
Abstract
Background
Little is known about the utilization of outpatient support services by people with mild cognitive impairment (MCI).
Objective
This study aimed to analyze the use of support services by people with MCI compared to people with mild to moderate dementia.
Methods
The data basis is the multicenter, prospective register study ‘Digital Dementia Register Bavaria – digiDEM Bayern’. The sample consists of 913 people with cognitive impairment, including 389 with MCI and 524 with mild to moderate dementia. Classification into ‘MCI’ and ‘mild to moderate dementia’ is based on the Mini-Mental State Examination and Montreal Cognitive Assessment. The use of support services was surveyed using the Dementia Assessment of Service Needs. Fisher’s exact test and multiple linear regression were conducted to analyze for group differences.
Results
Four out of thirteen support services are used less frequently by people with MCI than by people with mild to moderate dementia: ‘Outpatient care’ (p < 0.001, φ = −0.199), ‘Acquisition of aids’ (p = 0.004, φ = −0.096), ‘Adult daycare’ (p < 0.001, φ = −0.290), and ‘Respite care’ (p = 0.029, φ = −0.095). Even the overall utilization rate is lower for people with MCI (b = −0.18, p = 0.027), although other factors such as a care level (b = 1.01, p < 0.001) are more strongly related.
Conclusions
There are differences in utilization between people with MCI and people with mild to moderate dementia, but these are small. Therefore, access to support services should be provided at the first signs of cognitive impairment.
Introduction
The global prevalence of people with mild cognitive impairment (MCI) over 50 years is estimated at 15.56%. 1 The syndrome MCI describes a cognitive decline greater than expected for a person's age and educational level and represents a decline in the person's prior status of functioning.2,3 The activities of daily living remain largely unimpaired, so people with MCI do not require support due to cognitive impairment.2,4 Within five years, 72% of people with amnestic MCI progress to dementia, resulting in a need for support in their everyday lives. 5 There are currently more than 55 million people living with dementia worldwide, and about 10 million new cases are identified every year. 6 Most people with dementia are cared for at home by a family caregiver, often resulting in a high caregiver burden and stress.7,8 In Germany, for example, 80% of people in need of care are cared for at home by a family caregiver. 9 Using outpatient support services can provide relief for family caregivers in the home care situation.
Nevertheless, various international studies report low utilization of support services by people with dementia and their family caregivers.10–16 But, even family caregivers of people with MCI show increased levels of burden, mainly when neuropsychiatric symptoms deteriorate, and executive functions decline. 17 However, little is known about the use of support services by people with MCI and their caregivers.18,19 An American study examined the need for support services for people with MCI and their family caregivers, however, not the use. 19 The need for a support service was defined as ‘yes, it is used’ and ‘not used, but the service is needed’. The authors compared the need for family caregivers by people without cognitive impairment, people with MCI, and people with dementia. Results show a similar need for support services by family caregivers of people with MCI and dementia. These findings are surprising, as people with MCI are defined as having fewer cognitive impairments and are predominantly able to manage everyday life. Making use of support services at the beginning of cognitive impairment can not only relieve the burden on family caregivers at an early stage but makes it more likely that it will be used at a later stage when cognitive decline is more advanced. 10 A study from the Netherlands focused on the different combinations of service types used by people with cognitive impairment, providing a better understanding of care pathways. The results showed that people with MCI are less likely to use a combination of ‘informal care’ compared to people with dementia. 18 Other international studies address the utilization of medical services by people with MCI but do not consider other support services.20–23
To our knowledge, there is no research focusing on the use of outpatient support services by people with MCI. The use of support services by people with dementia and their family caregivers is investigated comprehensively. Therefore, our work aims to focus on people with MCI when analyzing the use of support services and compare them with the use of people with mild to moderate dementia. For a comprehensive overview, no focus is given to a specific type of support services. In addition to cognitive status, other associations with support services are investigated.
Methods
Study design and participants
This study is part of the ongoing project ‘Digital Dementia Registry Bavaria – digiDEM Bayern’. digiDEM Bayern is a multicentre, prospective, longitudinal register study conducted in all administrative regions of Bavaria (Germany). The detailed methodology of the project is described by Dietzel et al. 24
Study population
Participants are people with MCI and people with mild or moderate dementia, collectively called people with cognitive impairment. To identify eligible participants, people have to undergo a screening based on the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA).25,26 These psychometric tests are used to categorize ‘people with MCI’ and ‘people with mild to moderate dementia’ independent of the presence of a diagnosis. Inclusion criteria for people with dementia are MMSE scores between 15–23 points, living in their home environment, and having their primary residence in Bavaria. If the MMSE score is >23 points, the MoCA is conducted additionally to identify people with MCI. 27 If so, the range for inclusion is 0–23 points. 28 All types of dementia and all age groups are included. People with an MMSE score between 0 and 14 points or a MoCA score >23 points, people who live in a nursing home, people with psychiatric diagnoses (e.g., depression, schizophrenia, addictions) or aphasia, and people who are deaf or blind are excluded. If available, a family caregiver is included with the person with cognitive impairment. 24
Recruitment and data collection
Participants are recruited by research partners in all administrative regions in Bavaria beginning in August 2020. Research partners are institutions that are specialized and have experience in the management and care of people with cognitive impairment and their family caregivers, such as community counselling, support groups, flat-sharing communities, memory clinics, day-care hospitals, day-care facilities, outpatient care organizations, acute care hospitals, district hospitals, geriatric rehabilitation facilities, and general practitioners. In addition to recruitment, the research partners also conduct interviews and psychometric tests. To ensure the quality of the data collection, active participation in a 90-min course is mandatory for all research partners. The course covers topics such as the implementation of MMSE and MoCA, data protection, questionnaires, and data entry. Data collection is conducted using standardized face-to-face interviews using a web-based data entry system. 24
Data protection and ethics
digiDEM Bayern collects and stores all personal data separately from the registry data on different stand-alone systems to ensure data protection. The project is performed following the ethical standards of the Declaration of Helsinki and obtained ethical approval from the Ethics Committee of the Medical Faculty of the Friedrich-Alexander-Universität Erlangen-Nürnberg (application number: 253_20 B). Informed consent from the participants or their authorized representative is acquired before screening and study inclusion. 24
Measures
Use of support services
The use of various support services was surveyed using the Dementia Assessment of Service Needs (DEMAND). 29 The DEMAND covers the following outpatient support services: Primary care by a general practitioner, Housekeeping assistance, Outpatient care, Provision of psychosocial interventions, Acquisition of aids, Adult daycare, Counselling services, Supported living and alternative housing services, Respite care, Caregiver Training Programs for family caregivers, Short-term care, Palliative care, Nursing home. Insofar as a family caregiver participates in the interview, the family caregiver has answered the DEMAND. Based on the information about the 13 DEMAND support services, we built two scores to measure the number of support services used. First, a sum score (‘DEMAND Score 1’) consisting of all support services directly addressing persons with cognitive impairment was built. The utilization of ‘Respite care’ and ‘Caregiver Training Programs for family caregivers’ was not taken into account in ‘DEMAND Score 1’, as these services are only directed at family caregivers. Therefore, this service was only asked of people who took part in the surveys together with a family caregiver. For the second sum score (‘DEMAND Score 2’), the medical support services ‘Palliative care’ and ‘Primary care by a GP’ were not considered in addition to ‘Respite care’ and ‘Caregiver Training Programs for family caregivers’. This sum score was calculated to exclude support services that can only be provided in cooperation with physicians. The person with cognitive impairment or a family caregiver can't meet the demand in case of non-utilization of the support service.
Other measures
Sociodemographic information on age, sex, language, spatial type, family caregiver, educational level, and living situation (‘living alone’) was collected using a standardized questionnaire. The variable ‘language’ was assessed using the standardized question ‘What is the main language spoken in your household?’. The ‘spatial type’ is based on the allocation of the Federal Institute for Research on Building, Urban Affairs and Spatial Development (BBSR). 30 A ‘family caregiver’ is present when there is a person who provides support at least once a week. The ‘educational level’ was assessed according to the updated CASMIN classification based on school education and vocational training. 31 Current cognitive status was determined using MMSE and MoCA.25,26 Based on this, the groups ‘people with MCI’ and ‘people with mild to moderate dementia’ were defined, as described in more detail under ‘study population’. The presence of ‘severe disability’ is based on the definition of the German Social Code IX, Section 2 (1) [SGB IX, ‘Schwerbehinderung’]. Health-related quality of life was assessed with the EuroQuol-5 Dimensional questionnaire (EQ-5D) and is reported with the associated index. An EQ-5D index of 1 represents the best possible state of health, whereas an index of <0 represents the worst possible state of health.32,33 Based on the German Health and Care Insurance criteria, the need for care and support was asked by the classification into a care level [‘Pflegegrad’]. The analysis did not take into account the different care levels but only looked at the presence of any care level. This is due to the fact that this variable is primarily intended to investigate whether the classification into a care level results in a lower barrier (informational, financial) to accessing support services. Activities of daily living (ADL) were assessed with the Barthel index, with 0 points representing strong dependence and 100 points representing a state of complete independence in coping with ADL. 34 The variable ‘car driving’ was requested with the standardized question ‘Does the person with cognitive impairment actively participate in road traffic as a driver?’.
Statistical analysis
The baseline survey was used for the entire data analysis (survey period between August 2020 and August 2023). Descriptive data of the sample were presented. Group differences between people with MCI and people with dementia were determined using the T-test, Chi-square test, and Cohen’s d and Phi as effect size parameters. The results of the entire DEMAND were presented using descriptive data to provide a comprehensive overview of the use of various support services. To determine the differences in the use between people with MCI and people with dementia, Fisher's exact test and the Phi coefficient were calculated for each support service. In addition, group differences in ‘DEMAND Score 1’ and ‘DEMAND Score 2’ were analyzed using T-test and Cohen’s d. A multiple linear regression was calculated to determine whether cognitive group allocation is an independent factor in the number of support services used. As the dependent variable, the ‘DEMAND Score 2’ was used. This variable / the residuals of this variable show a slightly right-skewed distribution. Based on the existing literature, the results of regression models and T-tests are nonetheless robust.35,36 An exploratory approach was chosen to identify relevant control variables. Therefore, all variables with a bivariate significant correlation with the ‘DEMAND Score 2’ were included in the regression model. Correlation analyses were performed to check for multicollinearity. If the correlation coefficient was >0.50, the variable with the lower correlation coefficient with ‘DEMAND Score 2’ was removed from the model. A sensitivity analysis was performed to test the model concerning constructing two different DEMAND Scores. For this, a multiple linear regression with the same independent variables was performed with the dependent variable ‘DEMAND Score 1’. All analyses were performed using IBM SPSS Statistics 2. The significance level was set at p < 0.05.
Results
Descriptives
Table 1 provides an overview of the descriptive characteristics of the sample and presents differences between the subgroups of people with MCI and people with mild to moderate dementia. A total of 913 people with cognitive impairment were included in the analysis, with 389 people being categorized into the subgroup of people with MCI. In contrast, the other 524 persons are categorized into the subgroup of people with dementia. In addition to cognitive status, there are further group differences. The subgroup of people with MCI is younger (Welch's F(802.24) = −7.30, p < 0.001, d = −0.494), is less likely to have a family caregiver (χ²(1) = 74.48, p < 0.001, φ = −0.283), has higher levels of education (χ²(2) = 16.39, p < 0.001, φ = 0.134), is more likely to have a severe disability (χ²(1) = 10.31, p = 0.002, φ = 0.106), report higher health-related quality of life (Welch's F(865.85) = 3.62, p < 0.001, d = 0.239), is less likely to have a care level (χ²(1) = 138.98, p < 0.001, φ = −0.390), is less limited in ADLs (Welch's F(910.89) = 9.55, p < 0.001, d = 0.611), and is more likely to participate actively as driver in road traffic (χ²(1) = 139.71, p < 0.001, φ = −0.391). The groups do not differ significantly regarding sex, language, spatial type, or living situation. Of the support services considered in ‘DEMAND Score 1’, all people with cognitive impairment use a mean of 2.11 (SD = 1.44) support services. People with MCI use fewer support services than people with dementia (Welch's F(890.22) = −6.05, p < 0.001, d = −0.396). Of the support services considered in ‘DEMAND Score 2’, all people with cognitive impairment used a mean of 1.56 (SD = 1.27) support services. Even on this score, people with MCI use fewer support services than people with dementia (F(911) = −7.37, p < 0.001, d = −0.493).
Characteristics of participants.
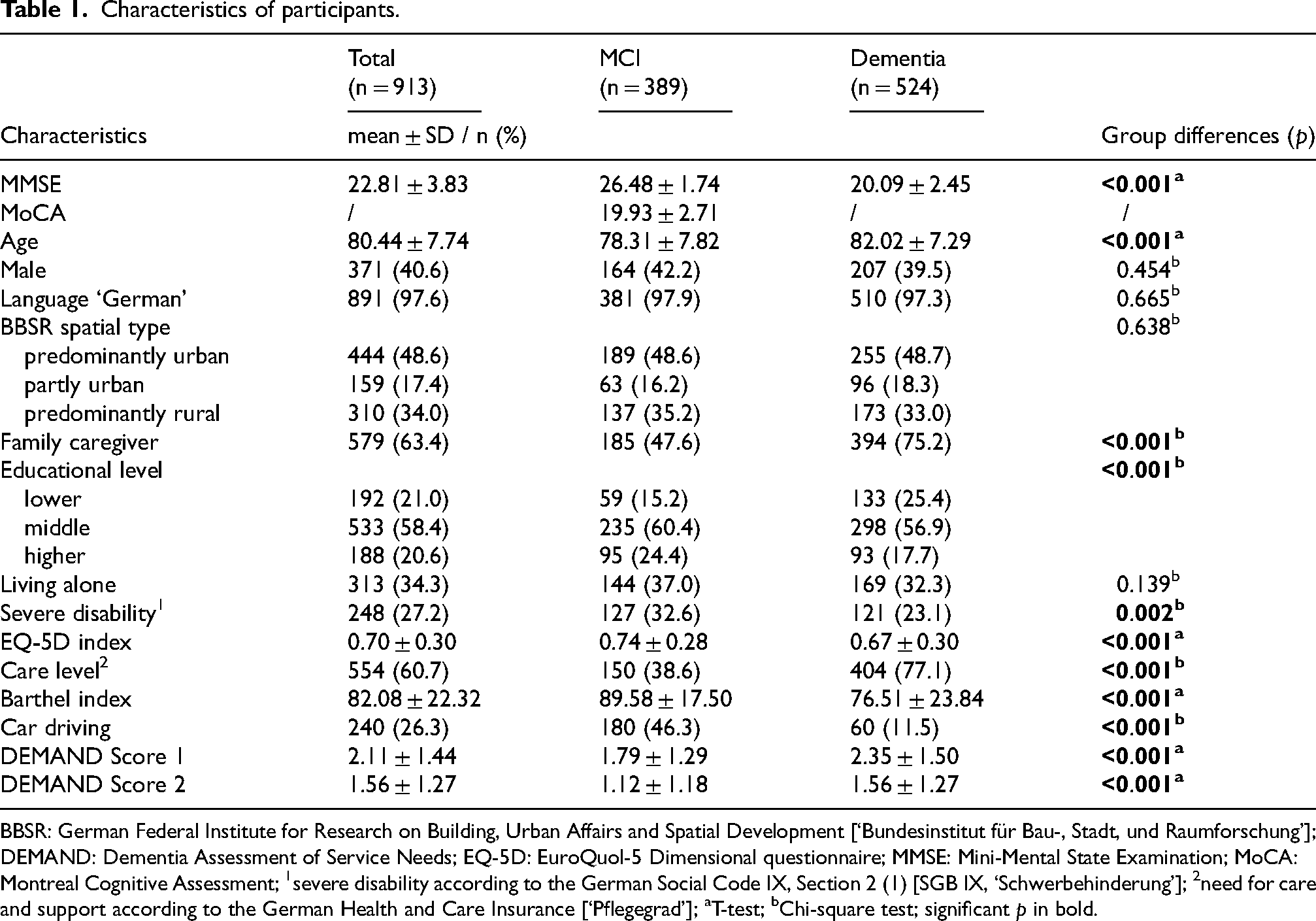
BBSR: German Federal Institute for Research on Building, Urban Affairs and Spatial Development [‘Bundesinstitut für Bau-, Stadt, und Raumforschung’]; DEMAND: Dementia Assessment of Service Needs; EQ-5D: EuroQuol-5 Dimensional questionnaire; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; 1severe disability according to the German Social Code IX, Section 2 (1) [SGB IX, ‘Schwerbehinderung’]; 2need for care and support according to the German Health and Care Insurance [‘Pflegegrad’]; aT-test; bChi-square test; significant p in bold.
Table 2 presents the use of support services by people with MCI and people with mild to moderate dementia. More than 30% of all respondents used ‘Primary care by a GP’ (54.4%), ‘Housekeeping assistance’ (36.5%), ‘Outpatient care’ (30.4%), and ‘Provision of psychosocial interventions’ (30.2%) in the past 30 days. The support services ‘Supported living and alternative housing services’ (5.4%), ‘Caregiver Training Programs for family caregivers’ (3.1%), ‘Short-term care’ (1.4%) and ‘Palliative care’ (0.2%) were used by less than 10% of the respondents. Excluding ‘Primary care by a GP’, all support services are used less often by people with MCI. However, statistically significant, only support services ‘Outpatient care’ (p < 0.001, φ = −0.199), ‘Acquisition of aids’ (p = 0.004, φ = −0.096), ‘Adult day care’ (p < 0.001, φ = −0.290), and ‘Respite care’ (p = 0.029, φ = −0.095) are used less often by people with MCI.
Utilization of support services by people with MCI and people with dementia.
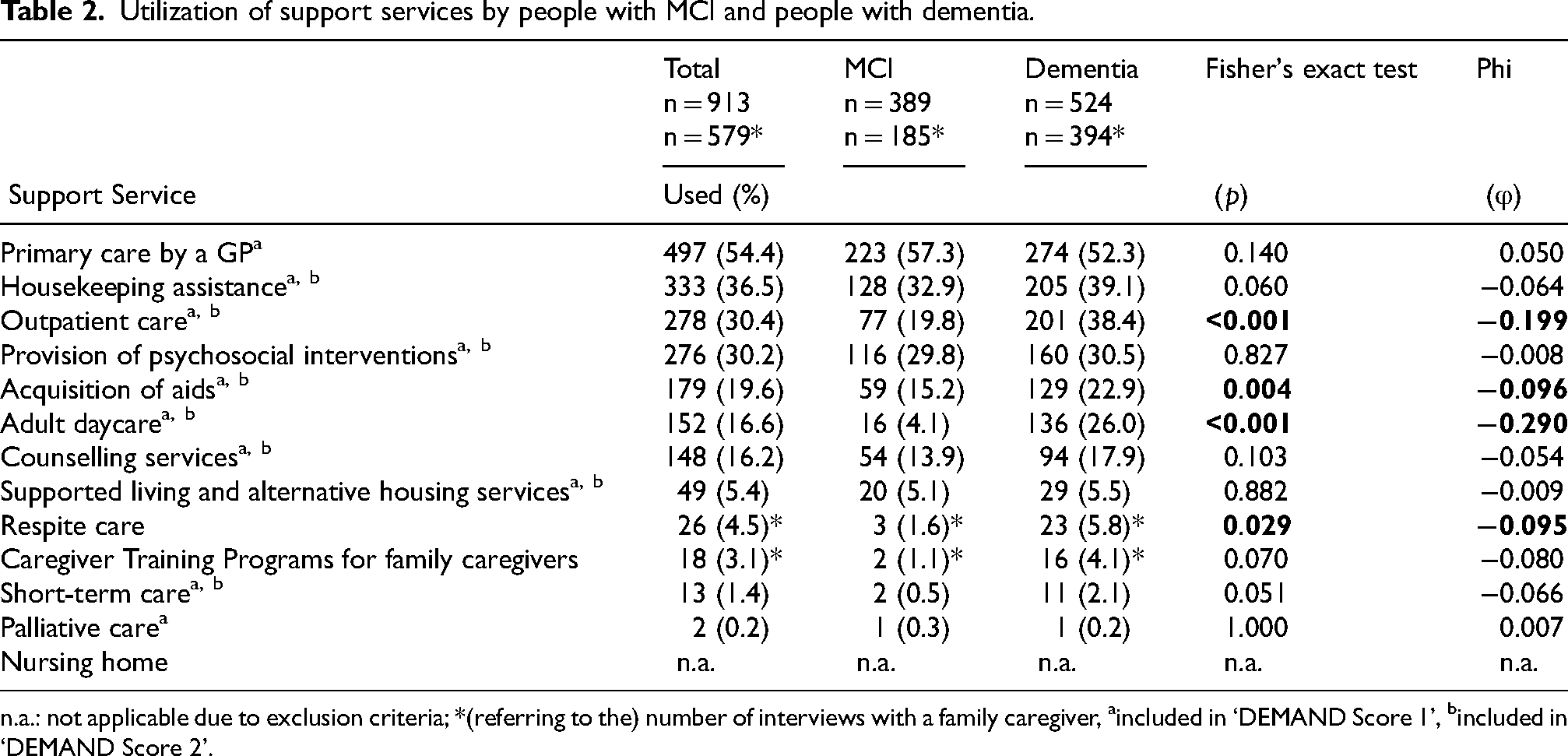
n.a.: not applicable due to exclusion criteria; *(referring to the) number of interviews with a family caregiver, aincluded in ‘DEMAND Score 1’, bincluded in ‘DEMAND Score 2’.
Main analysis
Table 3 shows the results of bivariate correlations for exploratory analysis of relevant independent variables for multiple regression analysis. Variables that do not correlate with ‘DEMAND Score 2’ are marked with an ‘a’ and were not included in the regression model. Those include language, spatial type, education (middle), and severe disability. Additionally, multicollinearity excluded two more variables from the regression model. The variables ‘Barthel index’ (p < 0.001, r = 0.521) and ‘car driving’ (p < 0.001, r = −0.575) correlated too strongly with ‘care level’. Thus, they could not be included in the regression model.
Correlation analysis with ‘DEMAND score 2’ to determine relevant independent variables.
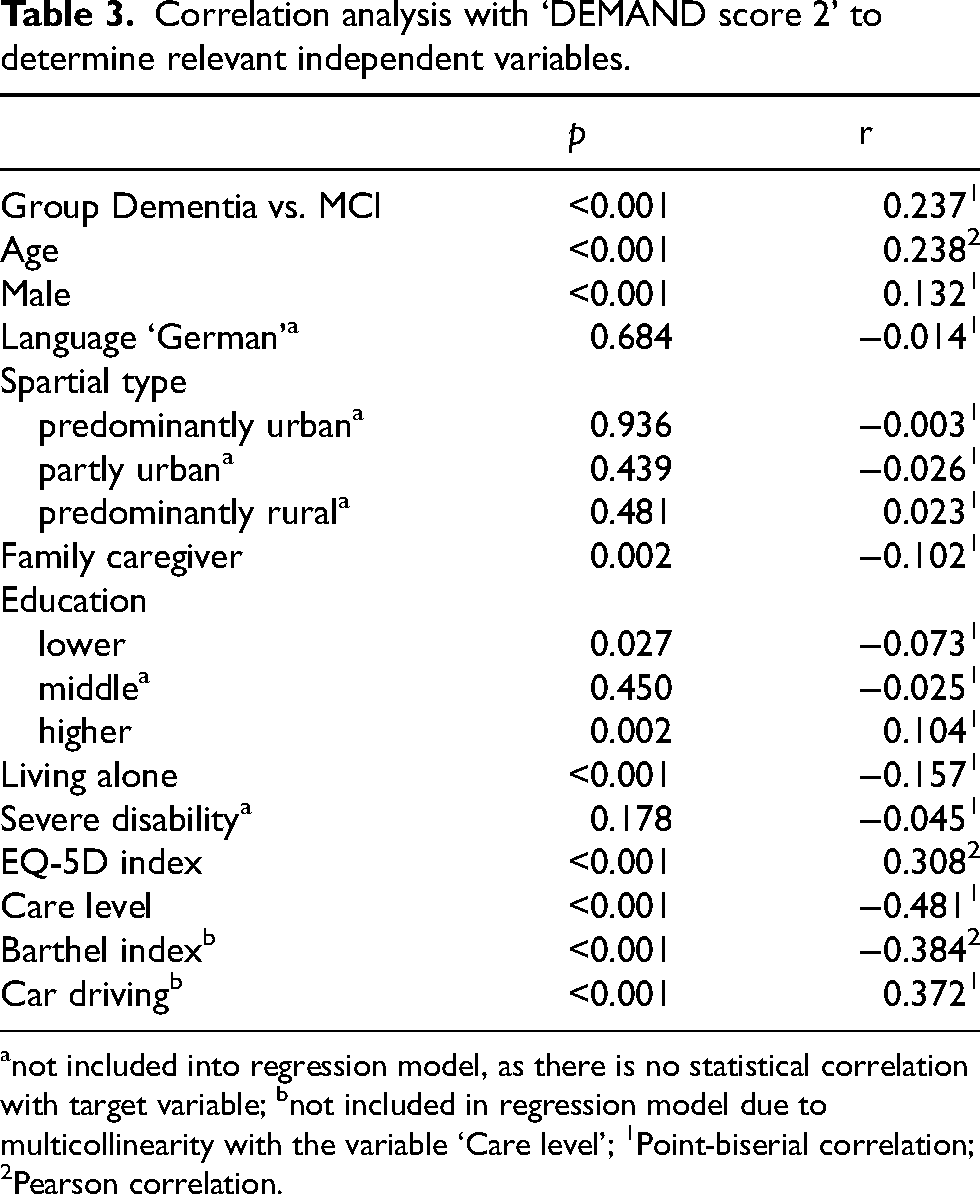
not included into regression model, as there is no statistical correlation with target variable; bnot included in regression model due to multicollinearity with the variable ‘Care level’; 1Point-biserial correlation; 2Pearson correlation.
Table 4 reports the results of the multiple linear regression. The model can significantly predict the number of support services used (F(9) = 40.21; p < 0.001). After controlling for several other potential predictors, people with MCI still use significantly less support services than people with mild to moderate dementia (b = −0.18, p = 0.027). However, other contributing factors are related to the number of support services used. More support services are used by older people (b = 0.01, p = 0.011), women (b = −0.20, p = 0.016), and people living alone (b = 0.27, p = 0.001). Furthermore, people with a lower health-related quality of life (b = −0.68, p = <0.001) and a care level (b = 1.01, p < 0.001) use more support services. The standardized beta coefficient shows that an existing care level is most strongly related to the number of utilization of services compared to the other variables (β = 0.39). ‘Group MCI vs. Dementia’ (β = −0.07), age (β = 0.08) and sex (β = 0.08) show the smallest associations.
Multiple regression analysis identifying independent associations with DEMAND score 2.
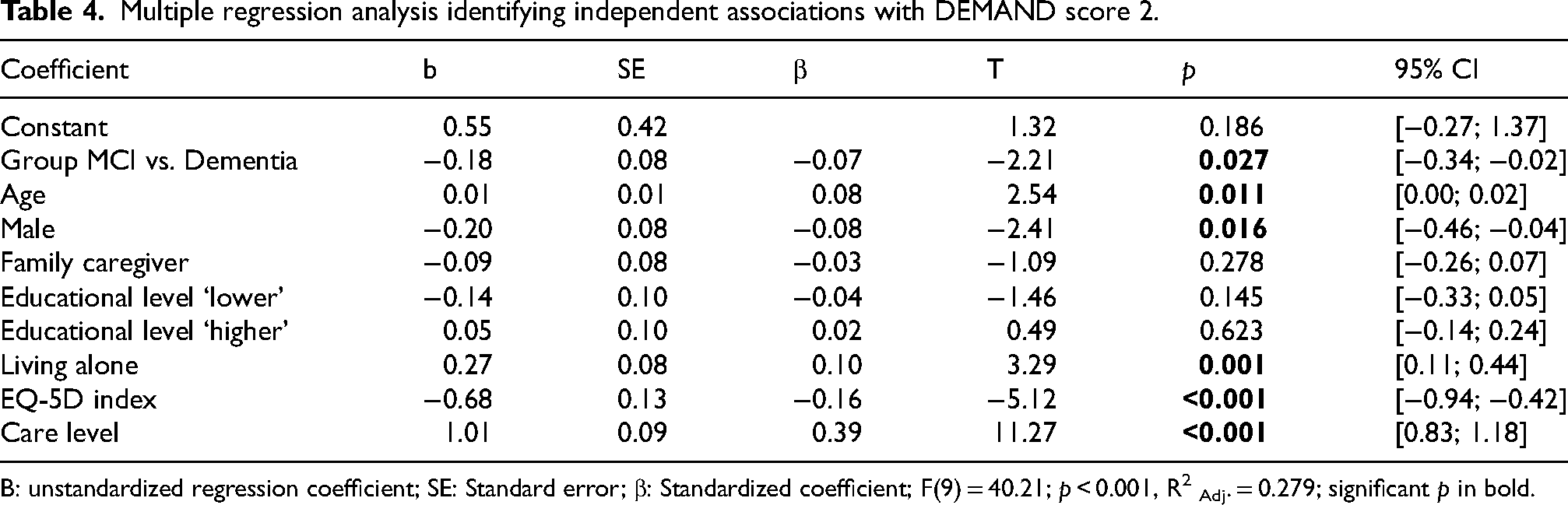
B: unstandardized regression coefficient; SE: Standard error; β: Standardized coefficient; F(9) = 40.21; p < 0.001, R2 Adj. = 0.279; significant p in bold.
The sensitivity analysis with ‘DEMAND Score 1’ as the dependent variable showed a change in significant results only for one predictor. When medical support services ‘Primary care by a GP’ and ‘Palliative care’ are taken into account in the score, no group differences between people with MCI and people with dementia in the number of support services used are apparent (b = −0.14, p = 0.135). Model quality deteriorated in the sensitivity analysis (R2 Adj. = 0.23).
Discussion
This is the first study describing and analyzing the use of different types of support services by community-dwelling people with MCI and comparing this with the use of support services by community-dwelling people with mild to moderate dementia. The main findings are: 1) While utilization of support services is generally low, the support services ‘Primary care by a GP’, ‘Housekeeping assistance’, ‘Outpatient care’, and ‘Provision of psychosocial interventions’ have decent utilization, 2) Only four out of thirteen support services are statistically significantly less likely to be used by people with MCI compared with people with mild to moderate dementia, 3) The number of support services used is lower for people with MCI, even after controlling for sociodemographic and health-related variables, 4) In addition to cognitive status, older age, female sex, living alone, low quality of life, and the presence of a care level have an association with the utilization of support services, with the presence of a care level being most strongly associated with the utilization of support services, 5) There are no differences in utilization between people with MCI and people with mild to moderate dementia when medical support services are taken into account, 6) Utilization of support services is not associated with language, spatial type, education (middle), or severe disability. These results provide a comprehensive insight into the care situation of people with cognitive impairment and their caregivers in Bavaria, as discussed below.
Our results show that the utilization of support services is relatively low in people with MCI and people with dementia, with an average score of 2.1 support services used in the past 30 days. This is a subjective assumption, as there are no cut-off values for the DEMAND so far, but this observation is consistent with the existing literature.10–16 The low utilization can be due to various reasons, such as no need, lack of knowledge about support services, fear of stigmatization, barriers such as transport or funding, values and beliefs, or negative experiences.15,29,37 In addition, some of the interviews were conducted during the COVID-19 pandemic. Contact restrictions, closures, and structural changes in the provision of support services can impact lower utilization rates. 38 The sample includes people with MCI or mild to moderate dementia - low use of support services may be sufficient for this level of cognitive impairment. 39 However, based on the ‘Barthel Index’, the ‘Care Level’, and ‘Severe disability’, the need for support of the sample is evident. It is also well-known in the existing literature that support services do not equate to existing needs.14,29,40–42
Considering the univariate model (Table 2), only four out of thirteen support services are statistically significantly less likely to be used by people with MCI compared with people with dementia (‘Outpatient care’, ‘Acquisition of aids’, ‘Adult daycare’, and ‘Respite care’). The differences in the utilization are surprisingly small. In our sample, people with MCI are less likely to have a care level and are less impaired in ADLs than people with dementia. People with MCI, therefore, live more independently and require less support due to cognitive or physical impairment. However, in our sample, people with MCI are more likely to have a severe disability, which could be related to an increased need for support services. Even so, their use of most support services is similar to that of people with dementia. Moreover, the group differences in these four support services show only small effects. These results are consistent with those of the study by Ryan et al., that found no difference between the needs of people with MCI and those of people with dementia. 19
Considering the multivariate model (Table 4), the number of support services used is lower for people with MCI, even after controlling for age, sex, existence of a family caregiver, lower and higher educational level, living alone, and quality of life. The results show that the use of support services is not only related to cognitive status. Other contributing factors are older age, female sex, living alone, low quality of life, and the presence of a care level of the person with cognitive impairment. These results are partially confirmed in previous studies.
The relationship between age and utilization of support services shows inconsistent results in existing literature. For example, in a German study, older age was not identified as a predictor for using day care, but a higher age of the family caregiver was identified as a significant predictor. 43 Another study from the United Kingdom, though, reports that older age is associated with lower use of support services. 13 However, there are study results from Norway that have analyzed a higher utilization of support services in older age. 12 This study result is consistent with our findings. There are also studies that have investigated the relationship between sex and utilization of support services. Some studies found no association between sex and utilization.10,43,44 Two other studies report opposite results to ours, reporting that men with cognitive impairment are more likely to use support services than women.12,13
However, concerning the use of support services by people with cognitive impairment living alone, there is a common consensus in the literature that people living alone use more support services.12,44,45
To our knowledge, previous studies have not focussed on the relationship between quality of life and the presence of a care level with support services in people with cognitive impairment. The heterogeneity of the study results, which exists in part, might be due to different methodological approaches, specific samples, and country-specific circumstances such as health policies.
The multivariate model also shows that living alone, low quality of life, and the presence of a care level are more strongly related to the utilization of support services than cognitive status. In particular, the presence of a care level is strongly associated with the use of support services. On average, people with cognitive impairment use one more support service when a care level is present. One reason might be the comprehensive consulting services offered as part of the assessment by the Medical Service of the German Health Insurance. On the other hand, the presence of a care level enables funding opportunities for support services by health insurance companies.
The sensitivity analysis shows that the group differences in utilization between people with MCI and people with dementia are only apparent insofar as the medical support services are not taken into account. No differences in utilization between people with MCI and people with dementia are evident when ‘Primary care by a GP’ and ‘Palliative care’ are included. Note that only two persons in the entire sample used ‘Palliative care’, so the sensitivity analysis results refer almost entirely to the support service ‘Primary care by a GP’. So it can be assumed that medical support services, especially ‘Primary care by a GP’, are used similarly by people with MCI or dementia. This may be due to the fact that a GP is consulted independently of dementia due to other health issues. On the other hand, household-related or caring support services seem to be more strongly related to group differences between people with MCI and dementia.
It is also essential to highlight variables that, according to our results, are not related to the use of support services. The outcomes show no relationship with language, spatial type, or severe disability. Since only 2.4% of all respondents state that they predominantly speak another language than German, this result may be biased due to the sample, as other study results show that language can impact the utilization of support services in people with cognitive impairment. 46 Other study results report that the use of support services relates to spatial type.11,15 Discrepancies in these results are possible due to the different definitions of spatial type or different geographical conditions in other countries. Regarding education, other study results report a relationship between the educational level of the person with cognitive impairment and the use of support services, which is partially consistent with our findings based on educational levels ‘lower’ and ‘higher’. 13
The study participants are exposed to selection bias. On the one hand, participants were recruited from health care providers, most of whom are themselves providers of support services. Therefore, a higher utilization than in the general community can be assumed. On the other hand, the low utilization in the sample may be attributable to the inclusion criteria. For example, severe dementia cases are excluded from the survey. The results also indicate a selection bias, as people with MCI are significantly more likely to have a severe disability and a higher level of education. Thus, the study participants are not a representative random sample for community dwelling people with cognitive impairment.
Another limitation is that the analyses are limited to the characteristics of people with cognitive impairment. Other studies considered the characteristics of family caregivers as potential contributing factors. For example, age, income, occupational status, or even the relationship to the person with cognitive impairment can influence the utilization of support services.12,16,47
Another limitation is the group allocation. Since people with cognitive impairment, even before a diagnosis, should be included in the study, allocation to the groups of ‘people with MCI’ and ‘people with dementia’ is not based on diagnoses supported by clinical parameters but on established, standardized psychometric screening tests. However, this has the benefit that there is no selection bias of people with difficult access to a clinical diagnosis.
A further limitation is the restricted information about other diseases that can influence the use of support services. Apart from cognitive impairment, no other health problems were queried during the interview. The use of support services may also be necessary based on other health conditions that are not controlled.
In addition, it is not possible to determine the causality of the relationship as this is a cross-sectional analysis.
Implication for practice
Given the increasing prevalence of people with MCI and people with dementia, it is essential to consider the use of support services to optimize care and support.
In addition to people with dementia, people with MCI are also an important target group for outpatient support services. Early utilization of support services can ensure the care and support of people with cognitive impairment and their family caregivers from the onset of the first cognitive impairment to severe dementia. It is important to note that health care services and consultation services are the main focus when symptoms appear. Care services become more important as the symptoms progress. The use of support services for people with MCI can be a preventive opportunity to avoid some burden on family caregivers.
For both, people with MCI and people with mild to moderate dementia, it is essential to reduce barriers to the use of support services. Our results show that raising awareness of support services is important at the first signs of cognitive impairment. To achieve this, there should be easy access to services that identify personal needs, provide information about unknown support services, and explain possible access pathways. This includes a comprehensive service of advice and information about local support services. Such services should always be low-threshold and have an outreach character. They are intended to provide an overview and orientation of regional support services, taking individual needs into account. Case management is a valuable method for this and should be offered not only to people with dementia but also to people with MCI. Apart from person-centered approaches, the stigma of using support services must be reduced, which is linked to rethinking the role of family caregivers. Other barriers, such as transport or financing, must be easily solvable with less bureaucratic solutions.
Conclusion
The use of support services by people with MCI is lower than for people with dementia. However, the differences are slight. Access to support services (regardless of a dementia diagnosis) should already be provided at the first signs of cognitive impairment so that these can be utilized in the early stages of cognitive decline.
Footnotes
Acknowledgments
The authors are grateful to the participating interviewers and study participants of digiDEM Bayern. The present work was performed by Anne Keefer in (partial) fulfillment of the requirements for obtaining the degree “Dr. rer. biol. hum.” at the Medical Faculty of the Friedrich-Alexander-Universität Erlangen-Nürnberg.
Author contributions
Anne Keefer (Conceptualization; Formal analysis; Investigation; Methodology; Project administration; Writing – original draft); Nikolas Dietzel (Conceptualization; Investigation; Project administration; Supervision; Writing – review & editing); Peter L Kolominsky-Rabas (Data curation; Funding acquisition; Investigation; Project administration; Resources; Supervision; Writing – review & editing); Elmar Graessel (Conceptualization; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project ‘Digital Dementia Registry Bavaria – digiDEM Bayern’ is funded by the Bavarian State Ministry of Health, Care and Prevention as part of the funding initiative ‘BAYERN DIGITAL II’ (grant number: G42d-G8300-2017/1606-83). The funder was not involved in the study design, in the collection, analysis, and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author.