and cleaning as “female-stereotypic” or “feminine tasks”. 23
Although Lawton's IADL scale, a commonly used assessment tool, exhibited gender differences in assessment categories, recently developed scales (i.e., Amsterdam IADL and ETUQ) do not consider gender variations. In modern society, where gender diversity is increasingly acknowledged, distinguishing between males and females may not be deemed appropriate. However, for the older generation (especially those in their 80 s), it may be relevant to consider the impact of gender differences.
Impact of age
The over 82 group had a particularly high percentage of not owning a mobile phone, indicating that IT devices may be unfamiliar to the older generation. Both the under 82 and over 82 groups exhibited high percentages of “no habit of using this item” in relation to home appliances, such as rice cookers, washing machines, vacuum cleaners, and automatic bath water heaters.
The model equation used to assess life disability, calculated separately for both groups, revealed variations in the focus on appliances by generation. The AUC calculated by model equation (d) for patients under 82 was lower than that of model equation (a) for all patients. Conversely, the AUC calculated by model equation (e) for patients over 82 was higher than that of model equation (a). This suggests that model equation (e) may be more suitable for individuals over 82 than model equation (a). Although there were no significant gender differences between the two groups, a significant difference was indeed observed in MMSE scores. The differences in household appliance usage cannot be fully explained by cognitive decline due to aging alone; other factors, such as differences in lifestyle and daily habits, may also play a role. In other words, appliance usage seems to depend not only on cognitive function but also on age. Therefore, it may be more appropriate to evaluate different types of appliances separately based on age to make more accurate assessments.
Internal validation
In this study, we validated the internal validity of the ROC-AUC using the bootstrap method. Post-bootstrap (Iteration = 1000) allowed for a more stable evaluation of the model's performance.
Comparison of Kyoto-IADL to other IADL scales
In this study, we focused on investigating essential appliances used in the daily lives of the elderly. Compared to previous studies using ETUQ and Amsterdam IADL,17,21,24 the number of appliance items investigated in this study is small. However, since we selected a wide range of home appliances, from cooking and housekeeping to communication and audio-visual appliances, we believe we captured a comprehensive view of daily life. Despite the limited number of items, the survey was efficiently completed in a short time (about 5–10 min), allowing us to assess life disabilities comprehensively.
The optimal model equation (a), determined through the stepwise method, identified the microwave oven and air conditioner as the two key factors, returning an AUC of 0.78. A previous study on the Amsterdam IADL questionnaire reported an AUC of 0.75 (95% confidence interval [CI]: 0.70–0.81) for discriminating between dementia and non-dementia patients, 21 and the discrimination performance in this study was comparable to existing scales. Further, our survey findings revealed that evaluating the types of equipment according to age and gender is more appropriate, considering differences in lifestyles and housework experiences.
To increase the utility of the Kyoto-IADL, it is imperative to incorporate the results gained from this study and update the tool to align with the specific home appliances relevant to the lifestyles of each country. Furthermore, future iterations of this application should consider the historical context of the elderly individuals’ lives and their evolving lifestyles.
Future research should also investigate the relationship between the Kyoto-IADL and other established IADL scales. For instance, the ADCS MCI-ADL, which assesses daily living activities in individuals with AD, includes sub-items such as “doing laundry,” “using the telephone,” “preparing meals,” “watching television,” and “using household appliances.” 25 These items are consistent with those found in the Kyoto-IADL. Kyoto-IADL differs from other IADL scales in that it investigates essential household appliances in more detail in the section regarding “using household appliances.” Since the ability to use household appliances declines early in dementia, Kyoto-IADL may have a greater potential to detect early MCI and dementia.
Limitations
Individual lifestyles vary greatly, leading to differences in the percentage of missing data for household appliances based on region, age, and gender. For instance, while air conditioner was found to have high discriminatory power in Japan, it may not be used in countries with different climate conditions. Therefore, air conditioning may not be a valid indicator in all countries or regions. While investigating two or three appliances, including air conditioner, is effective in Japan, it will be necessary to broadly examine appliances based on local lifestyles in other countries. This is a limitation of this study and requires further investigation.
In this study, missing data (i.e., “not owning this item” and “no habit of using this item”) was assigned a value of 0 points, which is the same as in the case of “do not have the ability to use.” Appliances with a missing data rate of 20% or more were excluded from the analysis. Moving forward, it is necessary to consider how home appliances that are “not owned” and “not originally in the habit of using” should be treated in the analysis.
This study was analyzed separately for male and female to examine the impact of gender differences on life disability assessment. A limitation of the study was the smaller number of male cases than female cases, highlighting the need for future research to increase male participation.
Furthermore, future analyses should be performed by increasing the number of cases to combine age groups and gender to, for example, find the optimal model equation for males/females over the age of 82.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251320668 - Supplemental material for Assessment of instrumental activities of daily living in patients with cognitive impairment based on their ability to use household appliances
Supplemental material, sj-docx-1-alz-10.1177_13872877251320668 for Assessment of instrumental activities of daily living in patients with cognitive impairment based on their ability to use household appliances by Momoyo Shimosaka, Hiroyuki Nishimoto, Sayaka Okahashi, Derong Zeng, Kayoko Fukui, Teruaki Kawasaki, Ichiro Akiguchi and Ayae Kinoshita in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We would like to acknowledge the technical experts at e.Soft Corporation for their assistance in developing the necessary software for our research.
Author contributions
Momoyo Shimosaka (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Software; Validation; Visualization; Writing – original draft); Hiroyuki Nishimoto (Conceptualization; Formal analysis; Methodology; Software; Supervision; Validation; Visualization; Writing – review & editing); Sayaka Okahashi (Conceptualization; Methodology; Software; Writing – review & editing); Derong Zeng (Data curation; Resources); Kayoko Fukui (Data curation; Resources); Teruaki Kawasaki (Data curation; Project administration; Resources; Supervision); Ichiro Akiguchi (Data curation; Project administration; Resources; Supervision); Ayae Kinoshita (Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the Mitsubishi Foundation (Project No. 203180600017), the Kyoto University GAP Fund Program (2020), and Pfizer Health Research Foundation (Project No. 203230600064). The funding sources did not have any specific involvement in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.